

















Topic
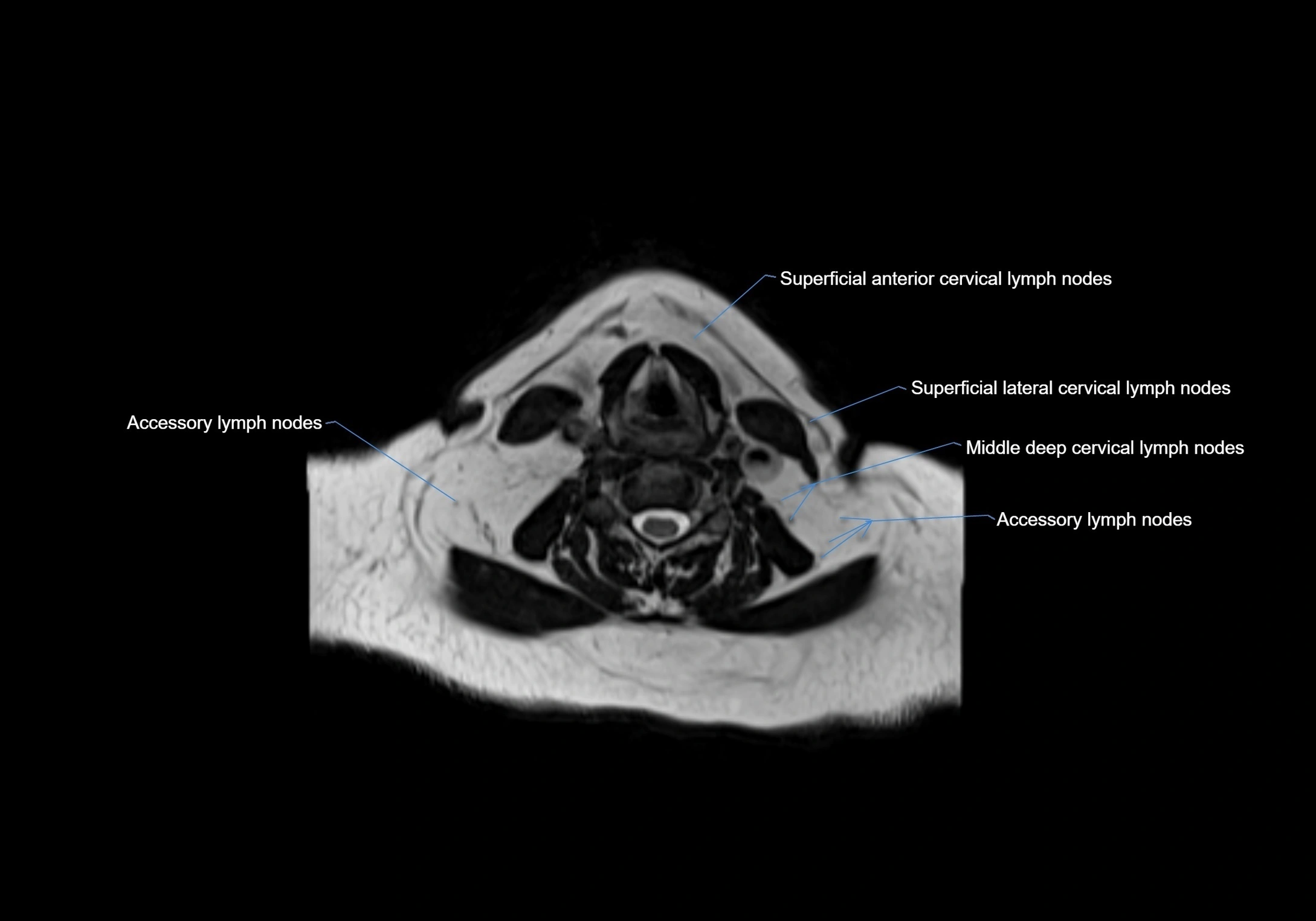
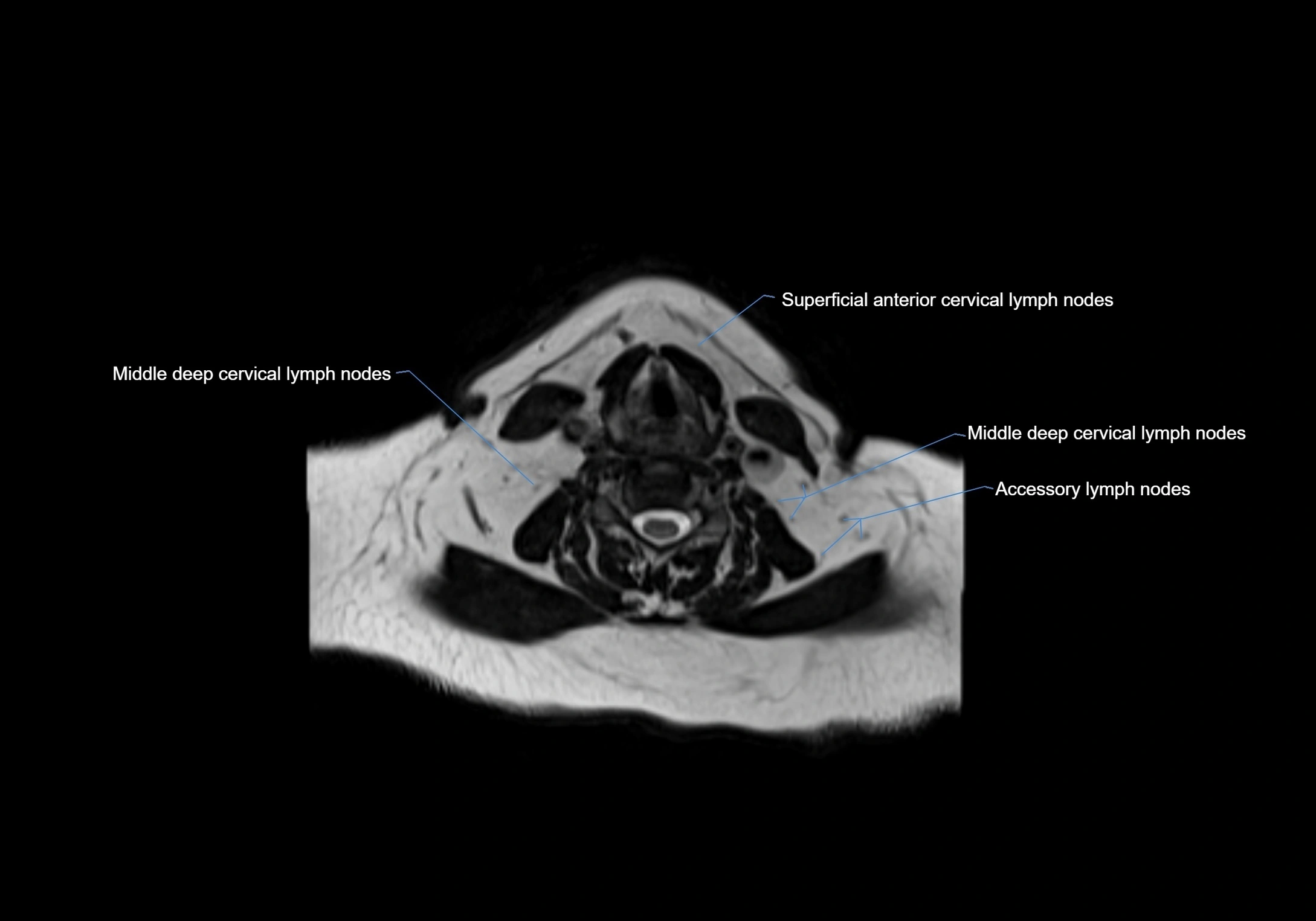
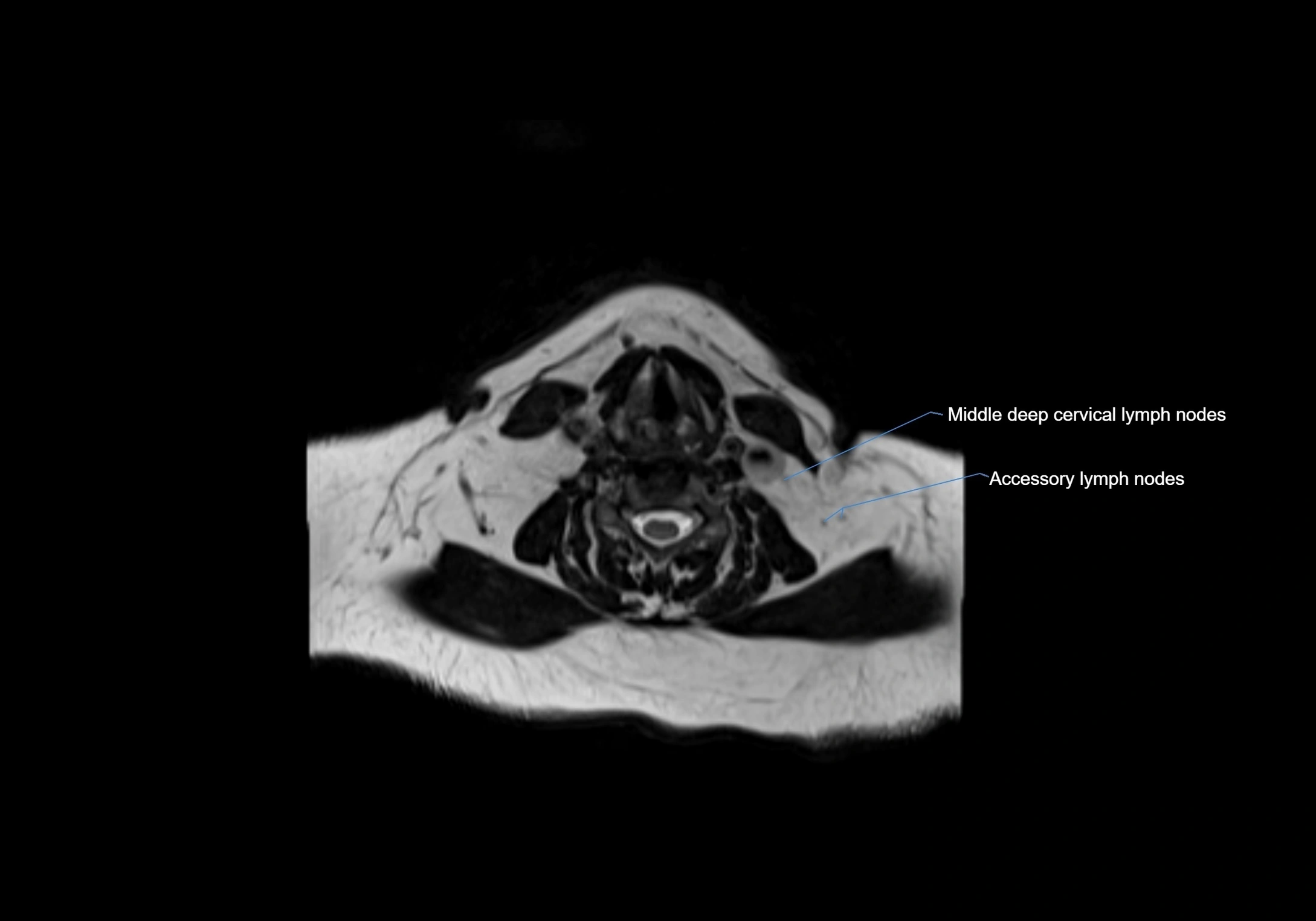
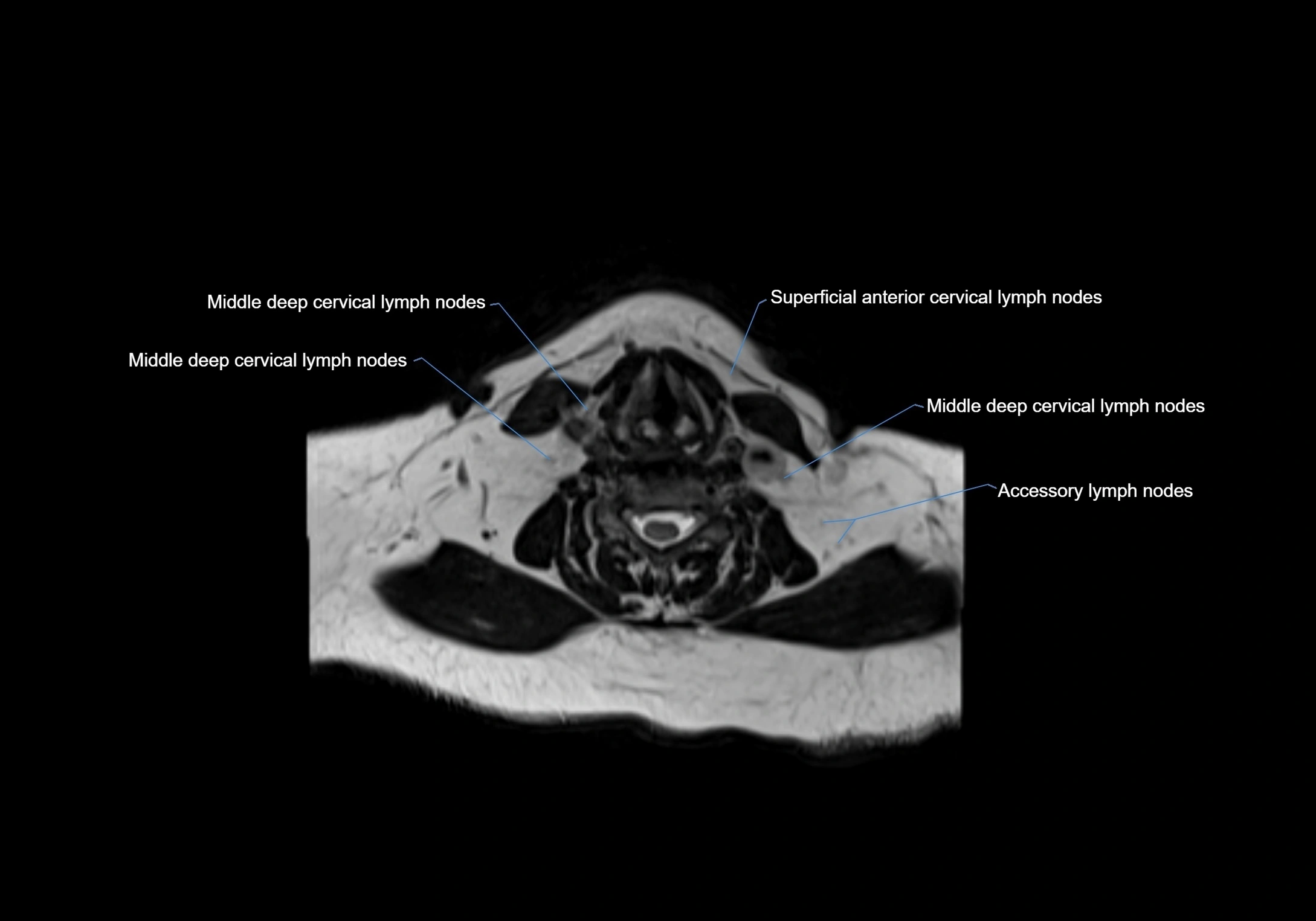
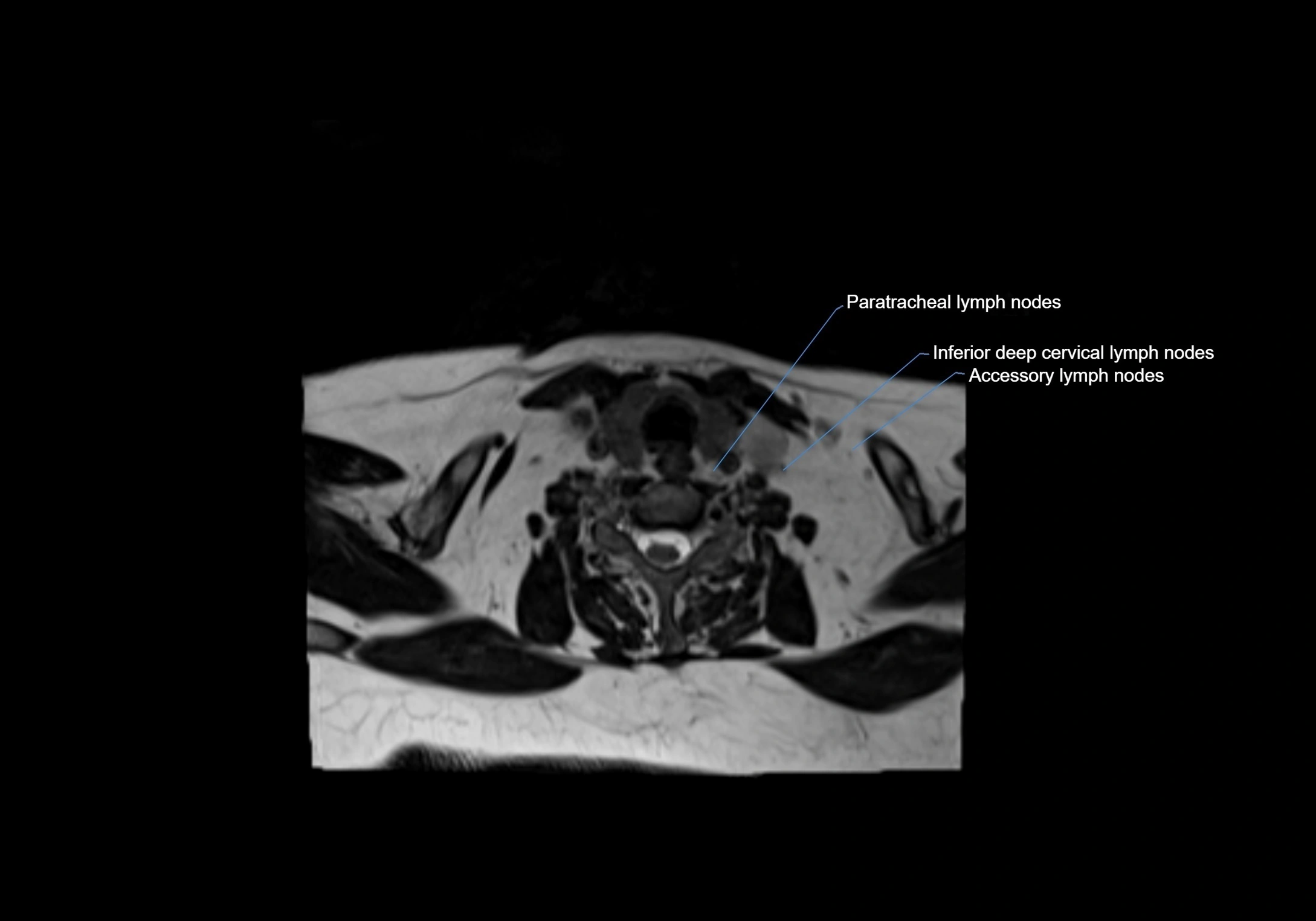
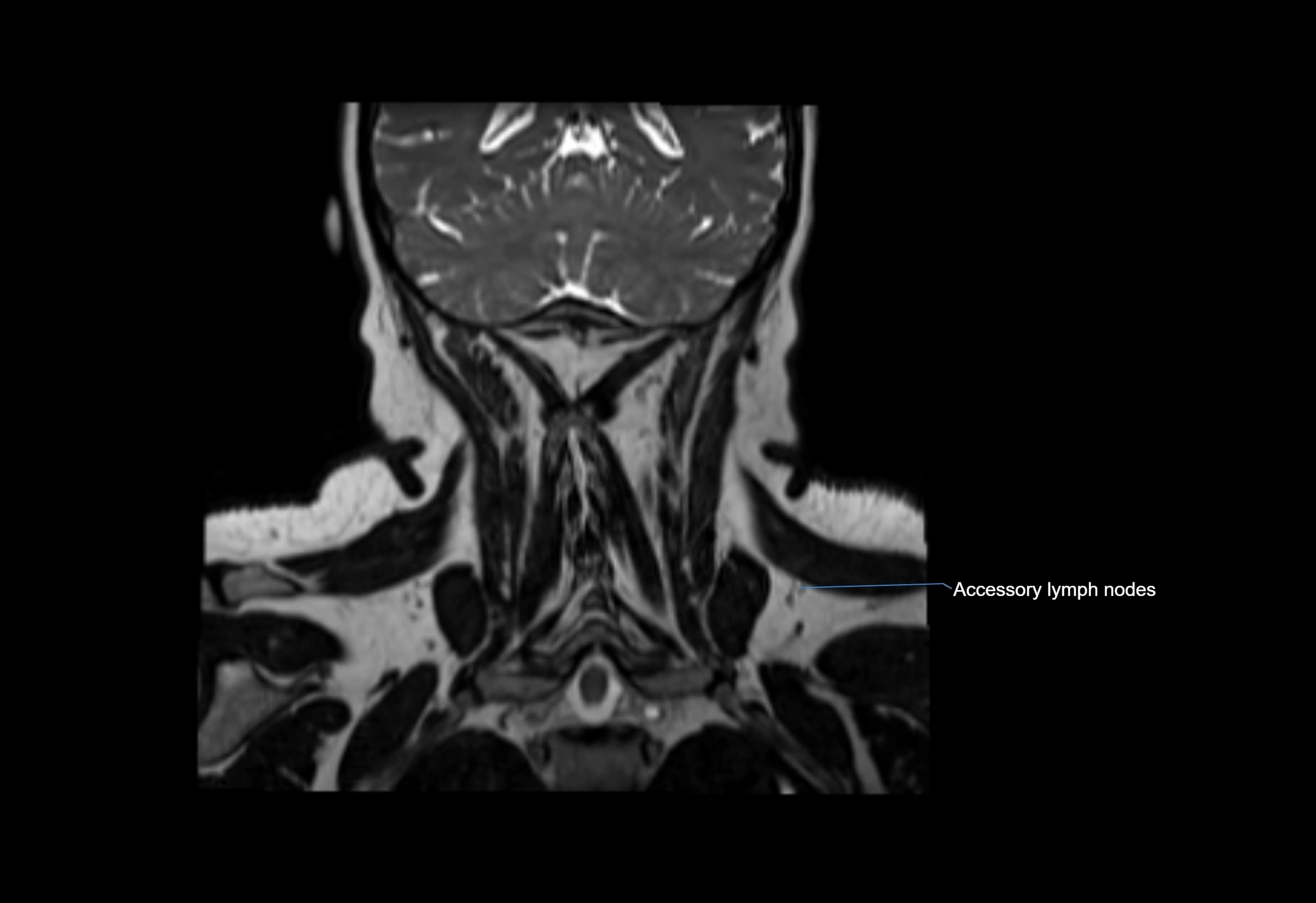
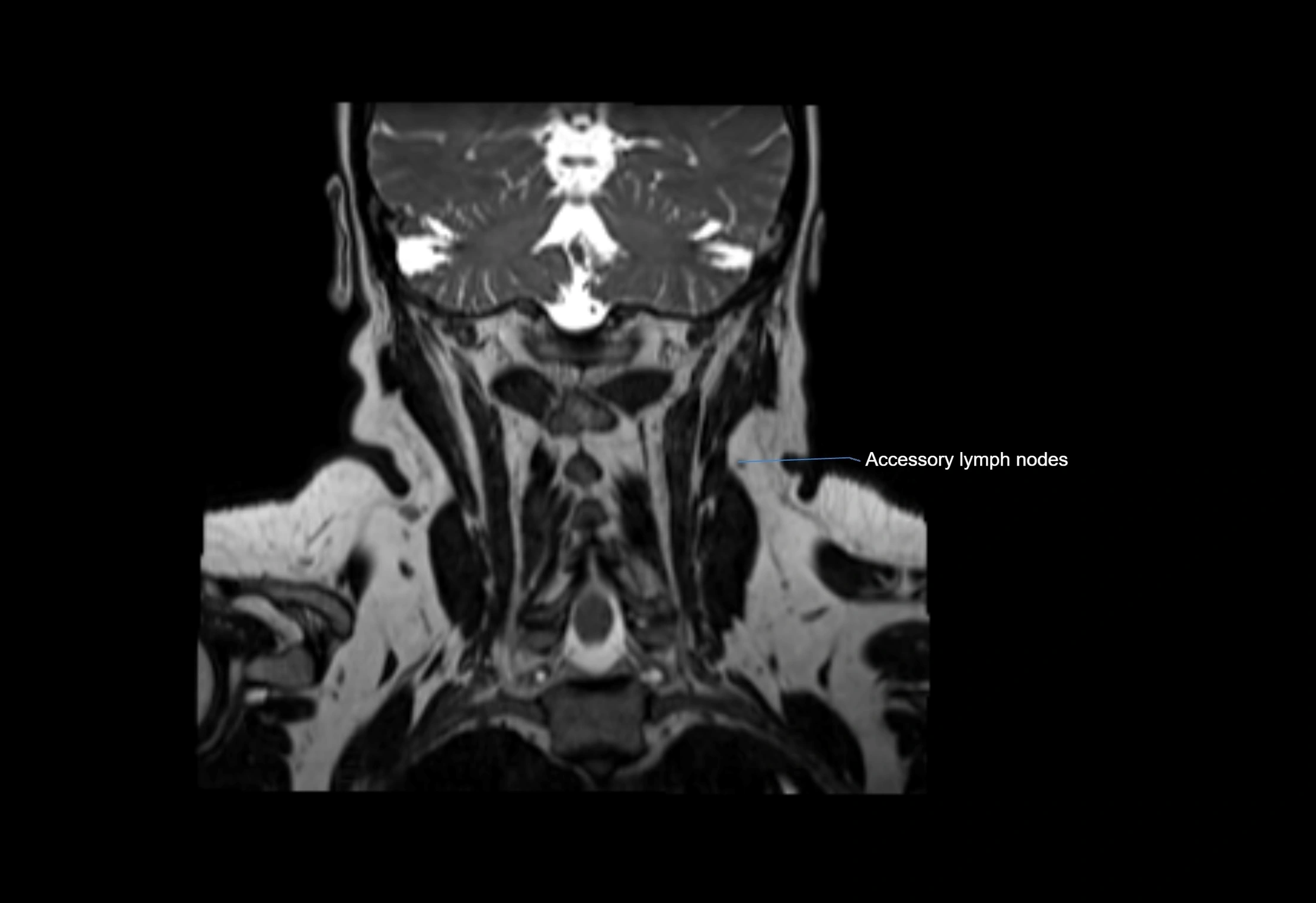
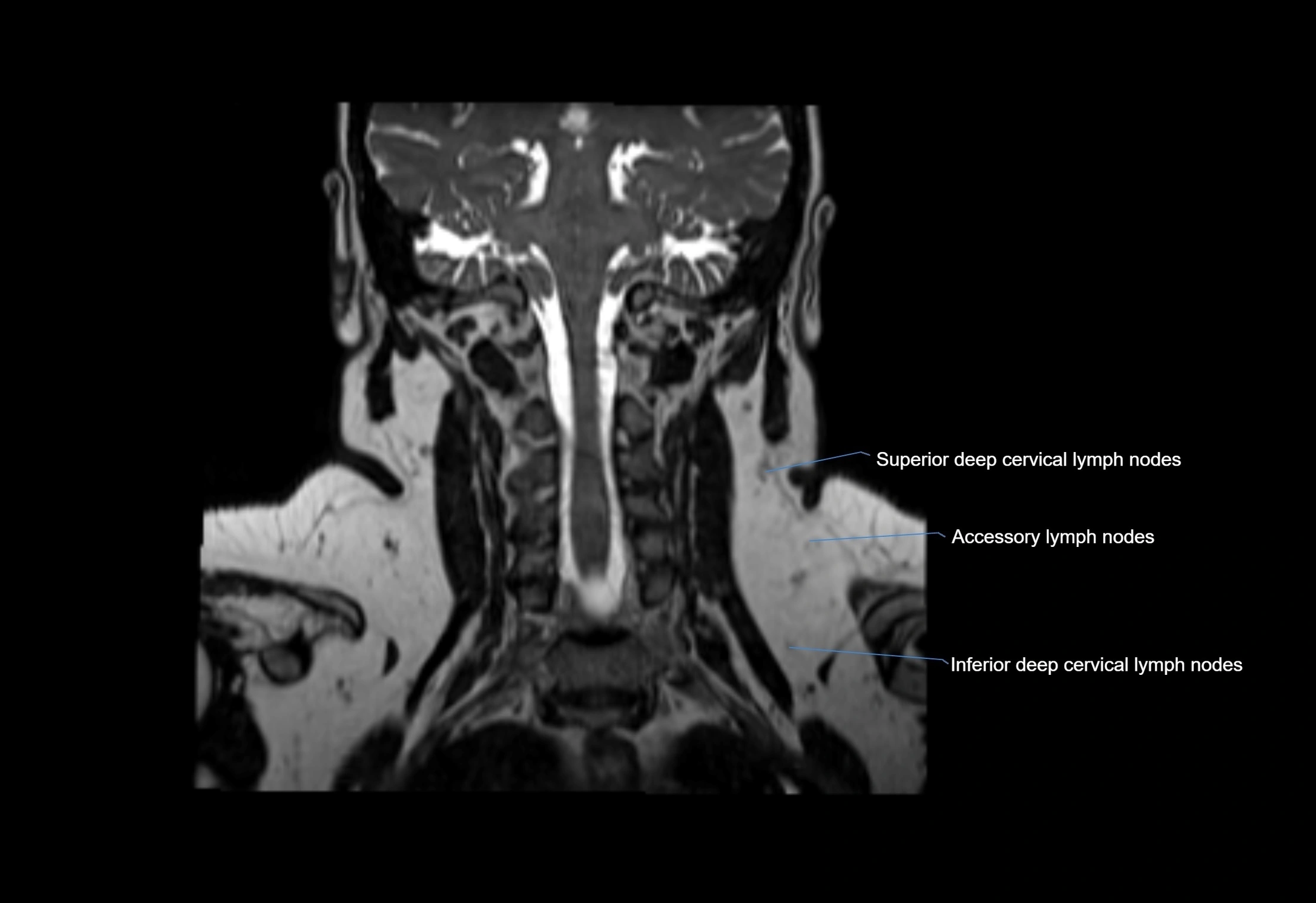
Accessory lymph nodes are small, secondary lymph nodes located along the main facial and cervical lymphatic chains, often adjacent to primary lymph nodes, such as preauricular, submandibular, or occipital nodes. They are typically less than 5 mm in diameter, embedded within subcutaneous fat or connective tissue, and may be variable in number and location. These nodes provide additional filtration and immune surveillance for lymph collected from the face, scalp, and neck regions. Accessory lymph nodes are usually non-palpable in healthy individuals but may enlarge in response to infection, inflammation, or metastasis, making them clinically significant.
Synonyms
-
Secondary facial lymph nodes
-
Collateral lymph nodes
-
Supernumerary lymph nodes
Function
-
Filter lymph from regions served by primary facial or cervical lymph nodes
-
Assist in immune surveillance, trapping pathogens and foreign particles
-
Provide redundant drainage pathways for facial and cervical lymphatics
-
Serve as early indicators of infection, inflammation, or metastatic spread
Location
-
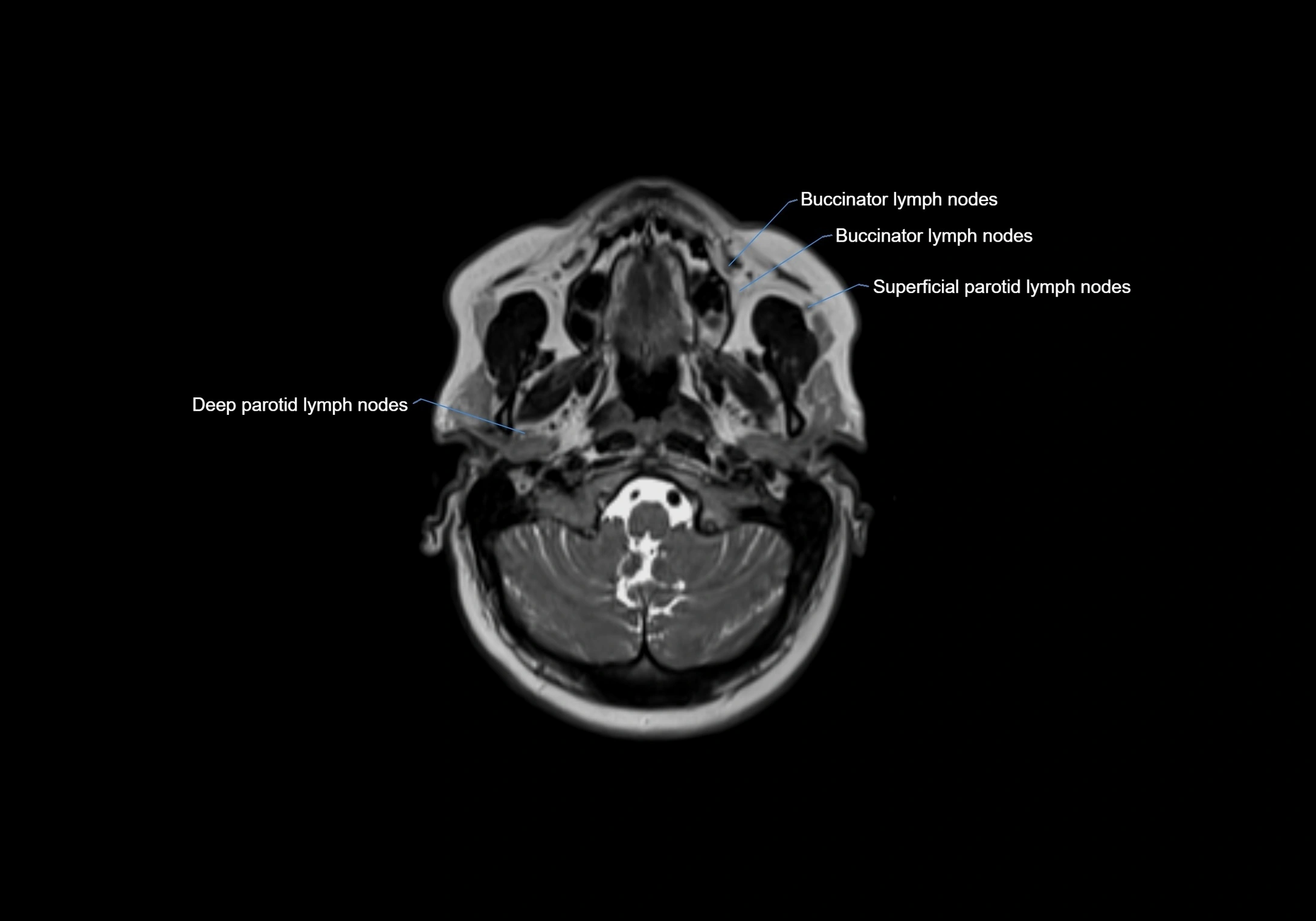
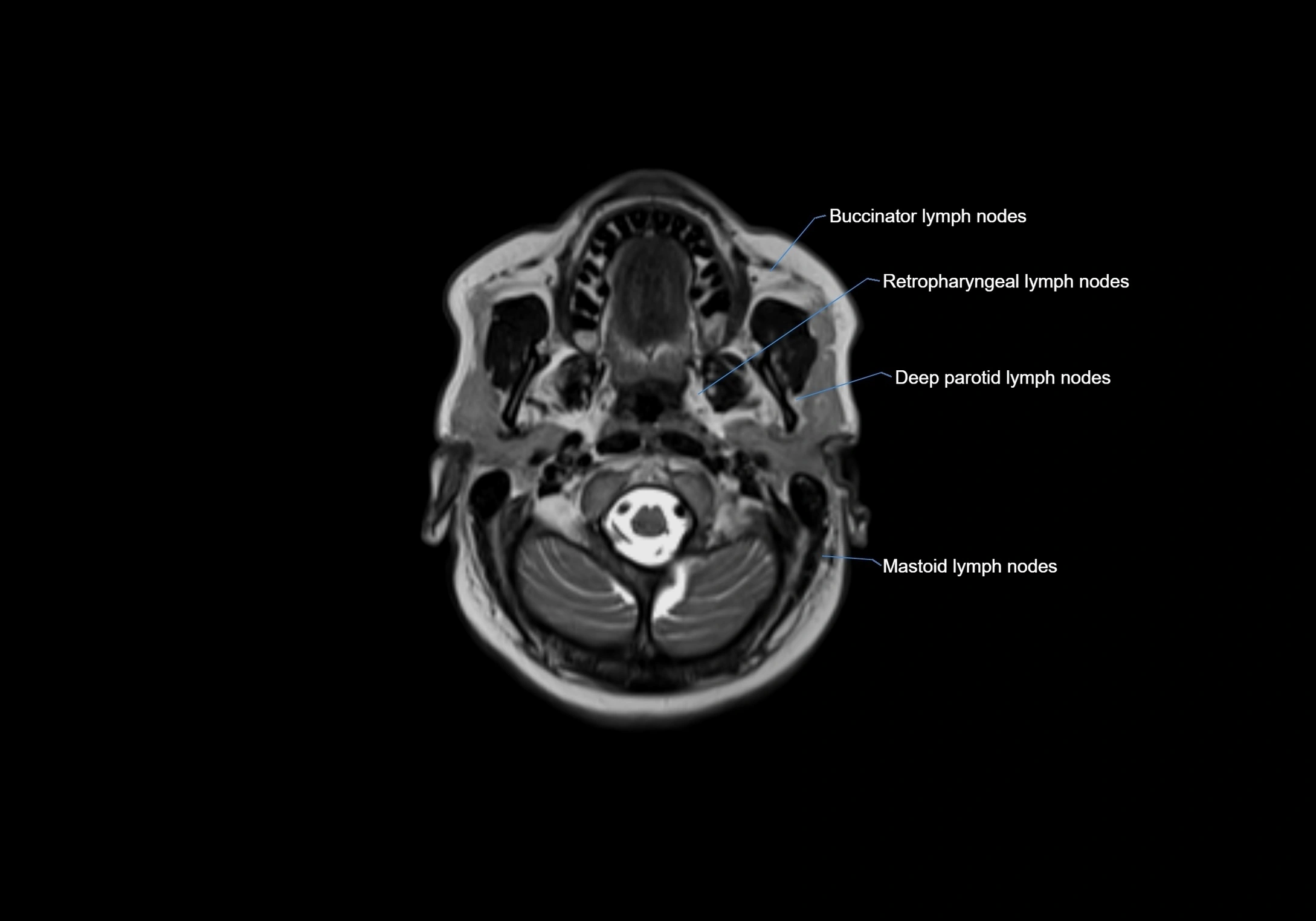
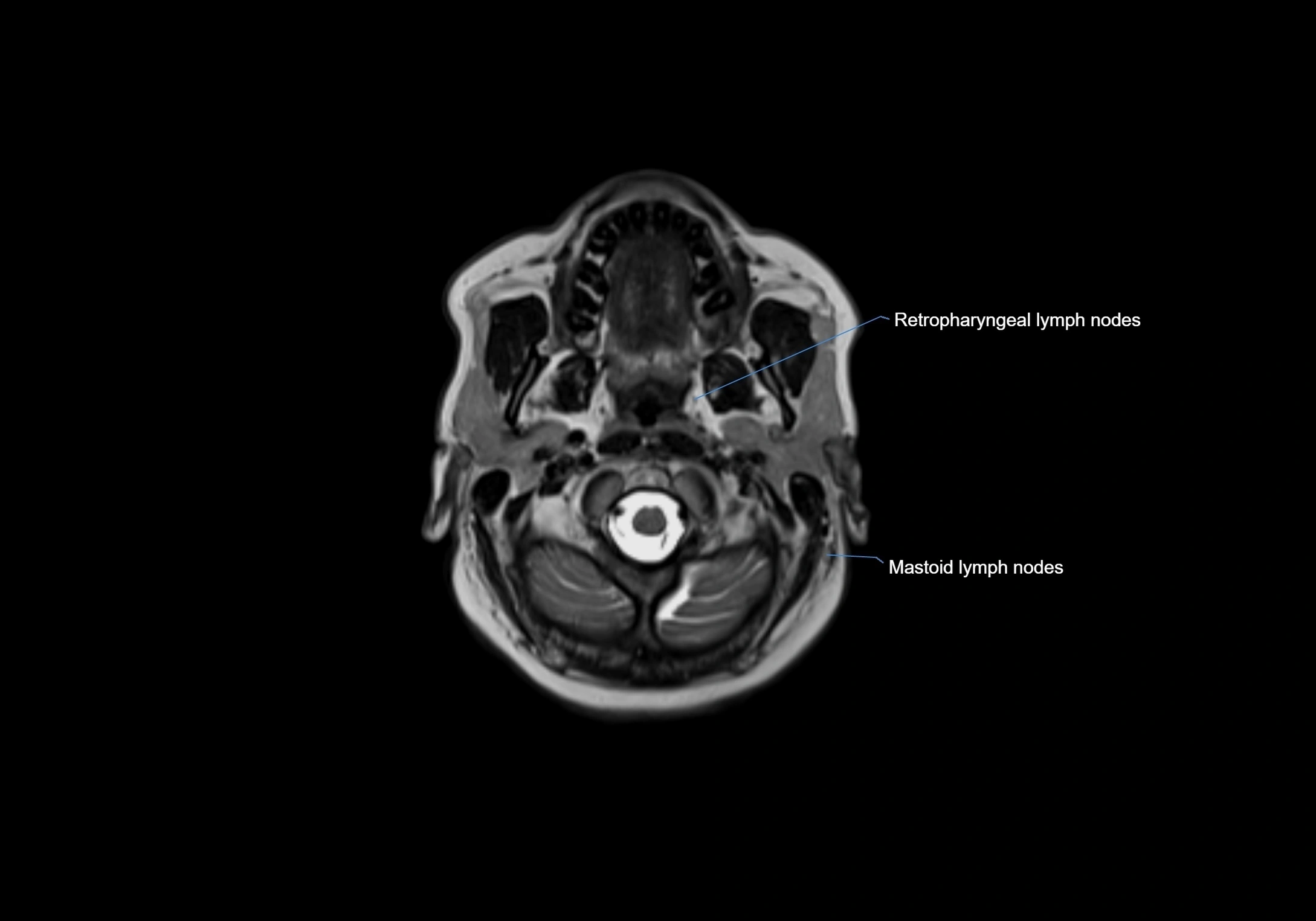
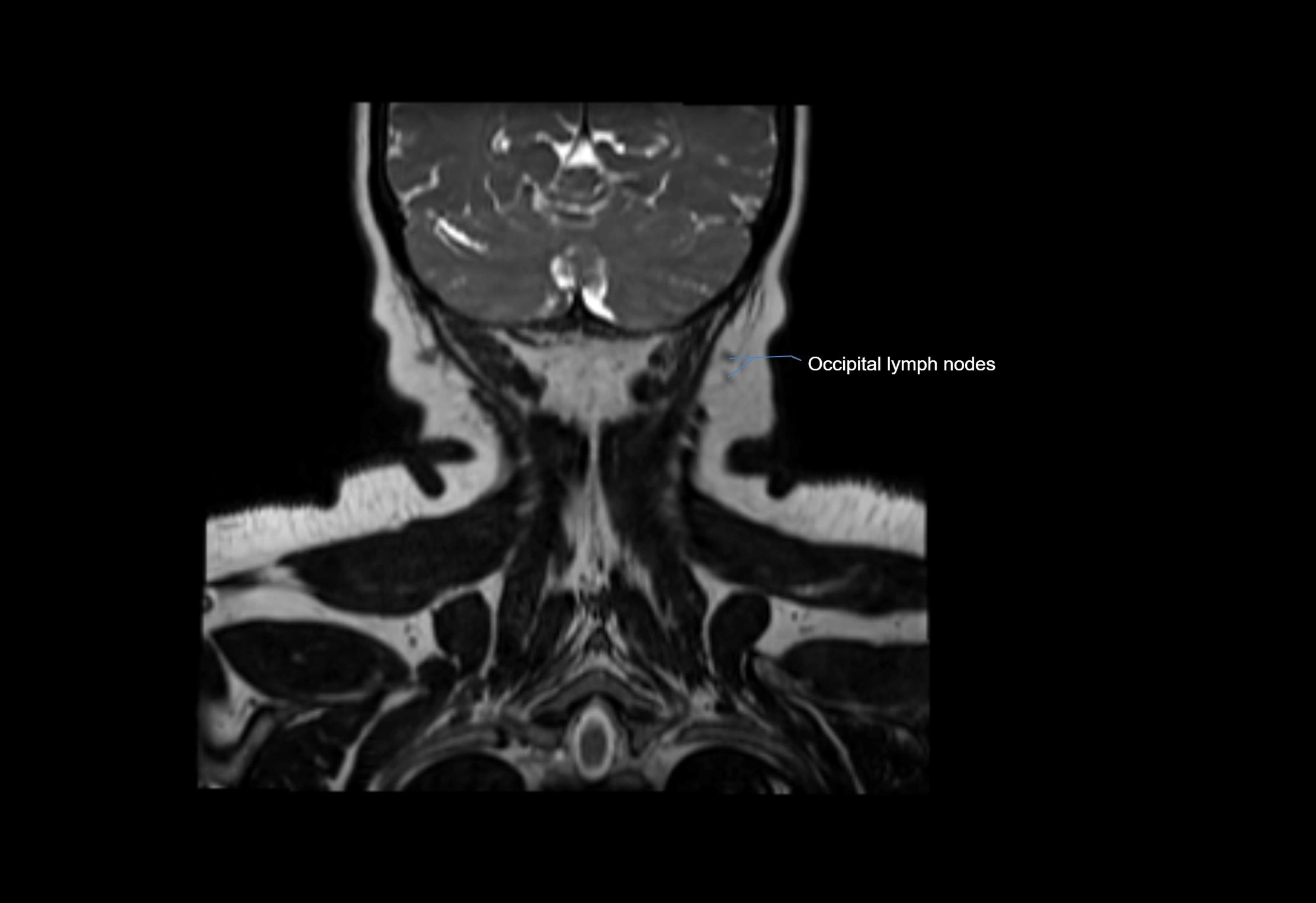
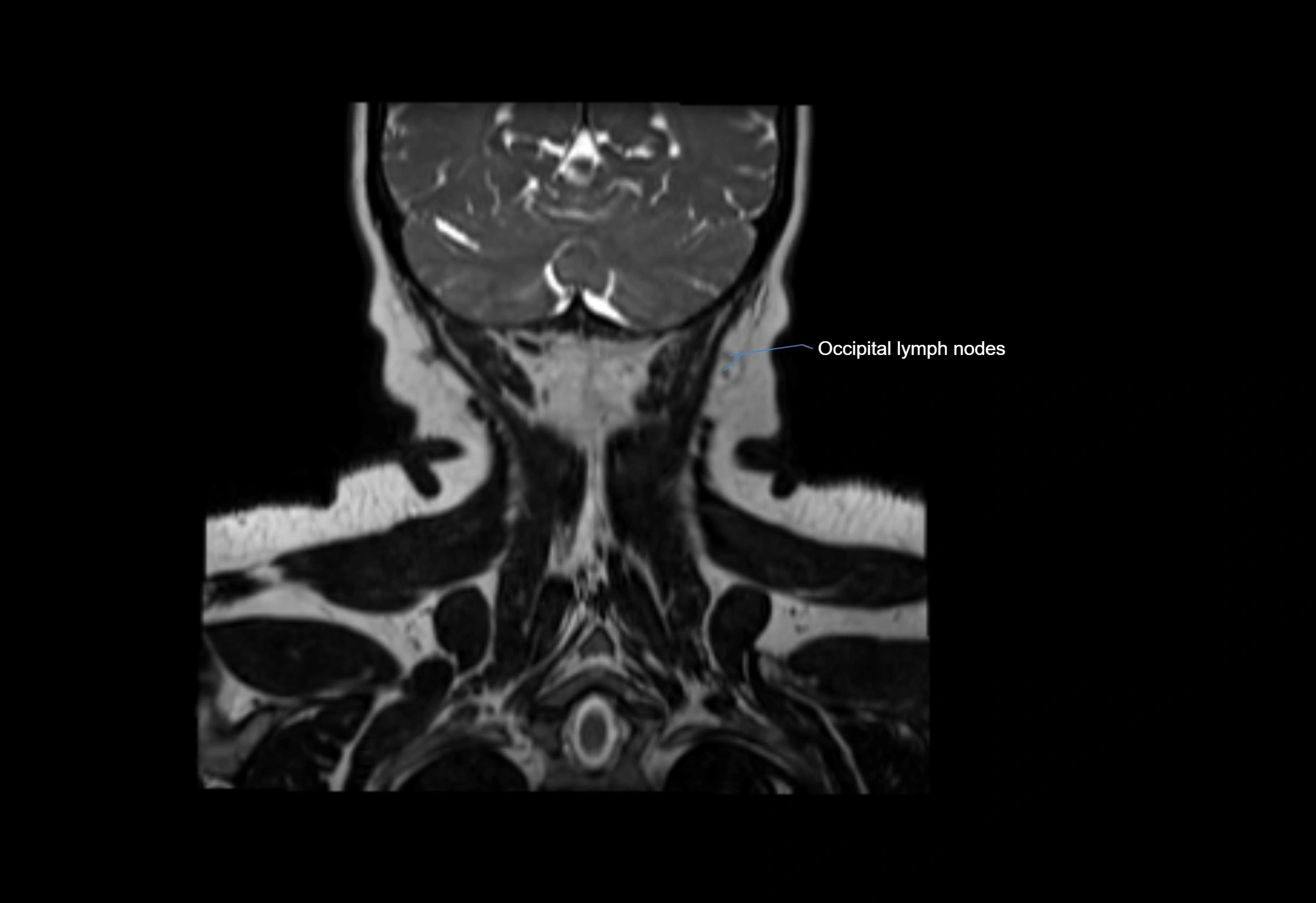
Found along primary lymph node chains, including preauricular, submandibular, parotid, and occipital regions
-
Embedded in subcutaneous fat or superficial fascia, often lateral or posterior to primary nodes
-
Variable in number; may occur unilaterally or bilaterally, depending on individual anatomy
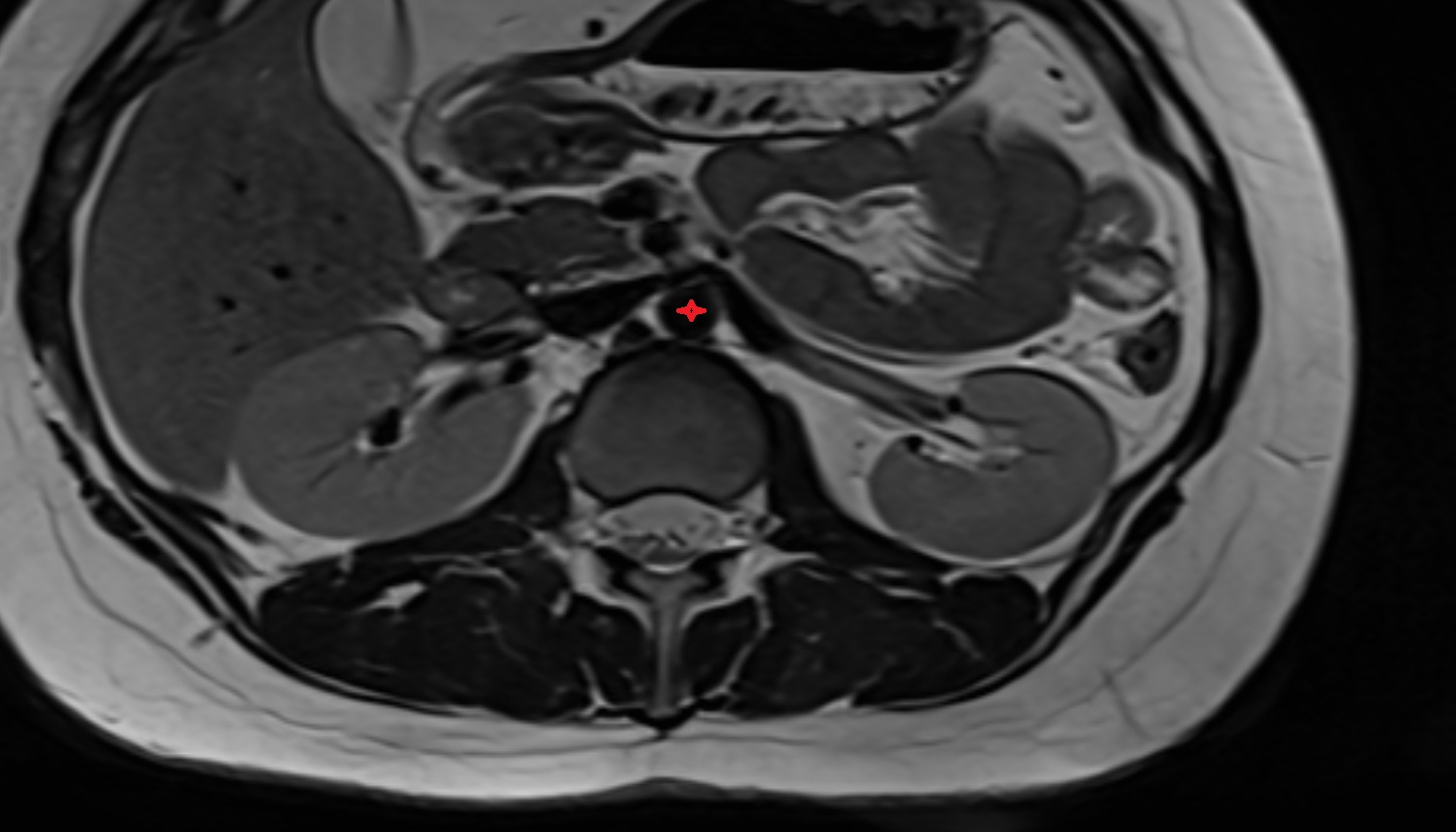
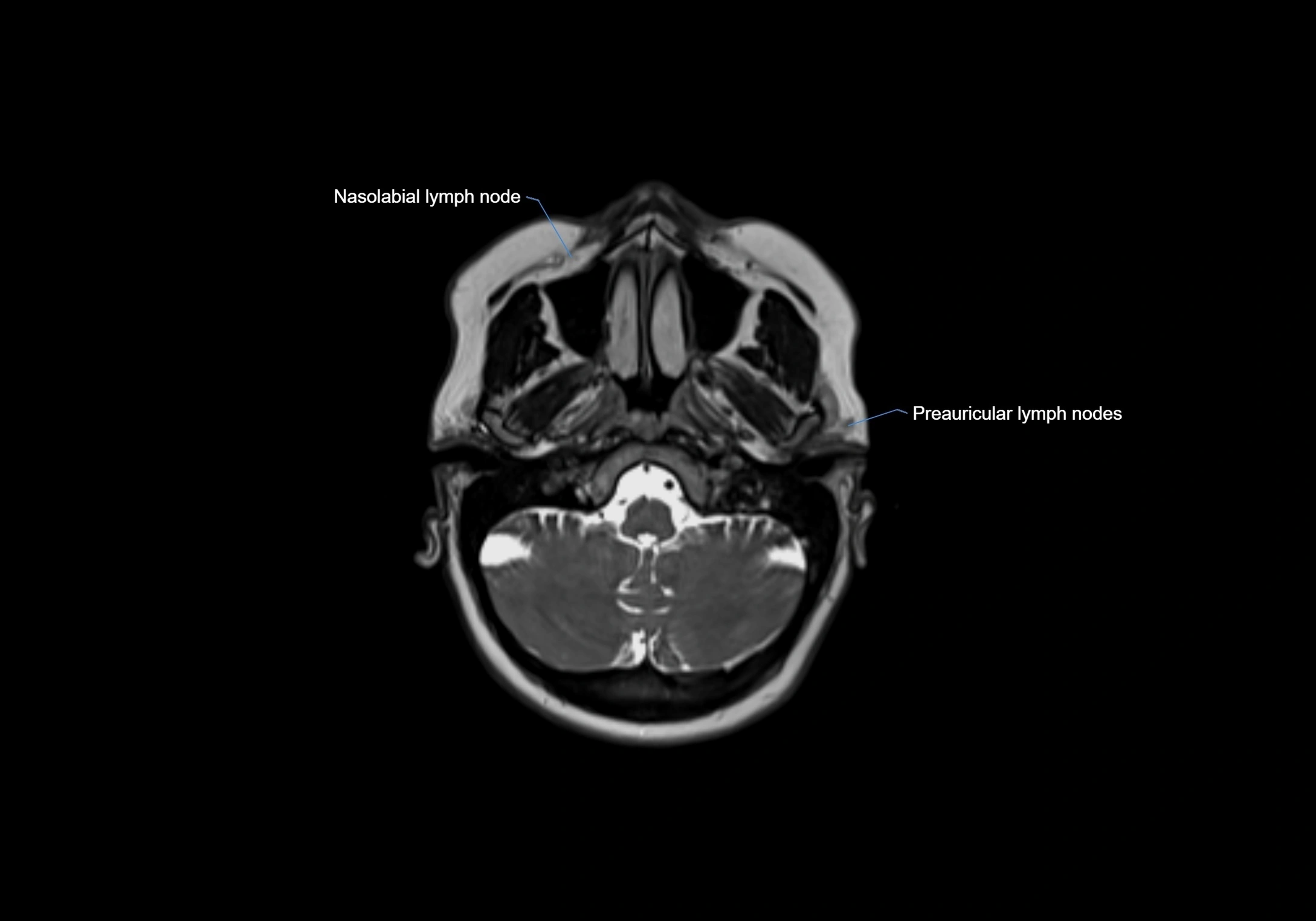
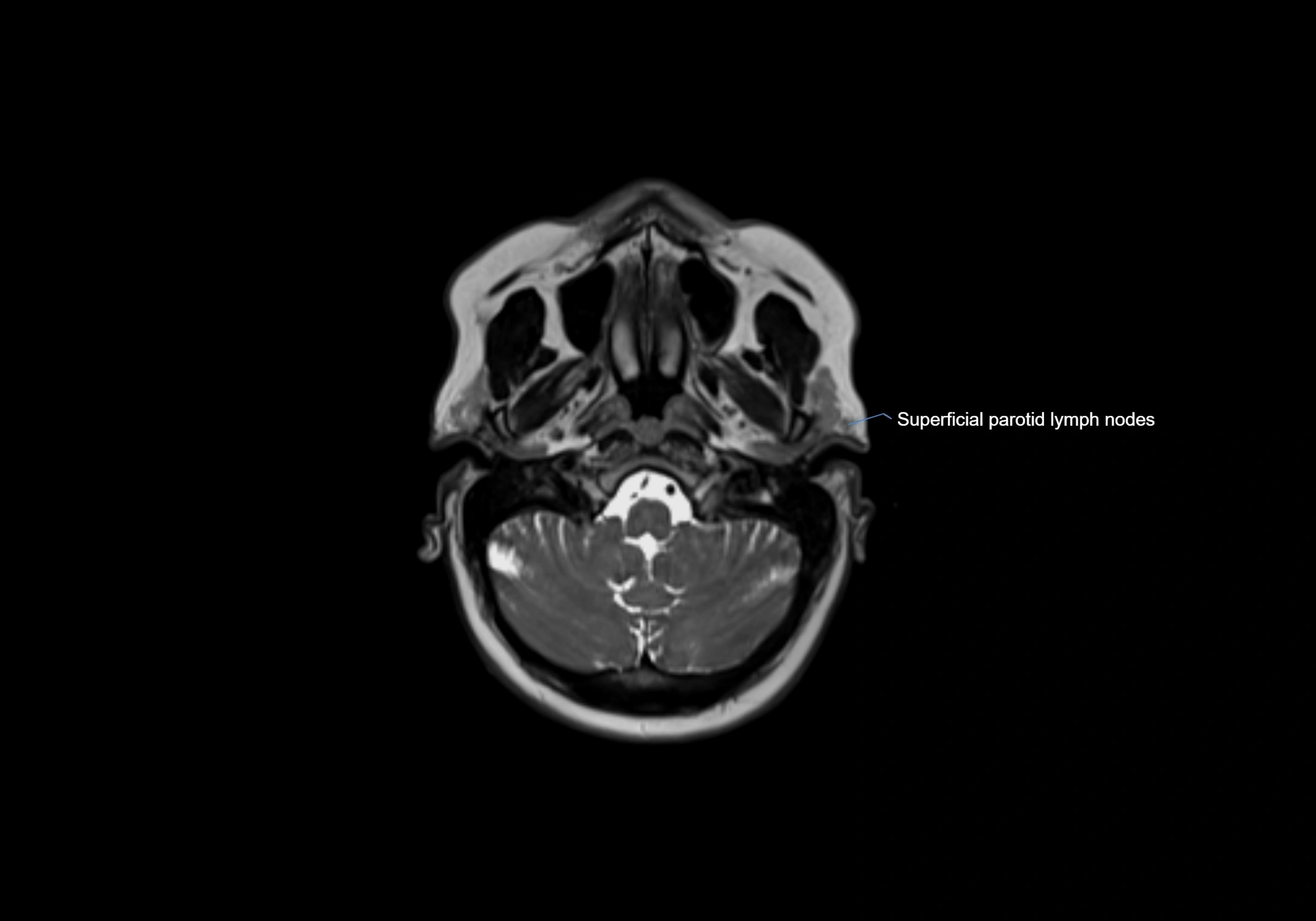
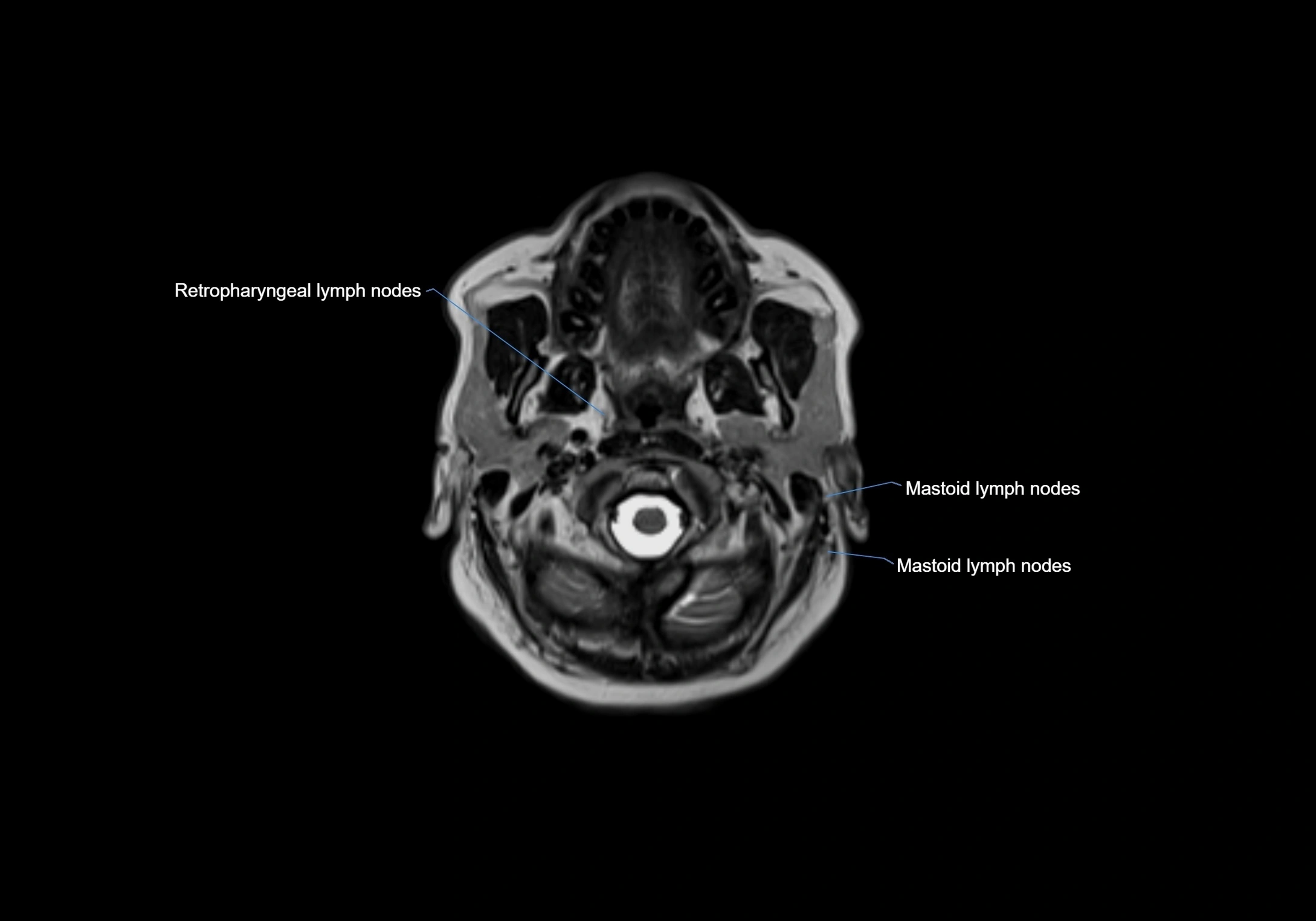
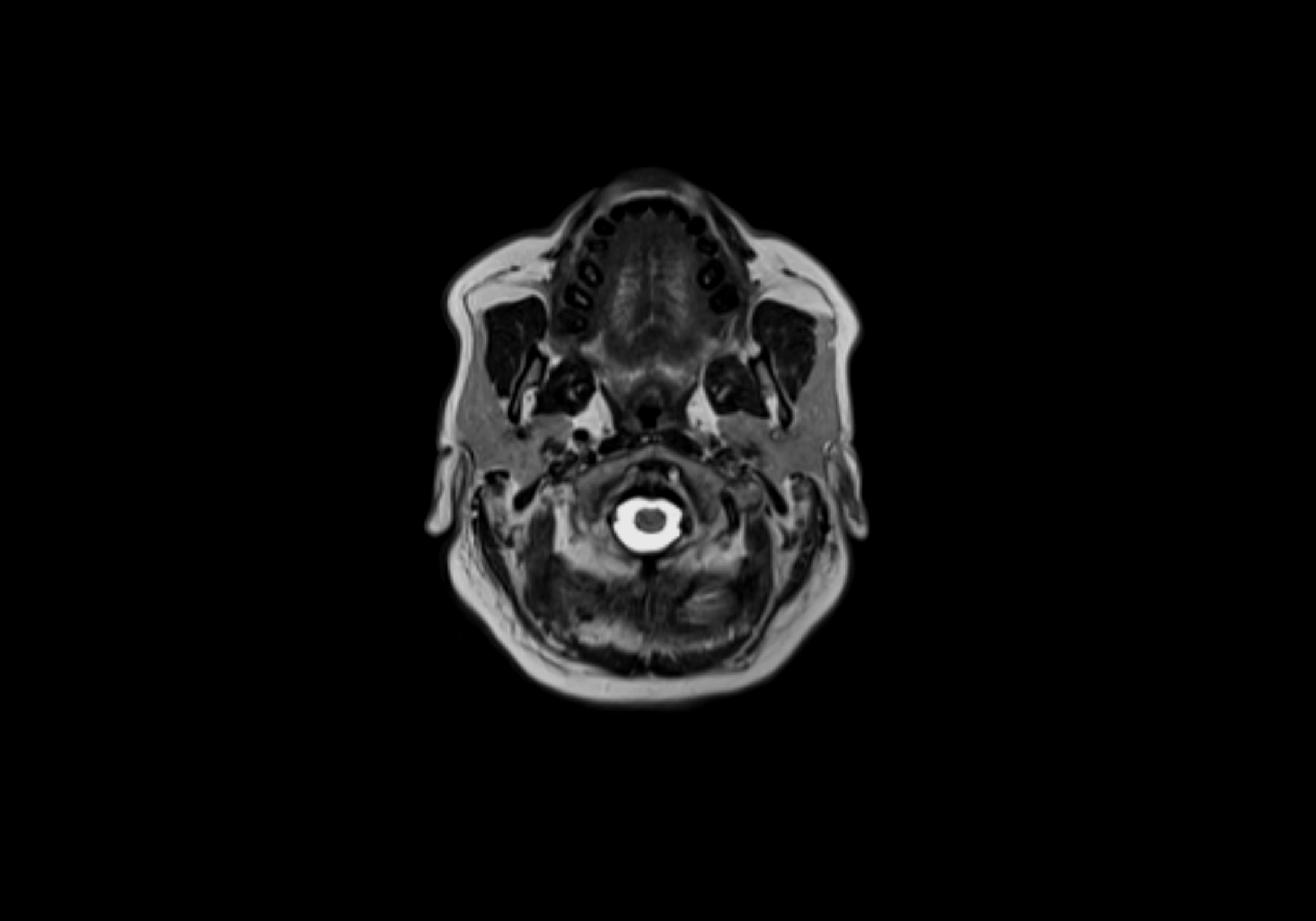
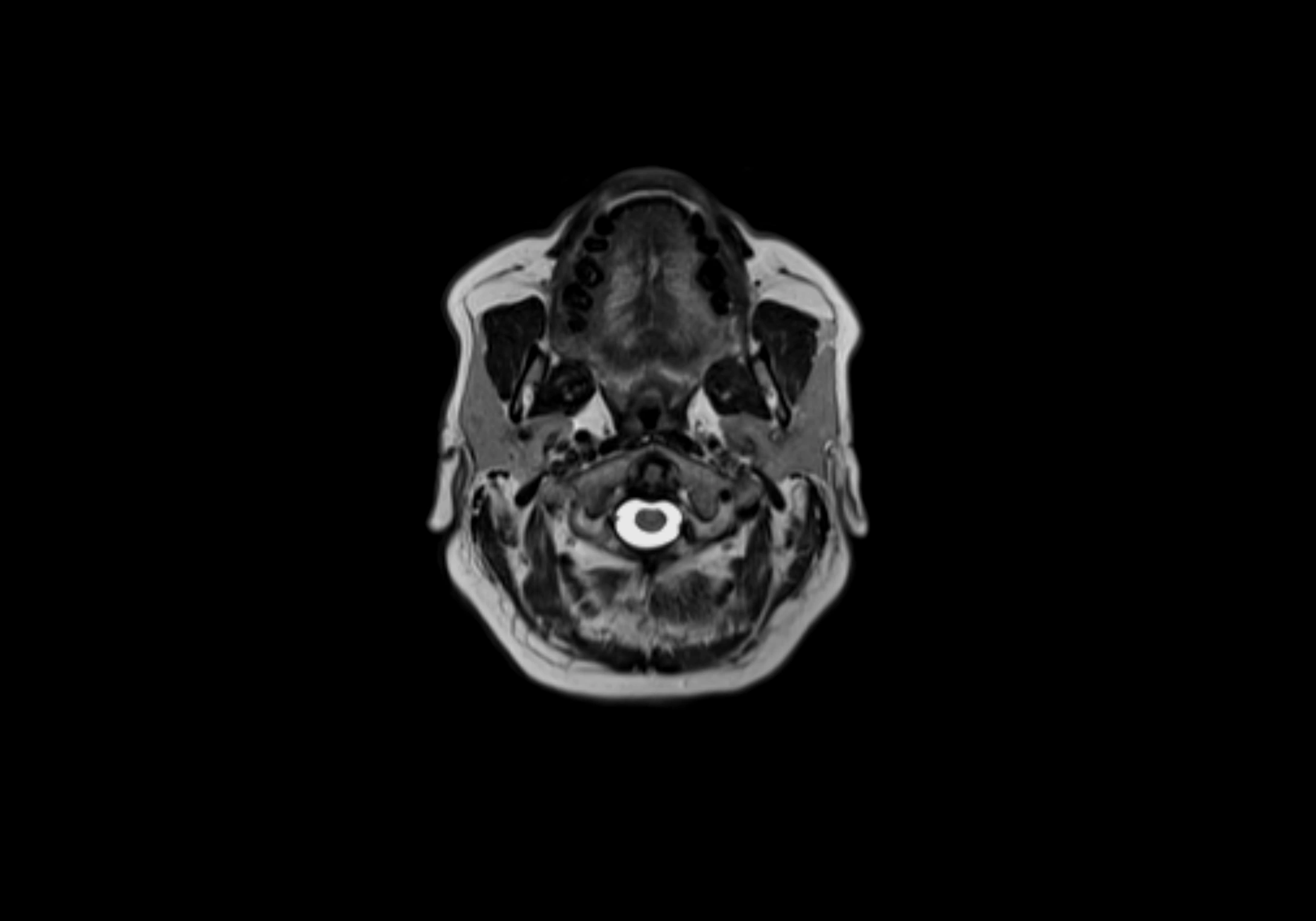
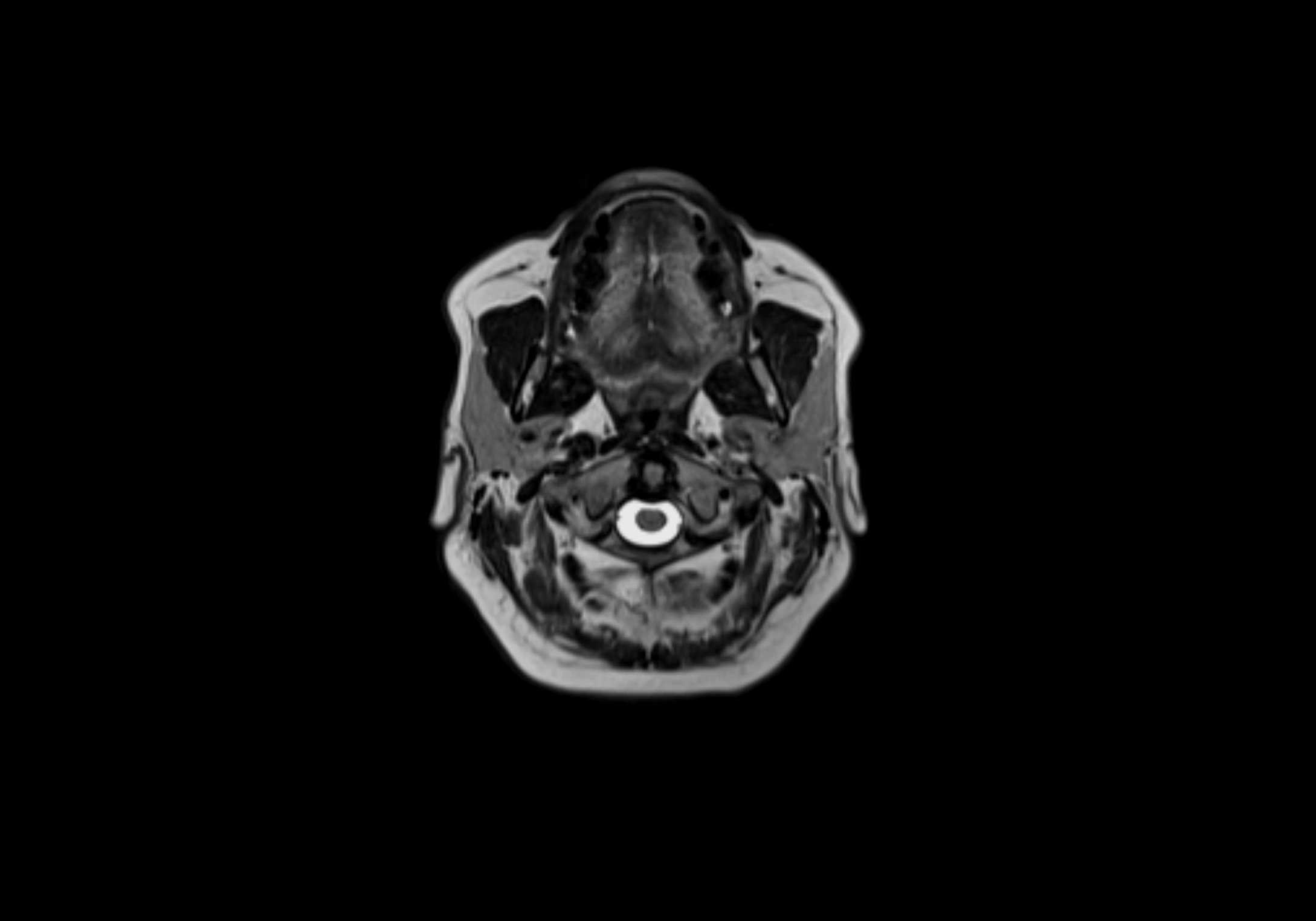
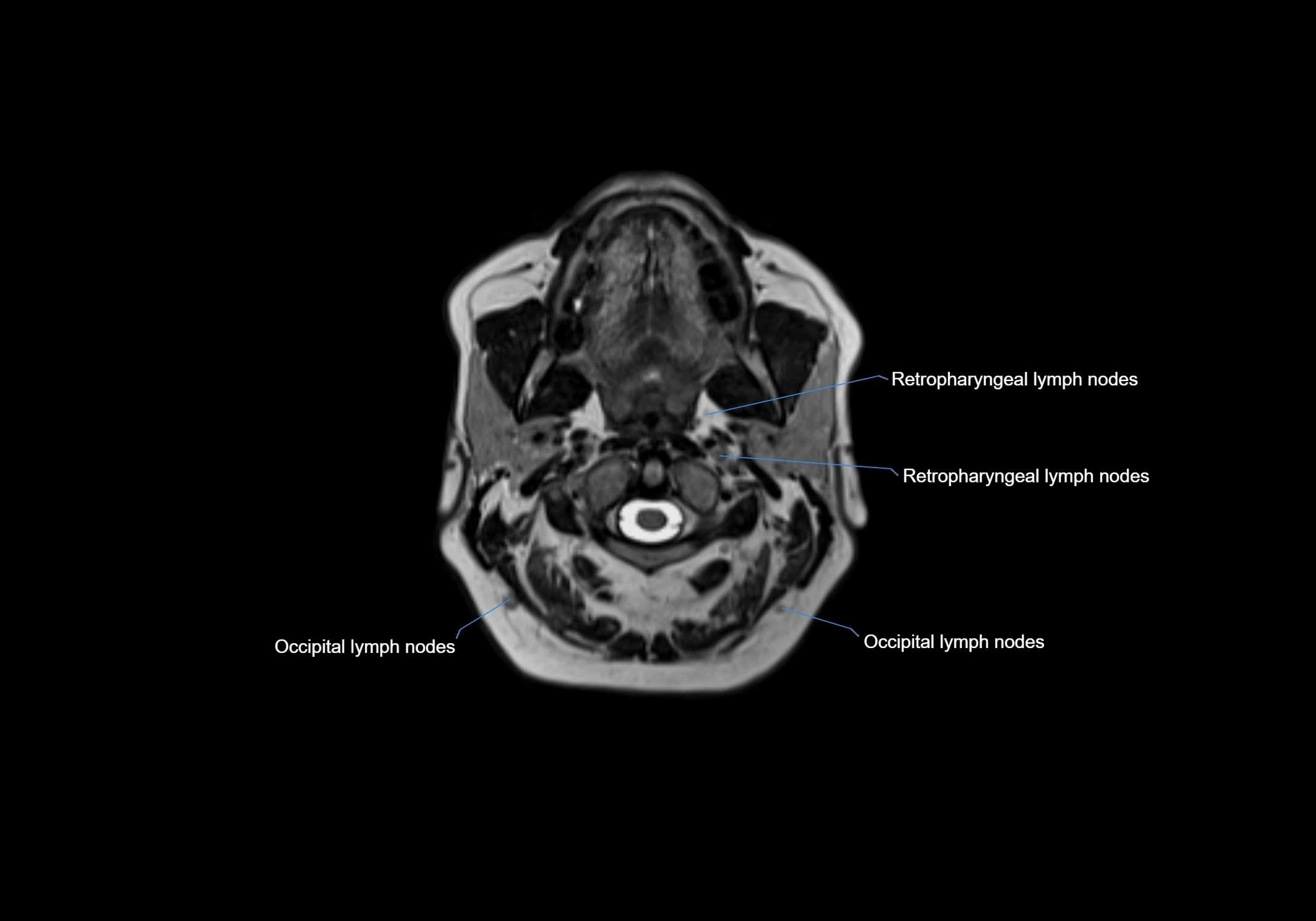
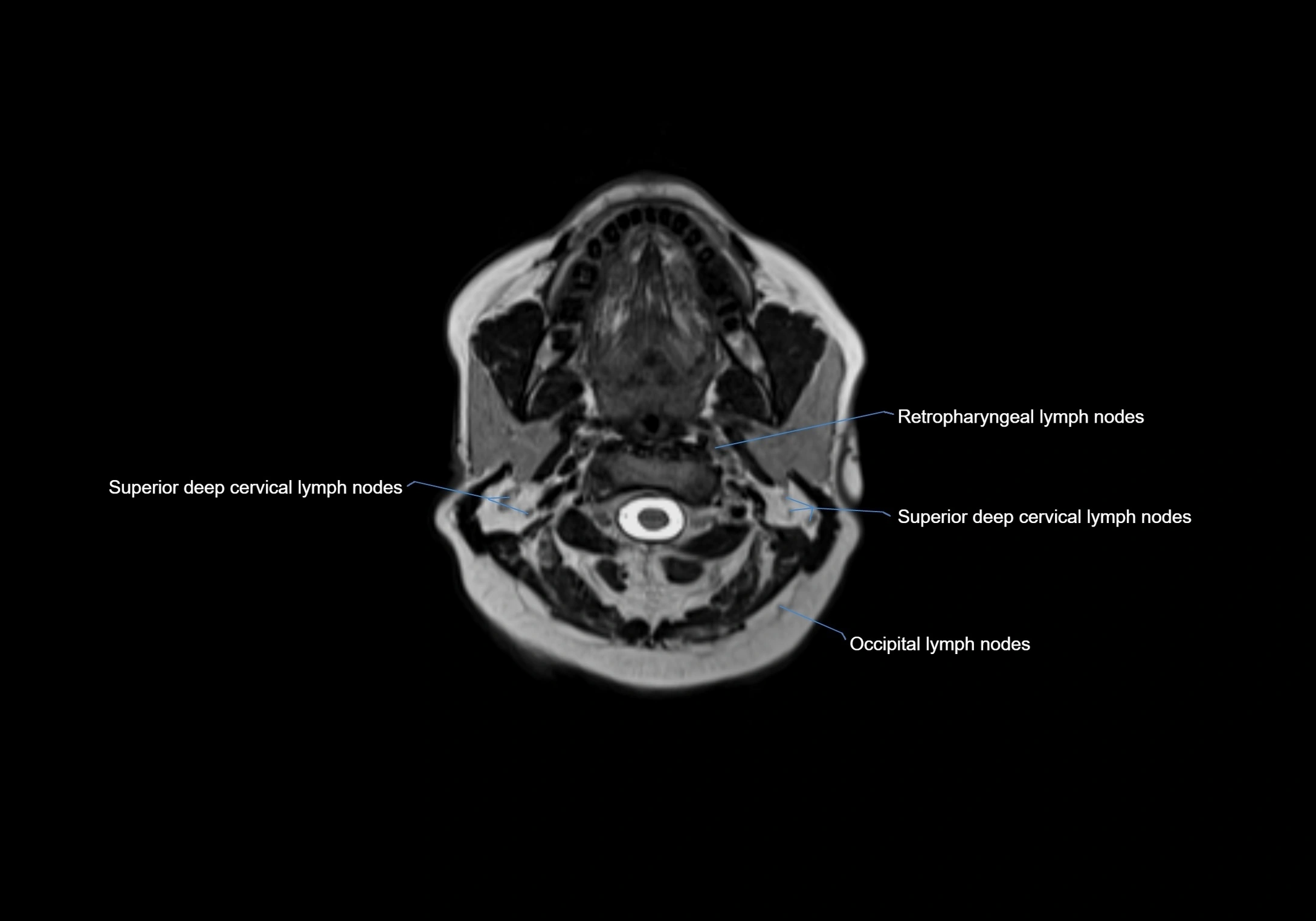
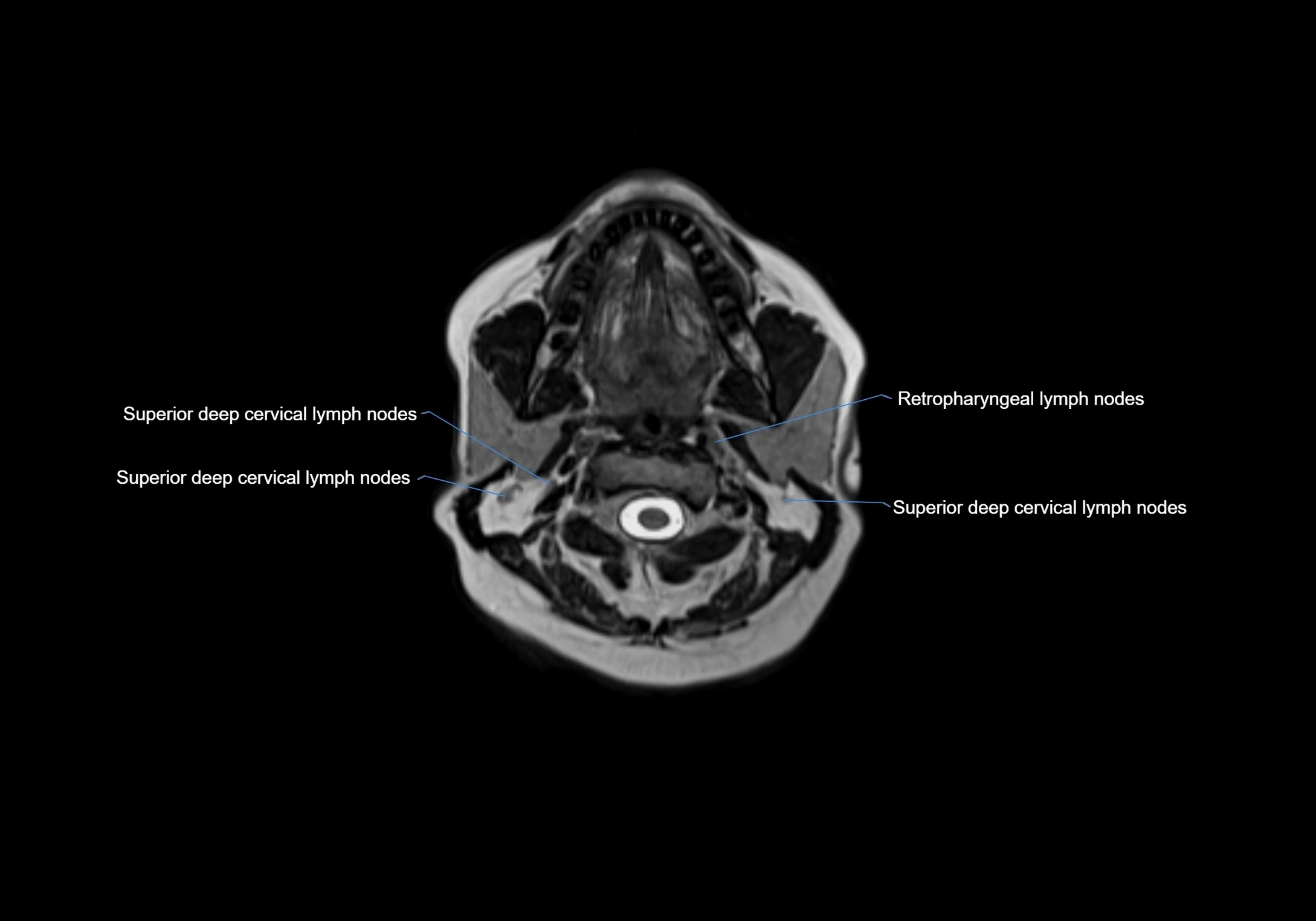
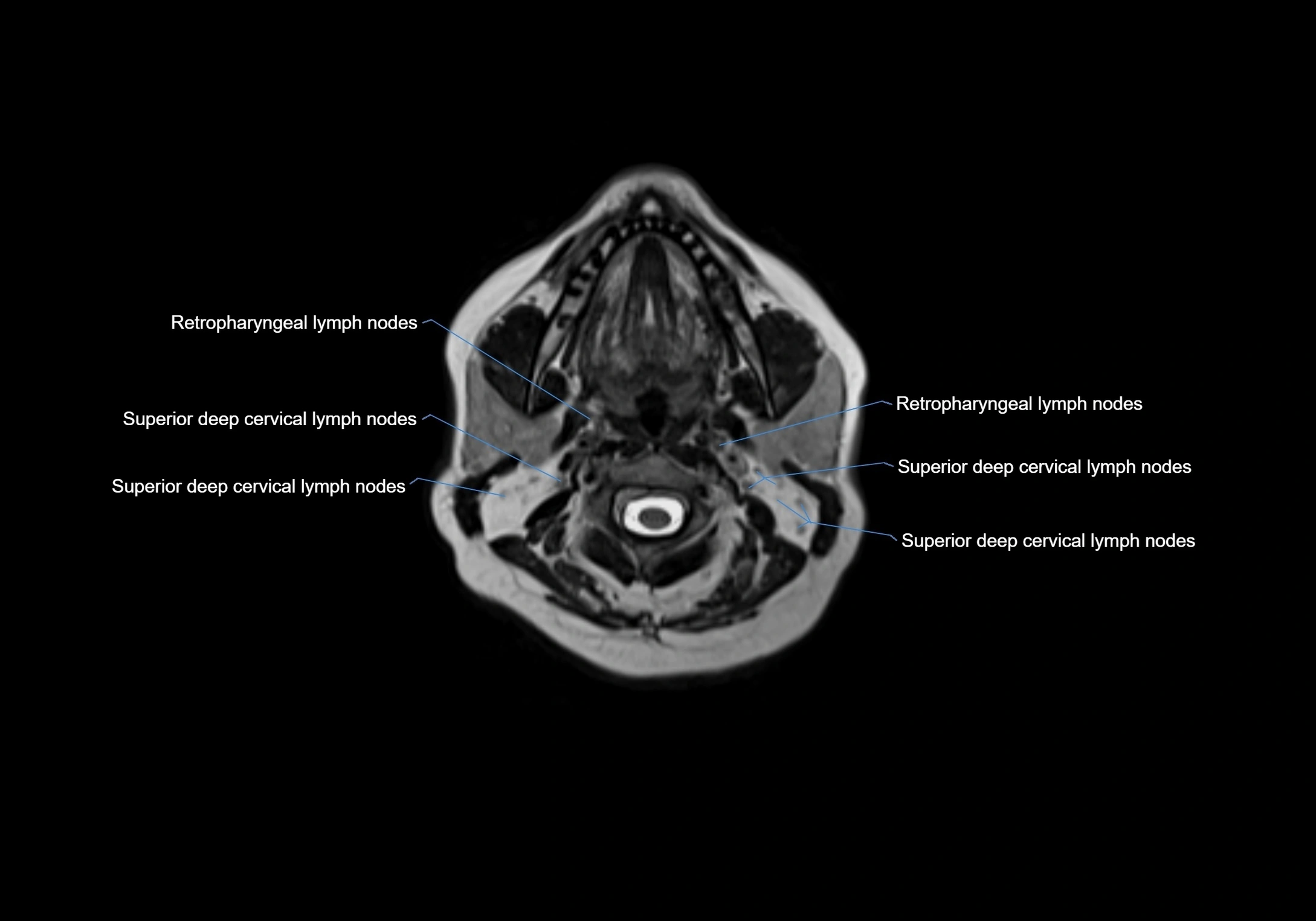
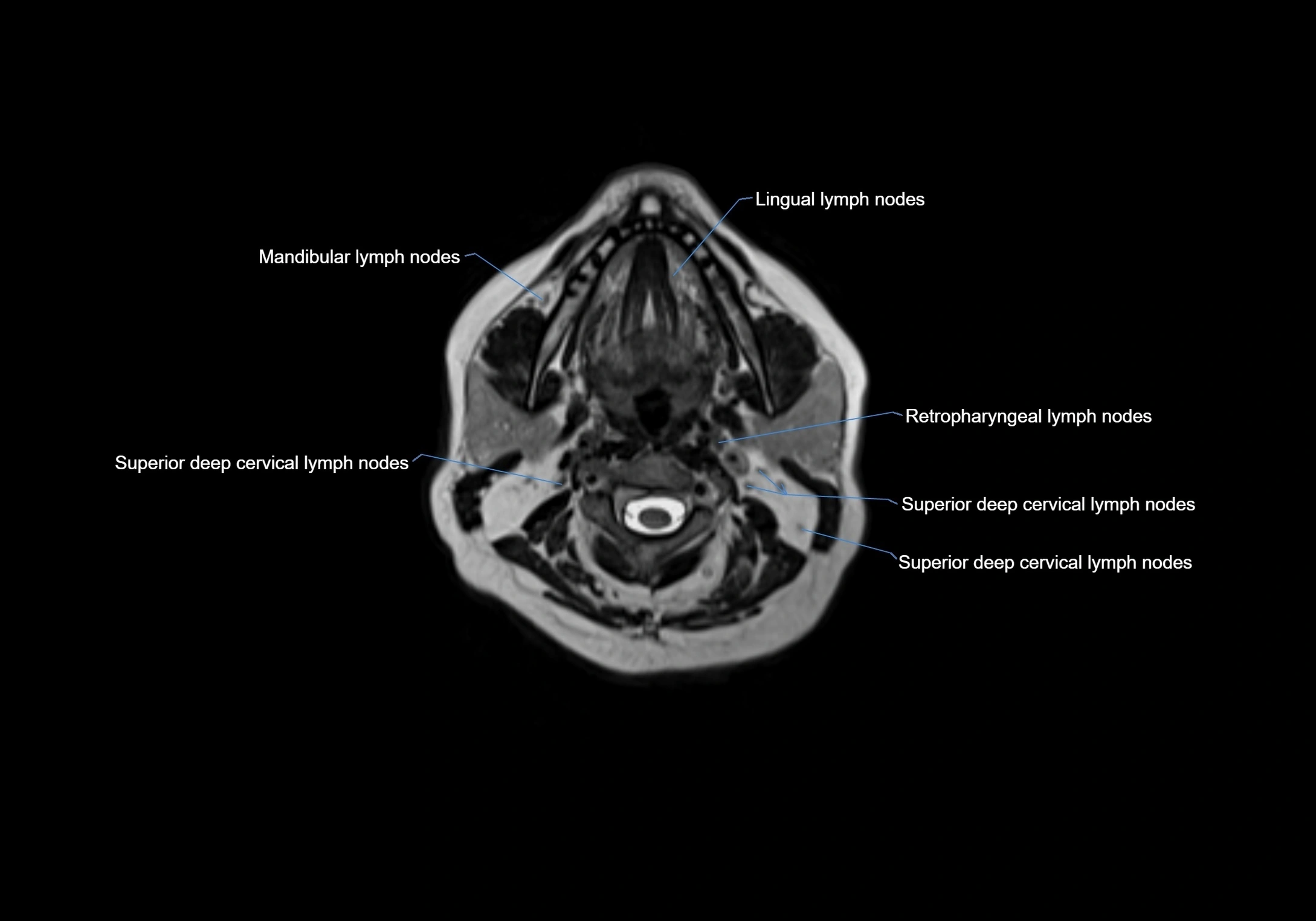
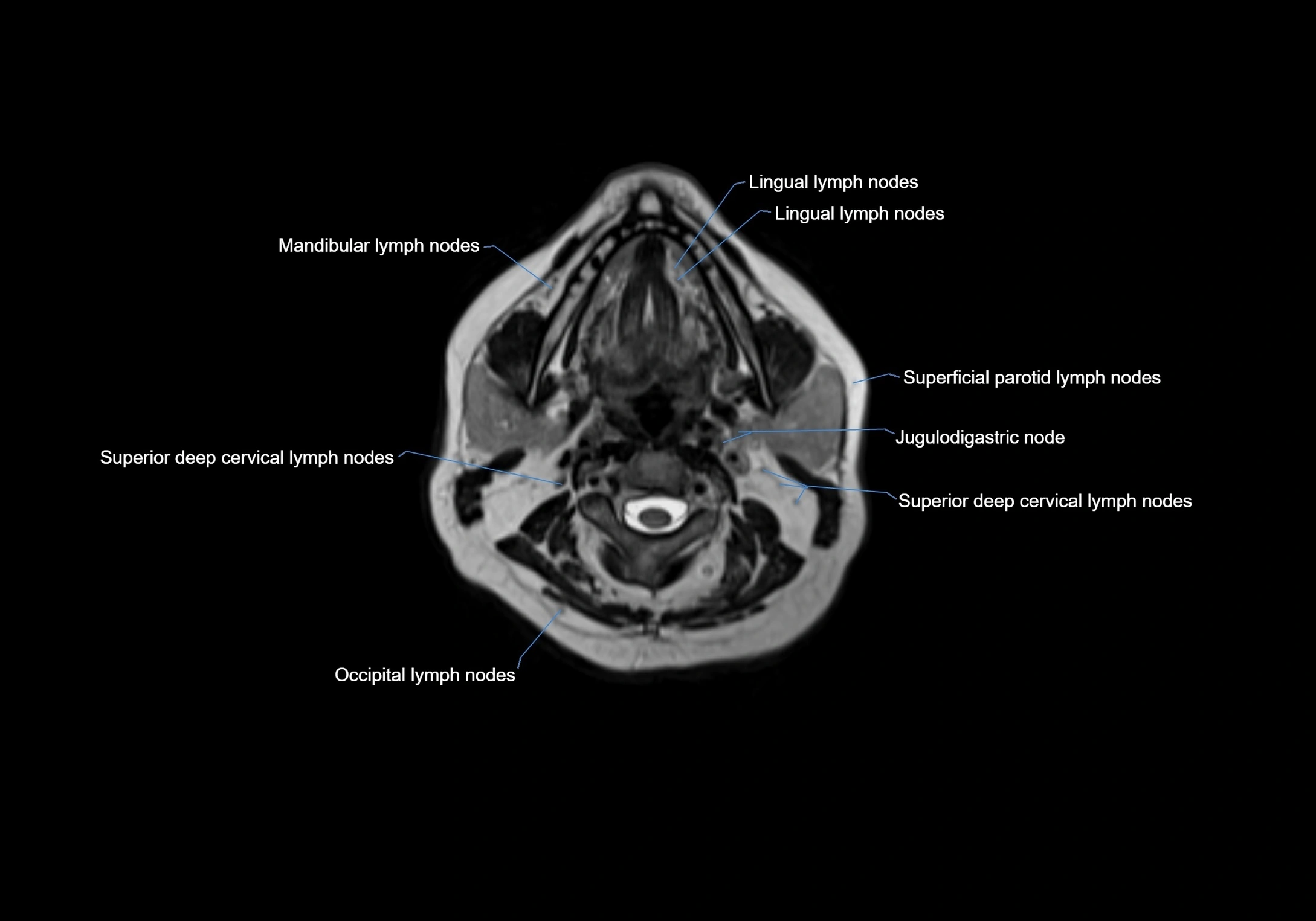
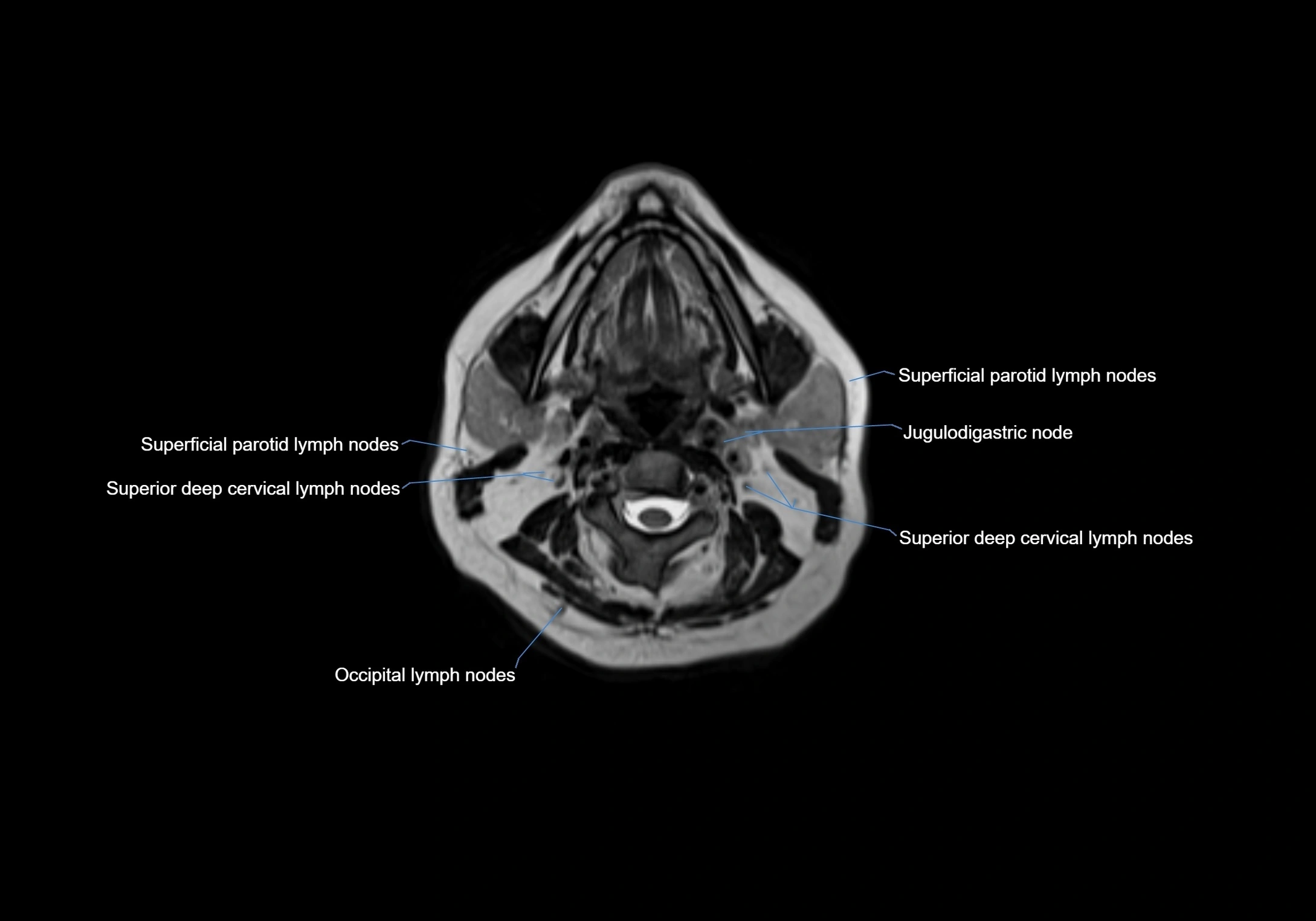
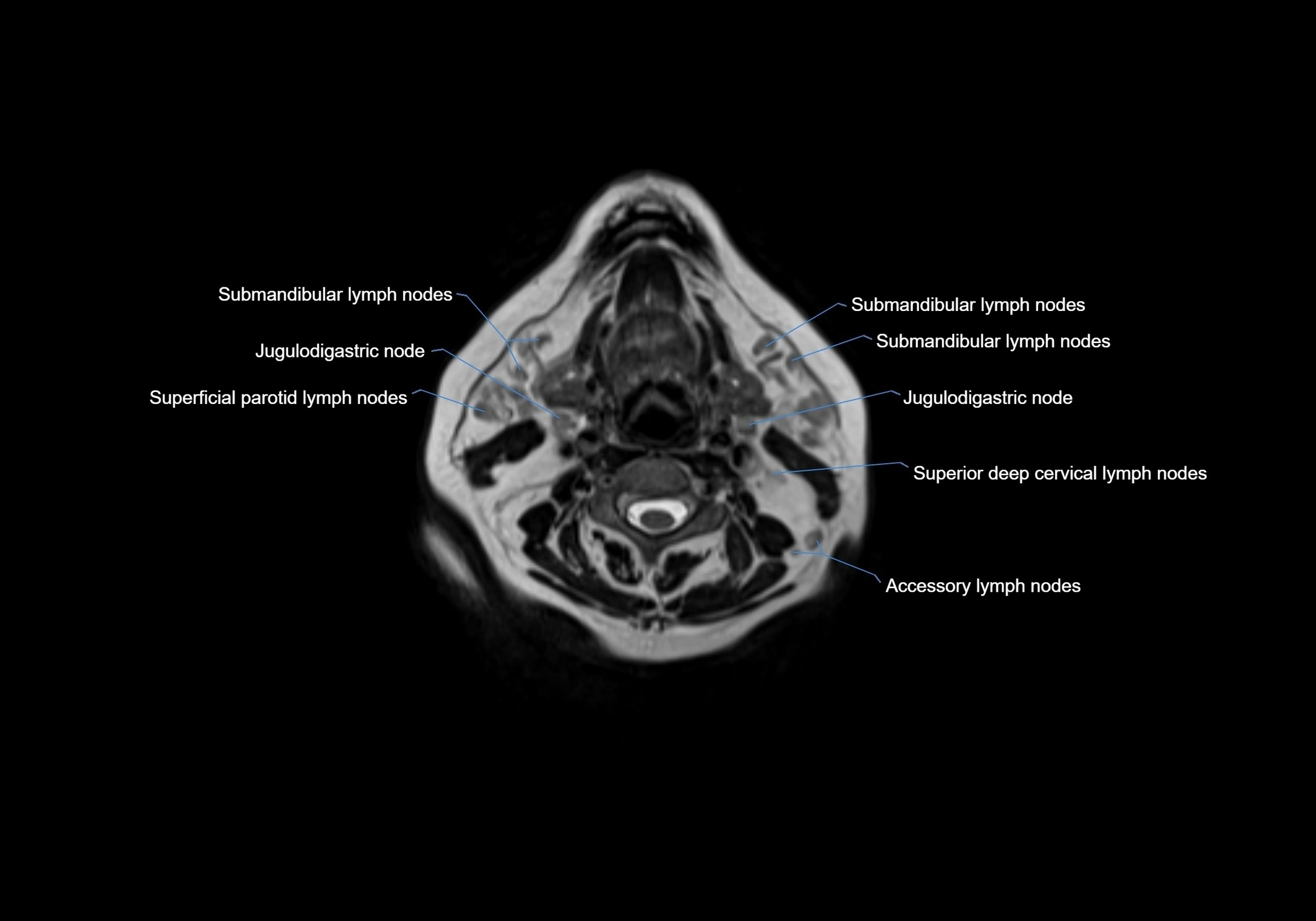
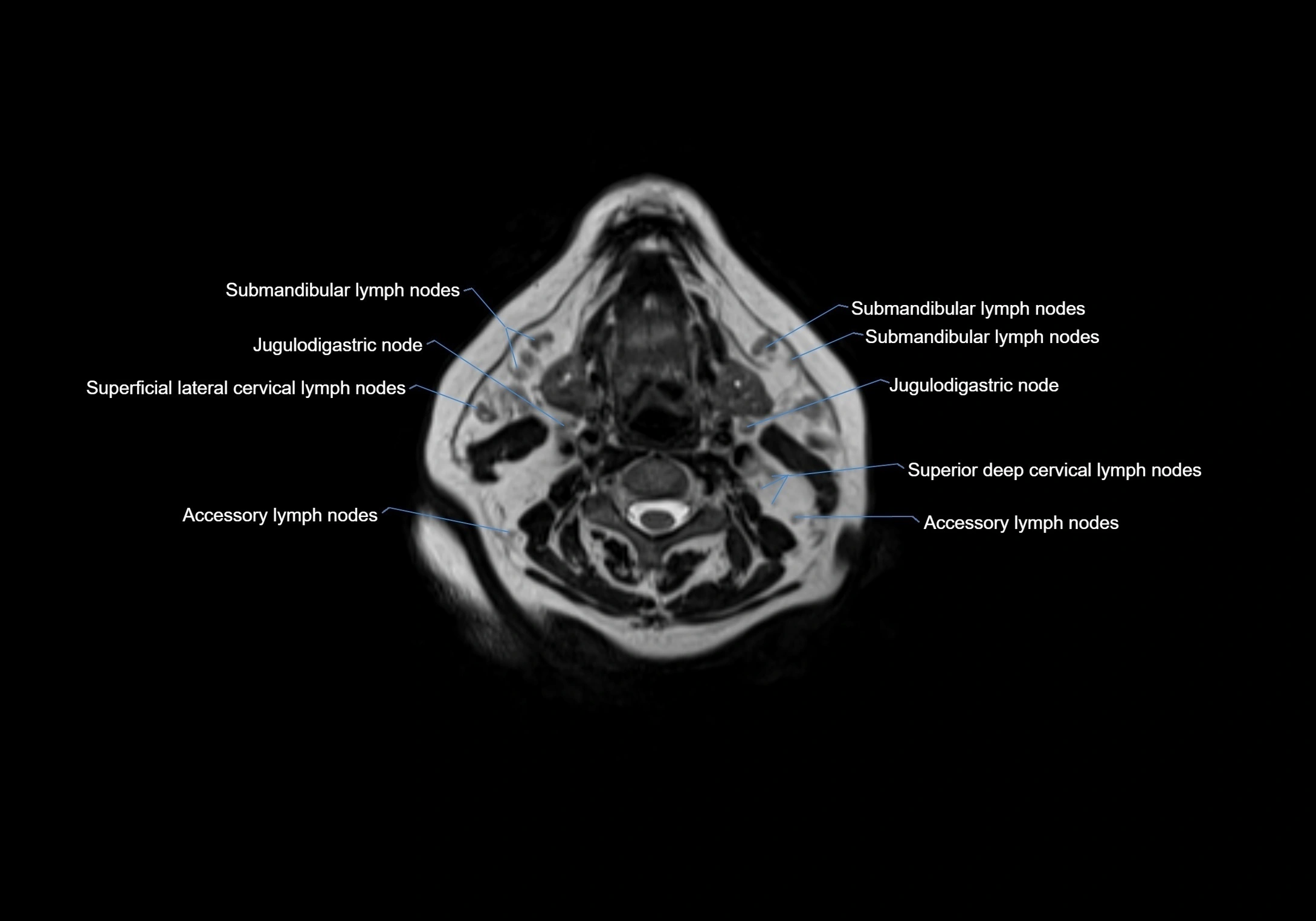
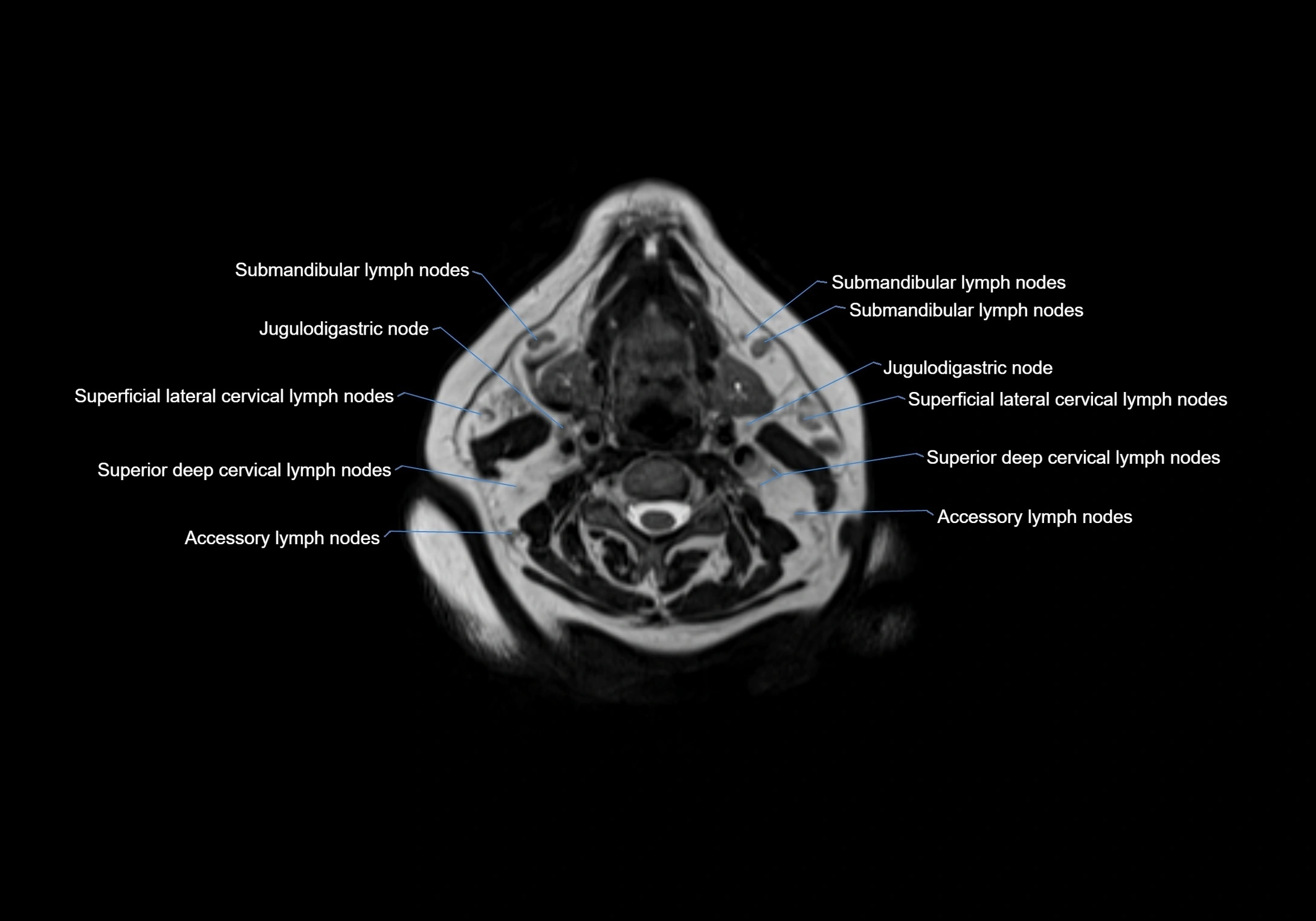
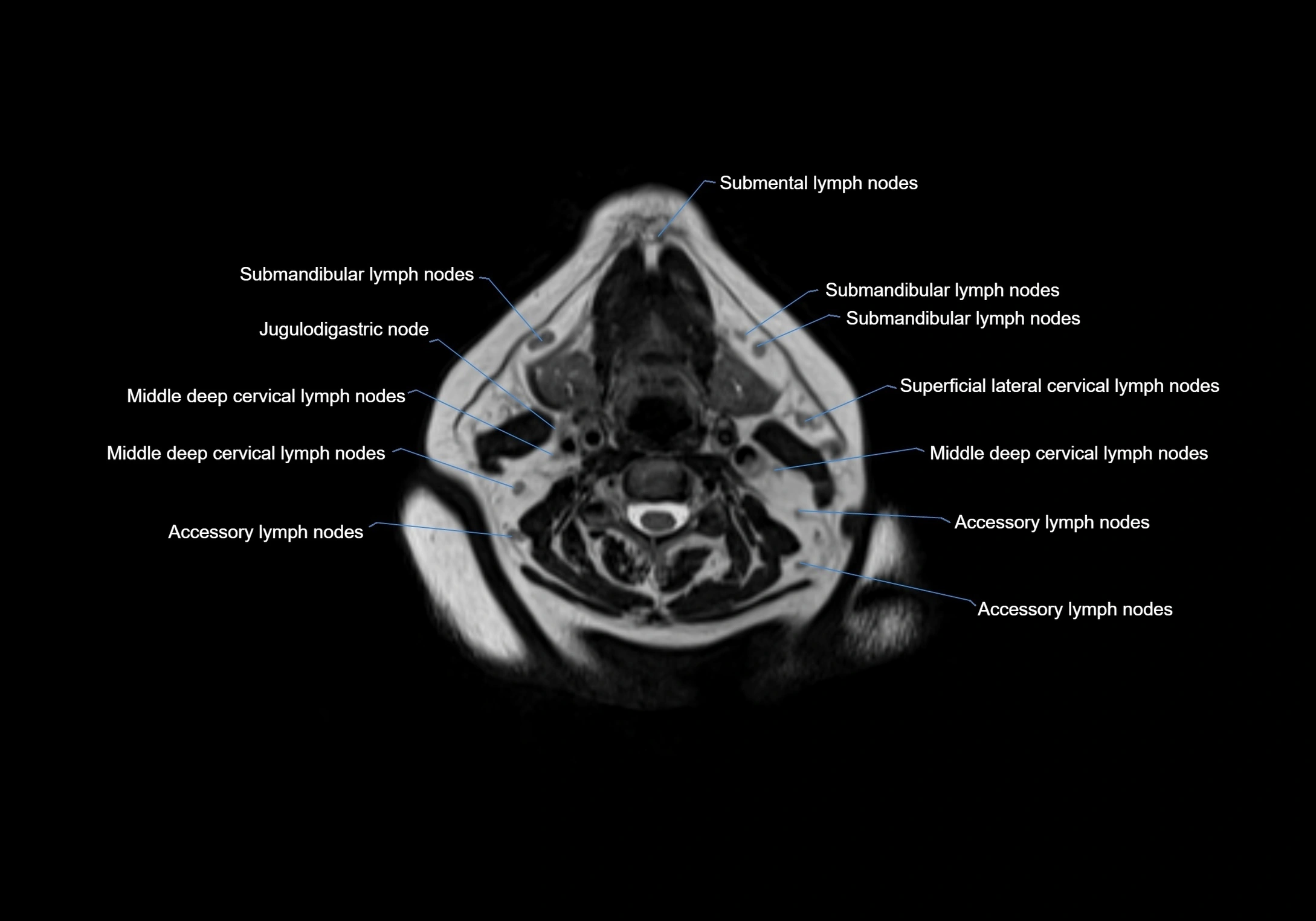
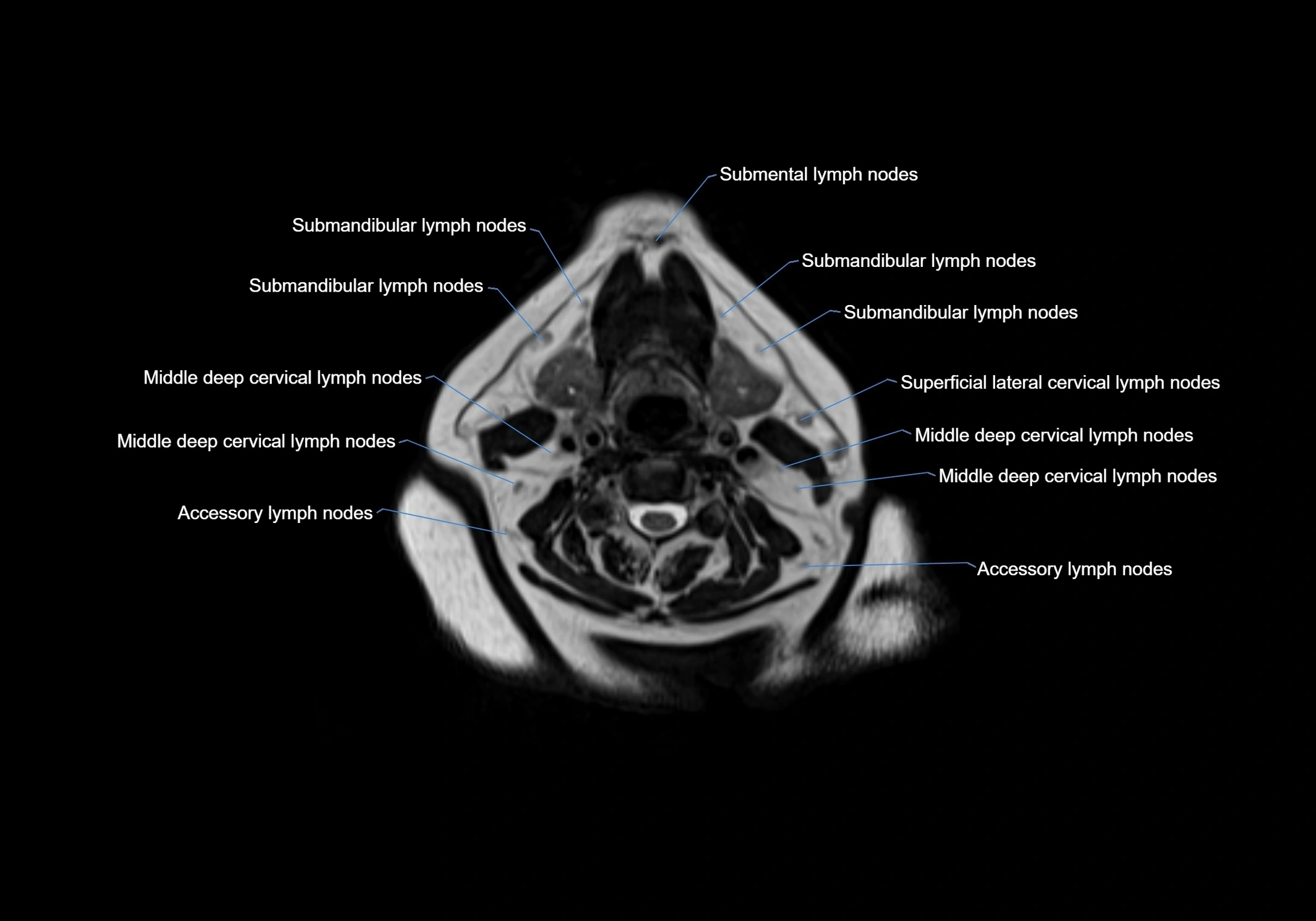
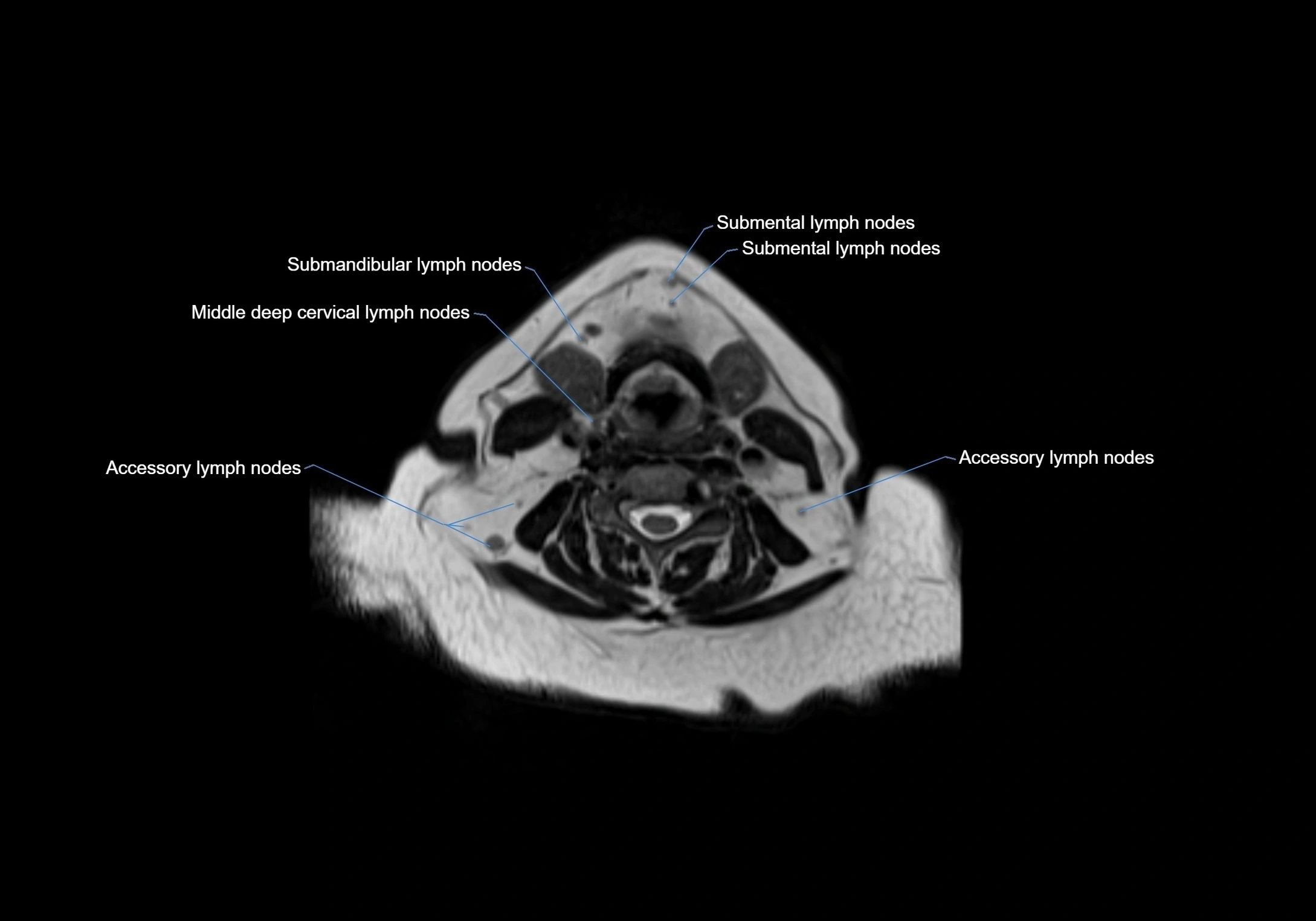
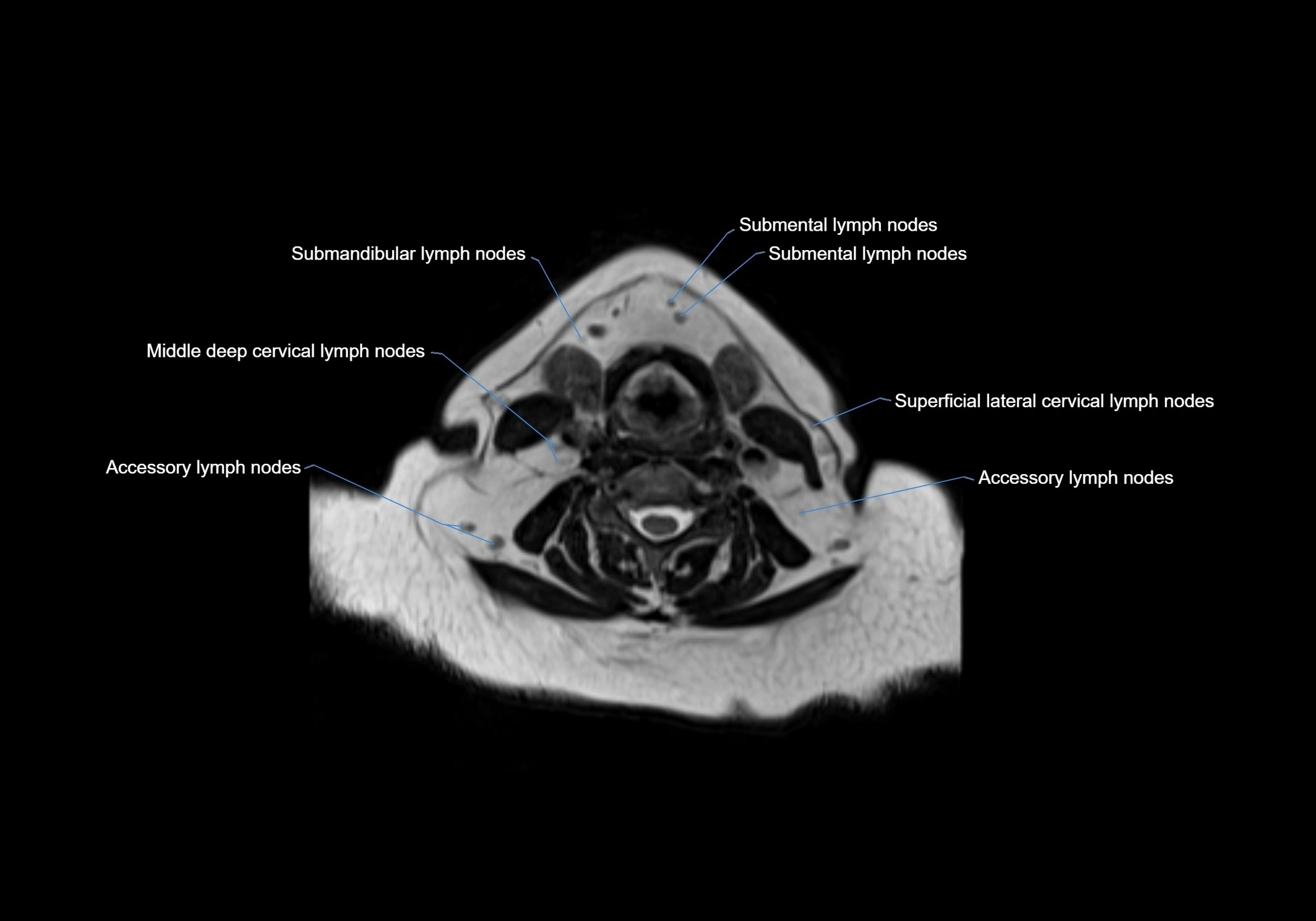
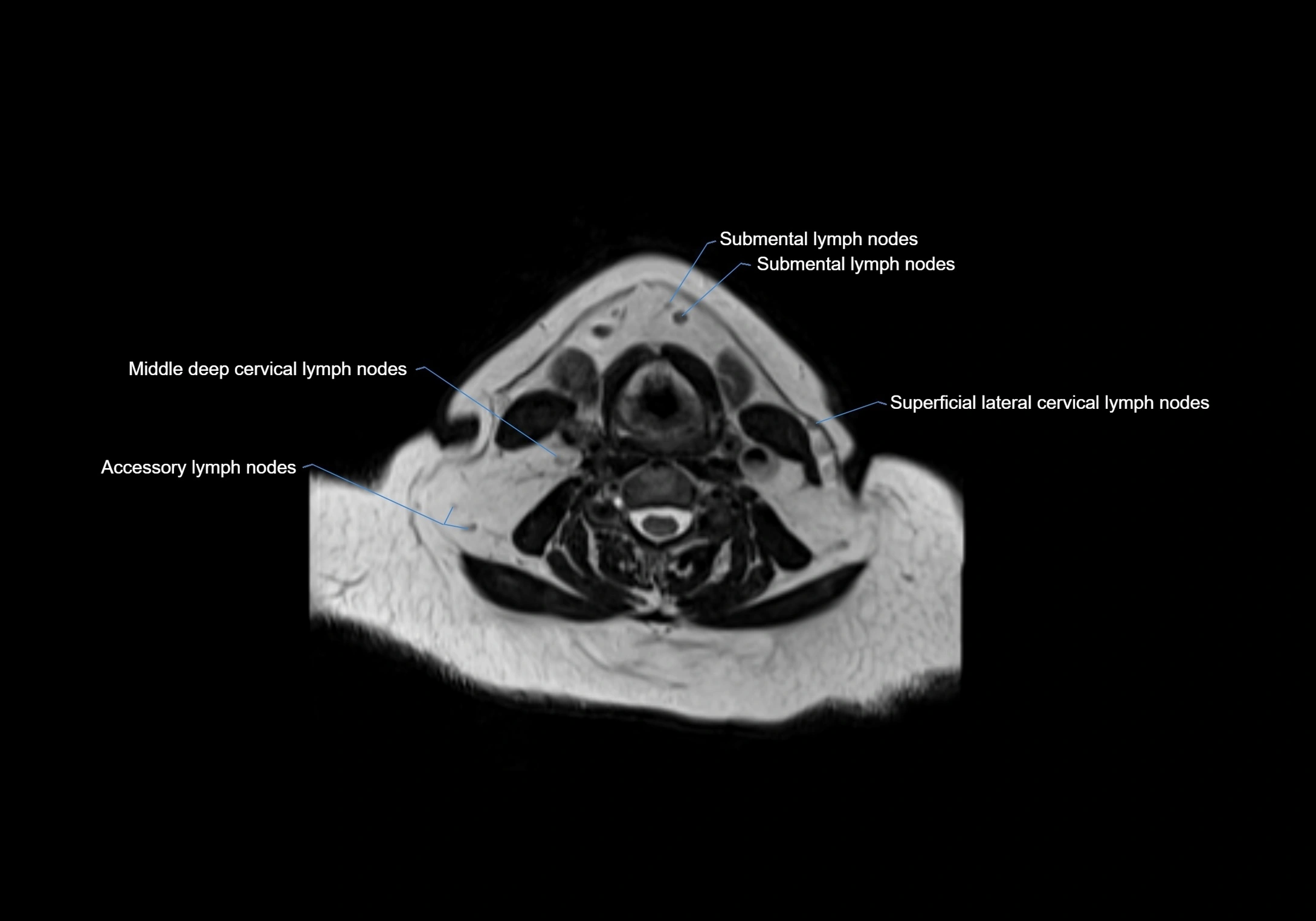
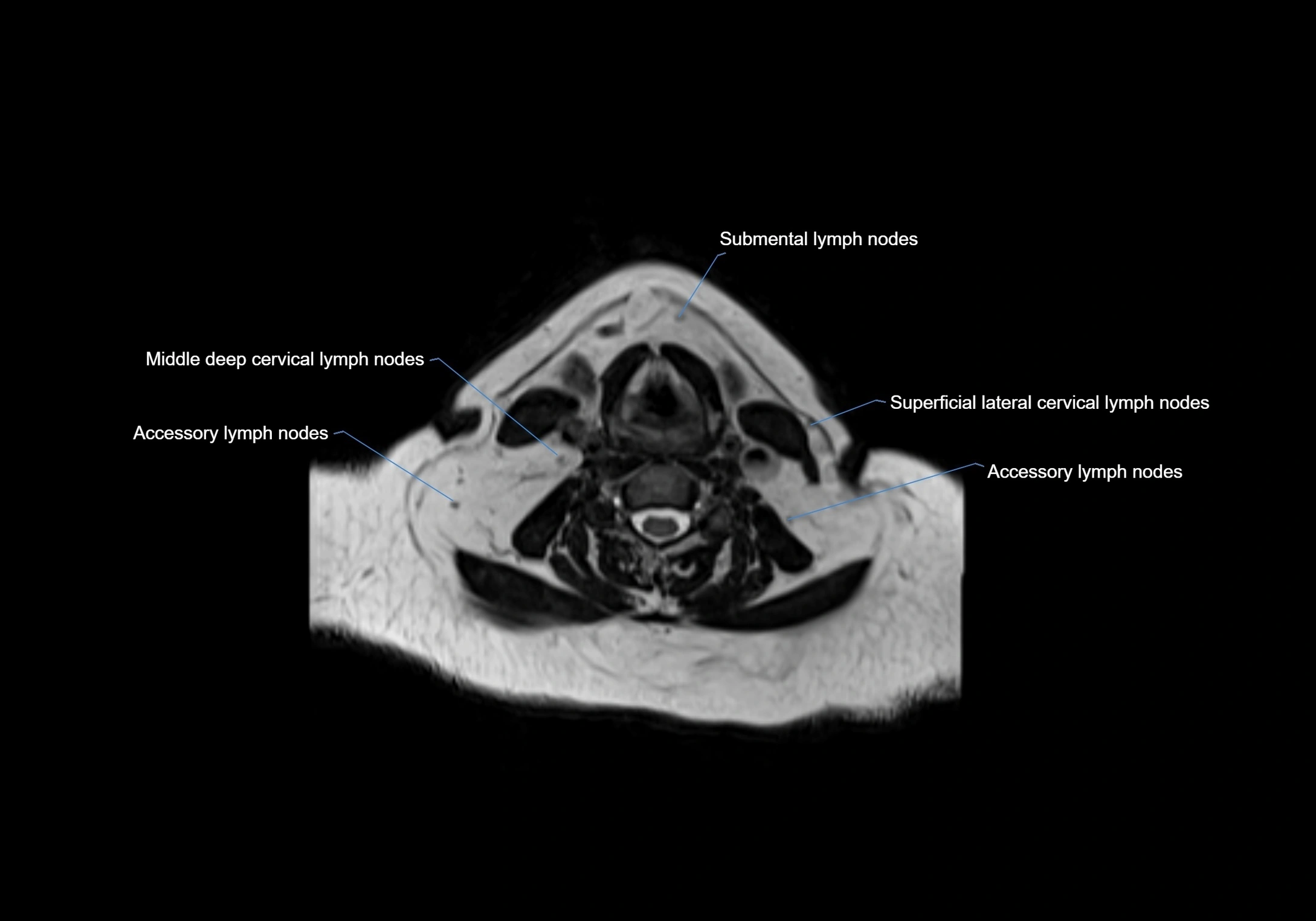
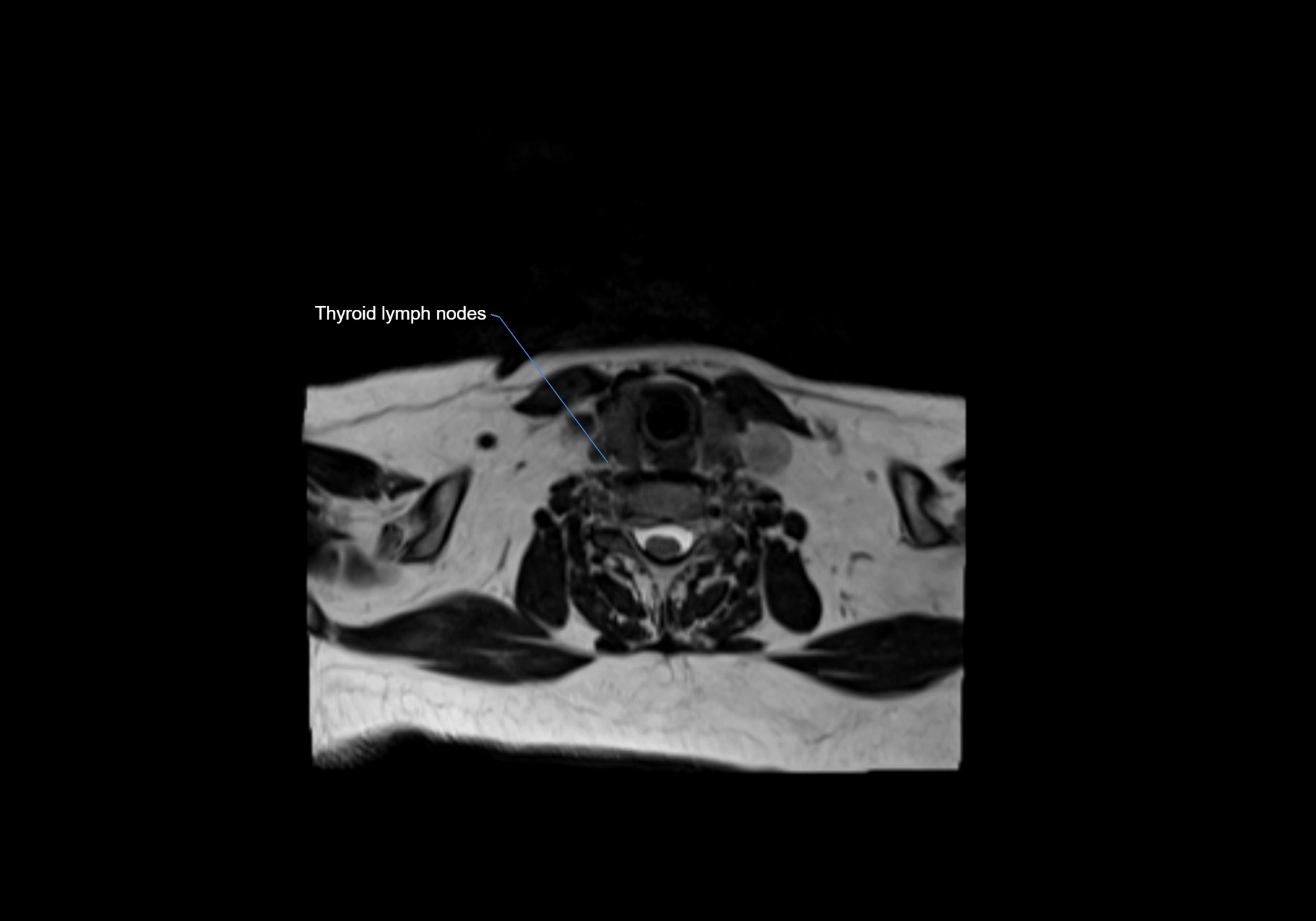
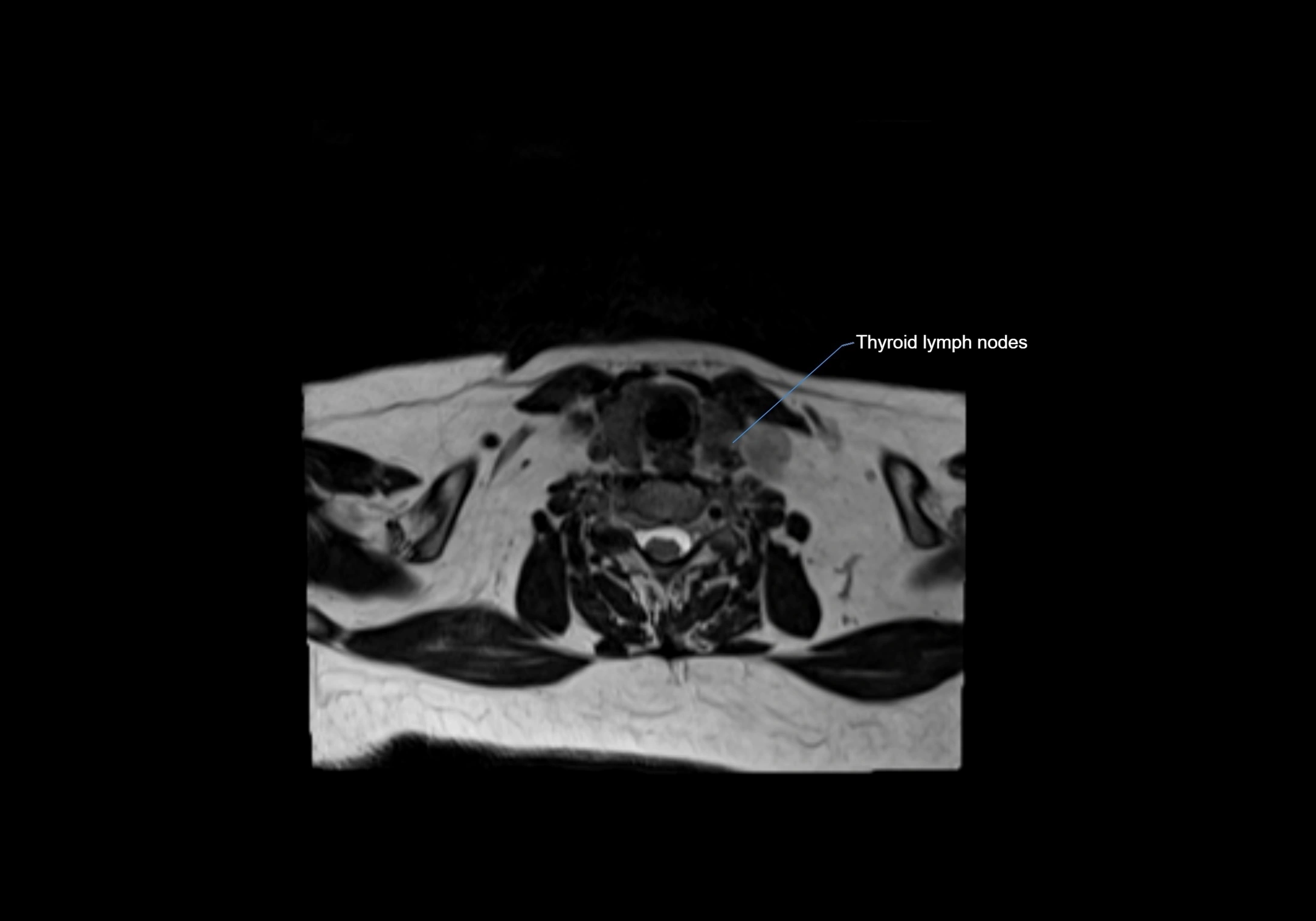
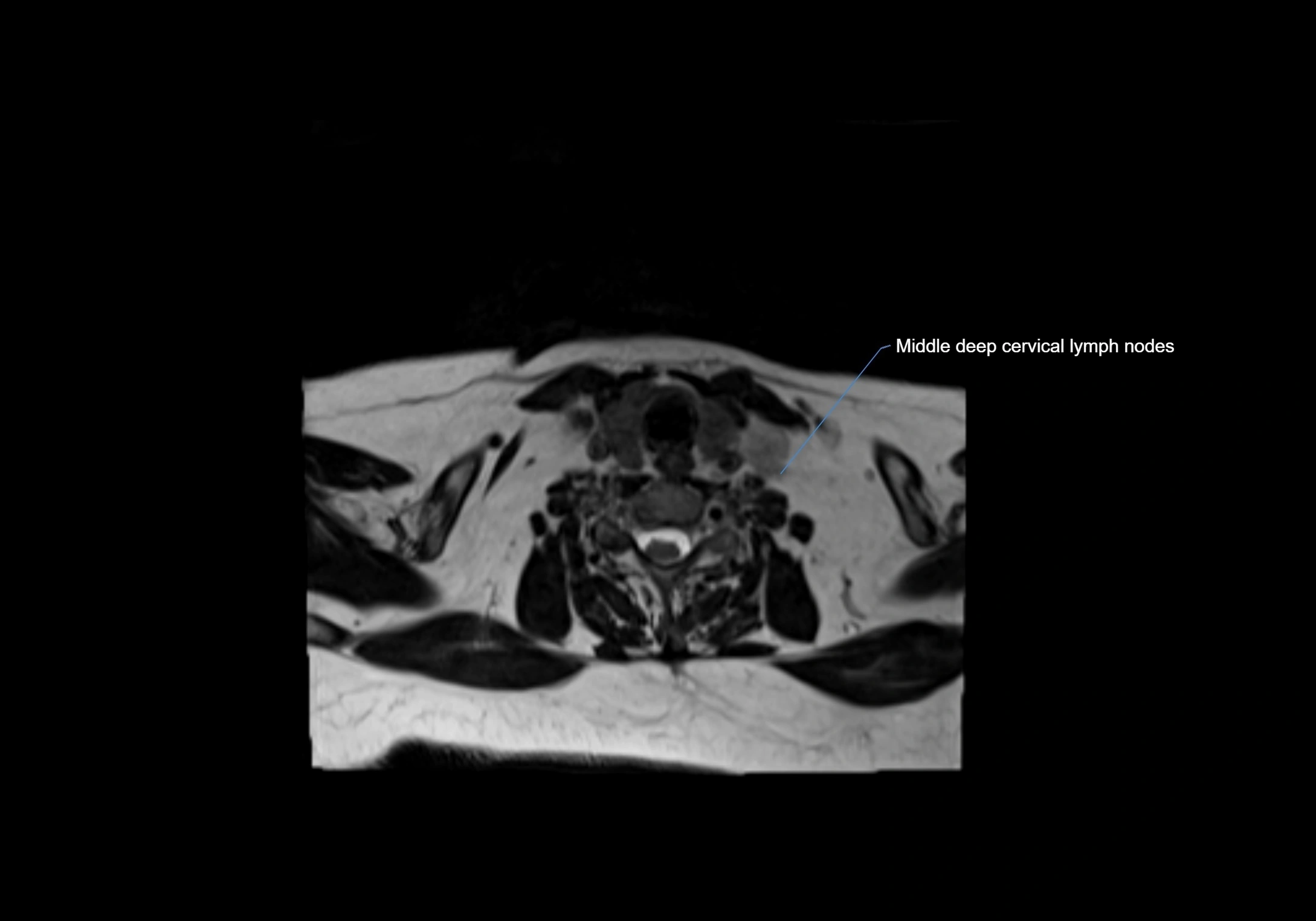
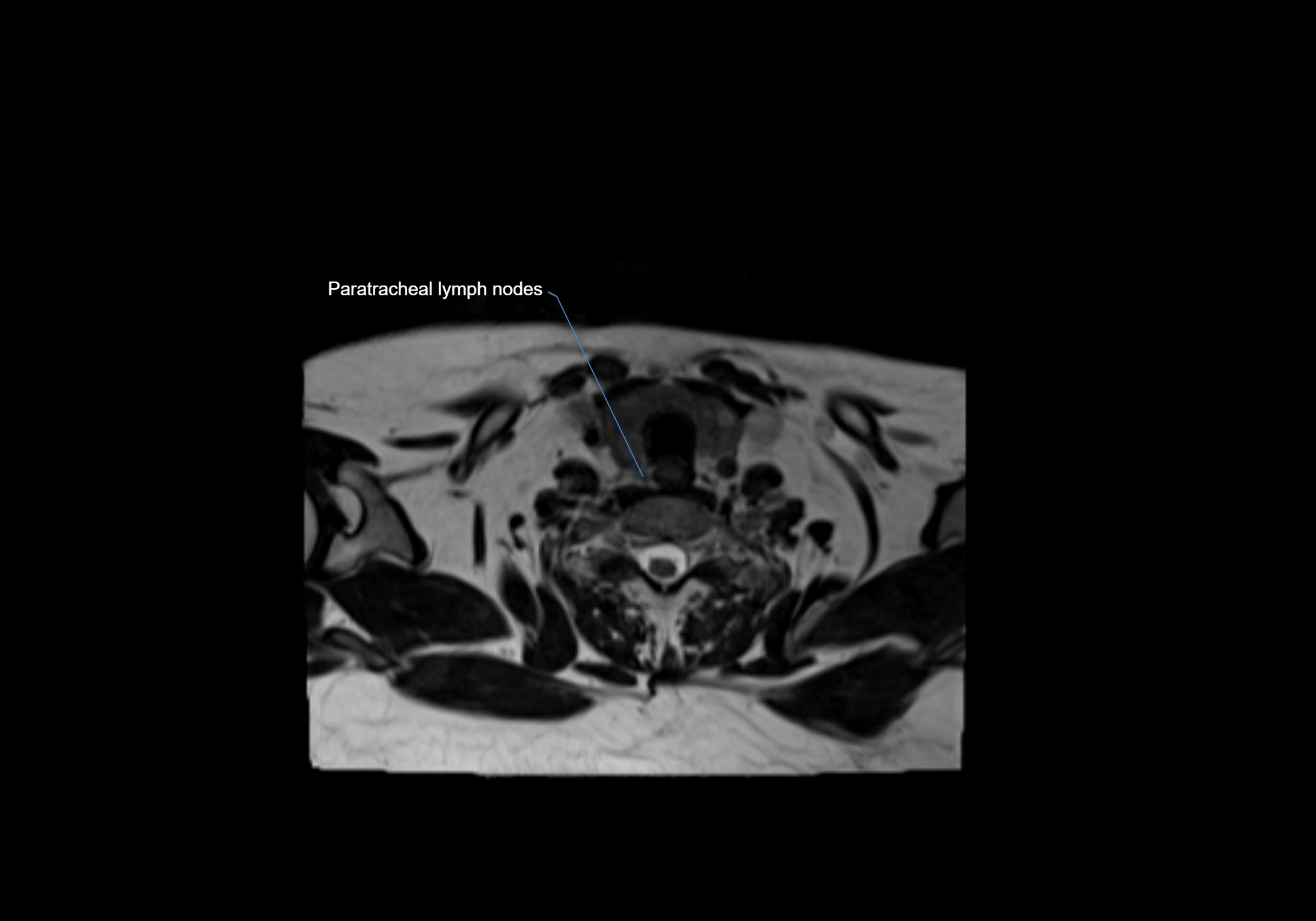
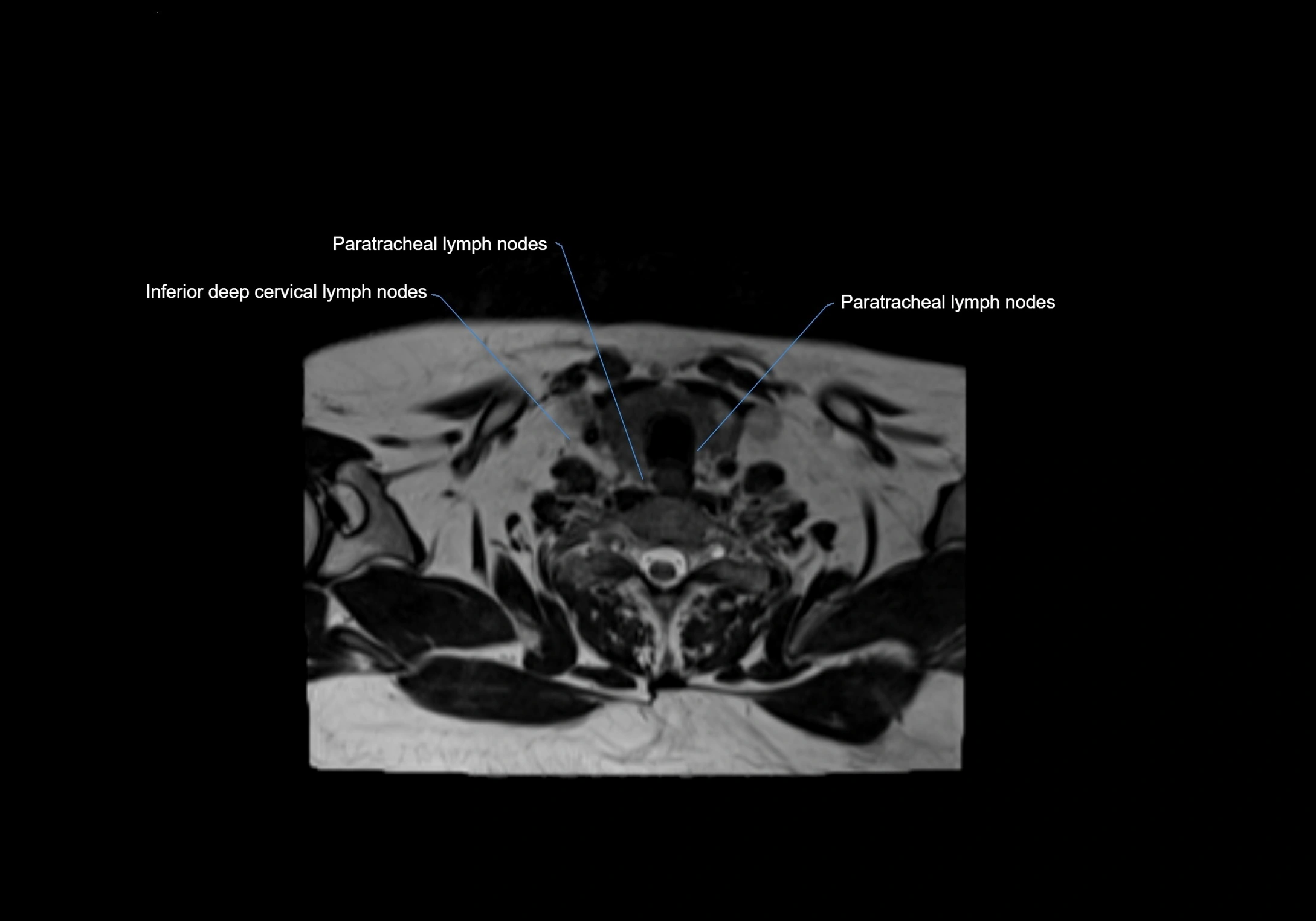
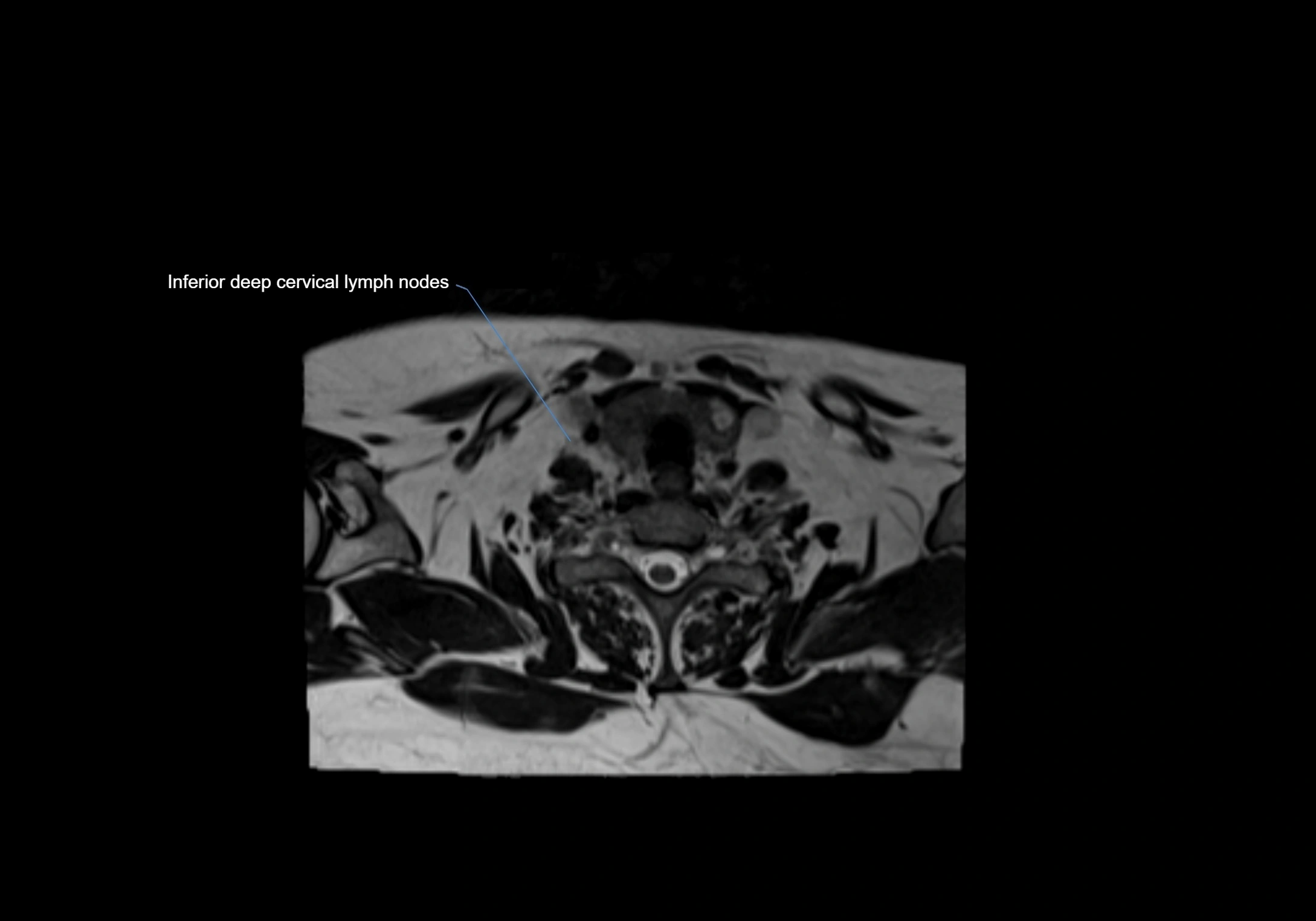
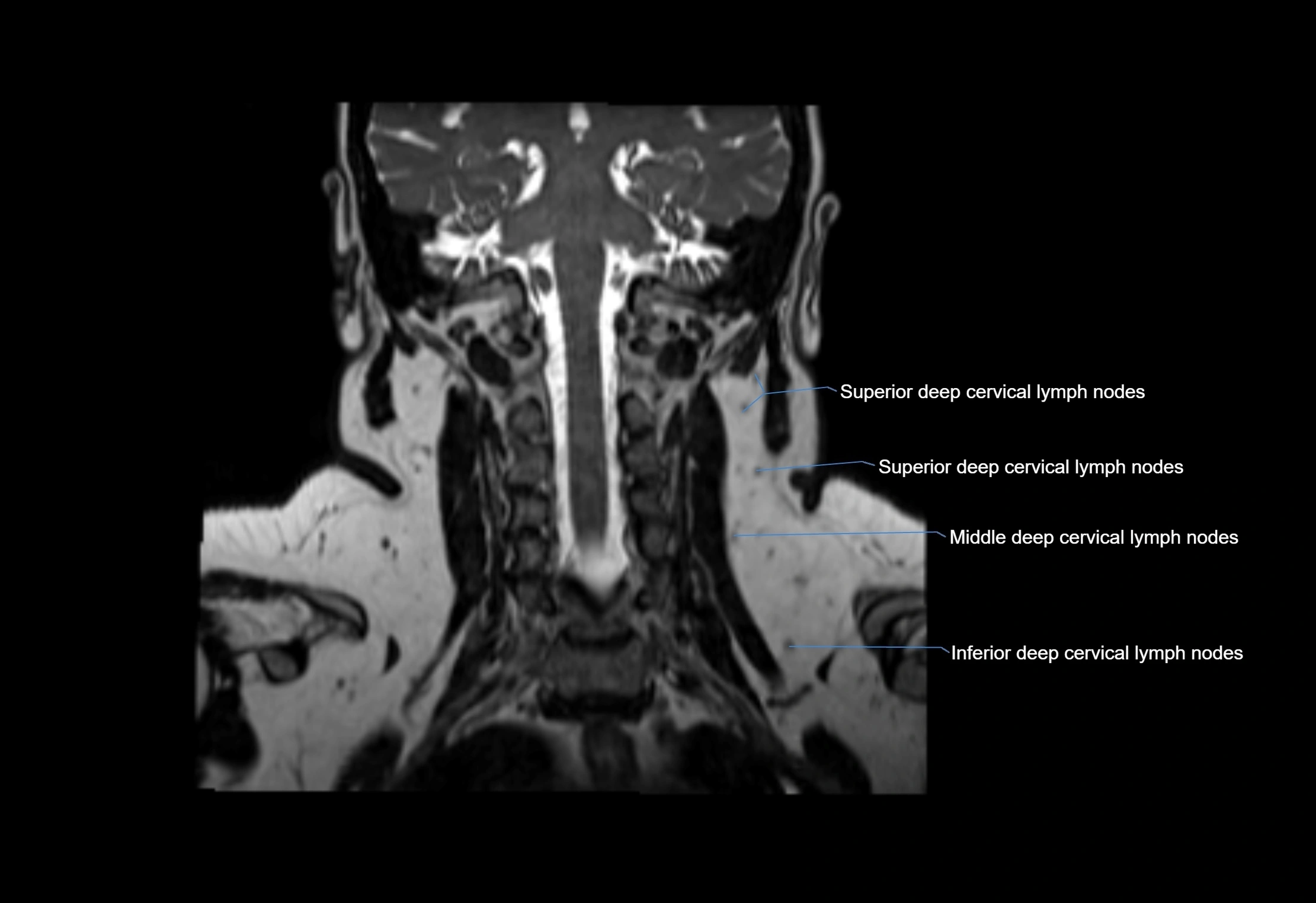
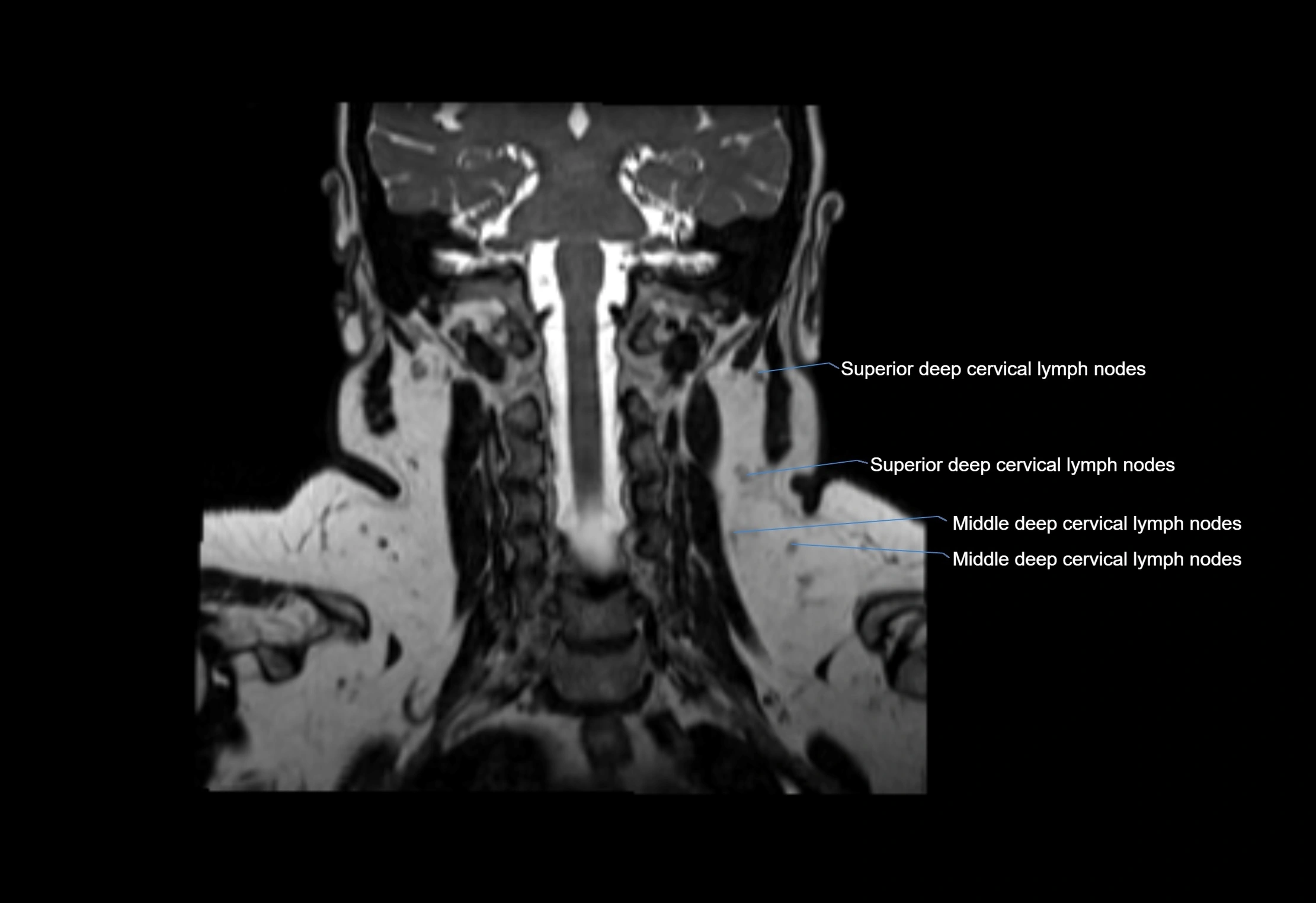
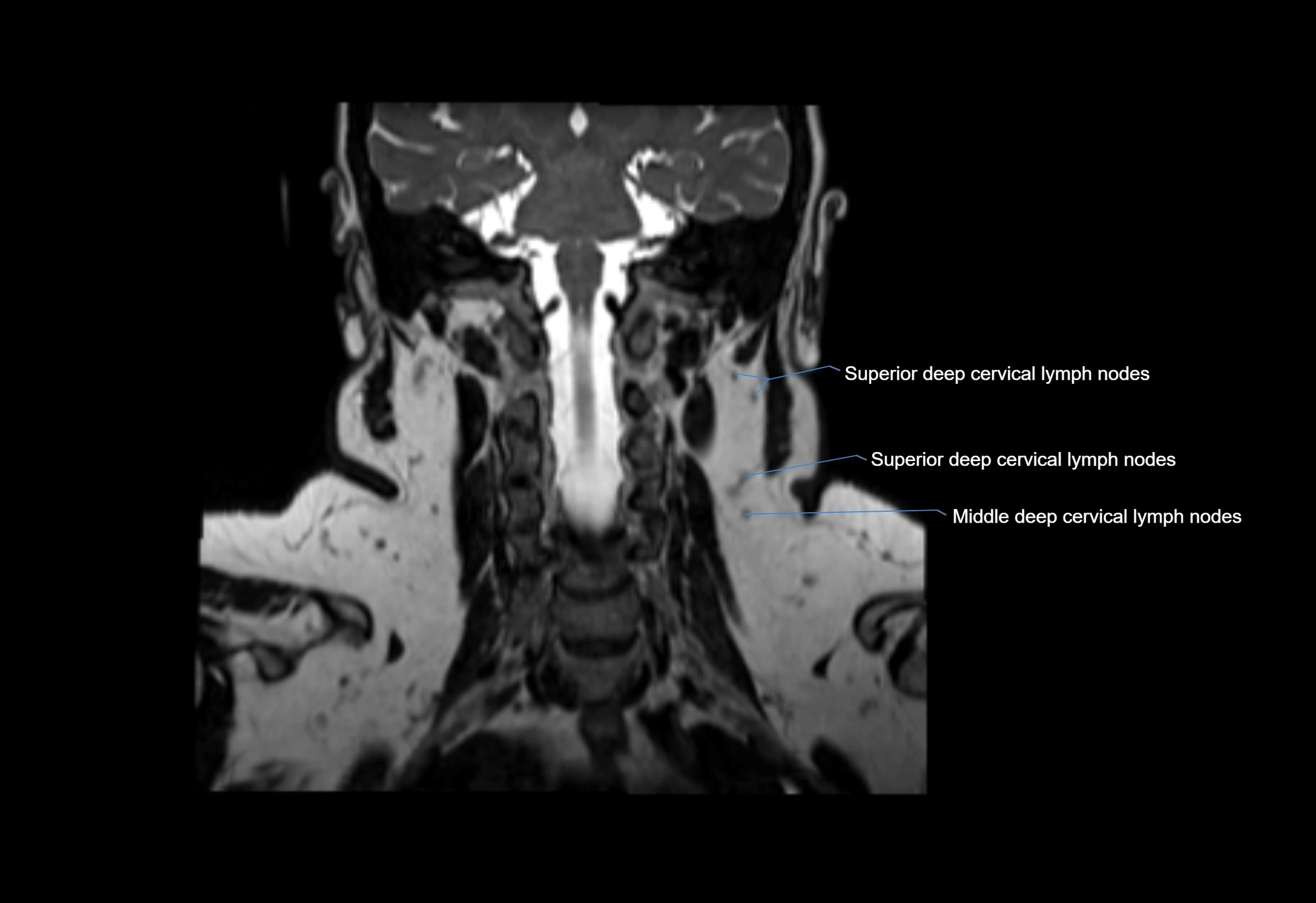
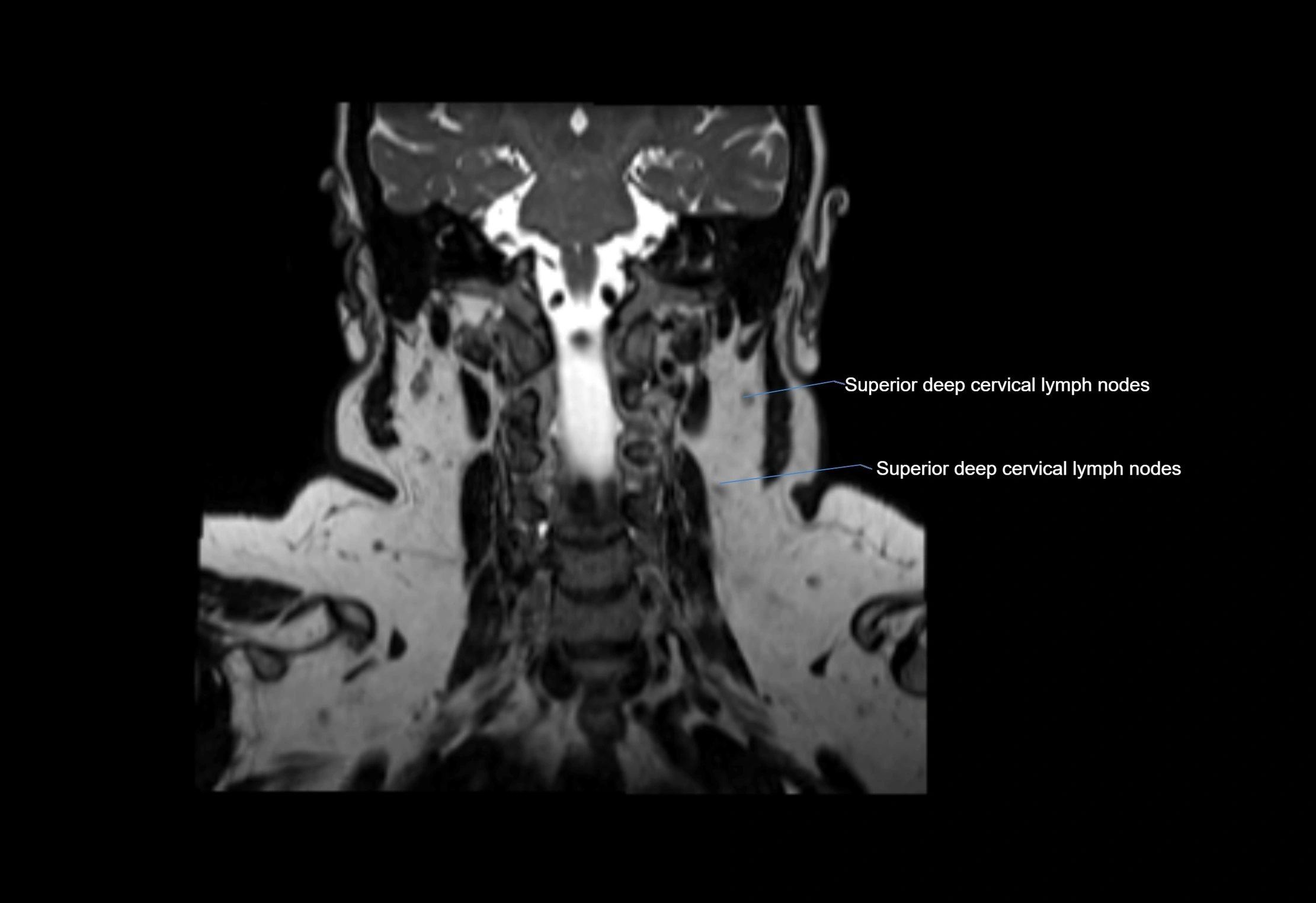
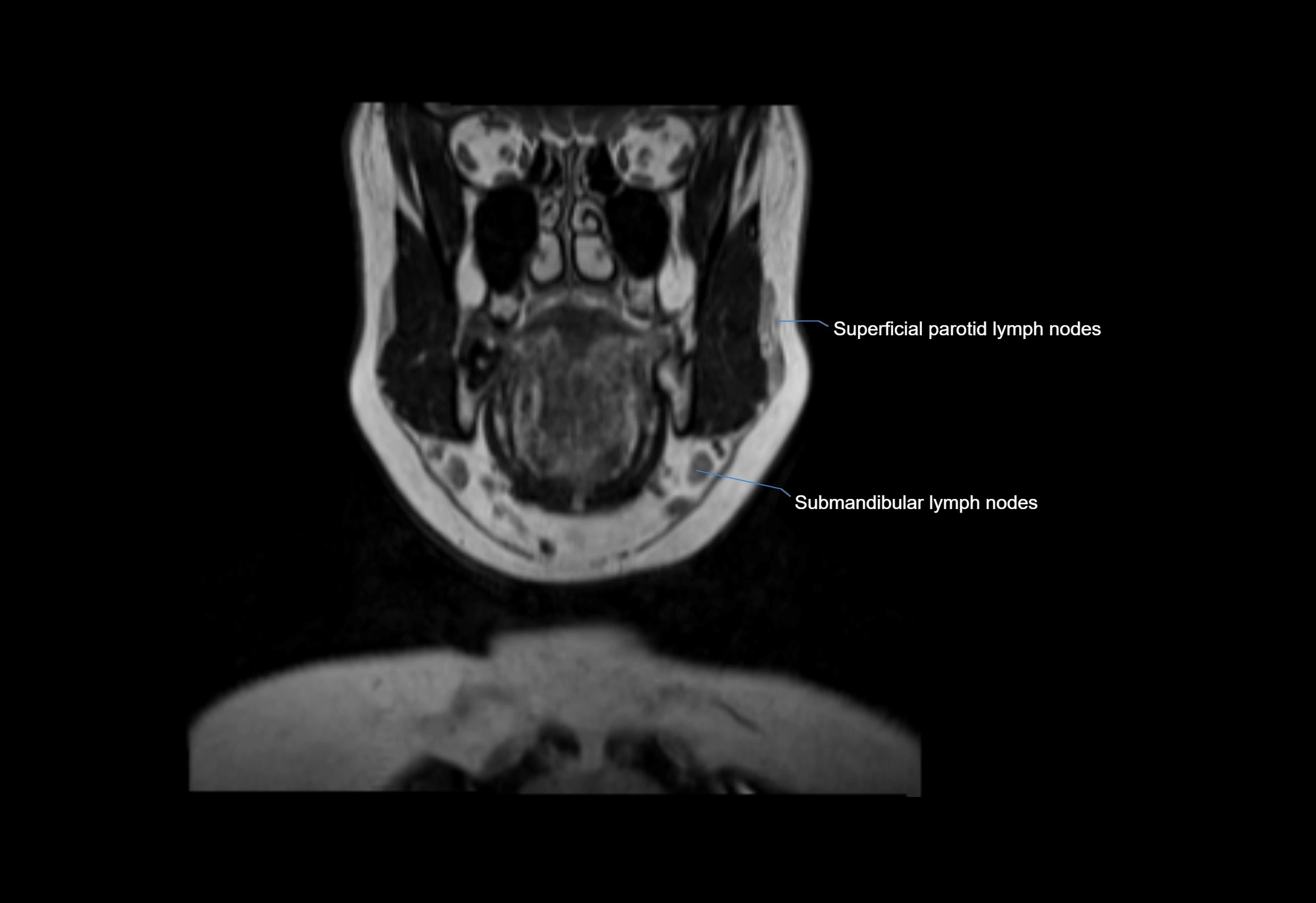
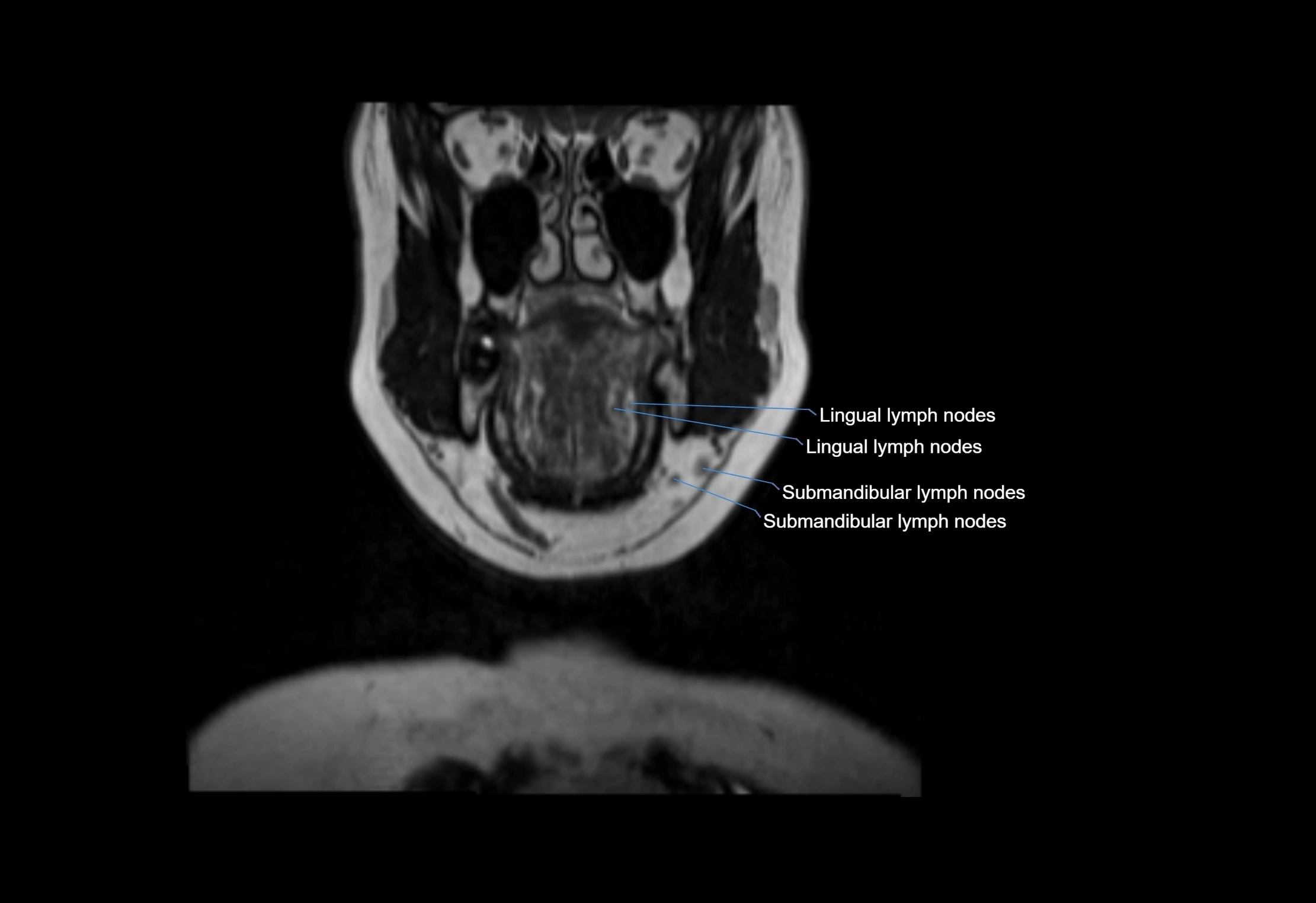
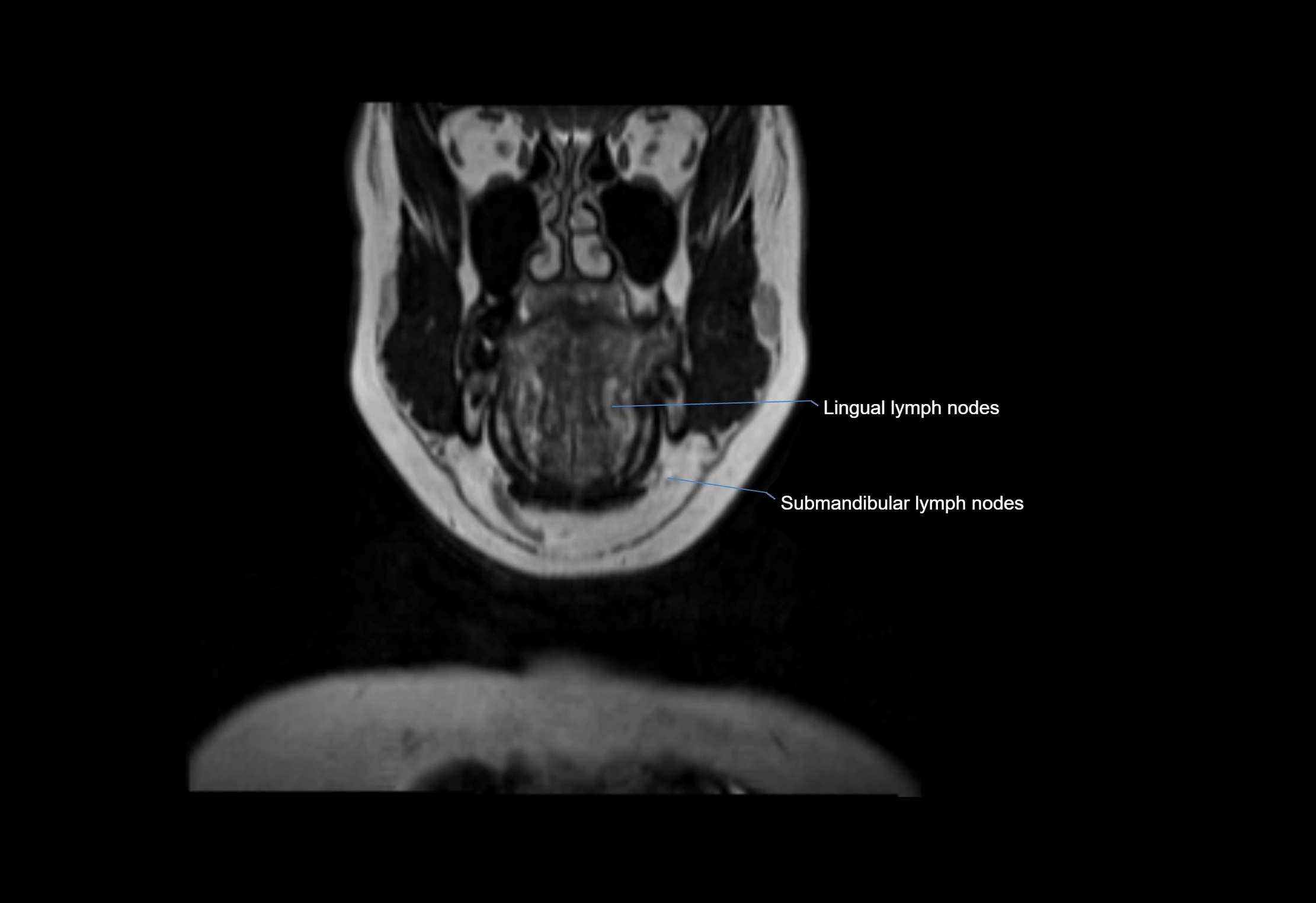
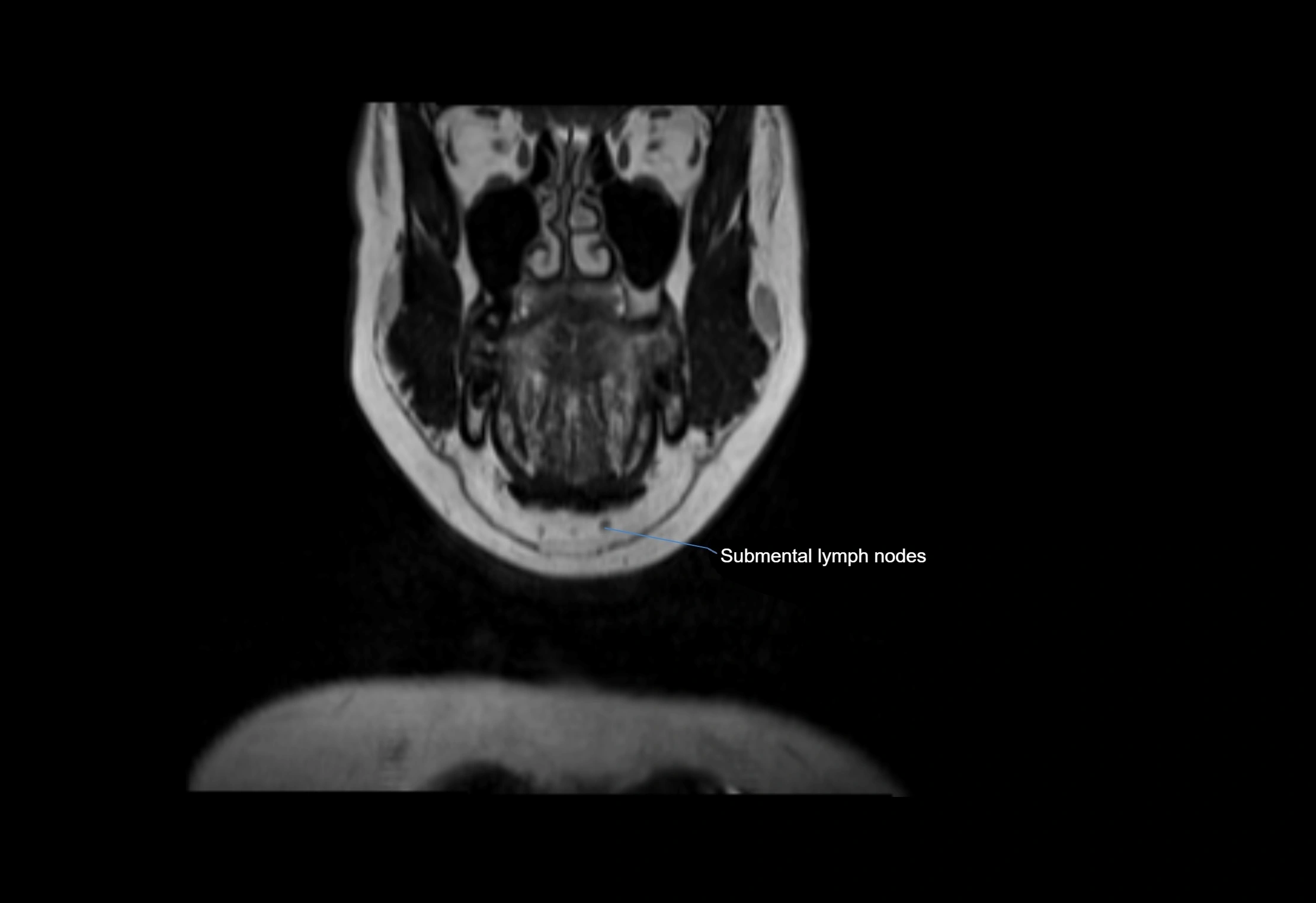
MRI Appearance
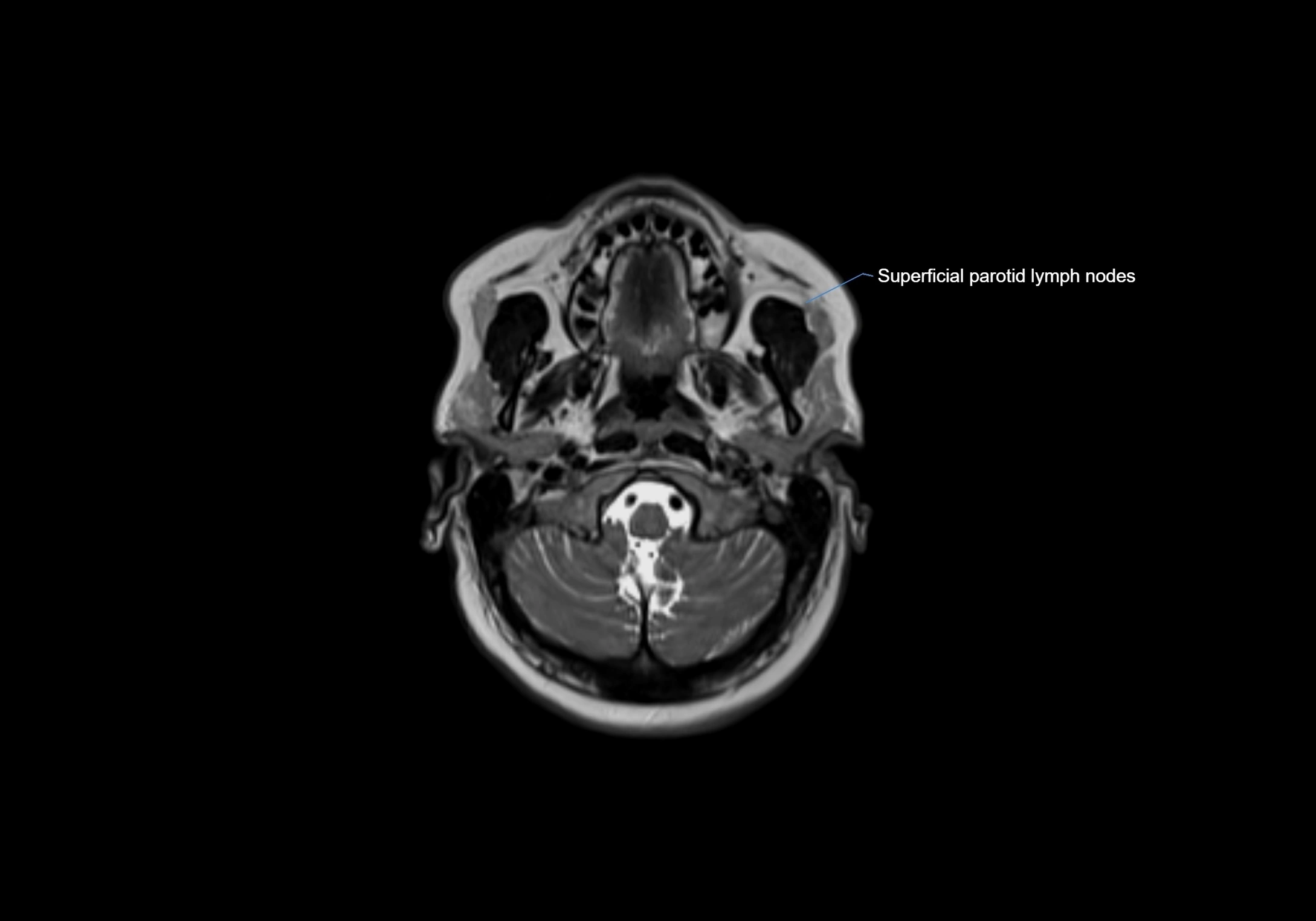
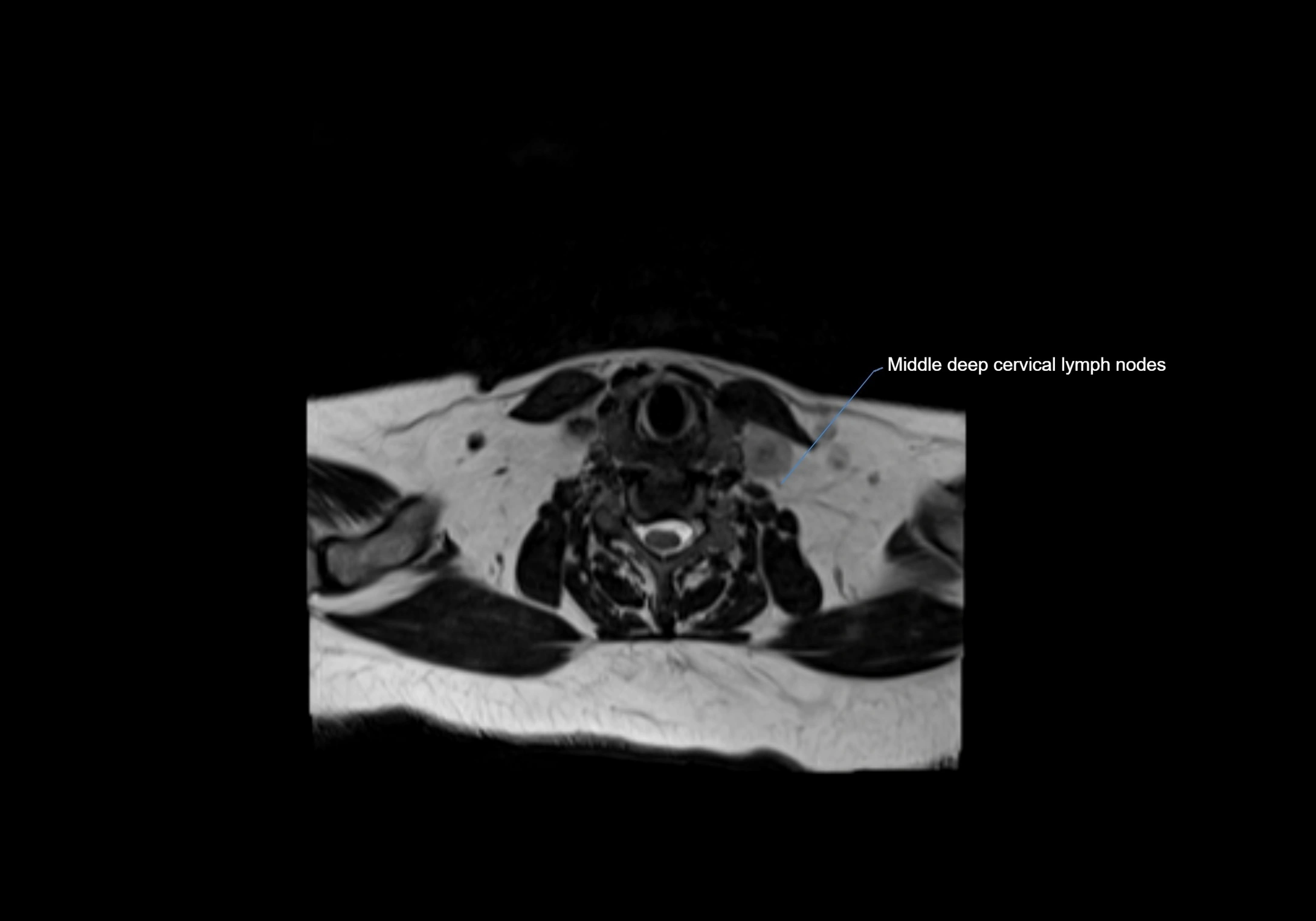
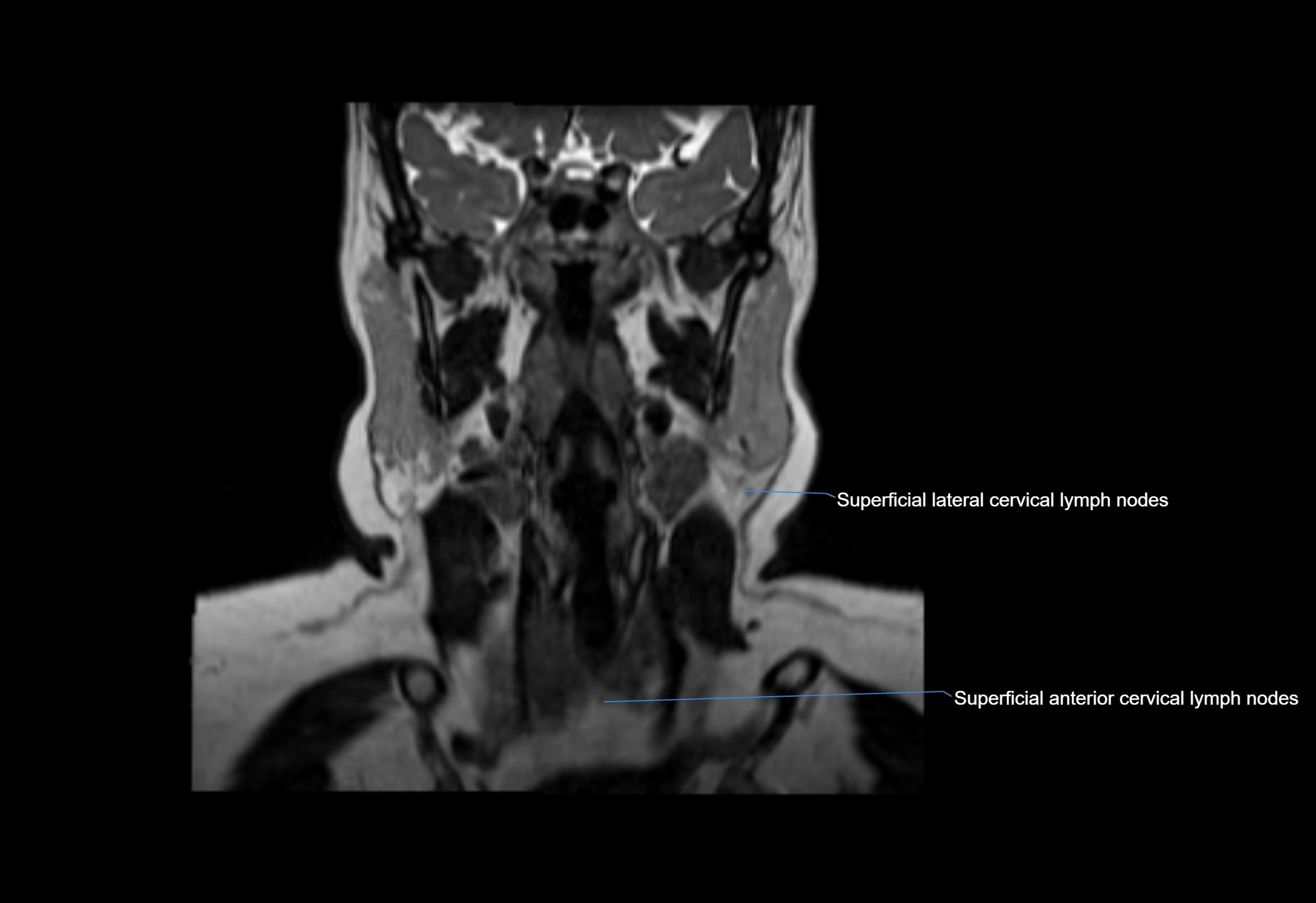
T1-weighted images:
-
Normal accessory nodes appear as small, oval hypointense to intermediate signal structures within subcutaneous fat
-
Surrounded by hyperintense fat, enhancing contrast for visualization
-
Pathological nodes may appear enlarged or rounded, sometimes with cortical thickening
T1 Post-Contrast (Gadolinium-enhanced):
-
Normal nodes may show mild, homogeneous enhancement
-
Inflamed or metastatic nodes demonstrate marked homogeneous or heterogeneous enhancement, highlighting the cortex and fatty hilum
-
Post-contrast imaging helps detect early metastasis, infection, or inflammatory changes
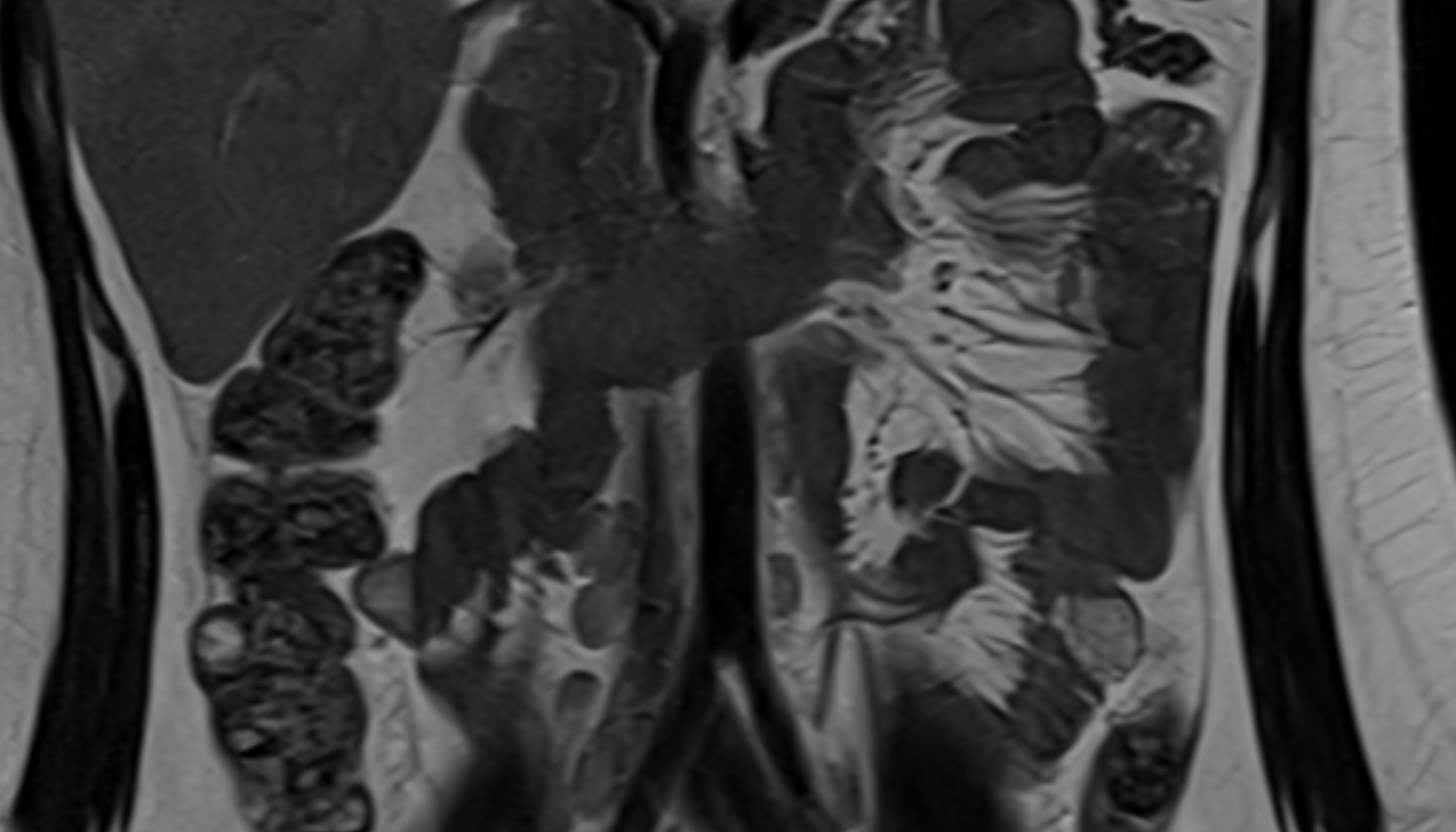
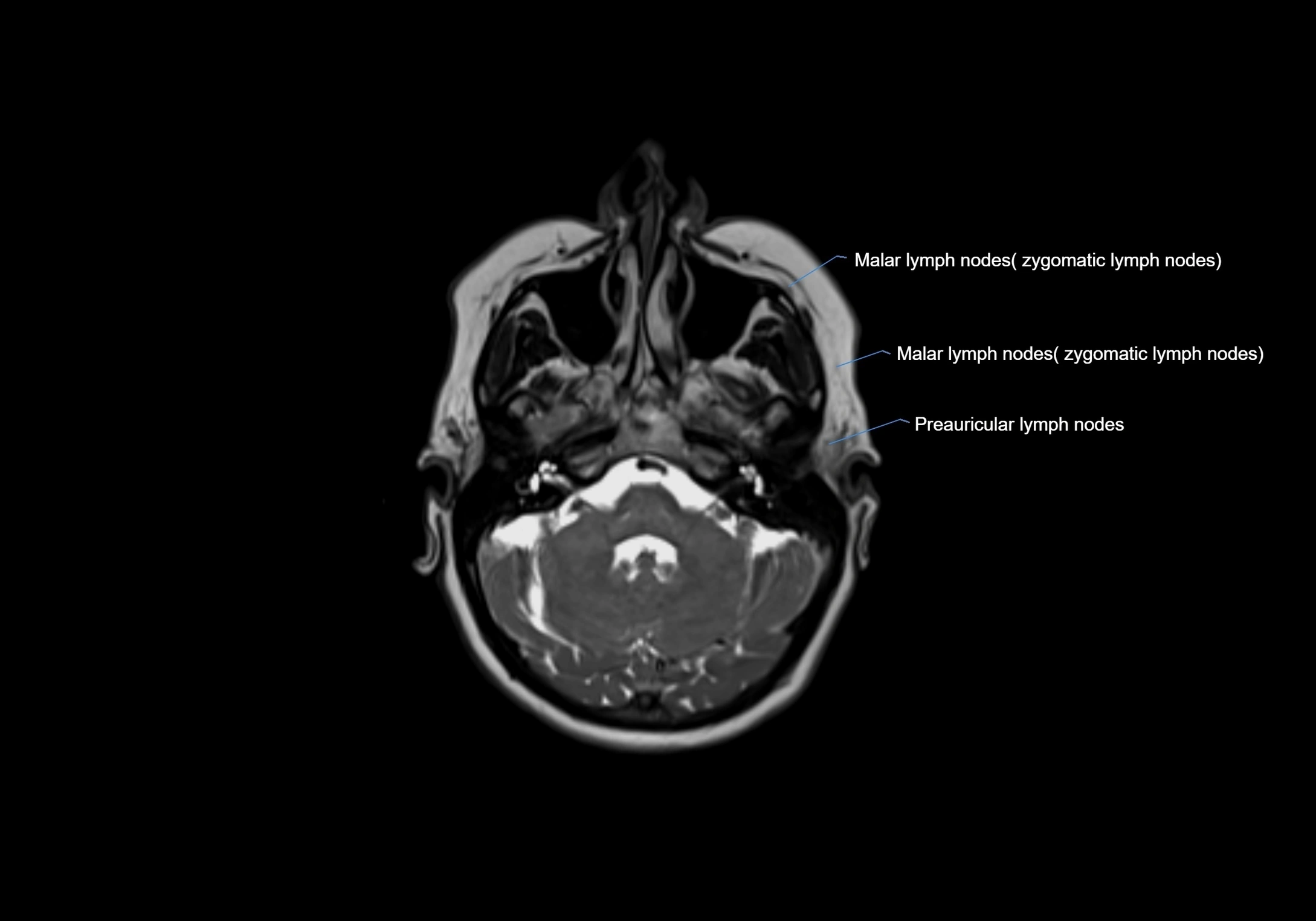
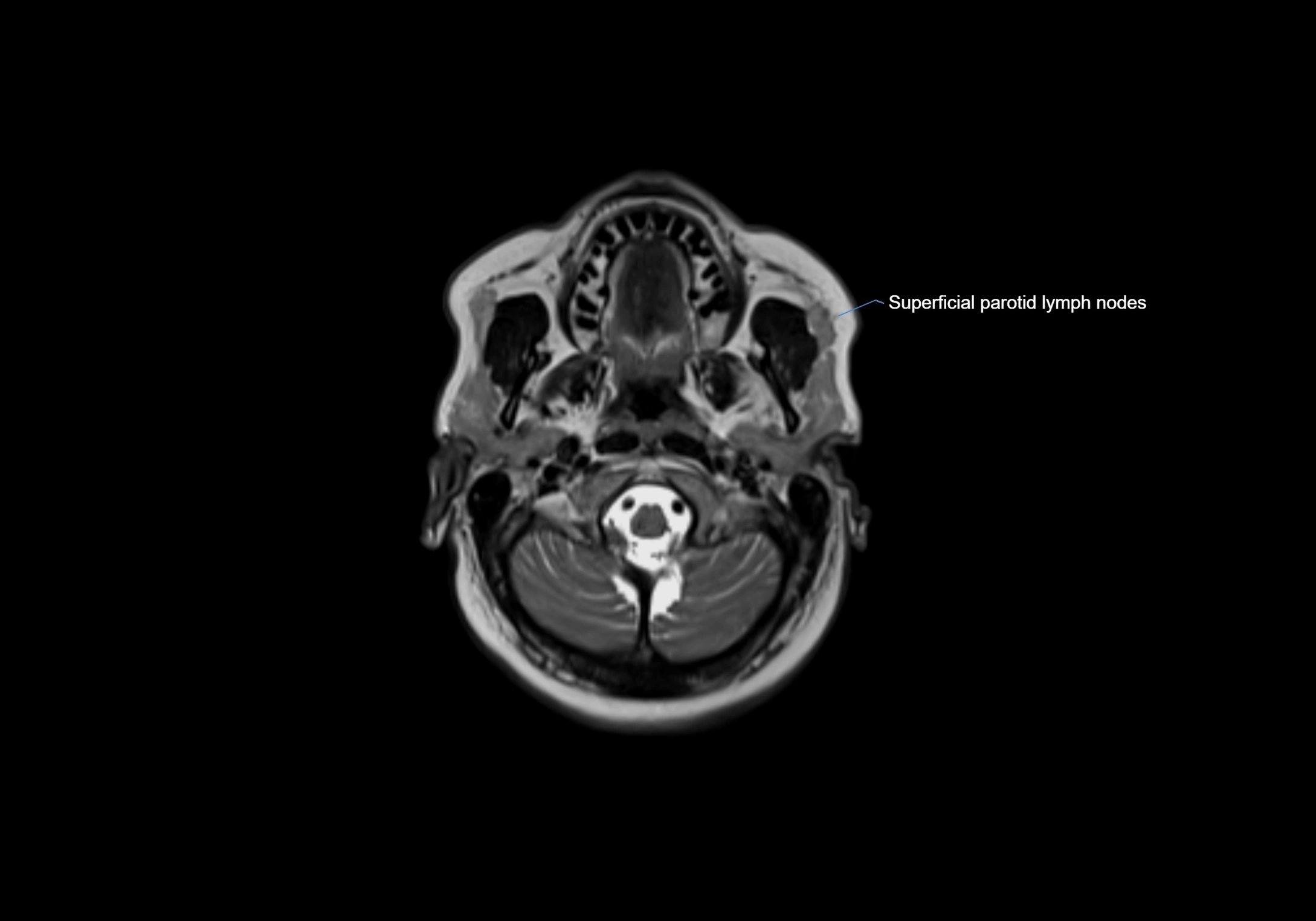
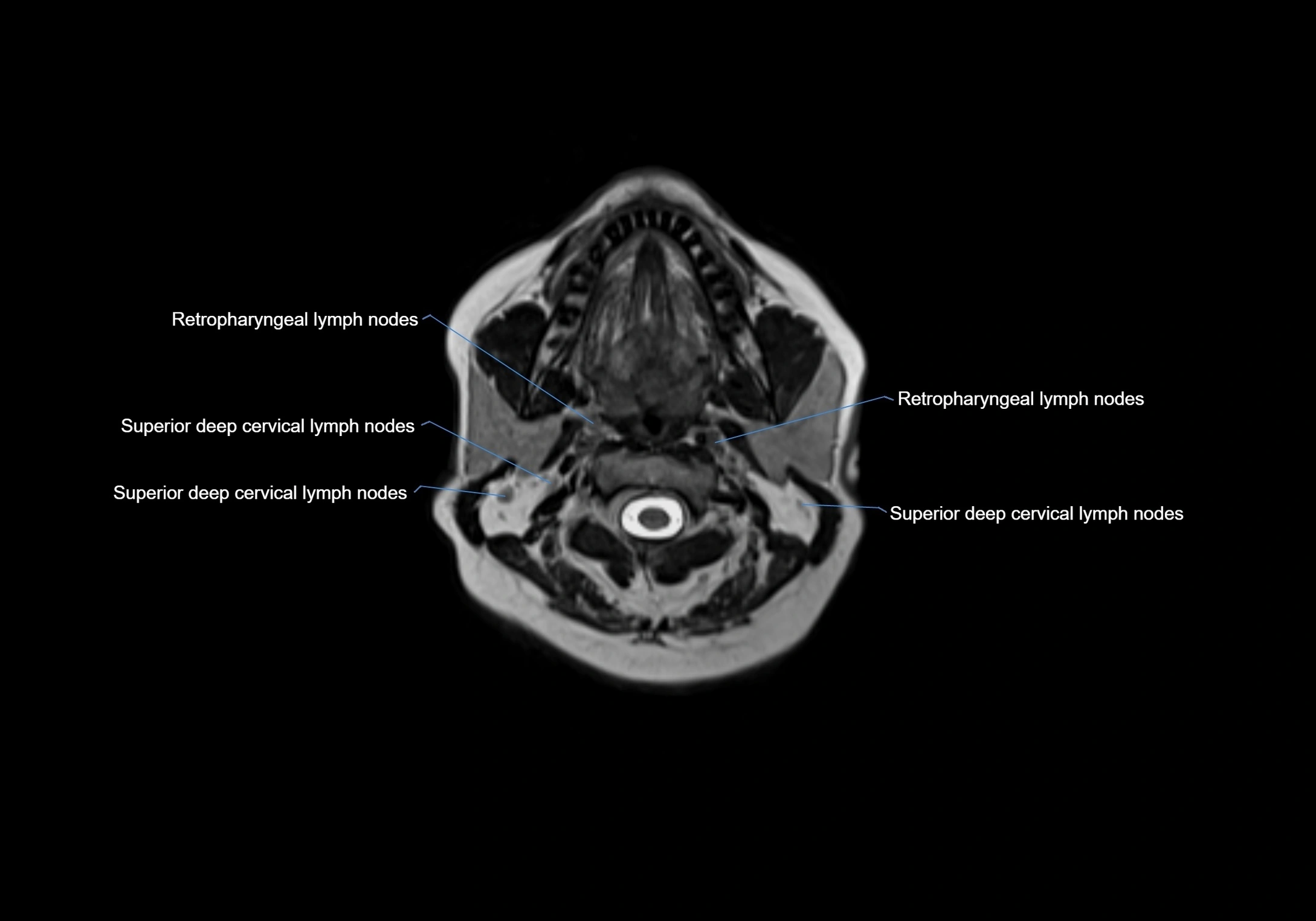
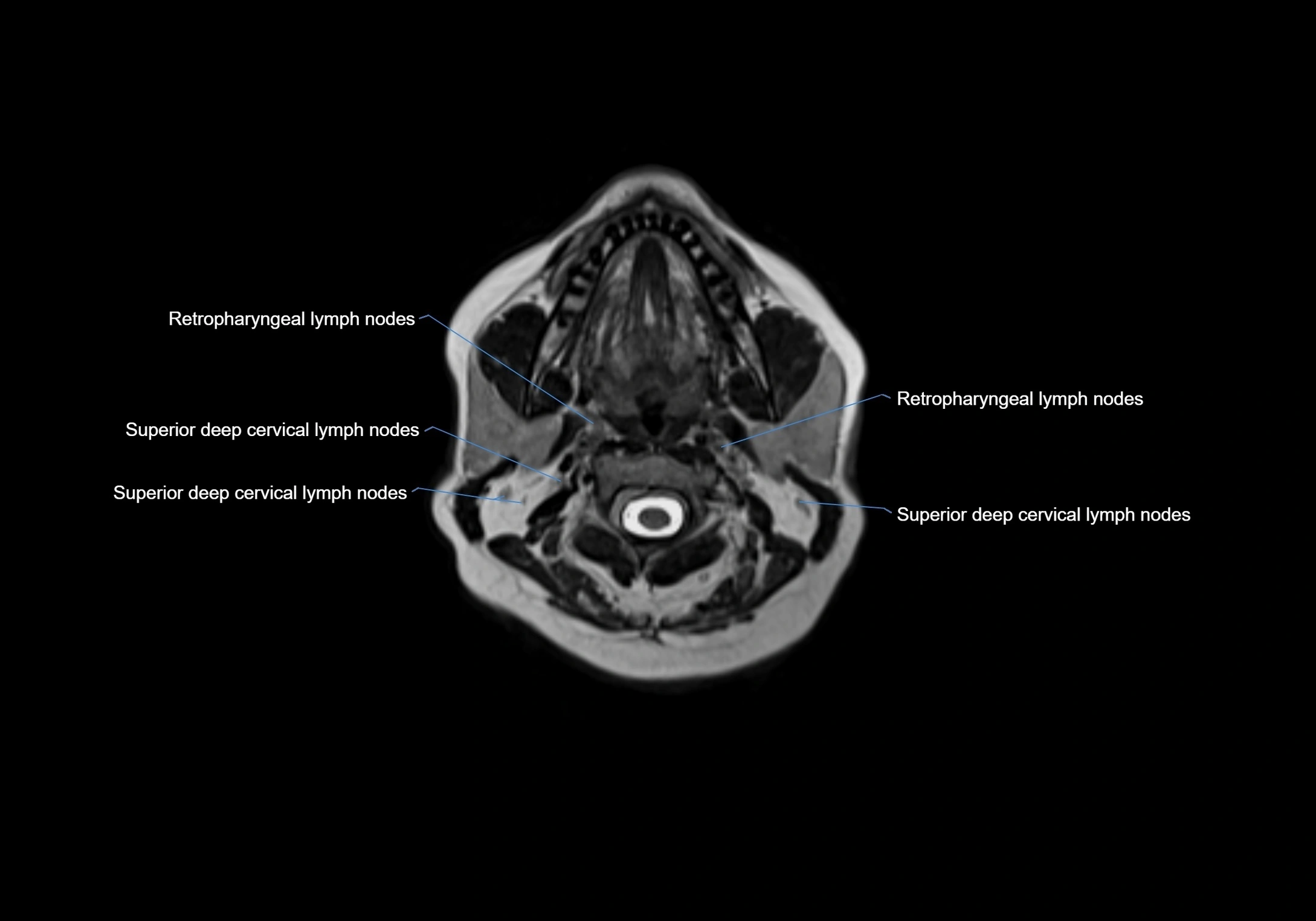
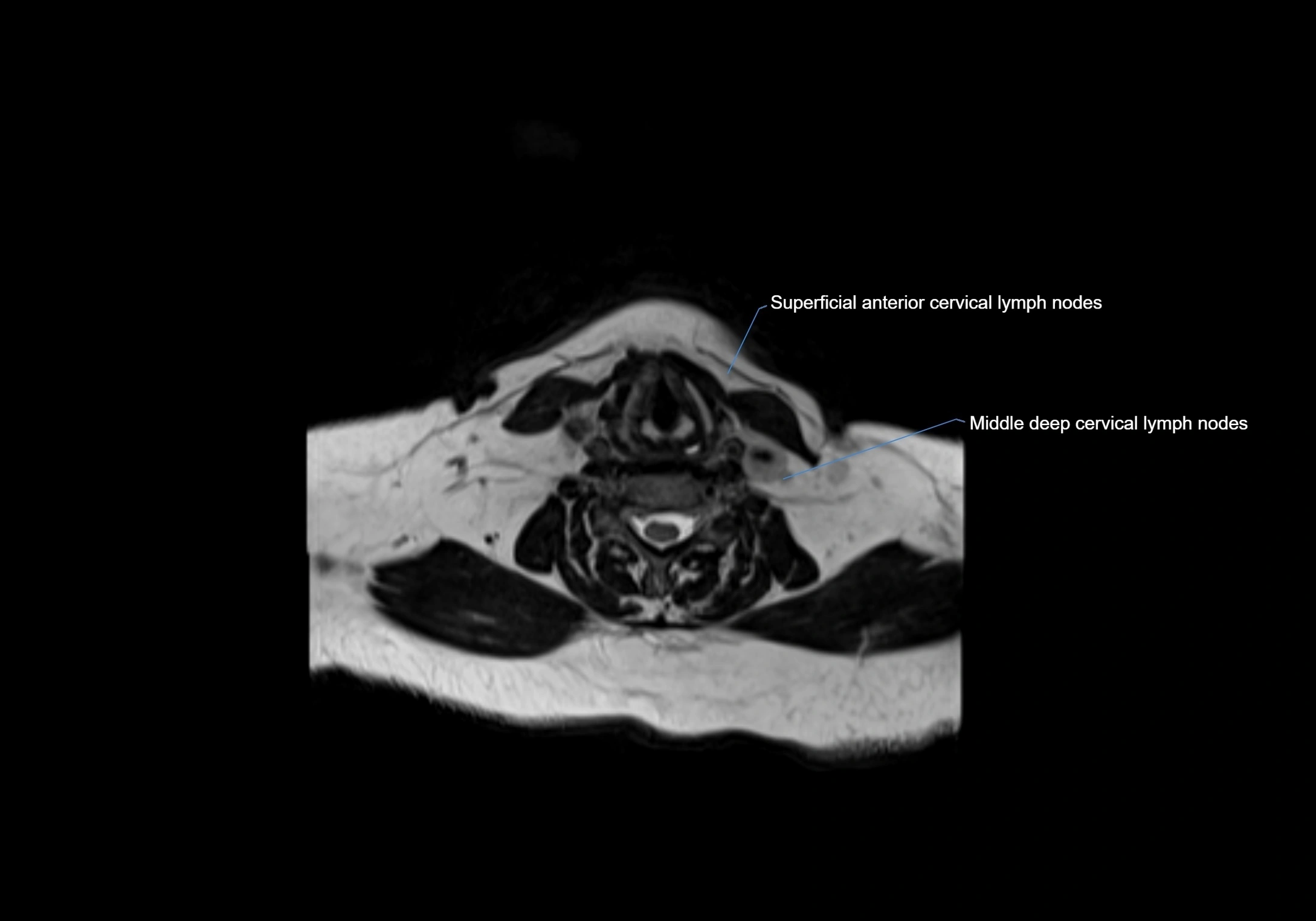
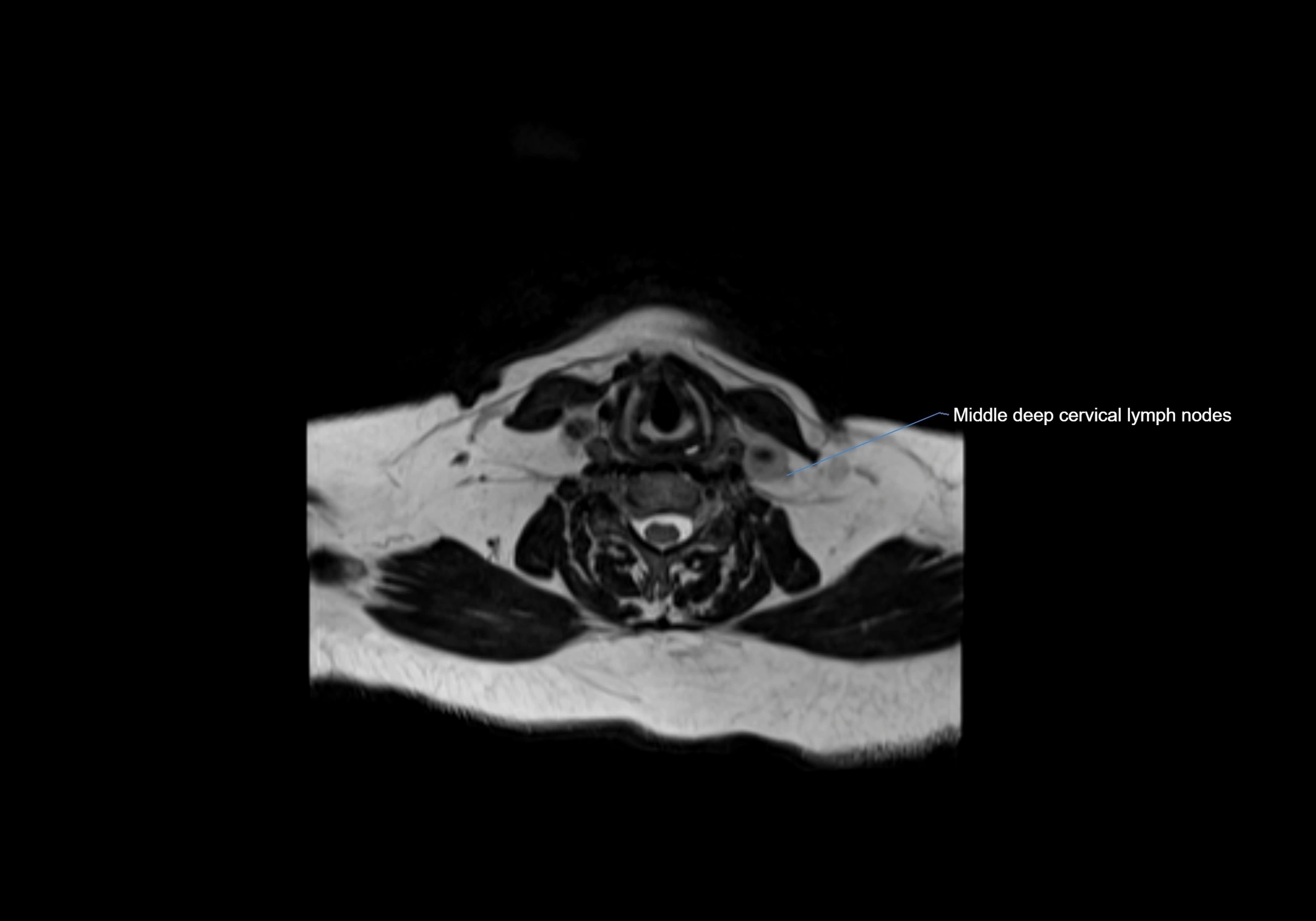
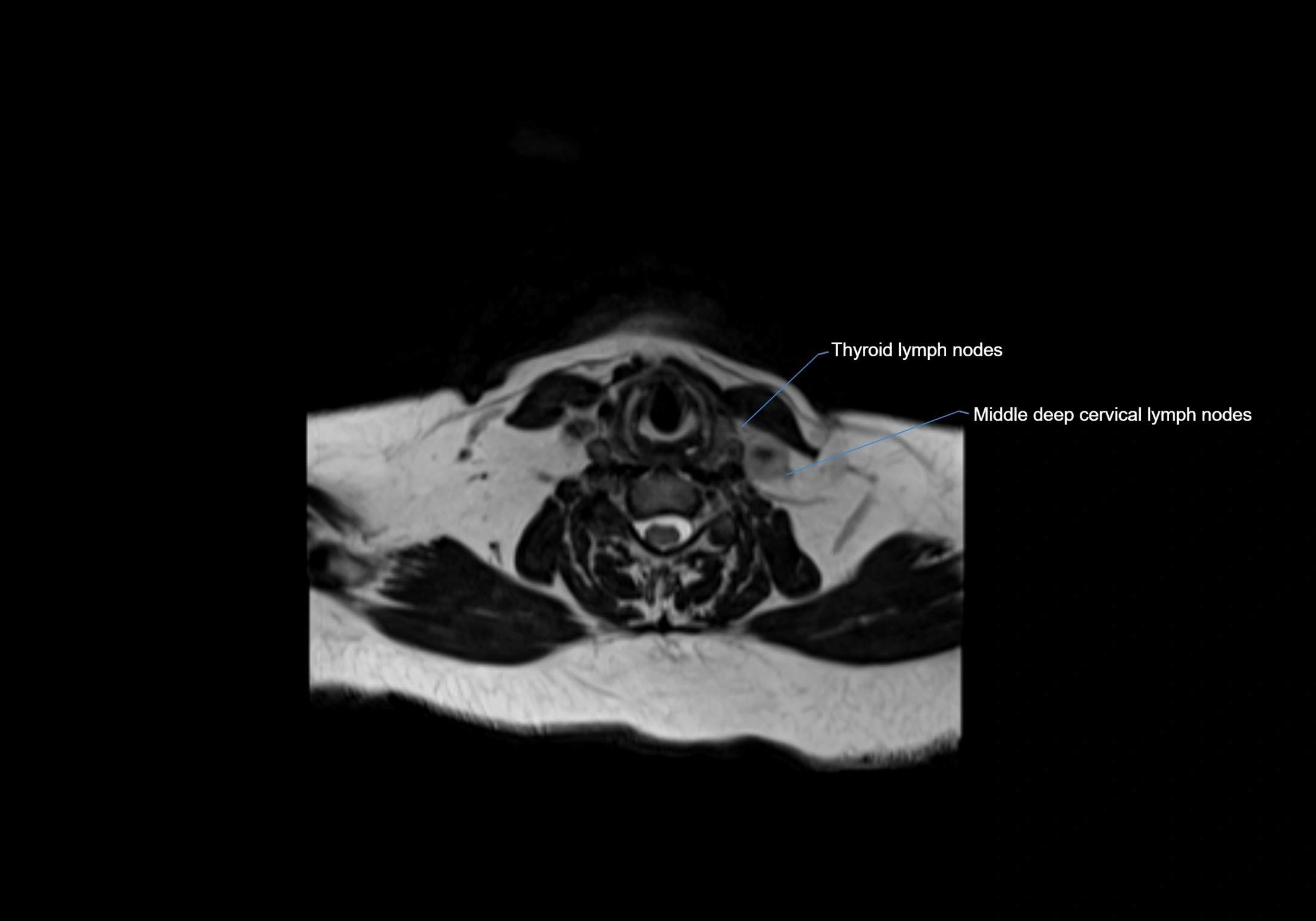
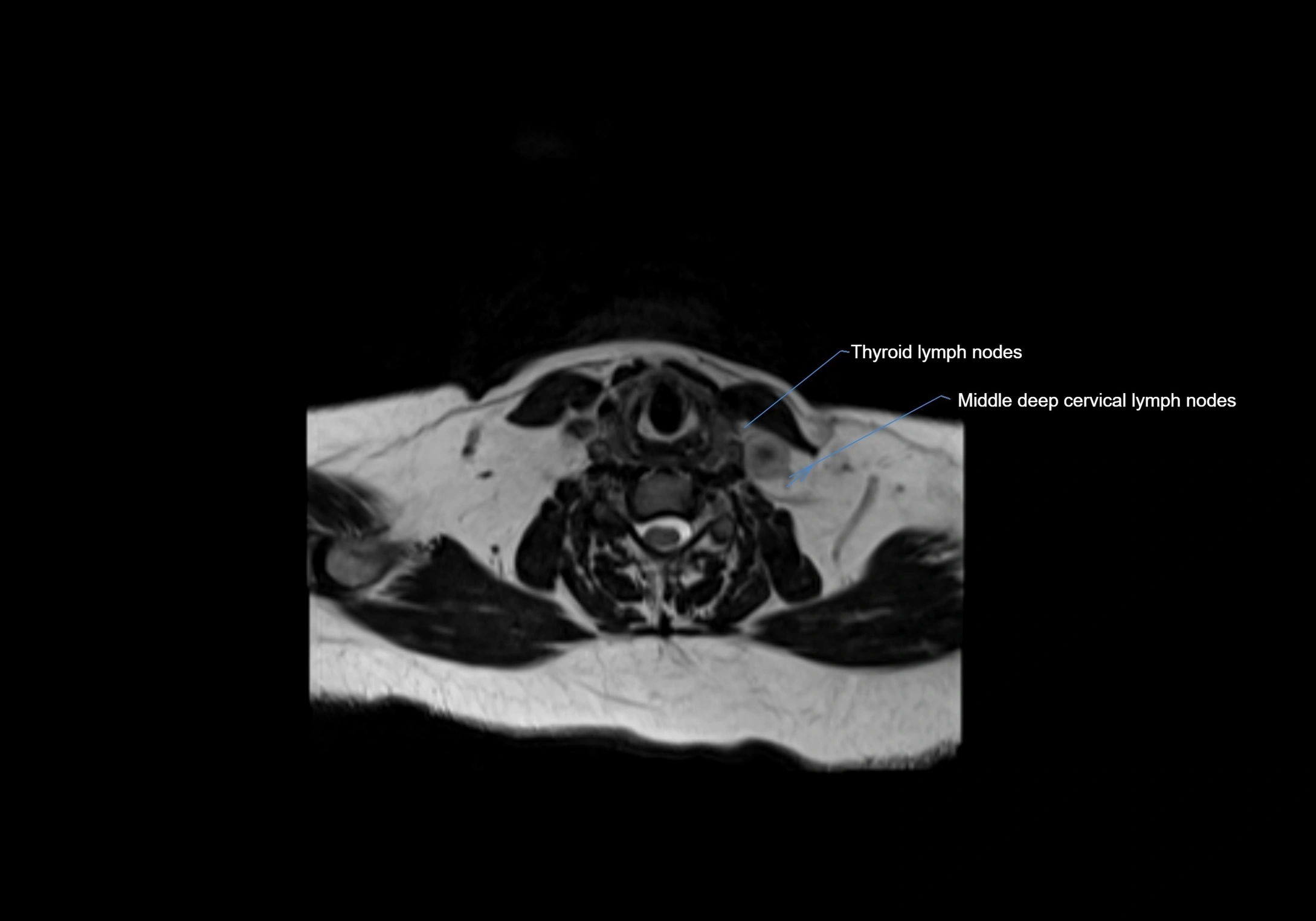
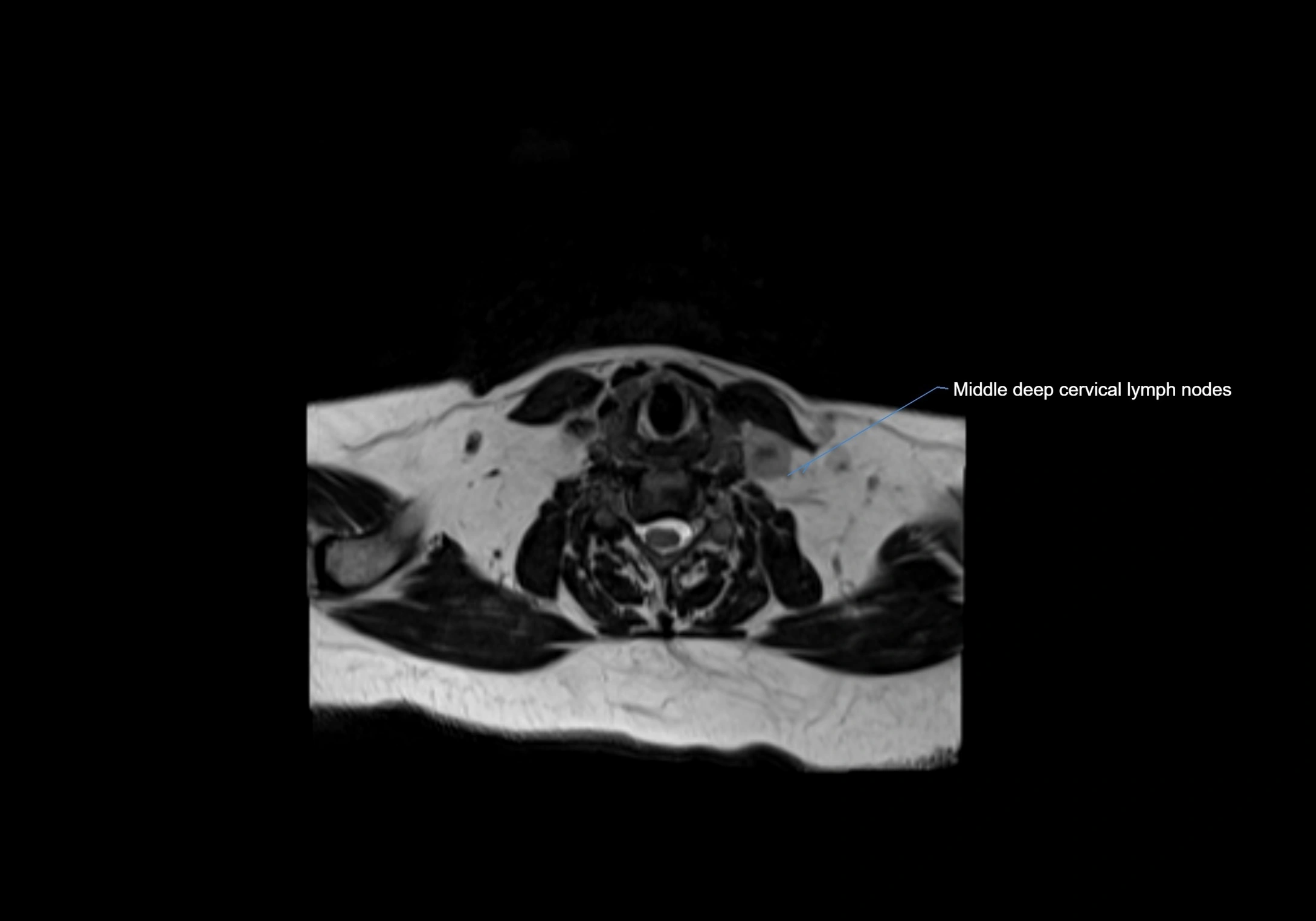
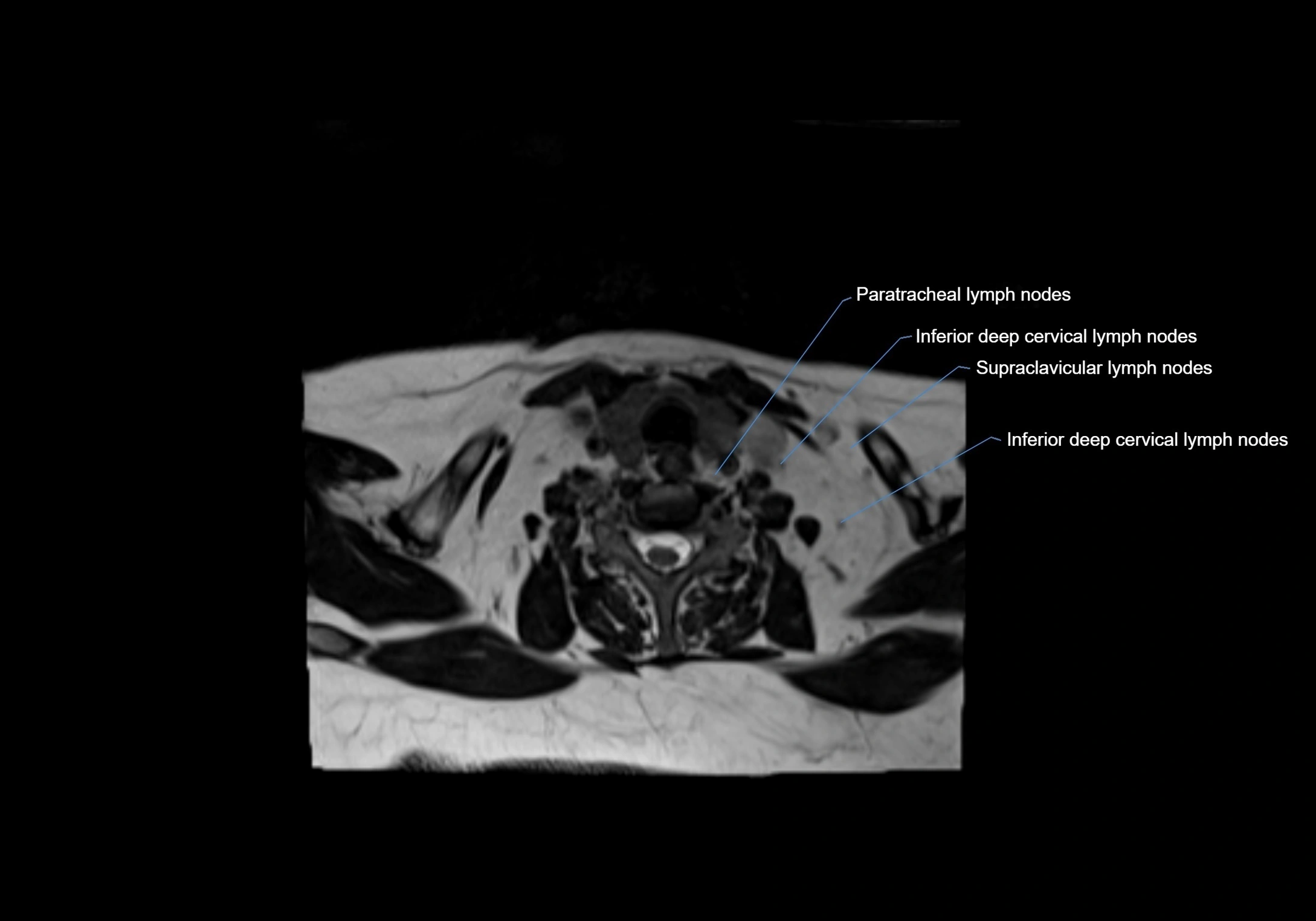
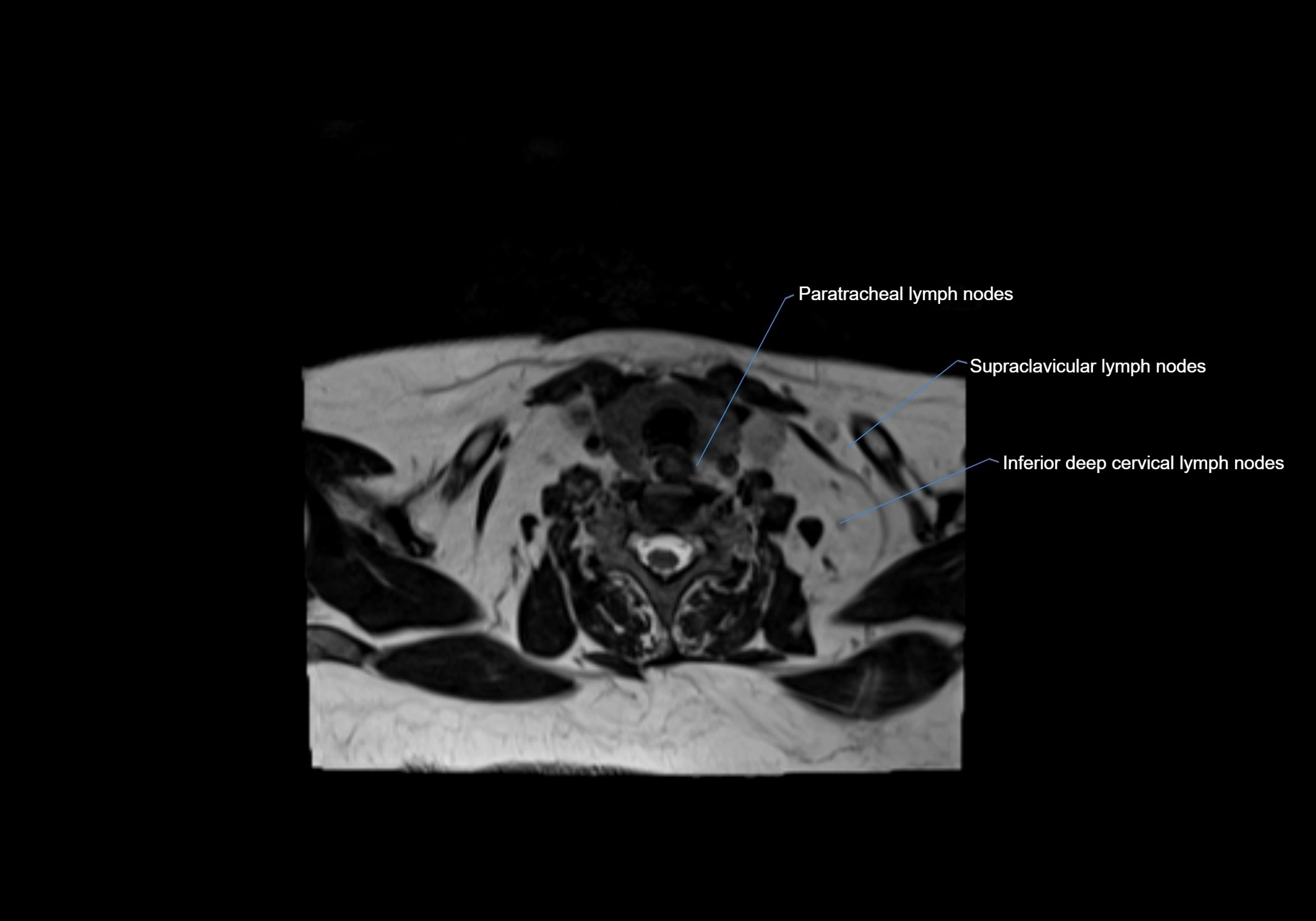
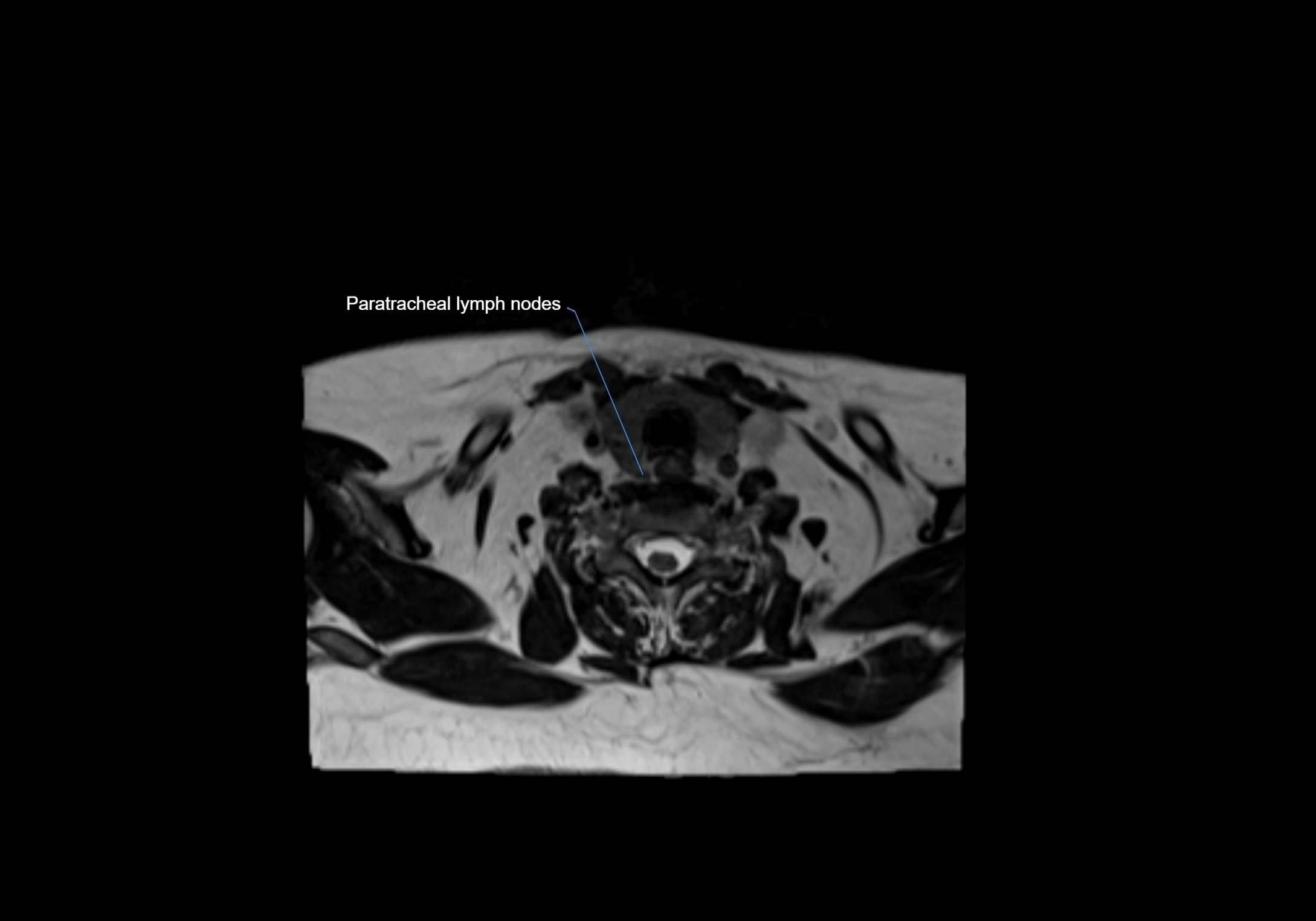
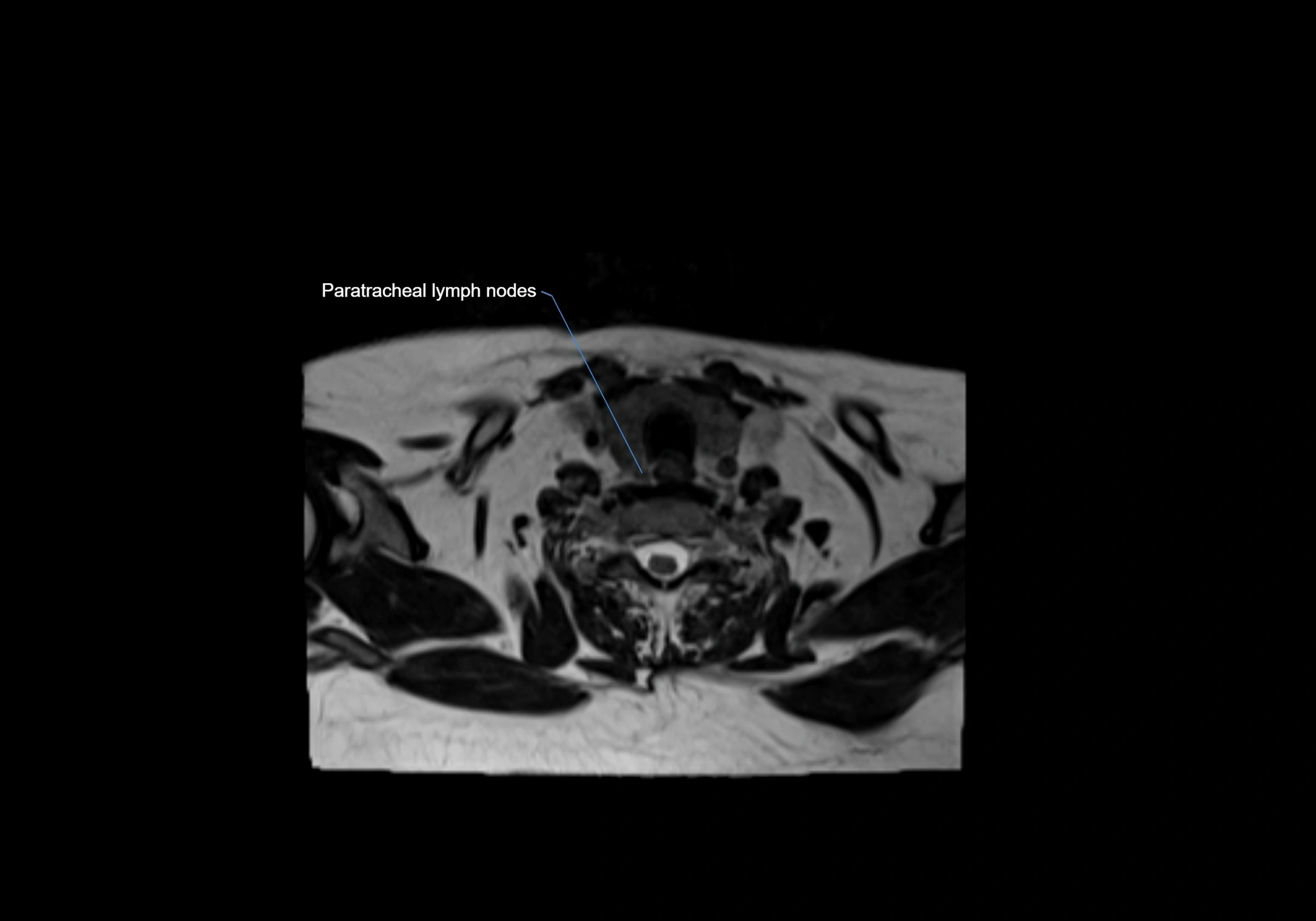
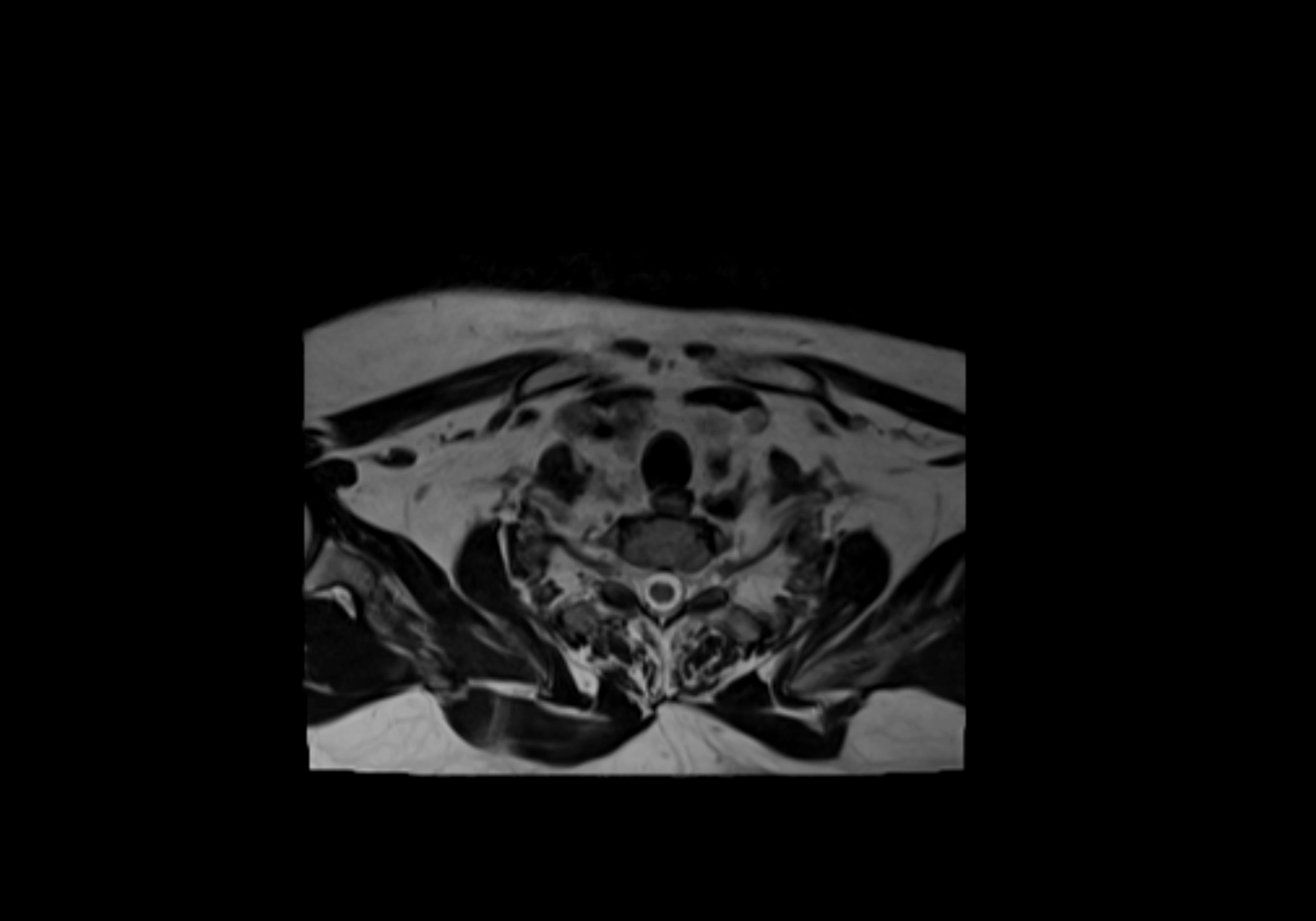
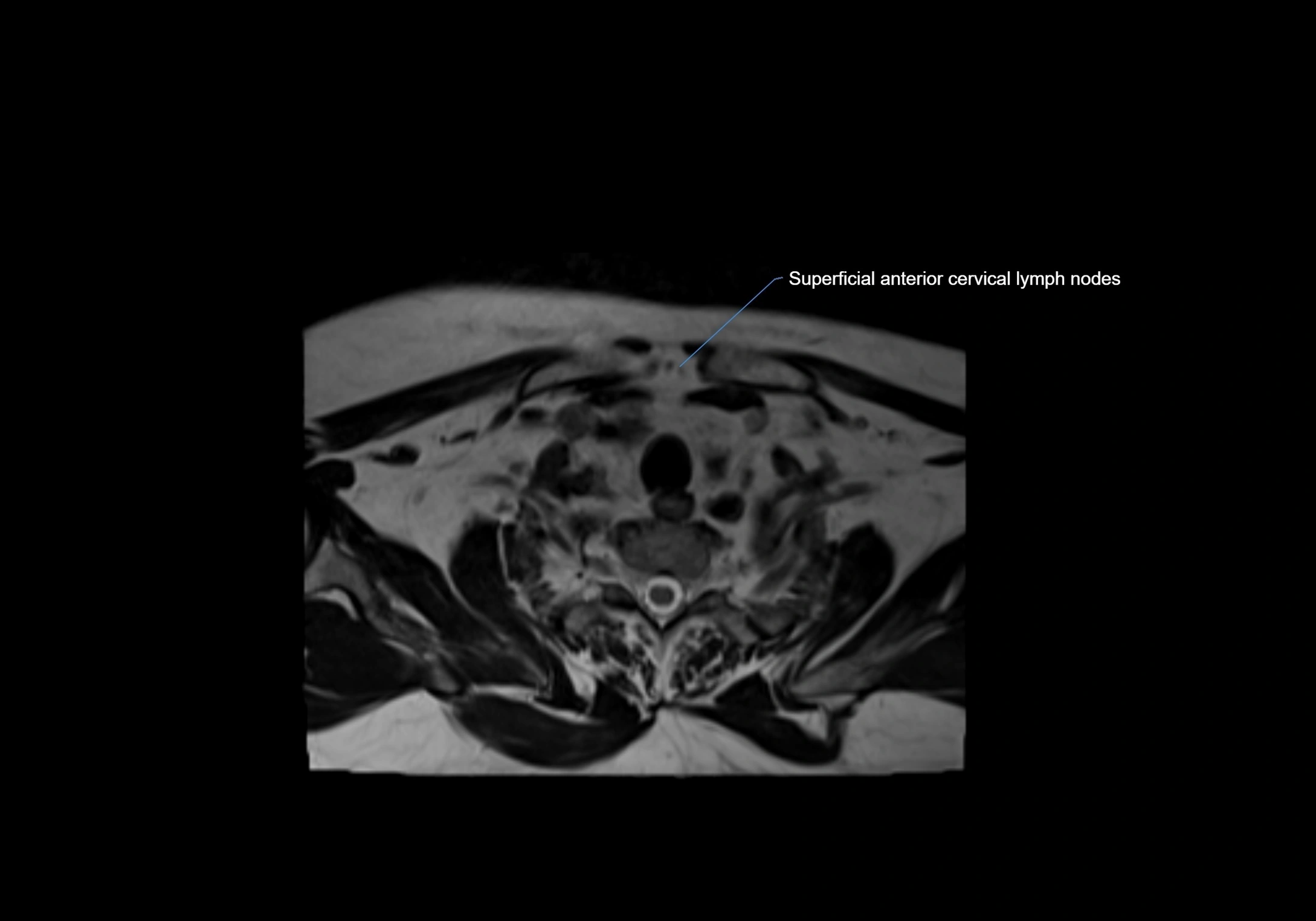
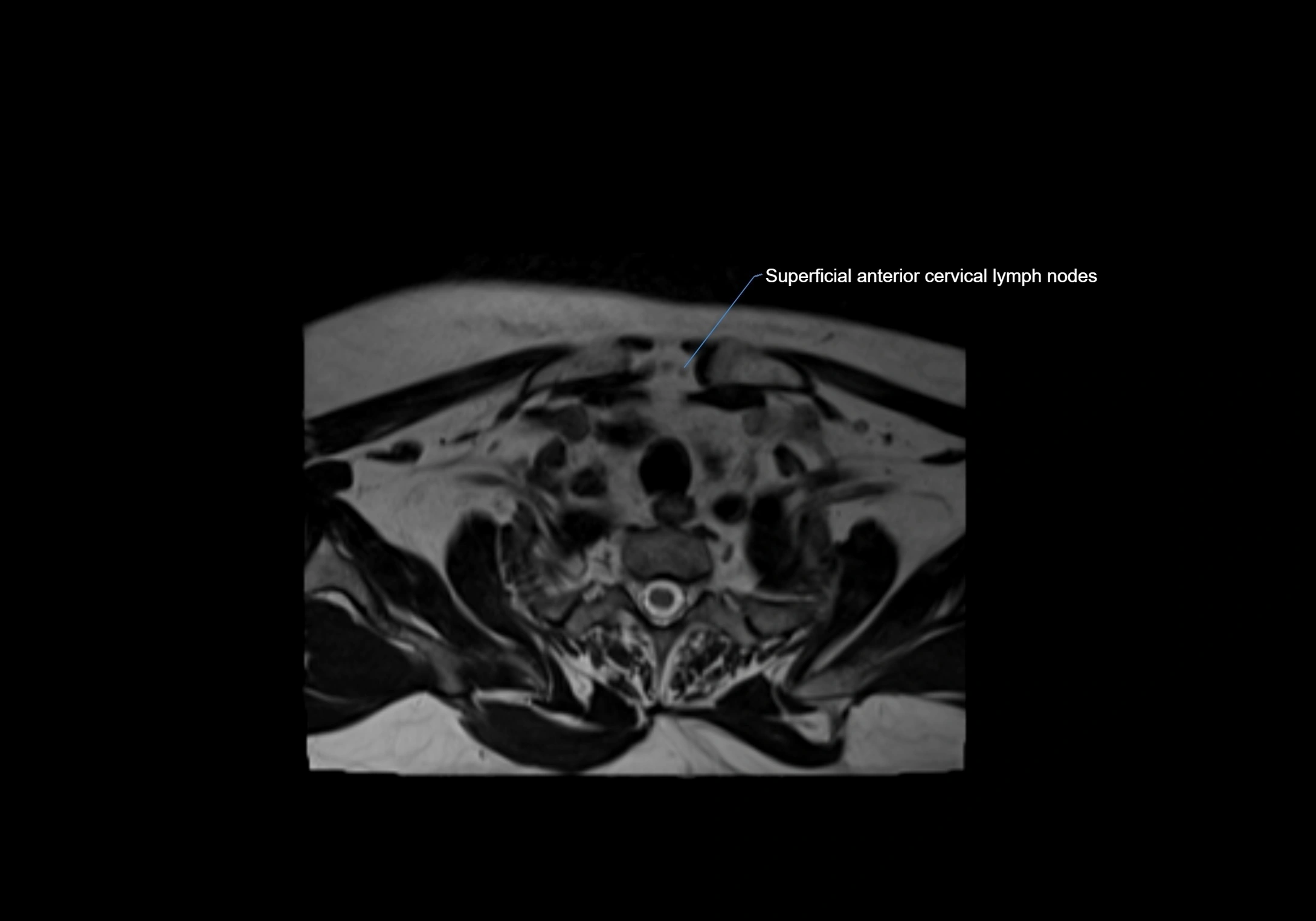
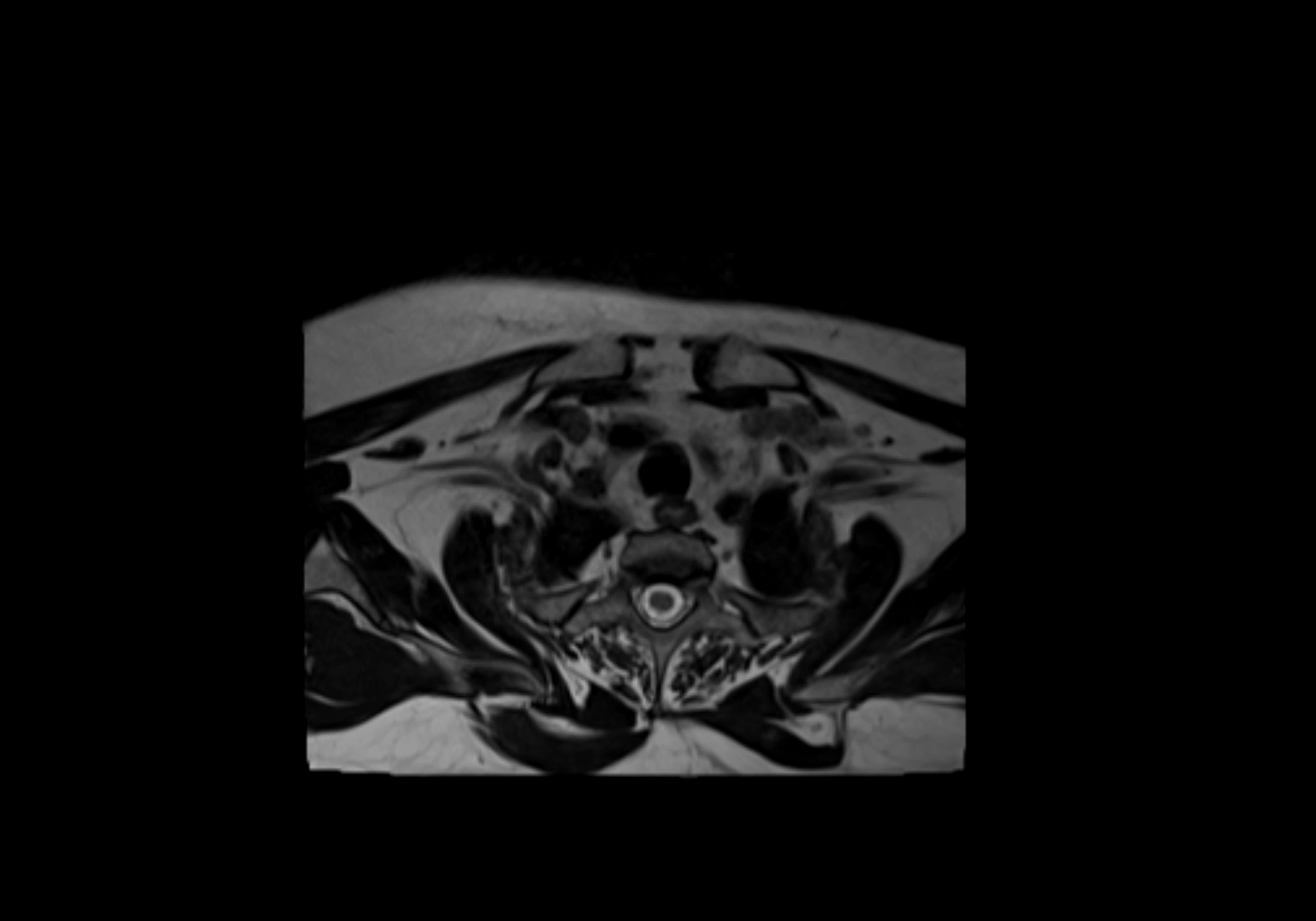
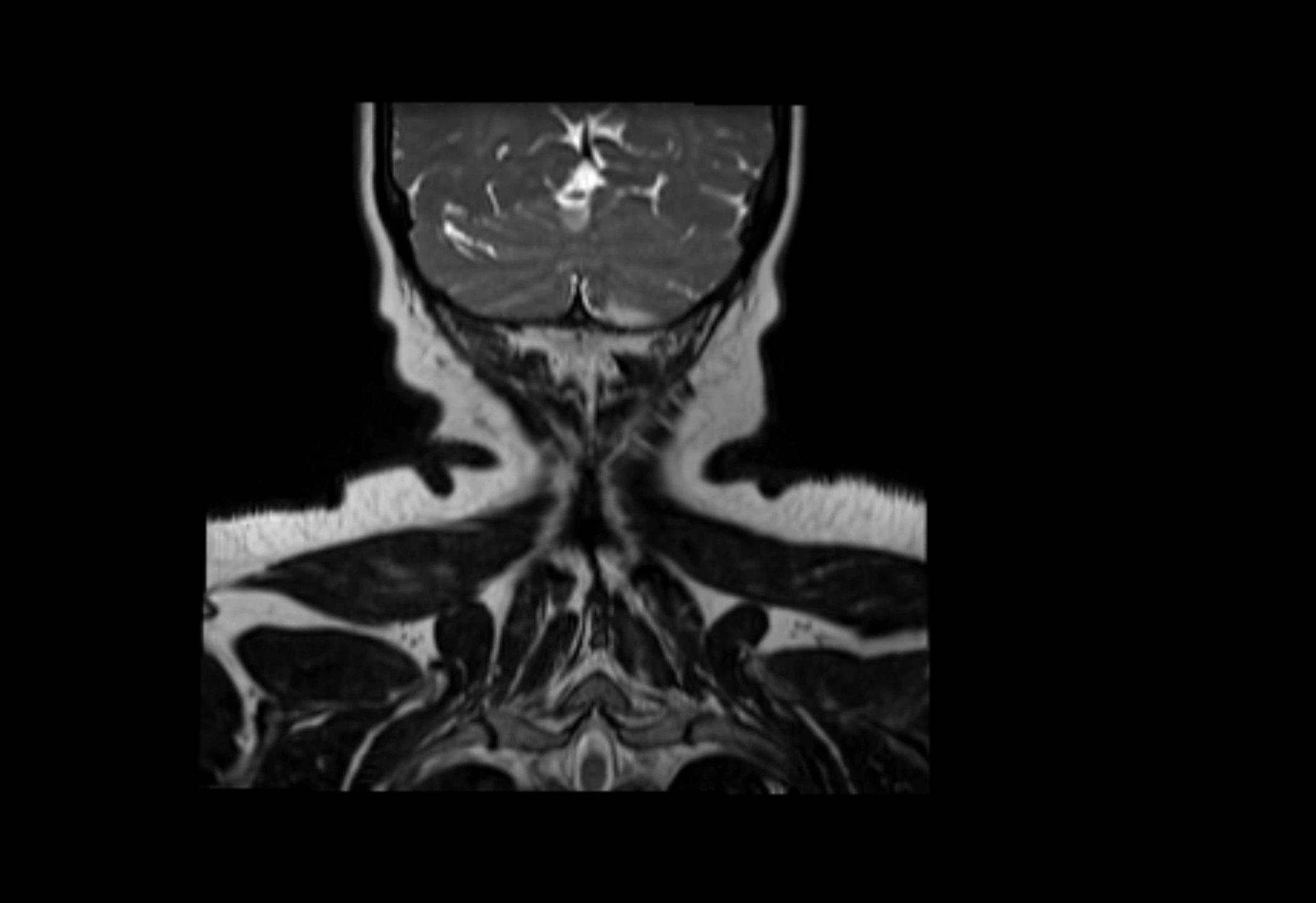
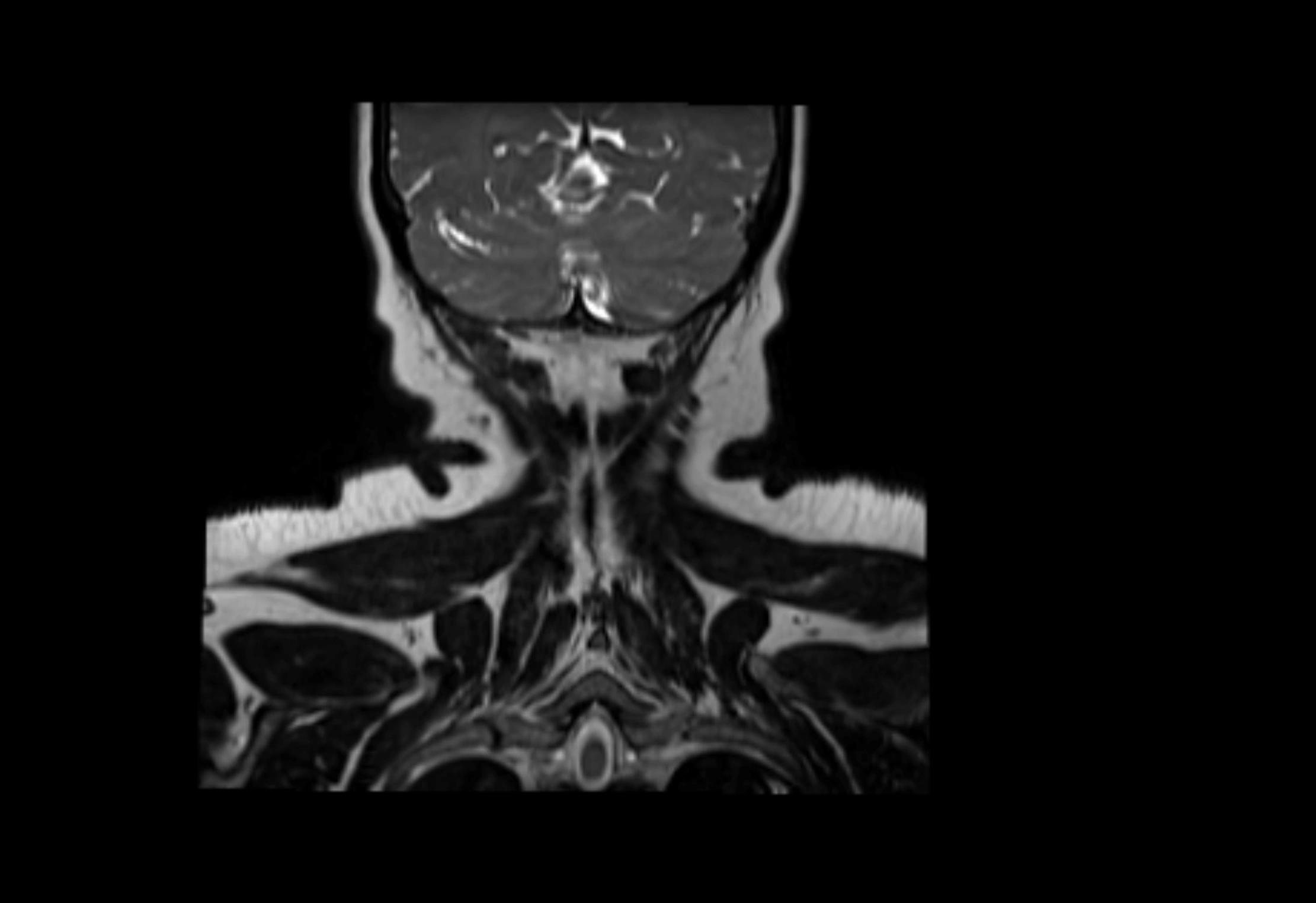
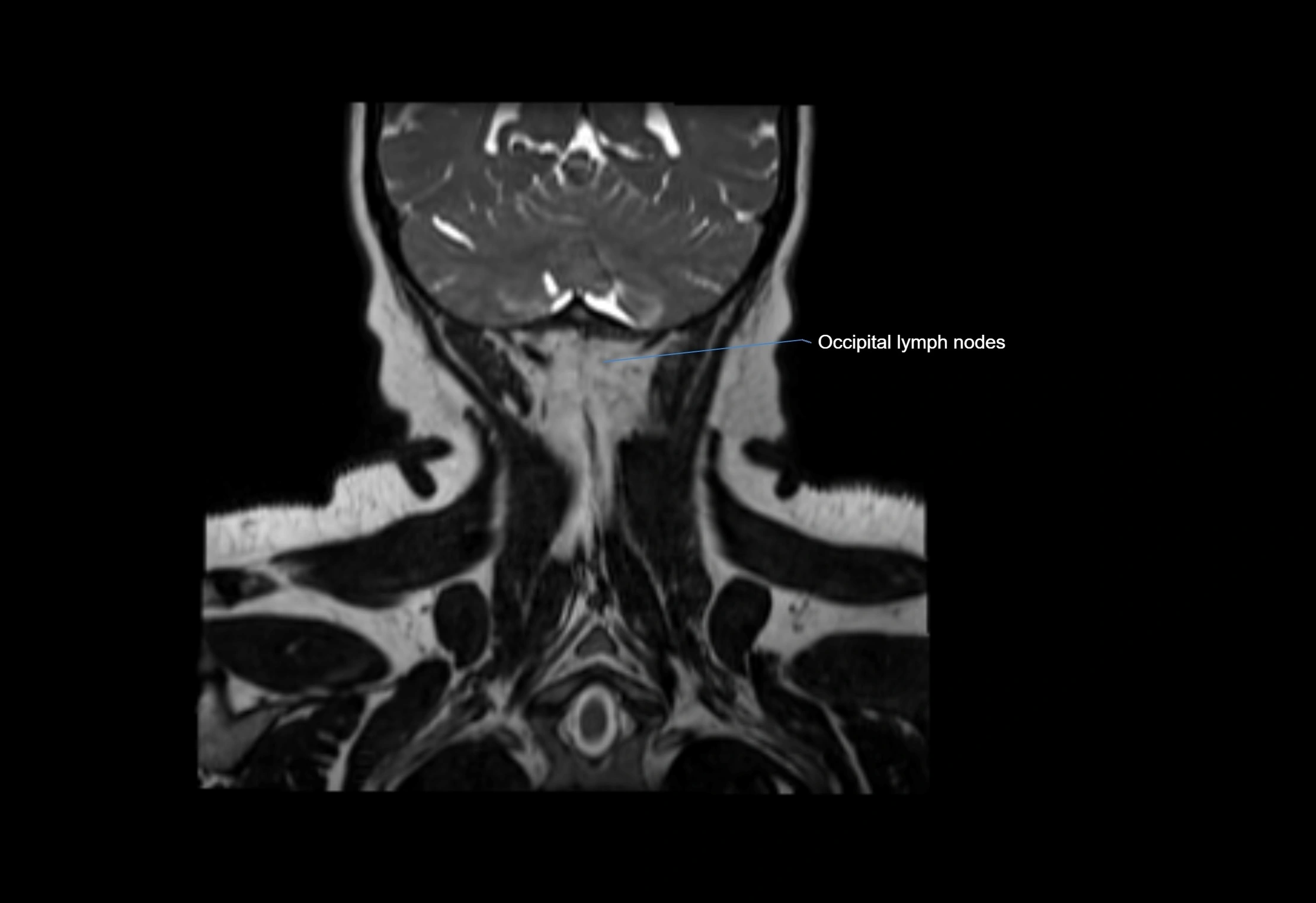
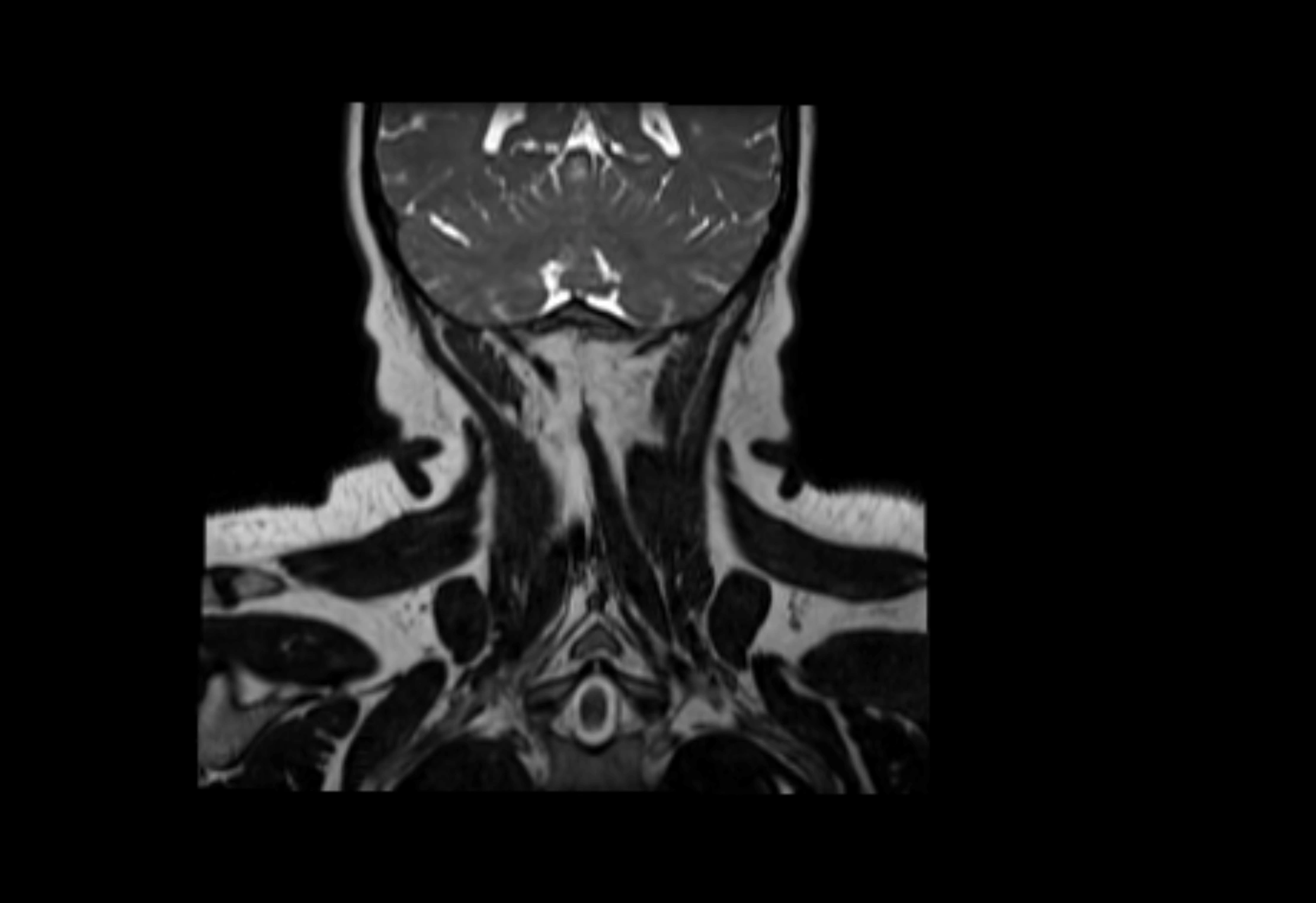
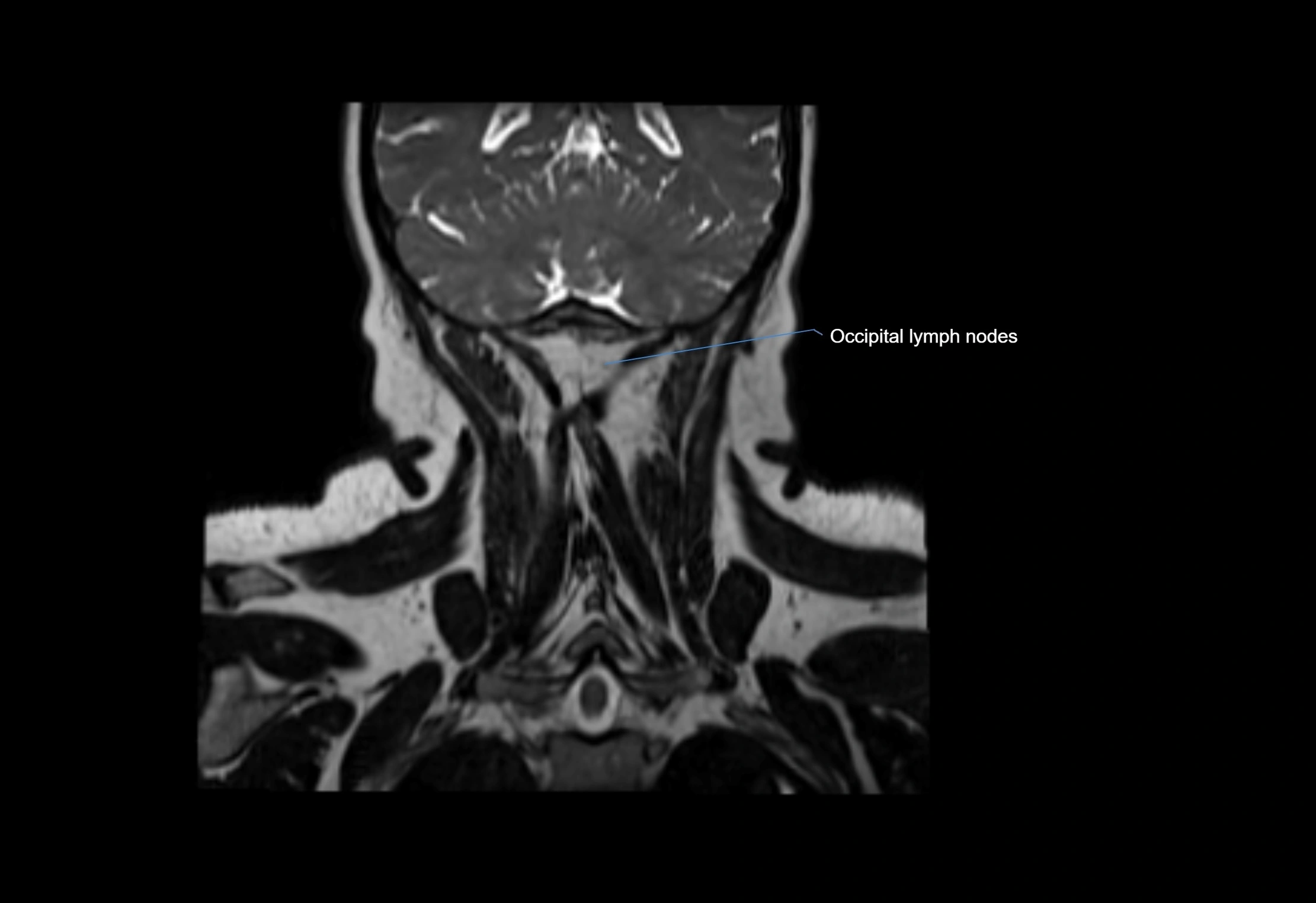
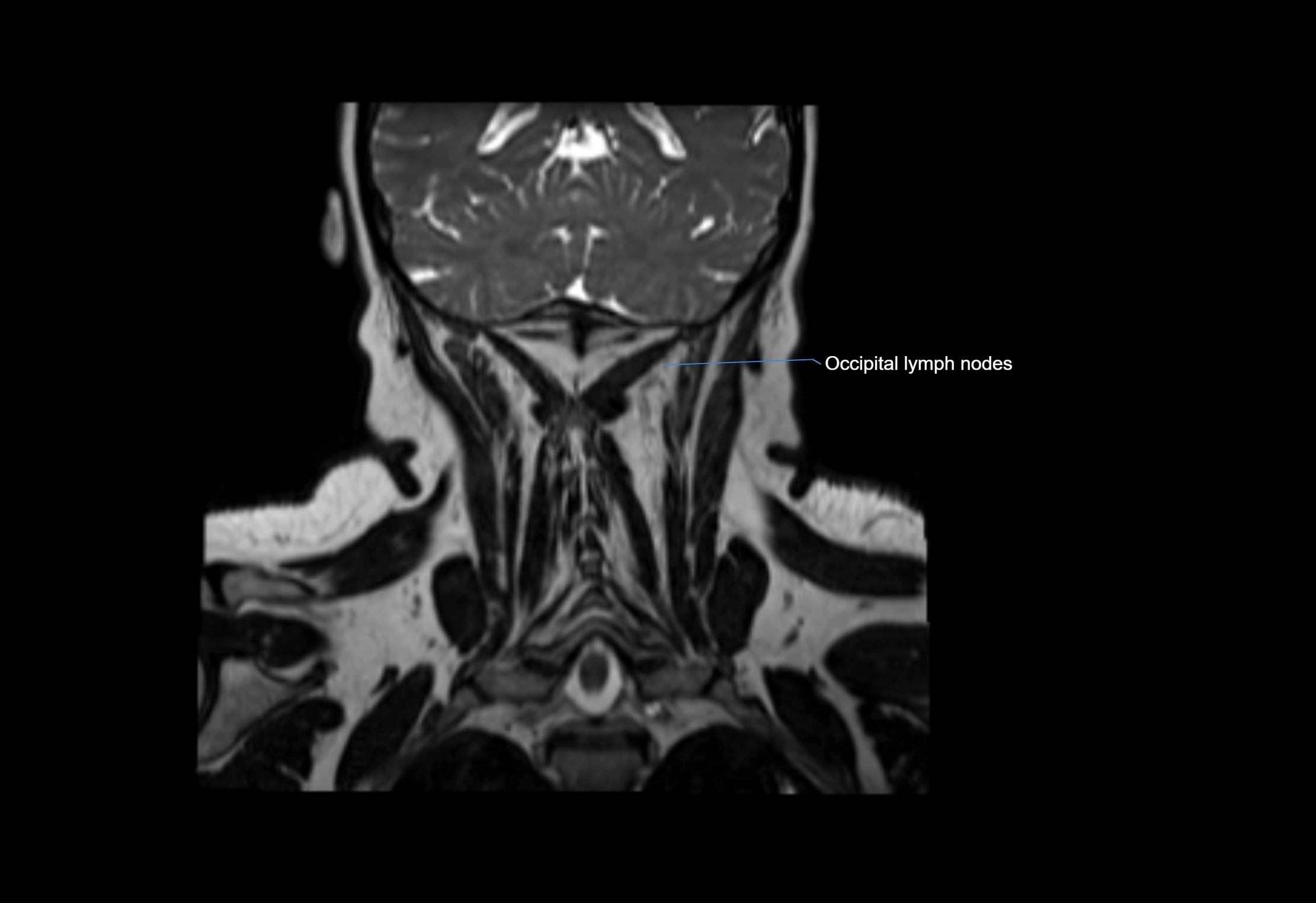
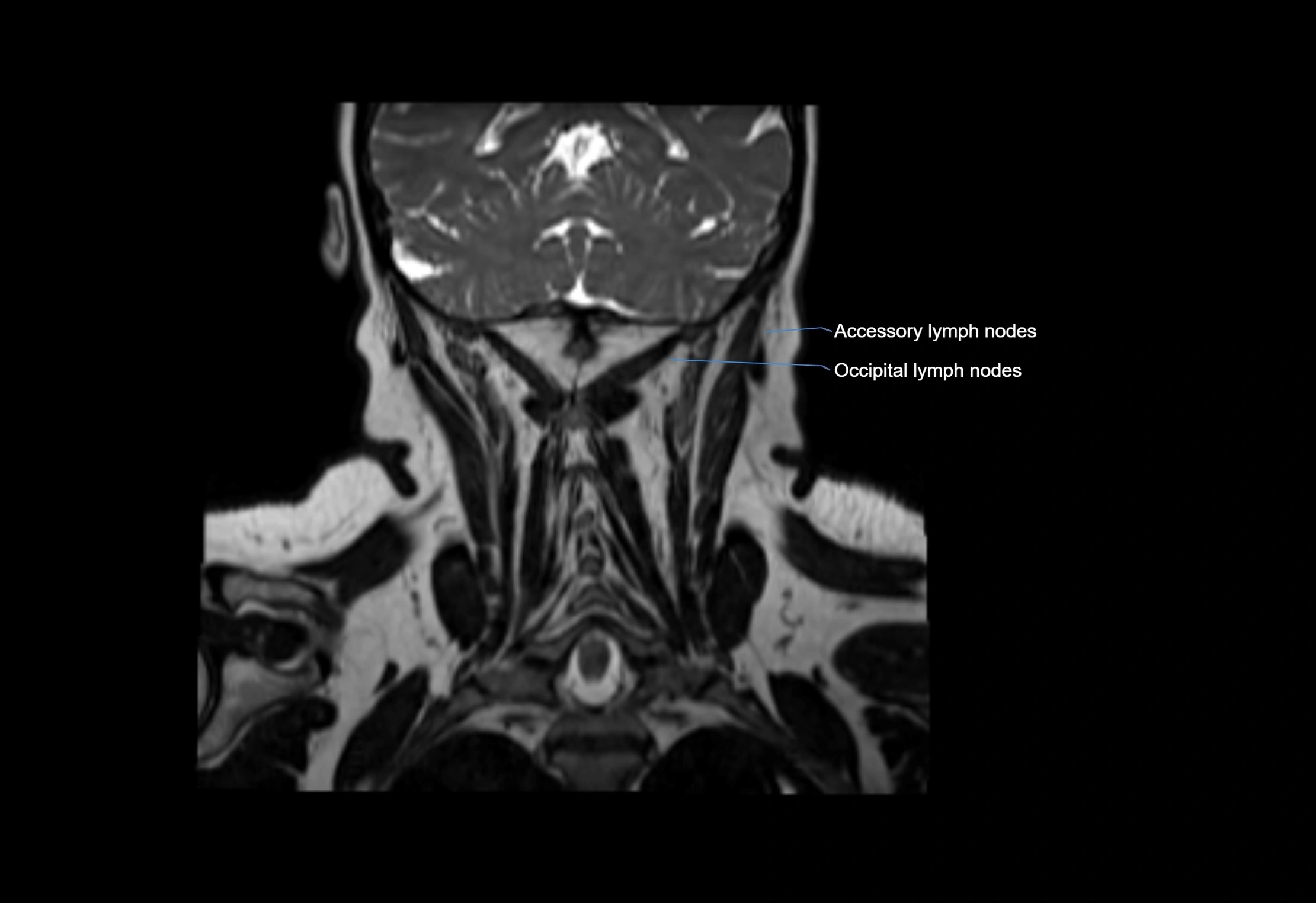
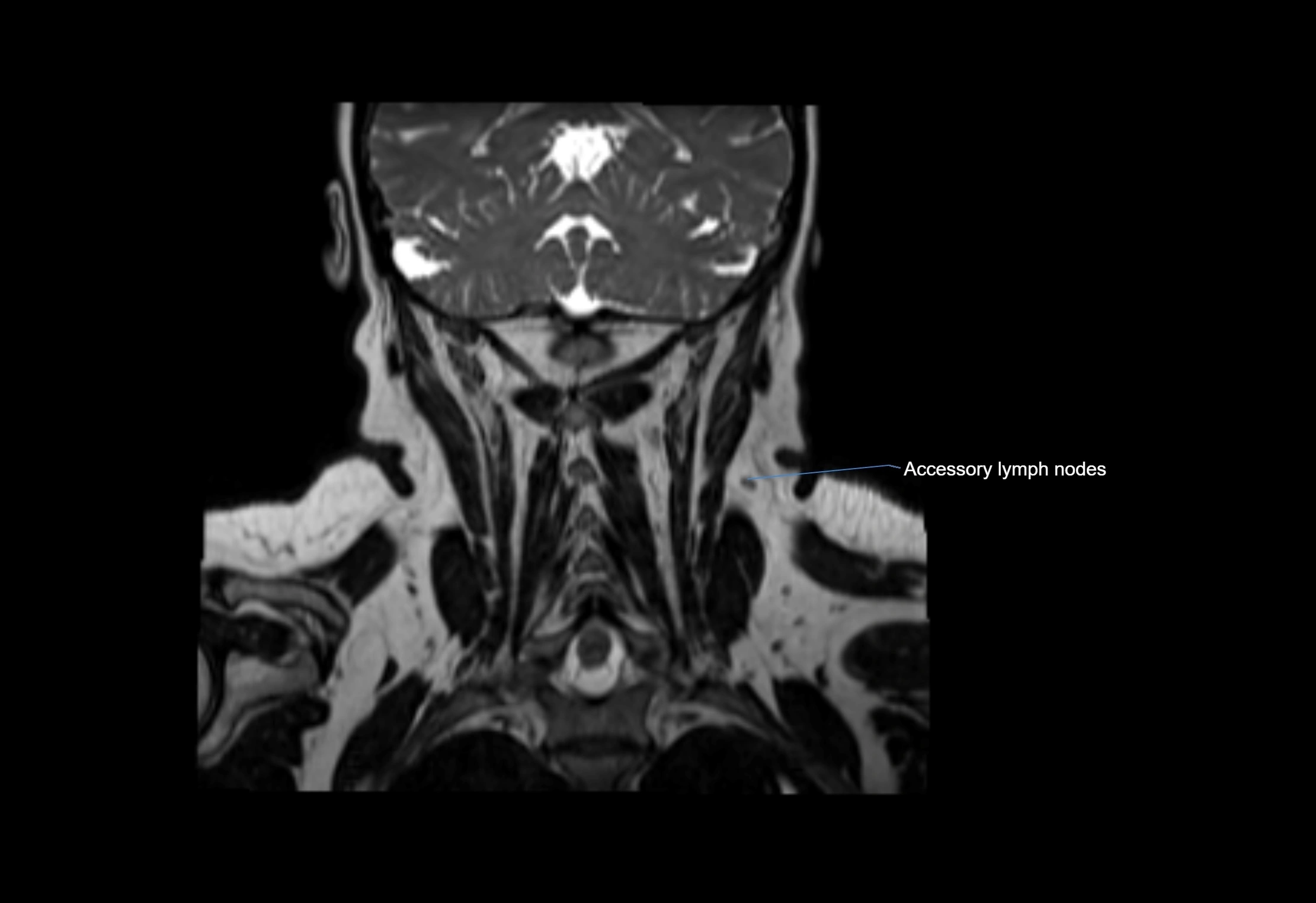
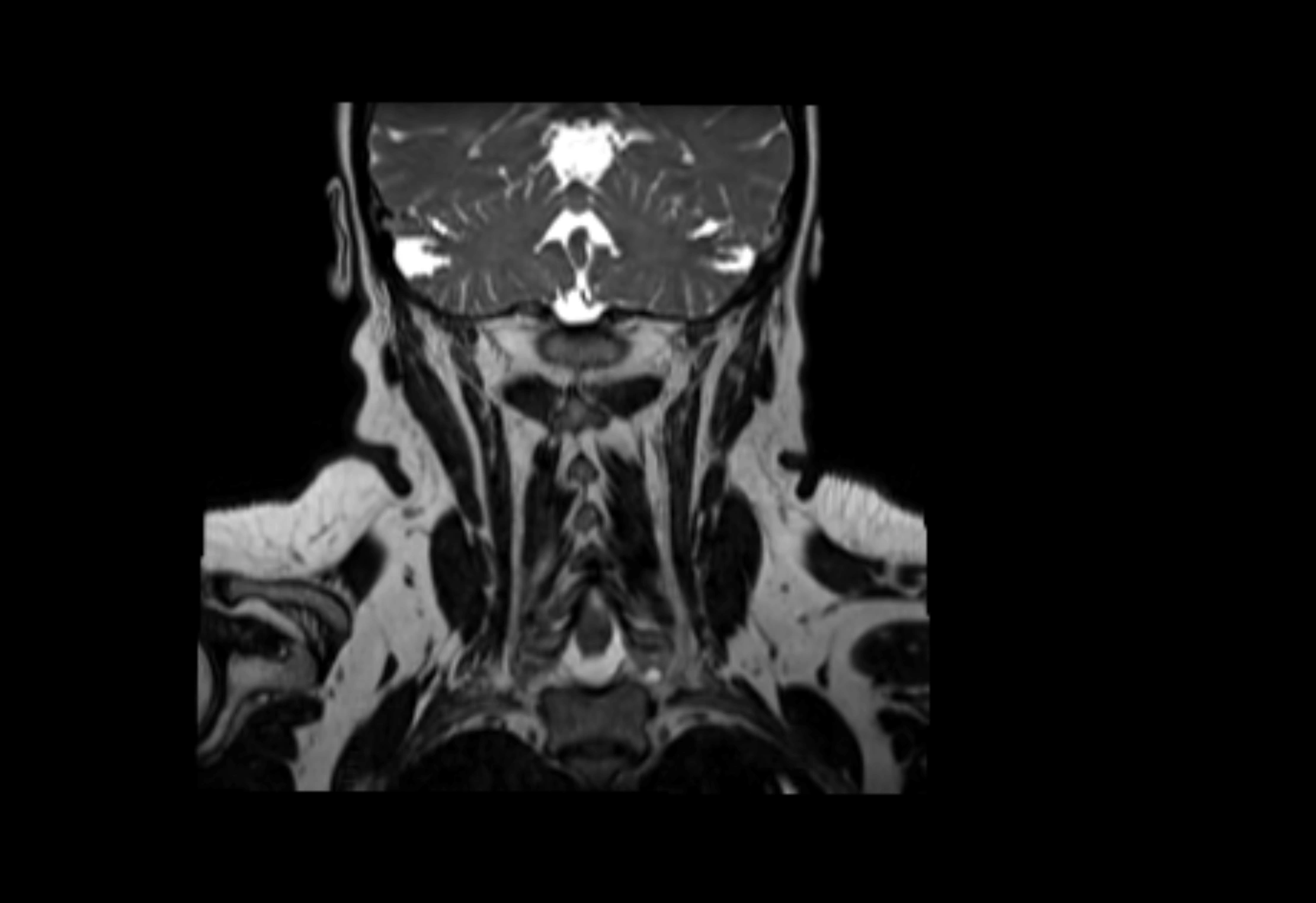
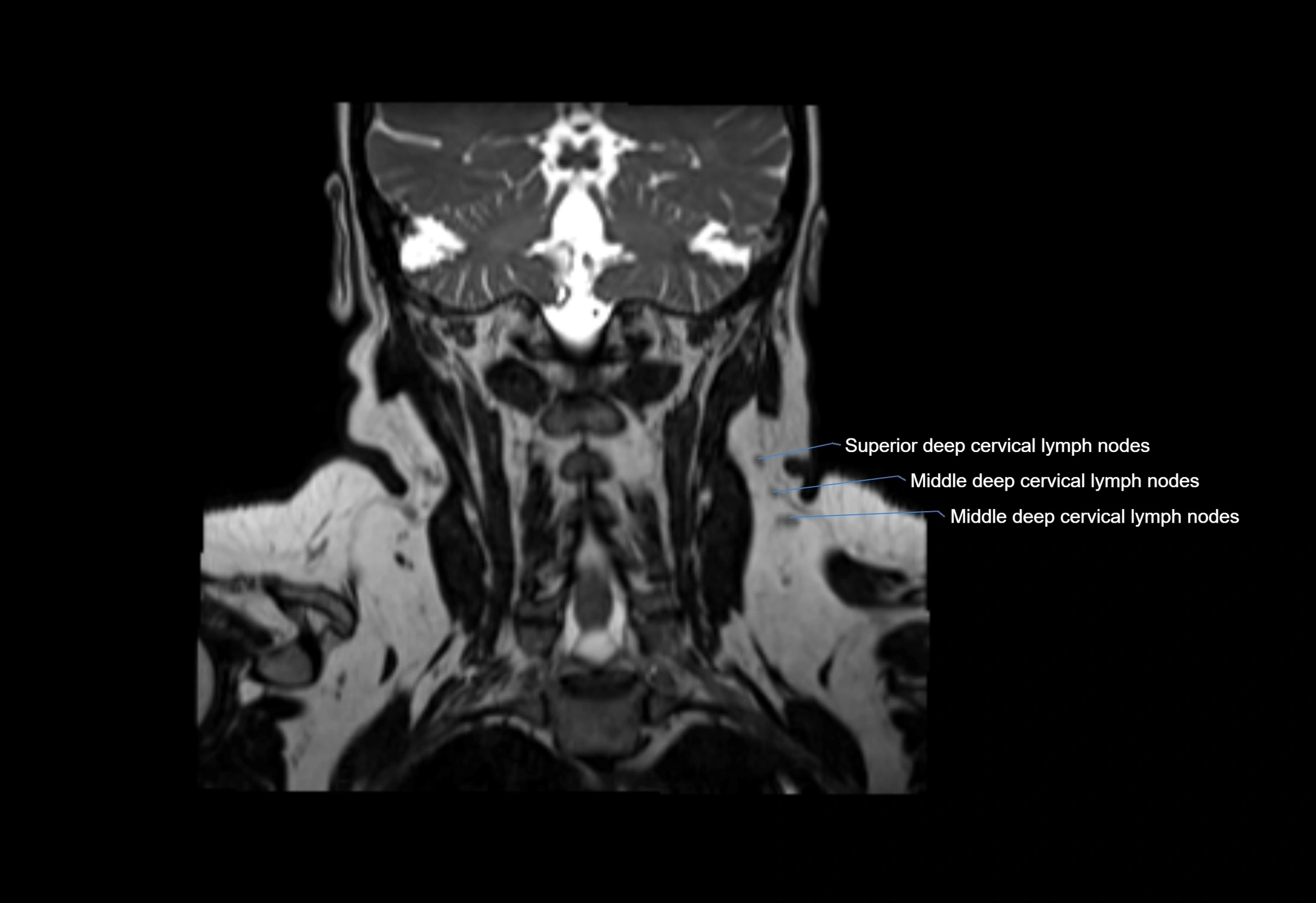
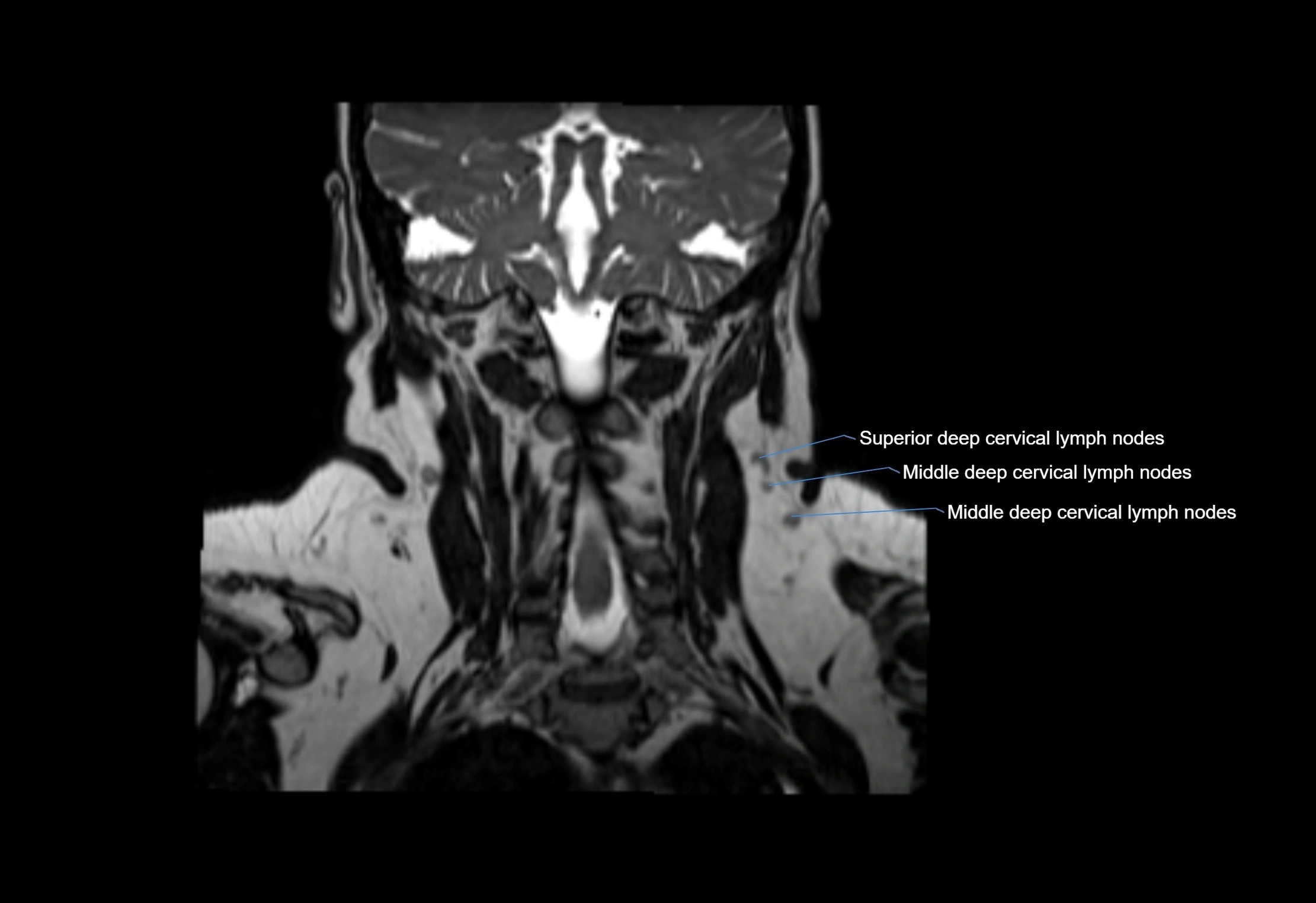
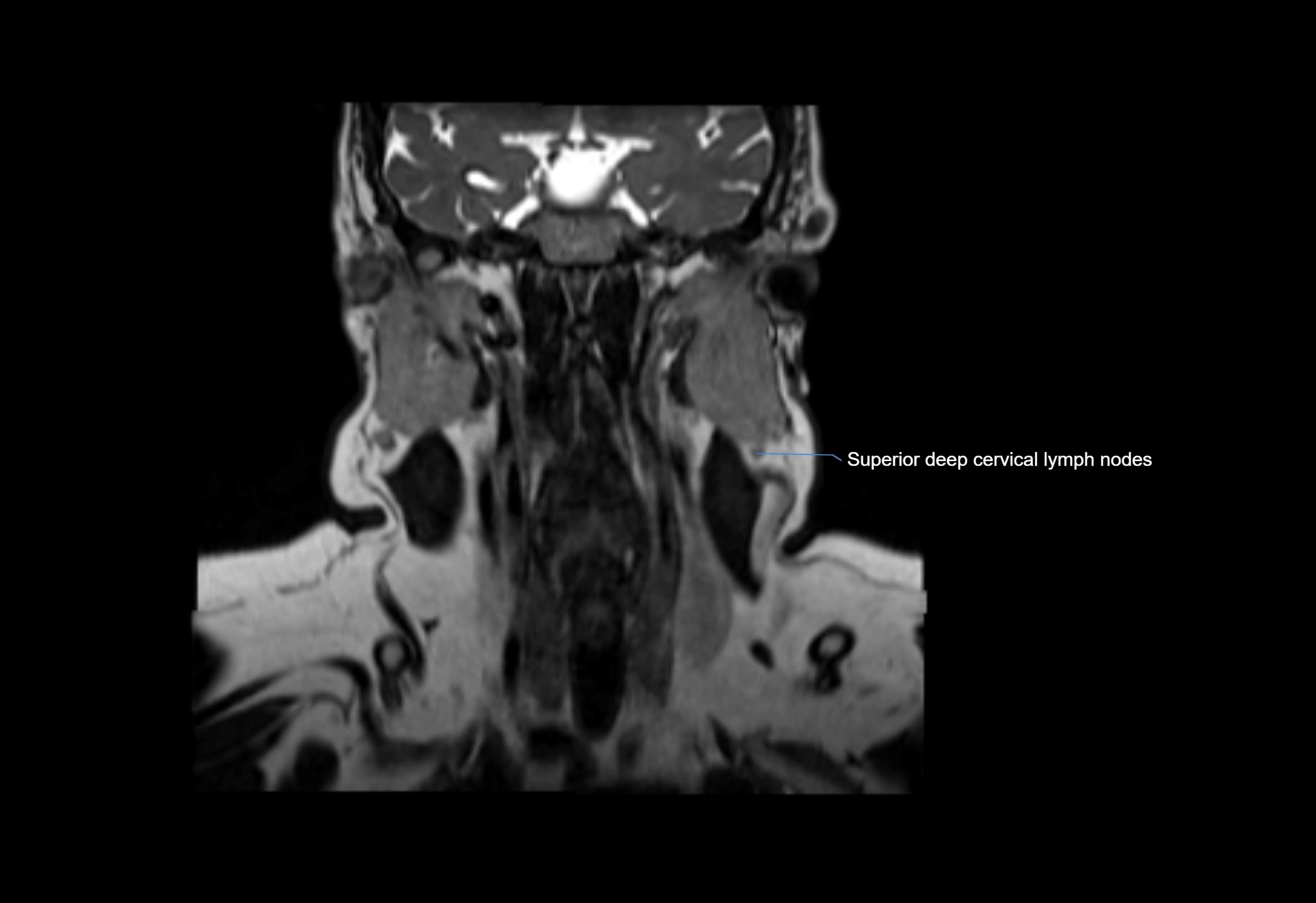
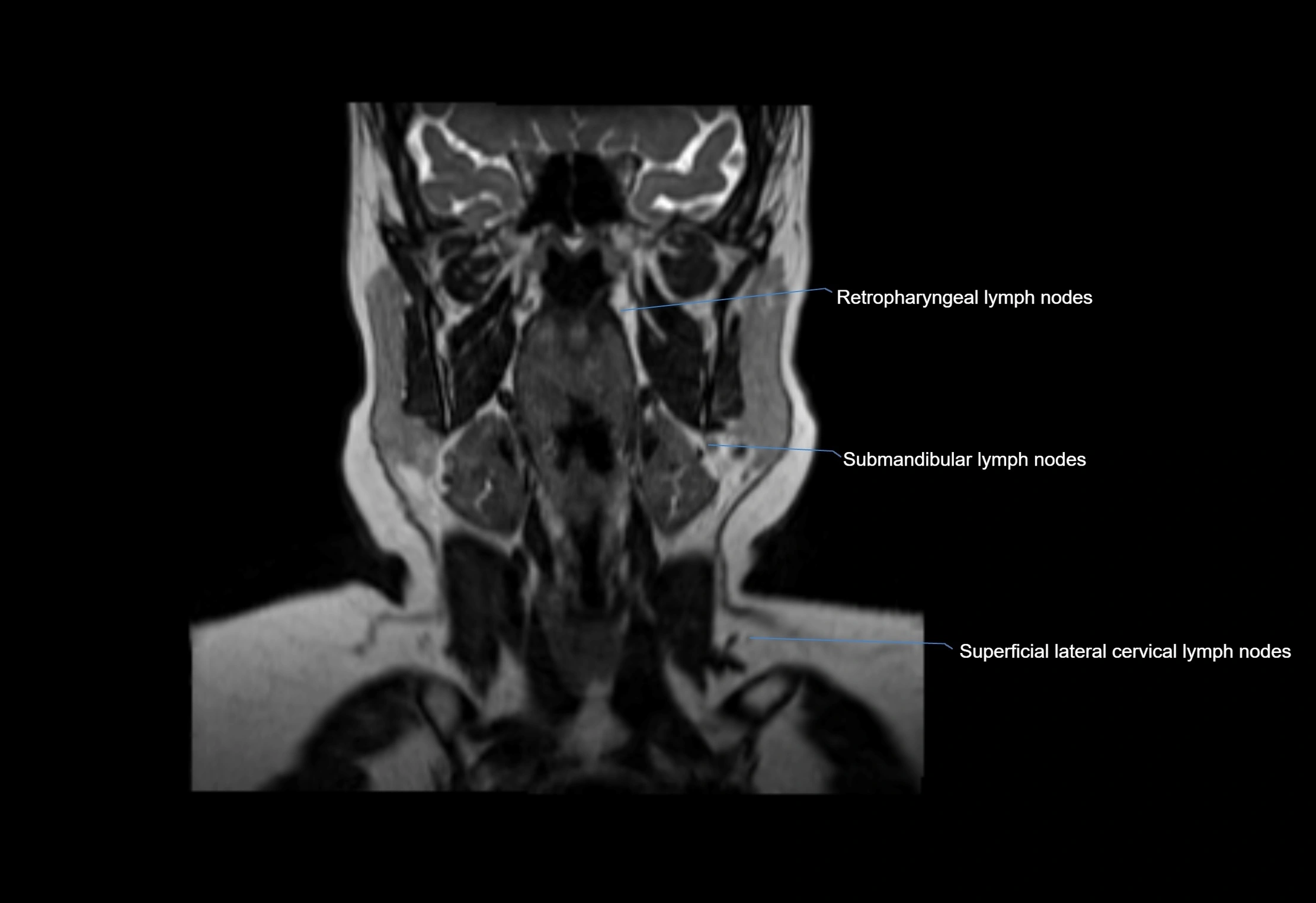
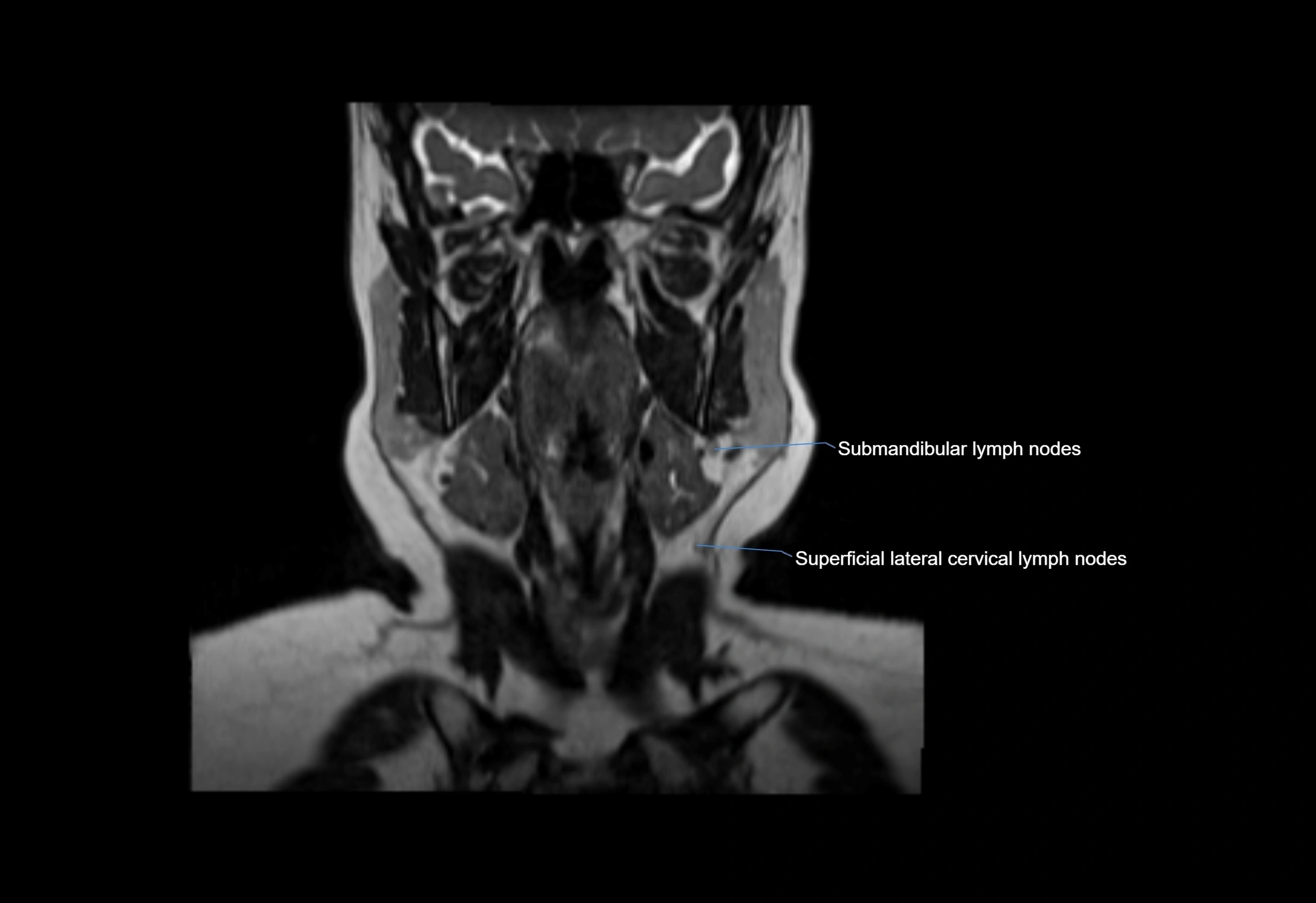
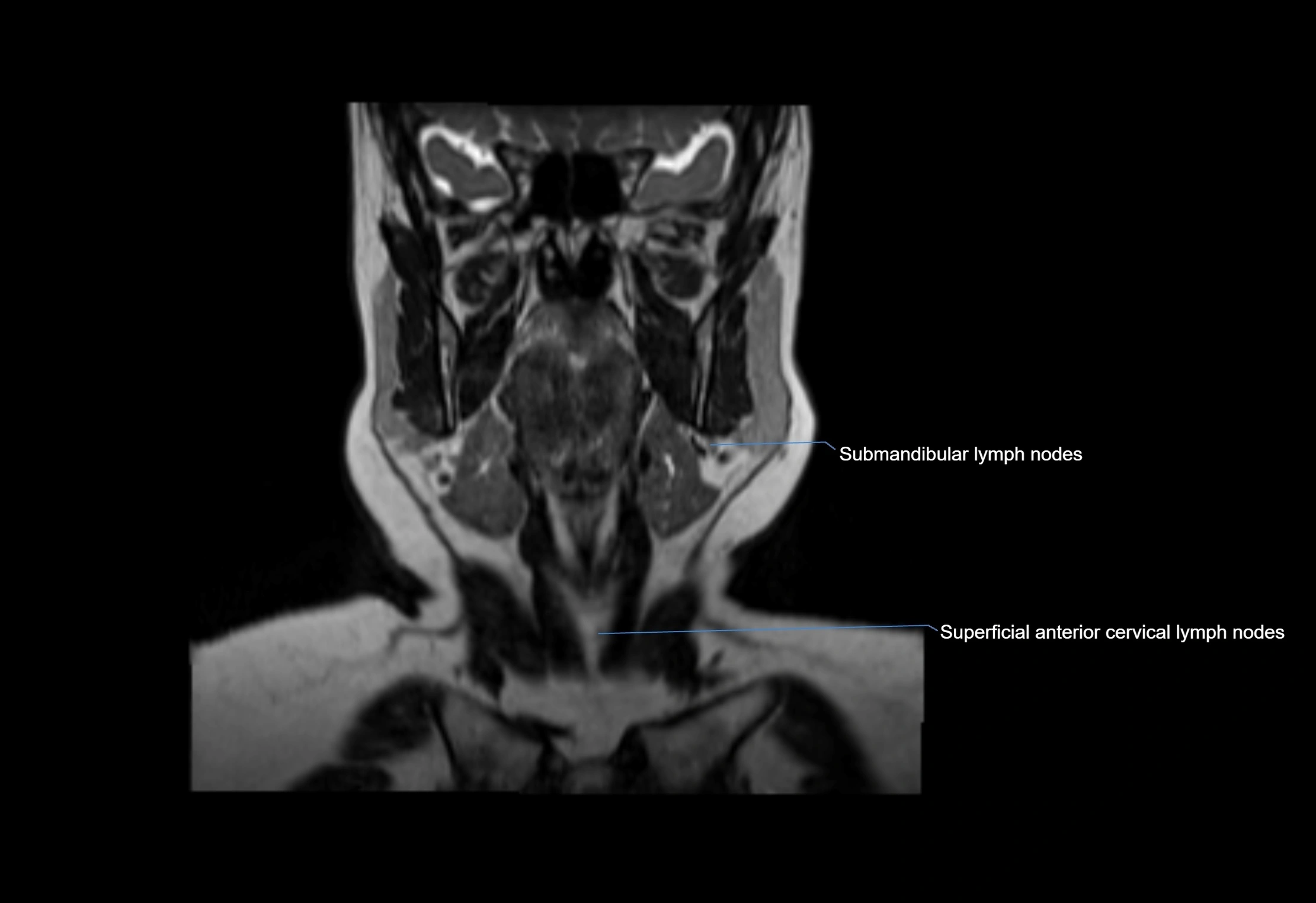
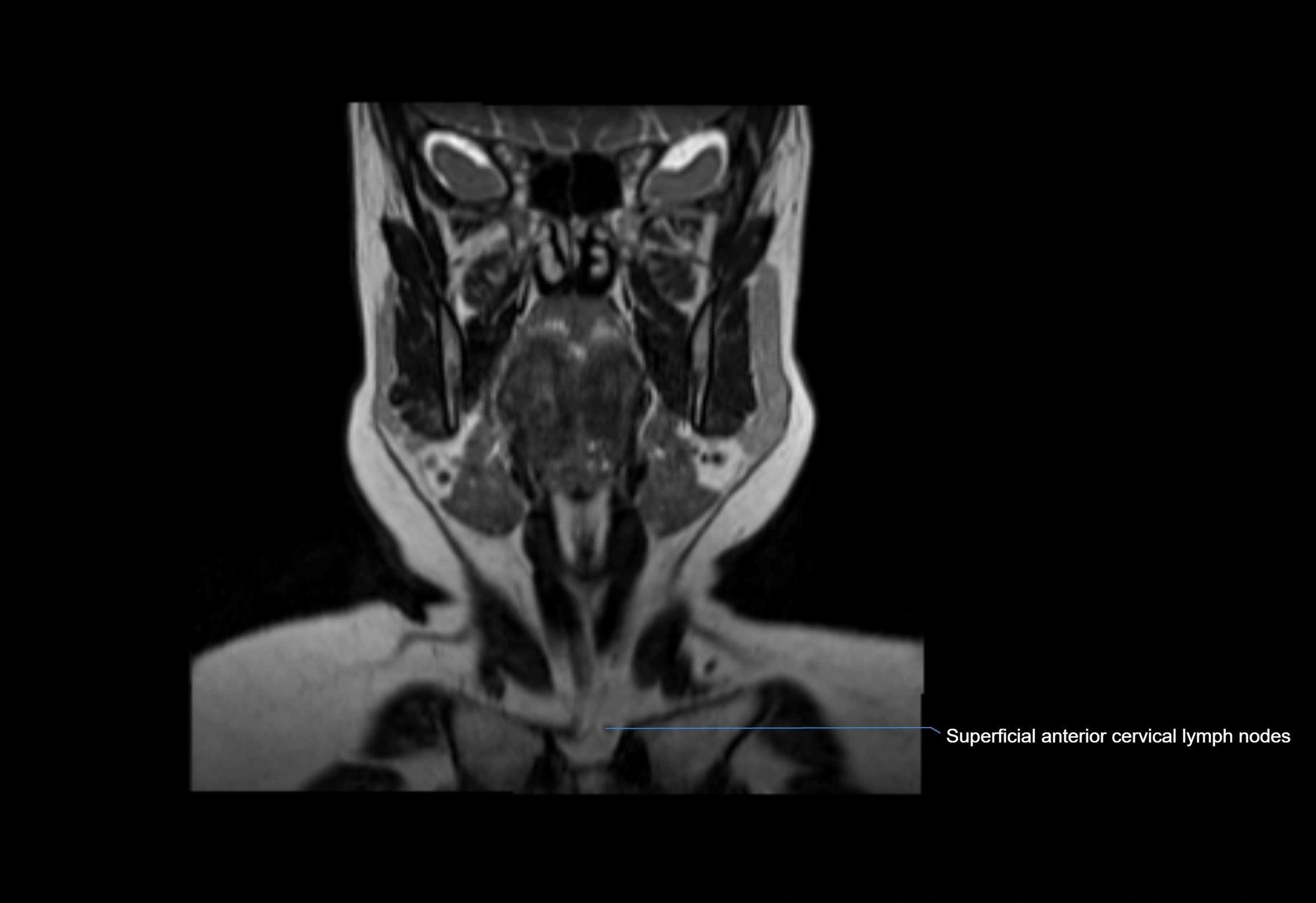
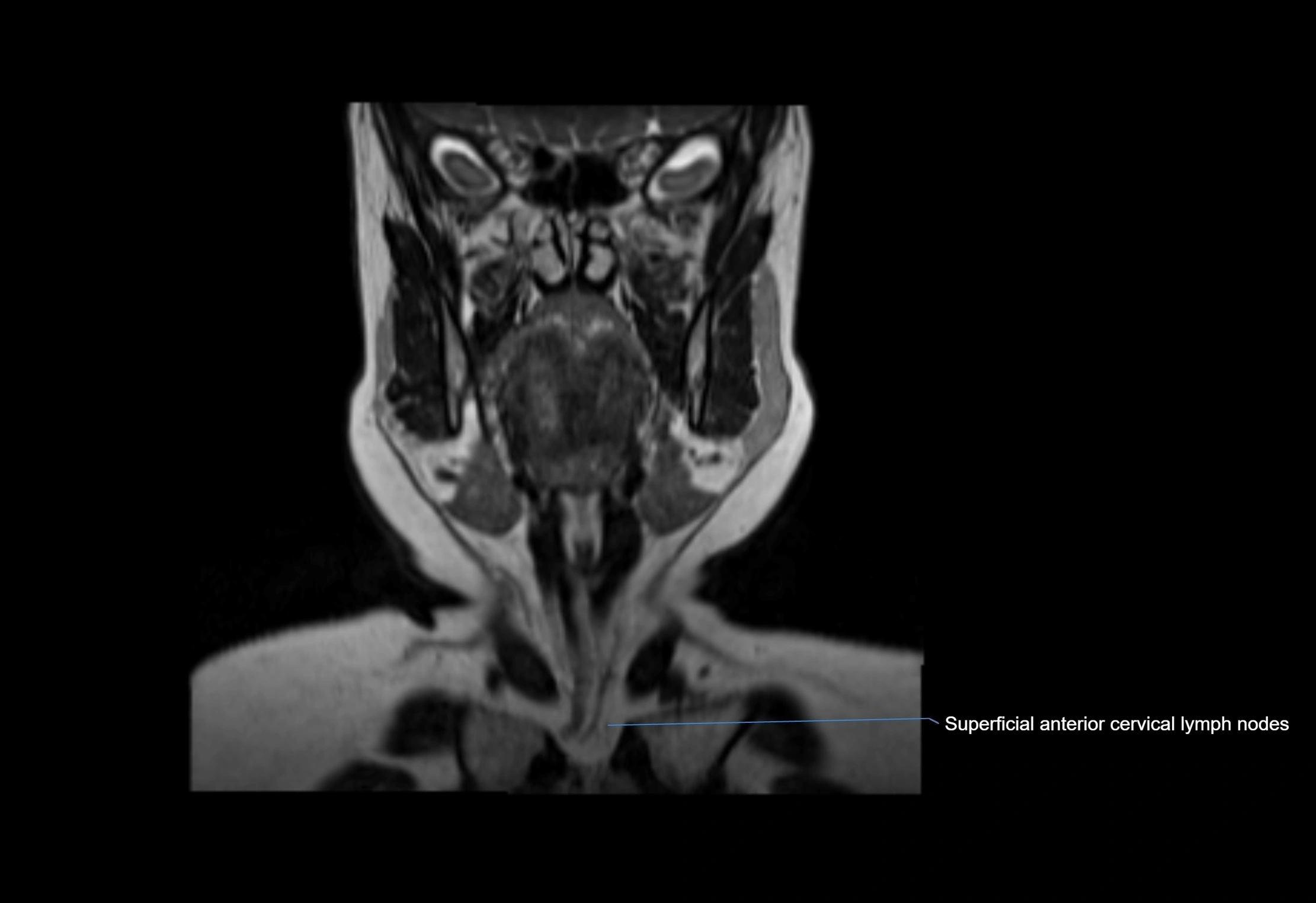
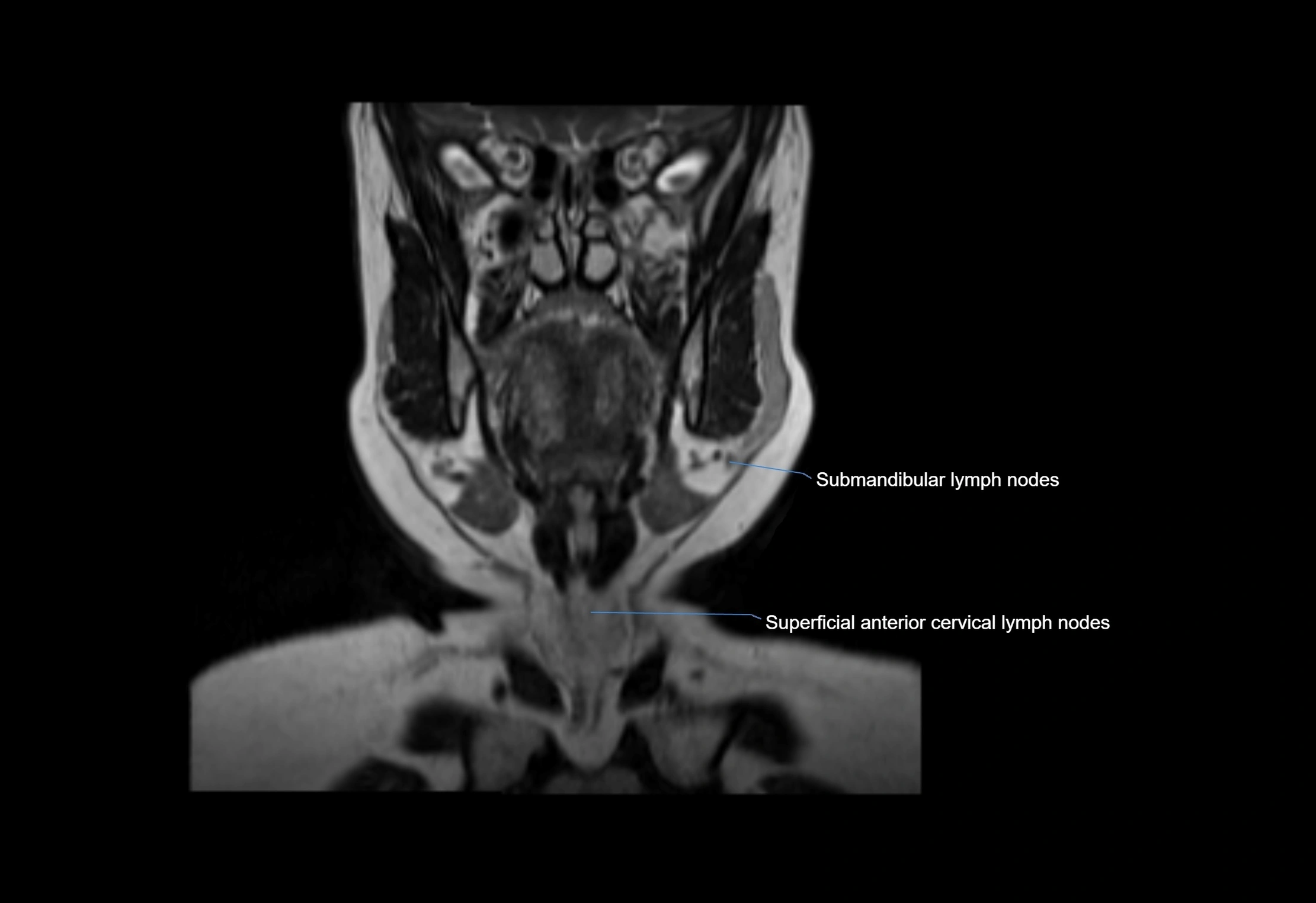
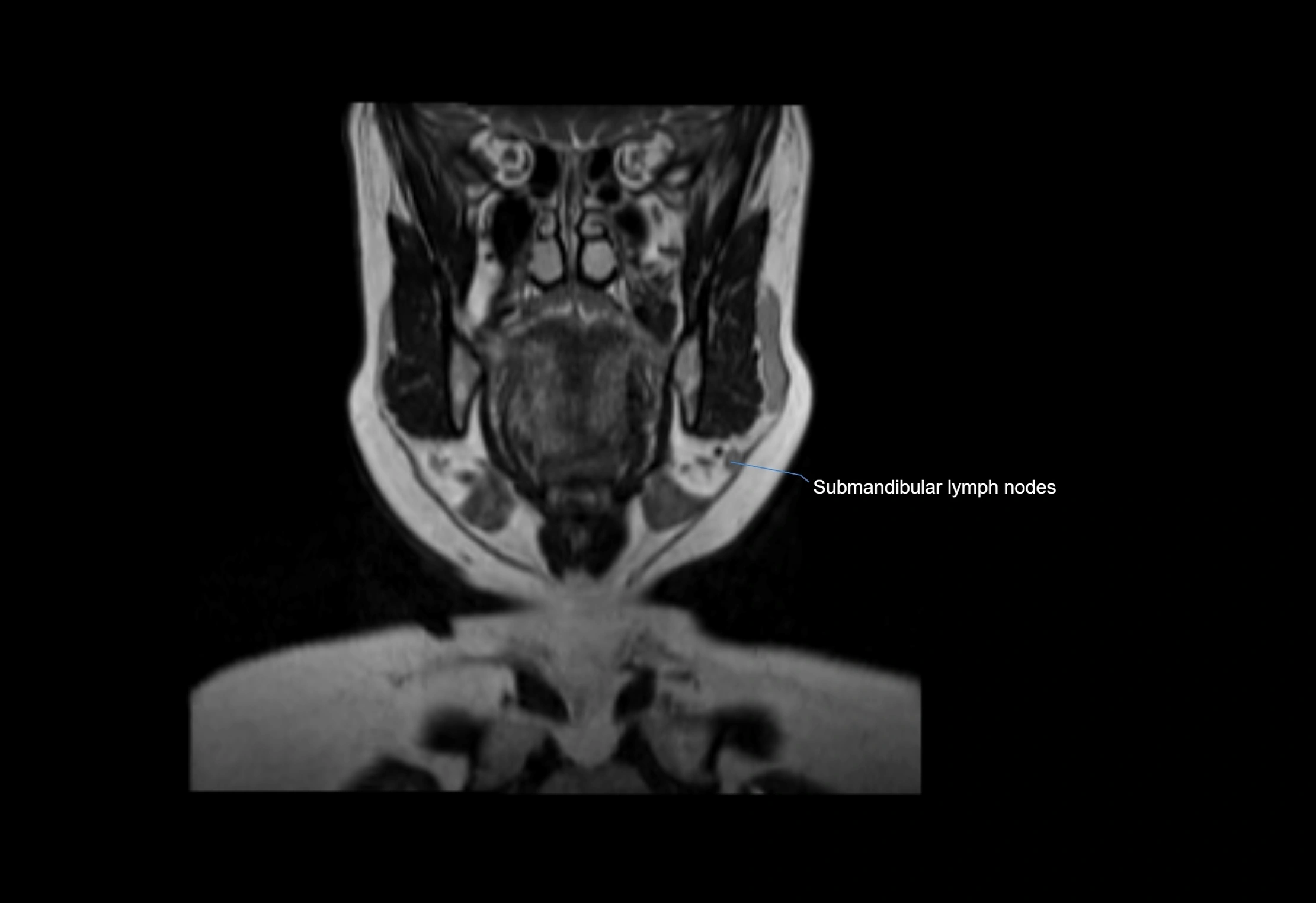
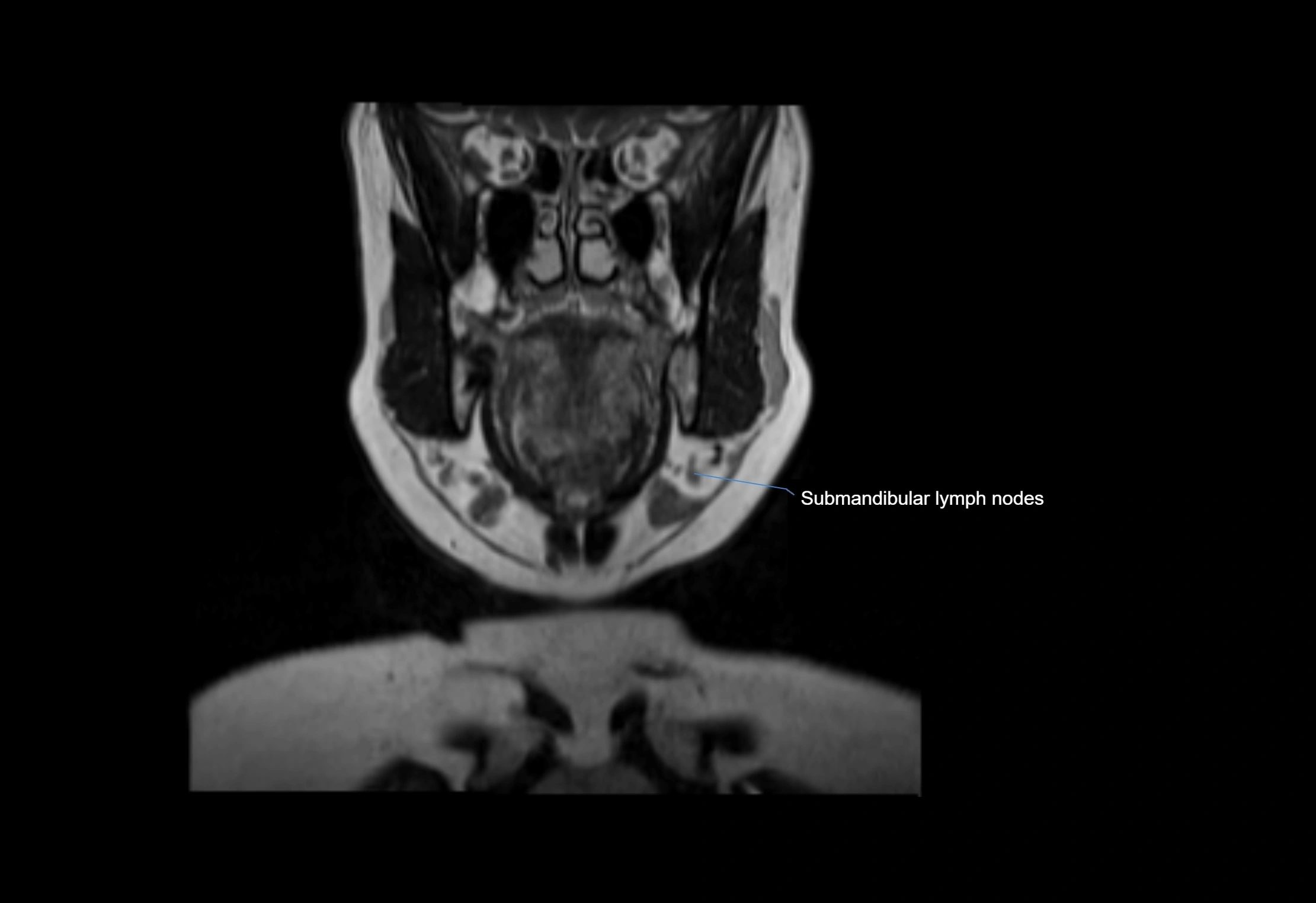
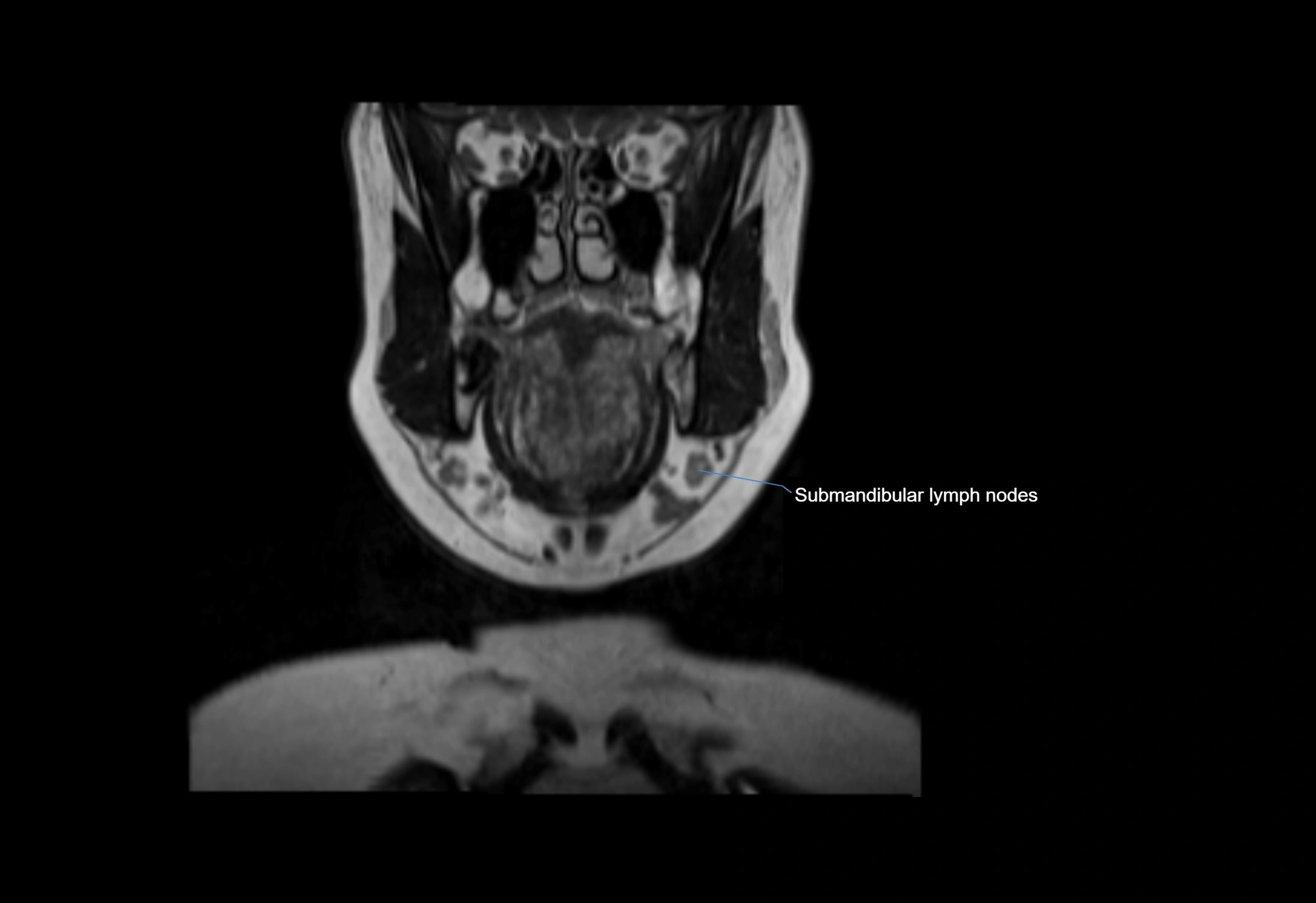
T2-weighted images:
-
Nodes show intermediate signal, with surrounding fat bright
-
Useful for detecting edema, inflammation, or infiltration
-
Fatty hilum may appear slightly hyperintense relative to cortex
STIR (Short Tau Inversion Recovery):
-
Fat suppression enhances visualization of edematous or pathological nodes
-
Normal nodes appear low to intermediate signal, while inflamed or metastatic nodes appear hyperintense
-
Useful for detecting subtle lymphadenopathy or early pathology
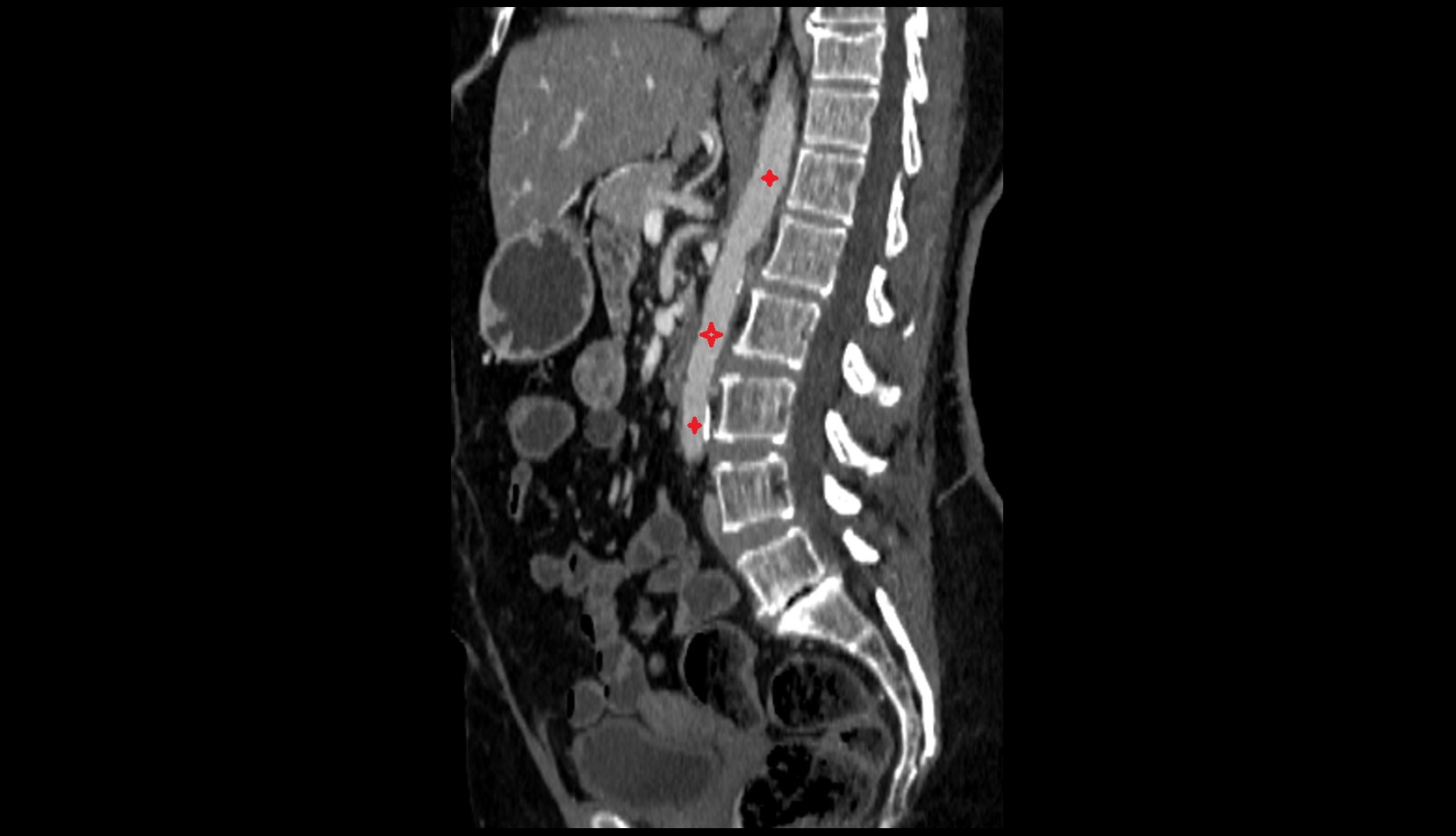
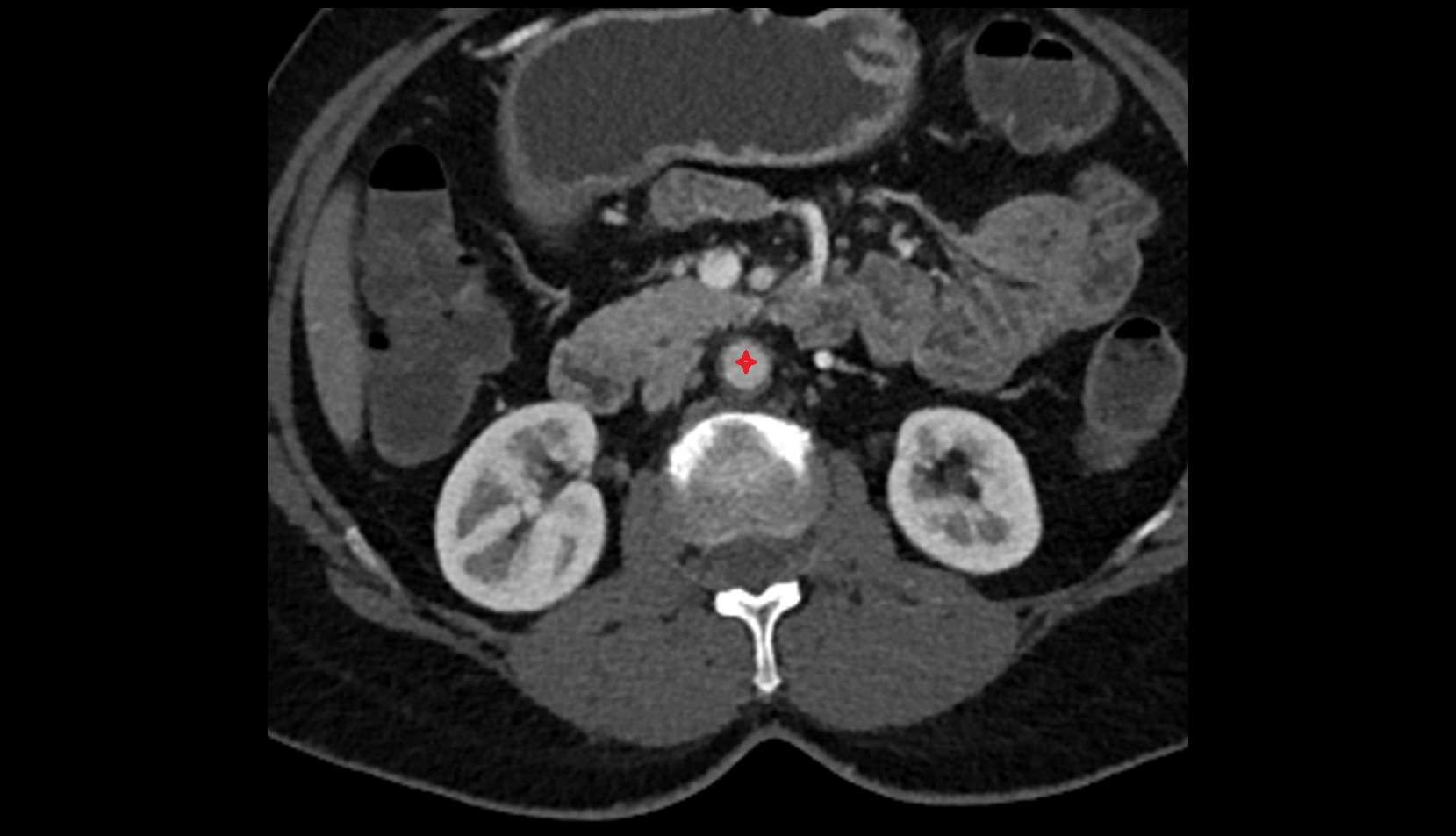
CT Appearance:
-
Nodes appear as small, soft tissue density structures embedded in subcutaneous fat near primary lymph nodes
-
Surrounded by air in adjacent facial cavities or normal soft tissue, providing natural contrast
-
Enlarged or pathological nodes appear as well-defined or irregular soft tissue masses
-
CT is particularly useful for preoperative assessment, infection evaluation, or detection of metastatic spread
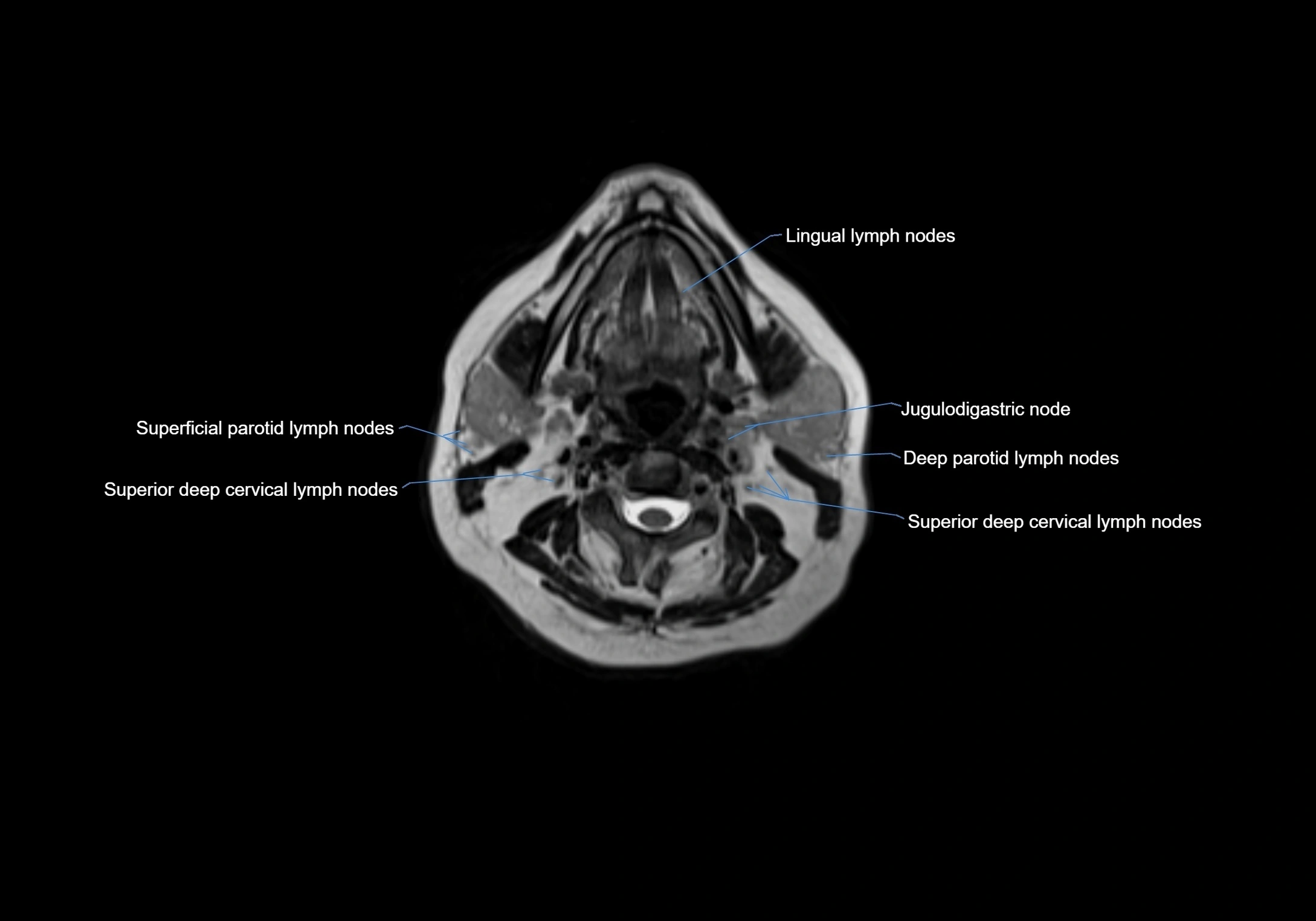
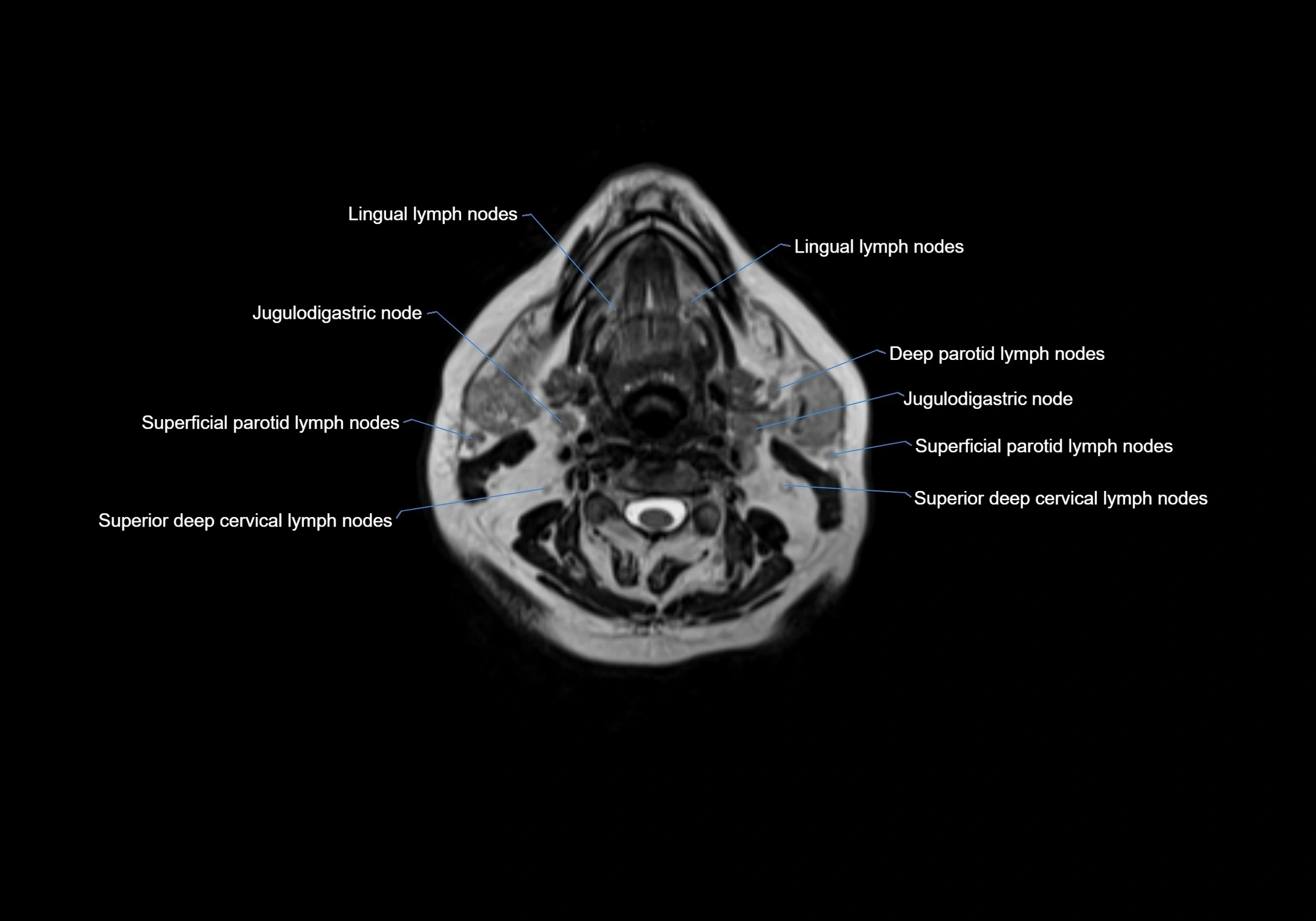
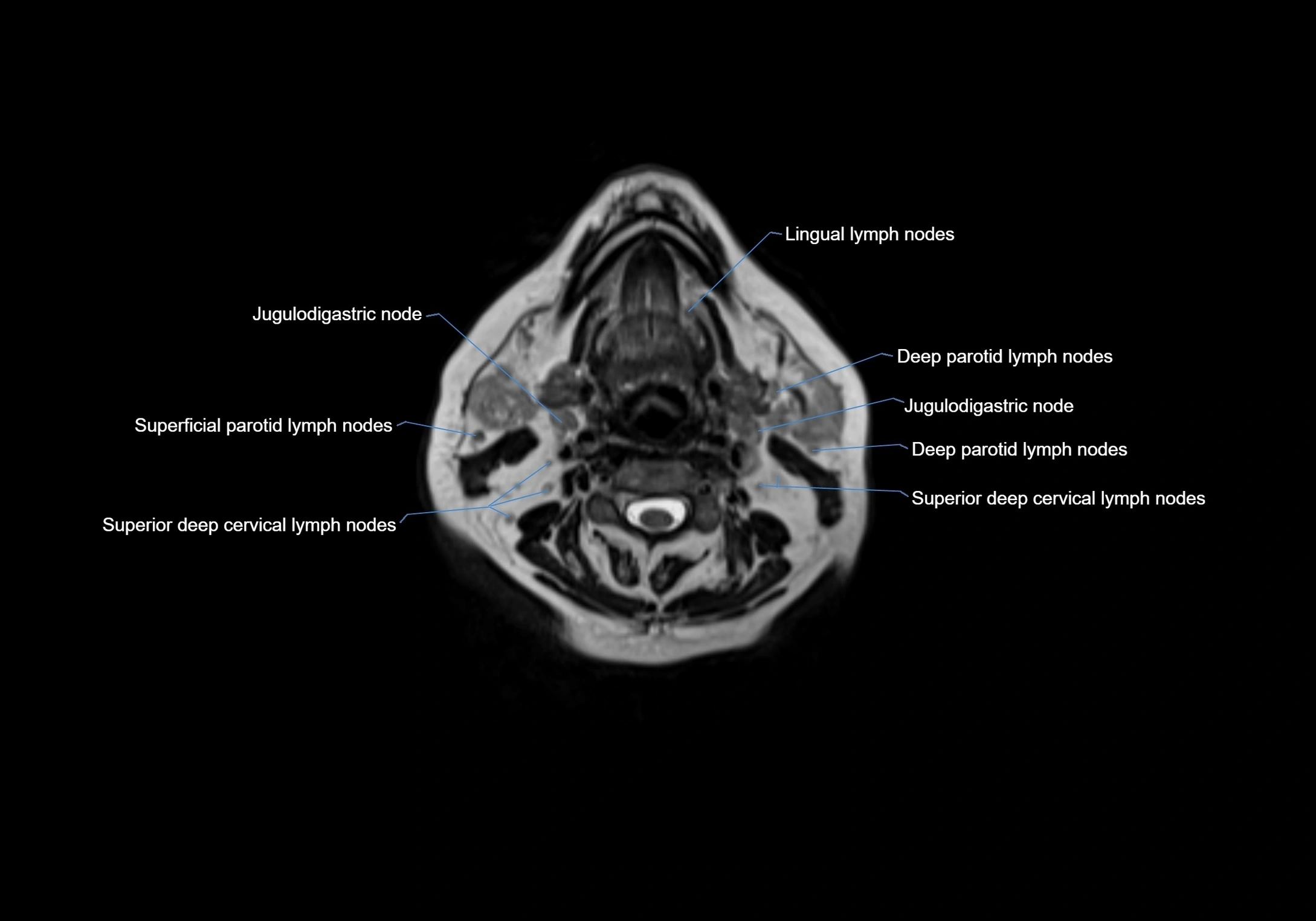
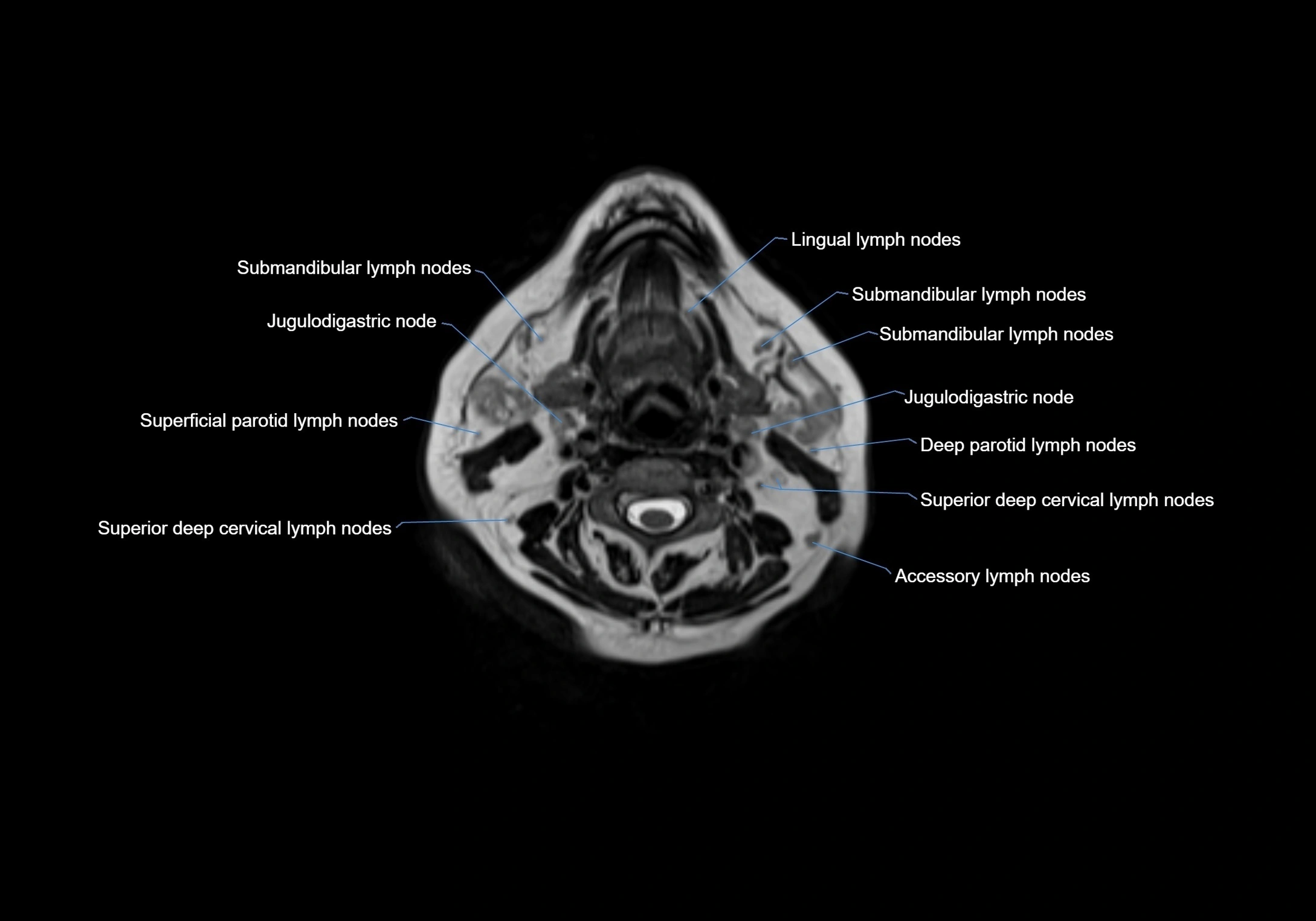
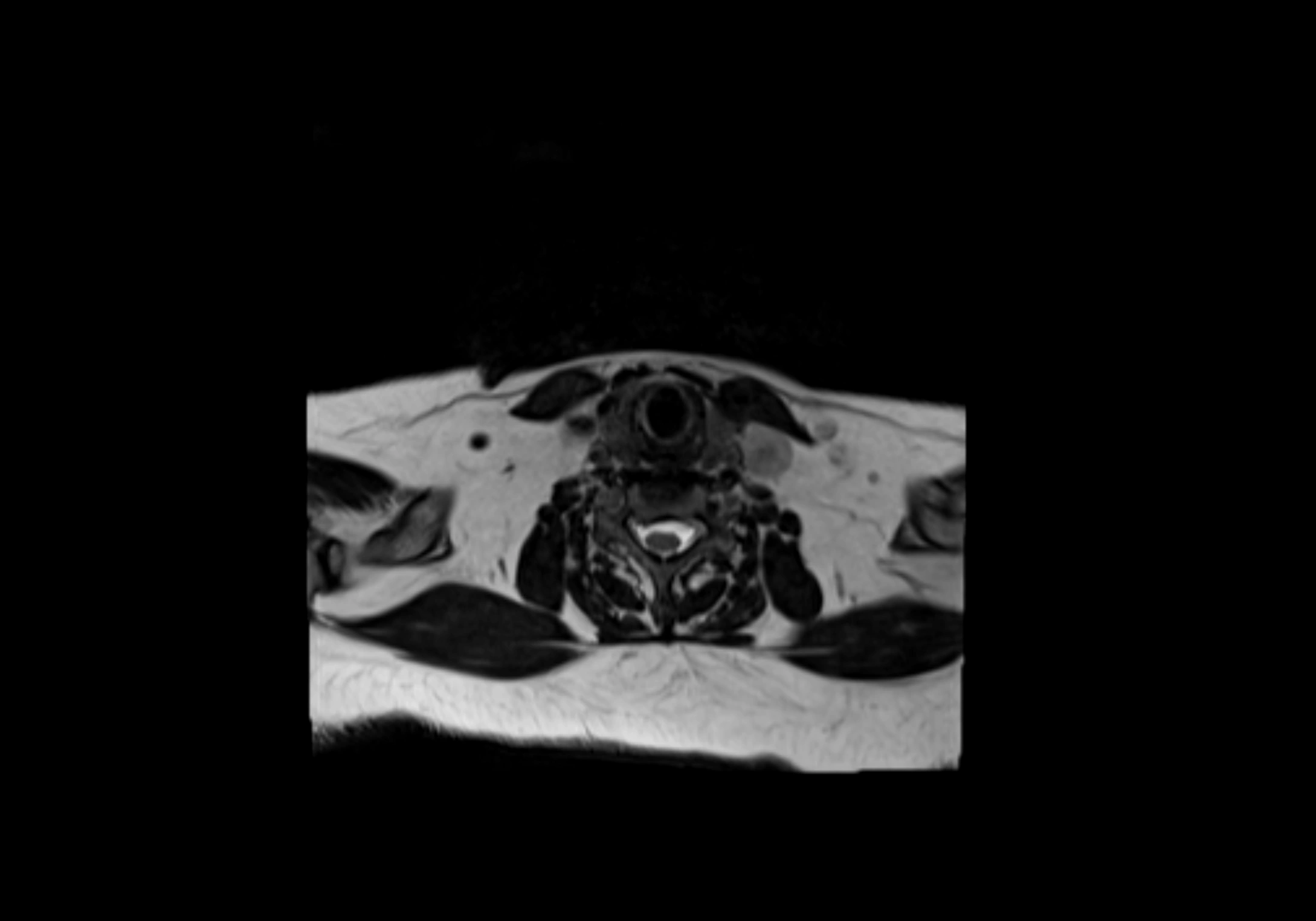
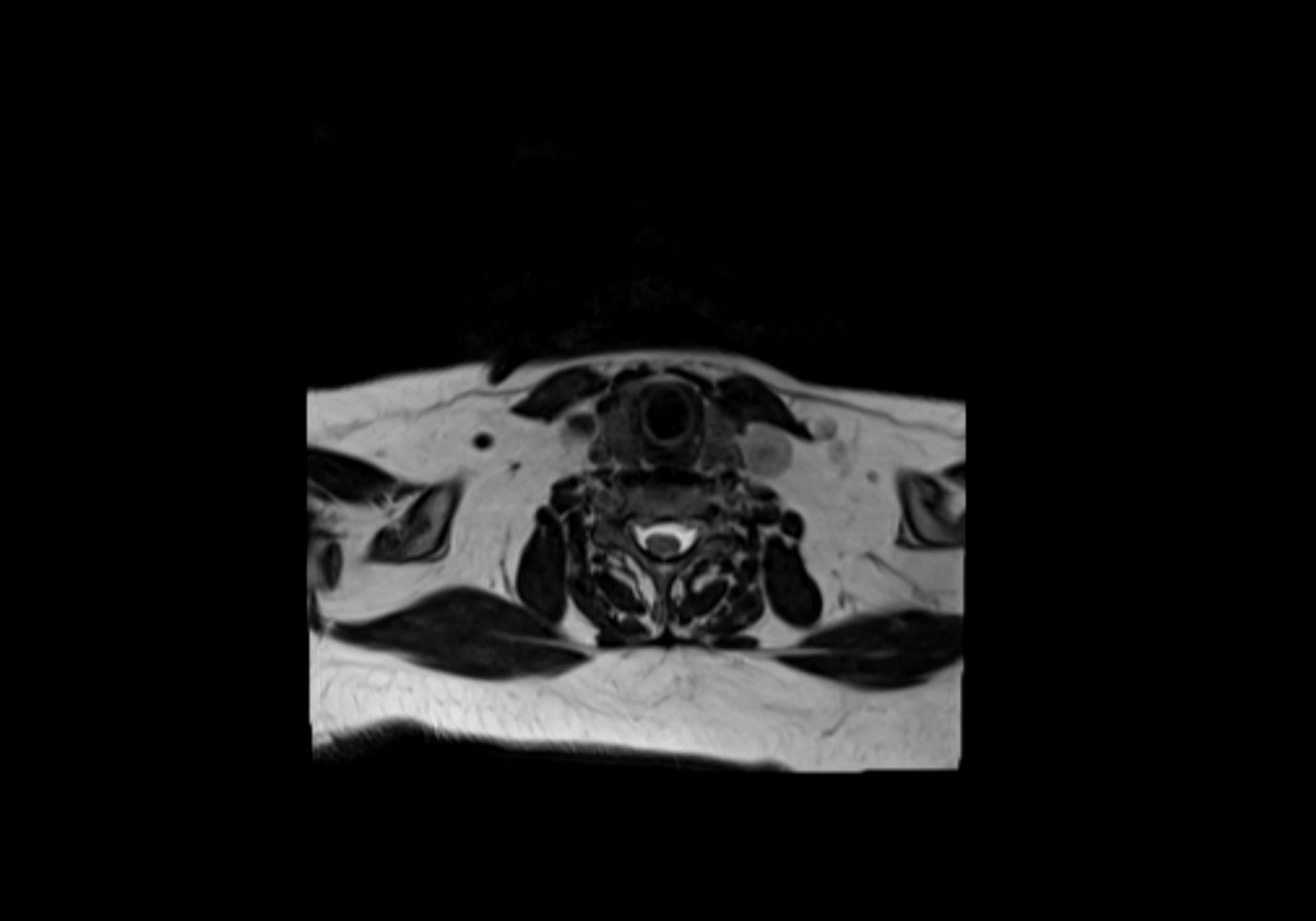
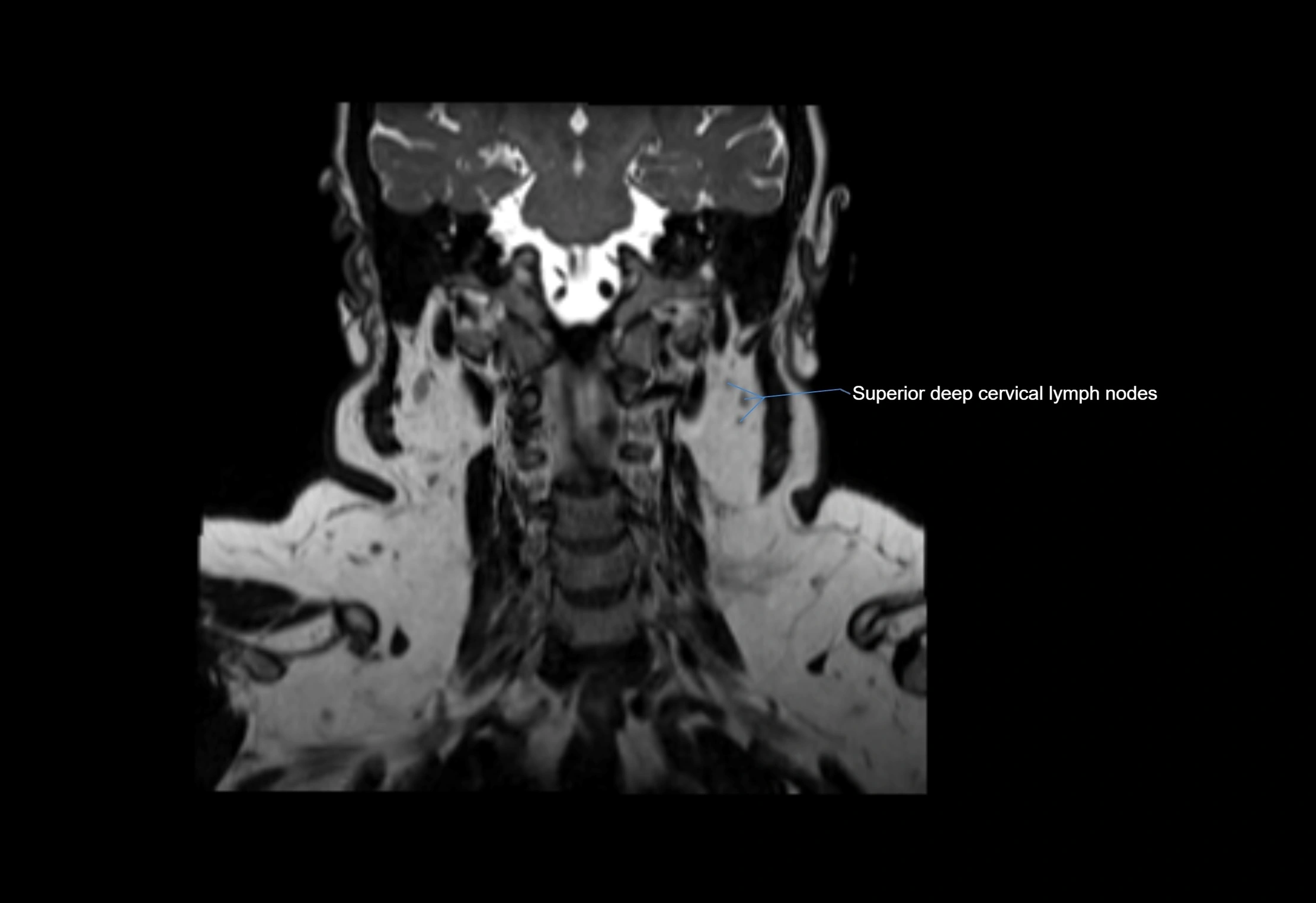
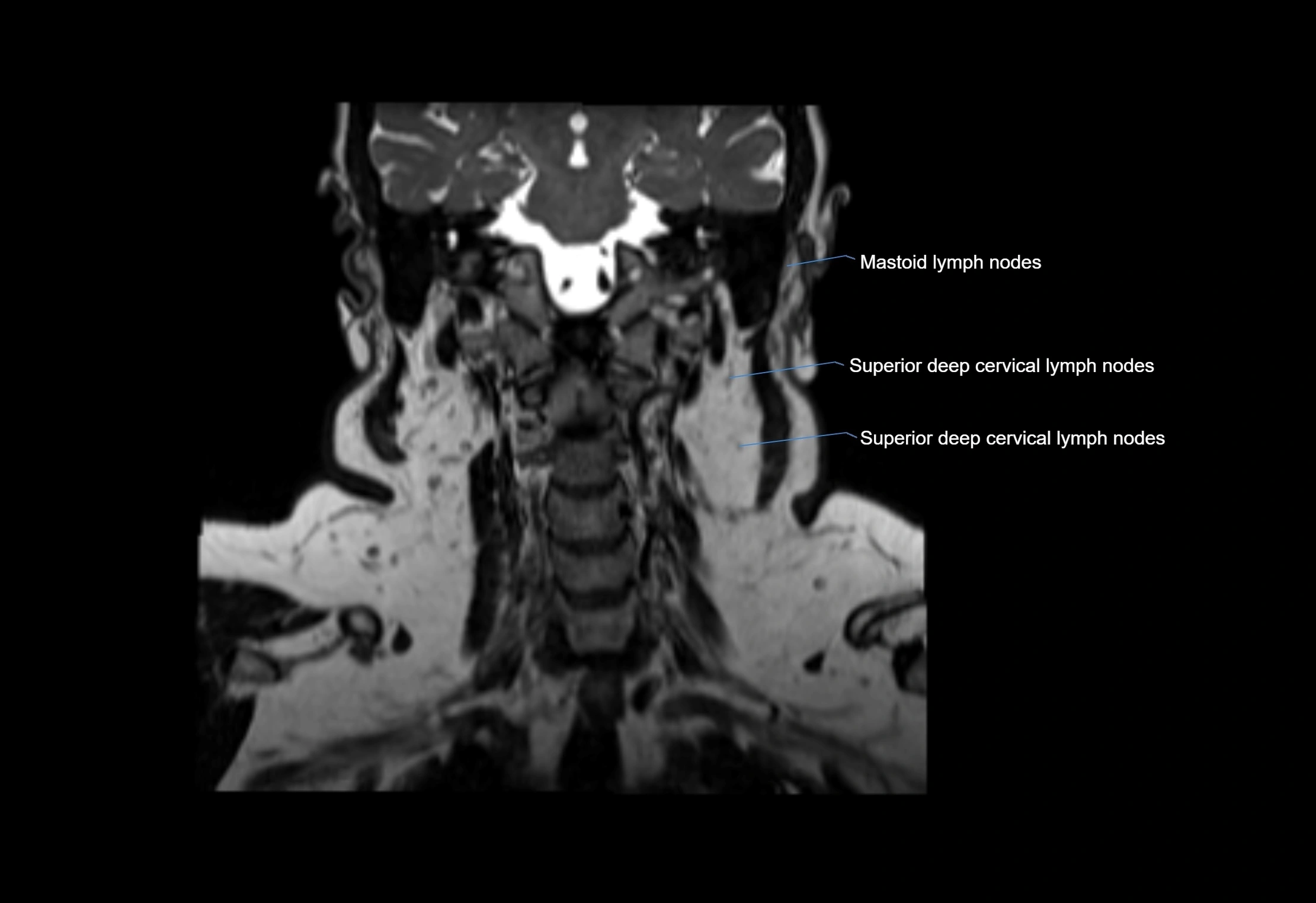
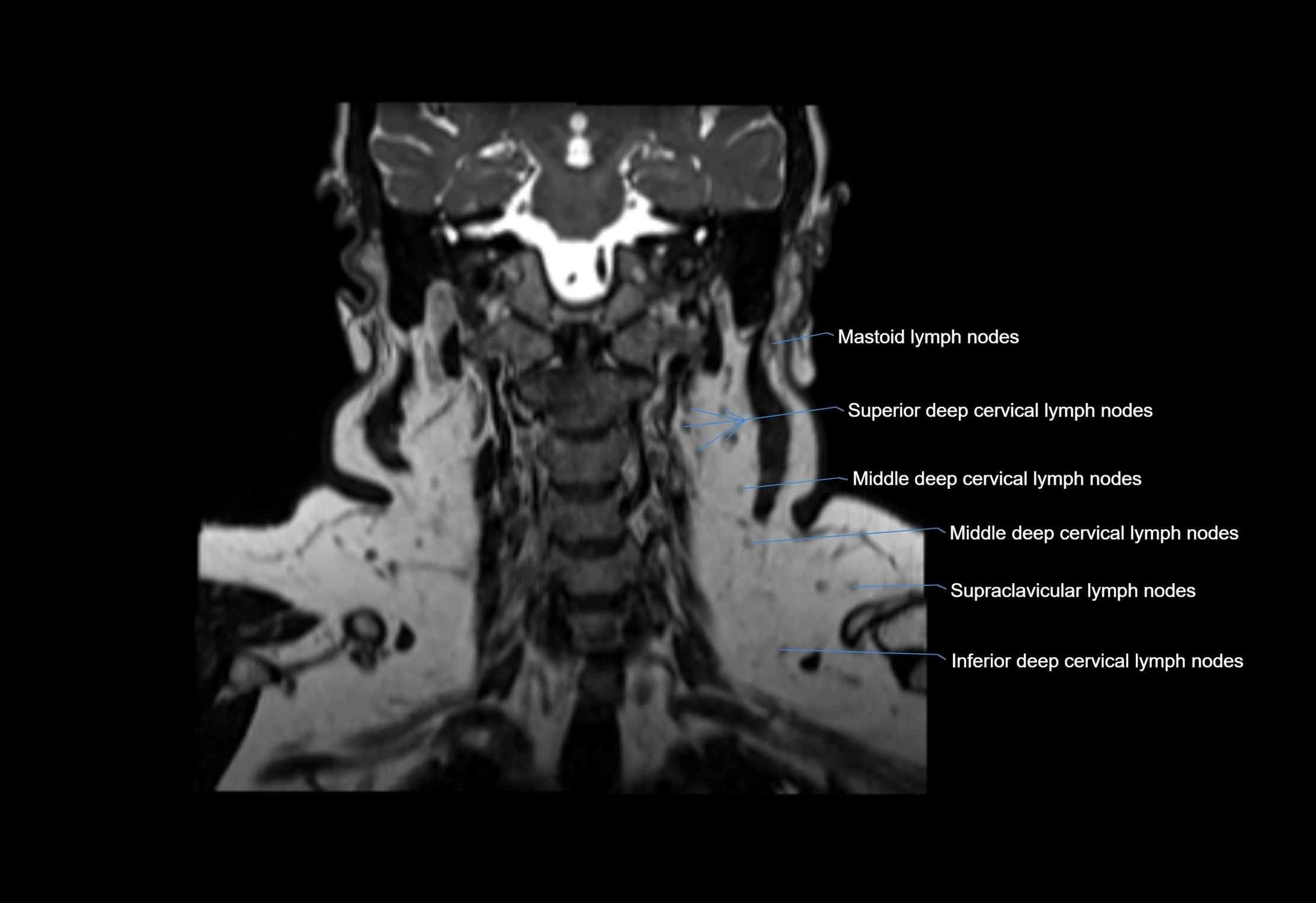
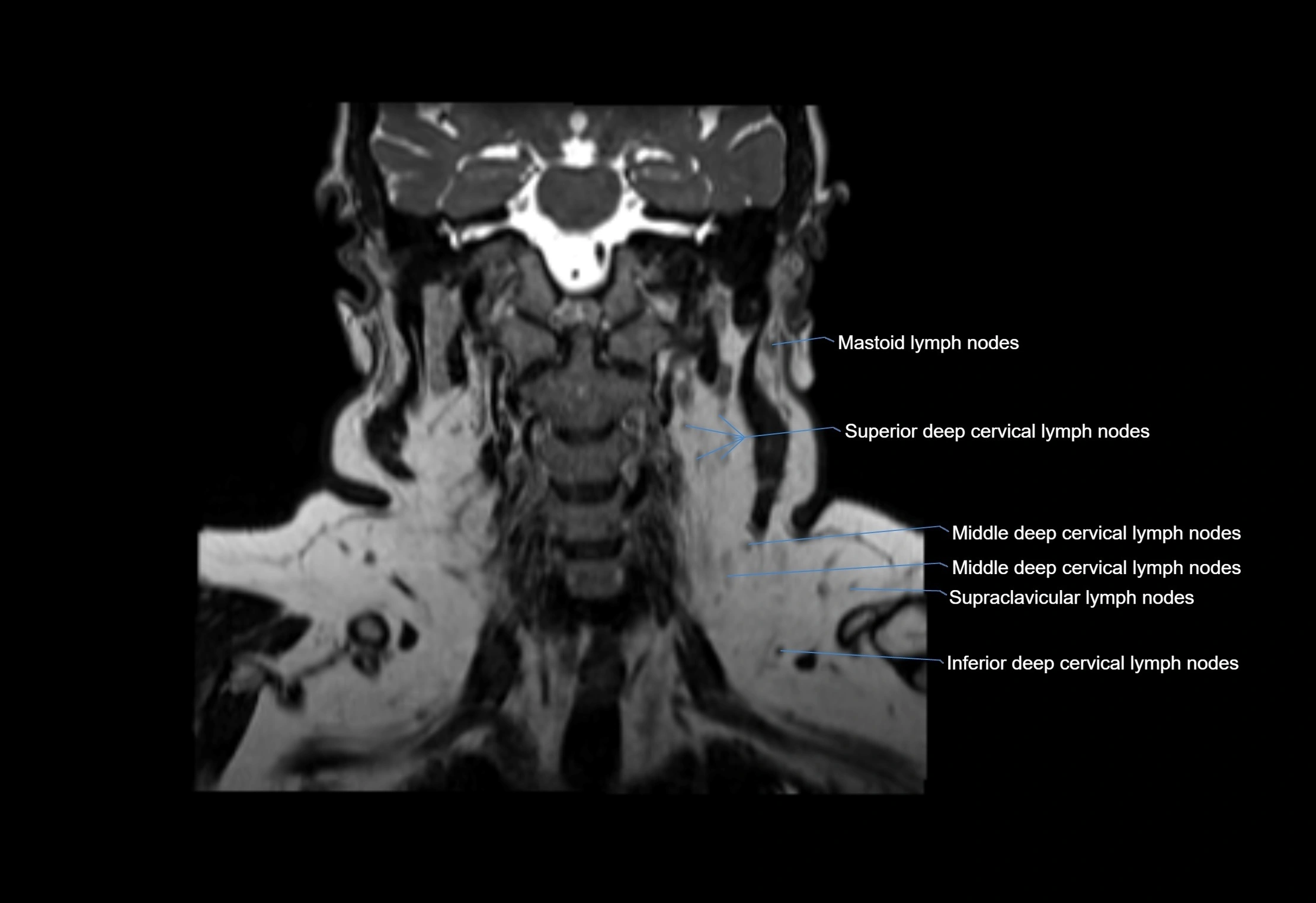
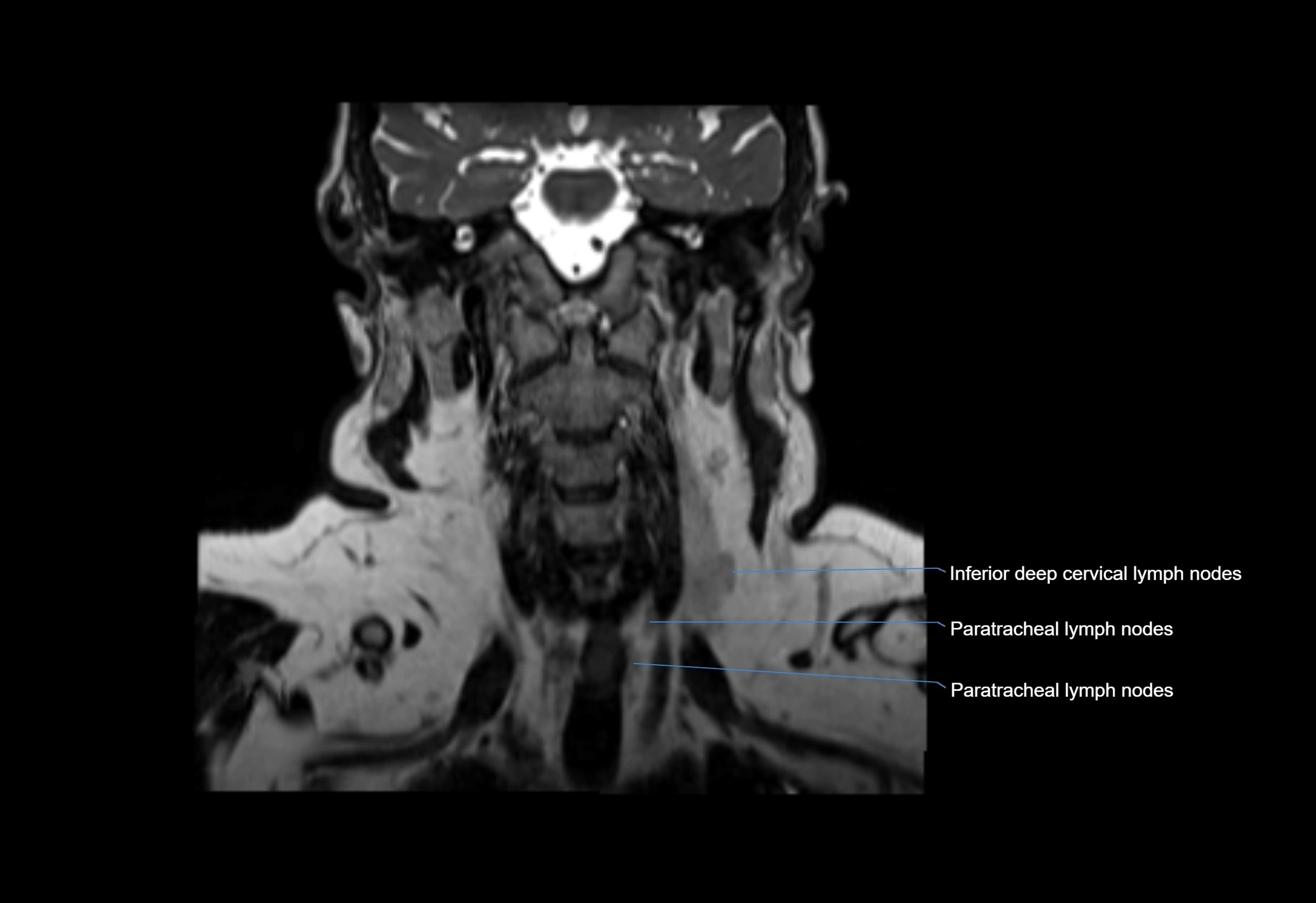
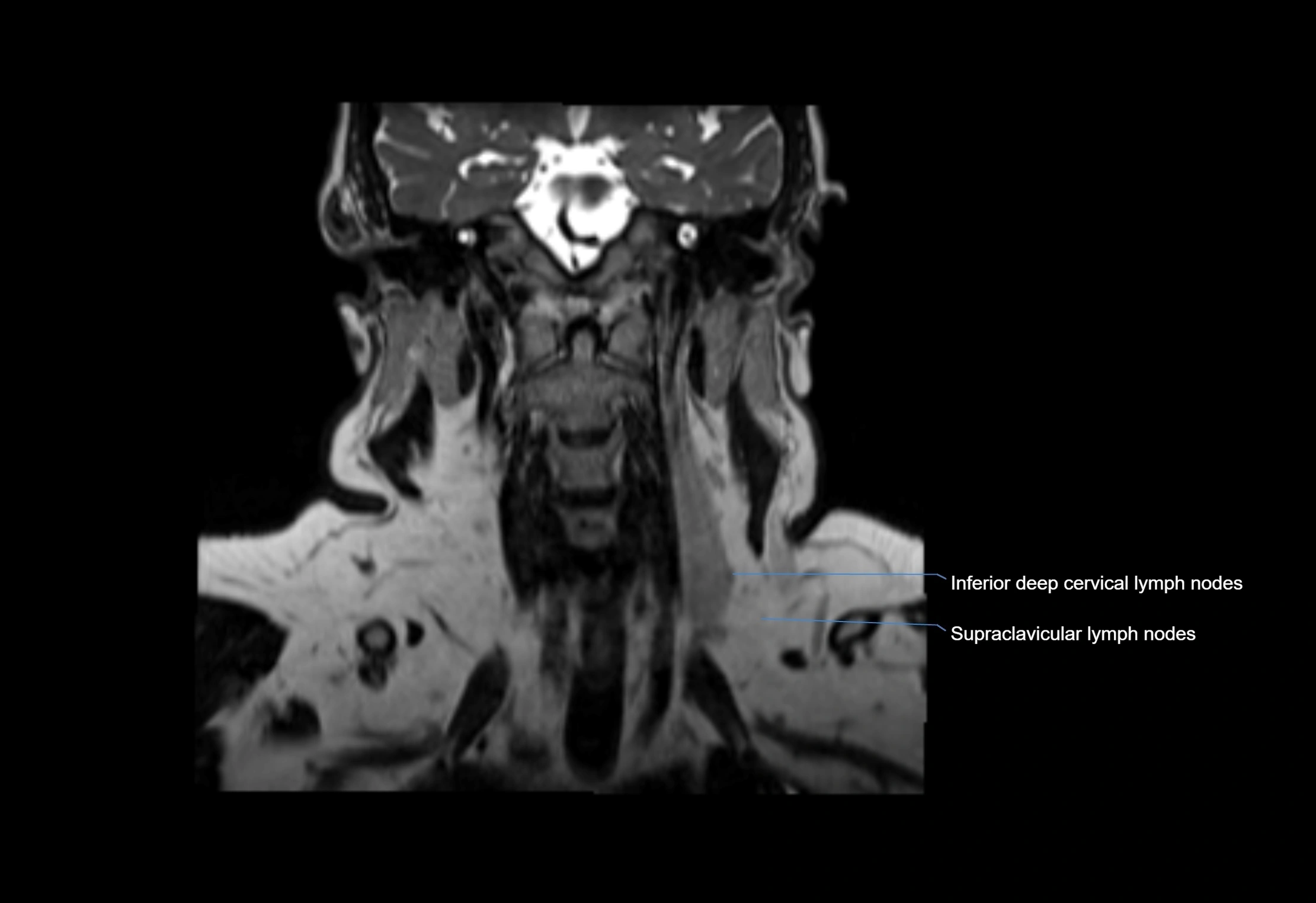
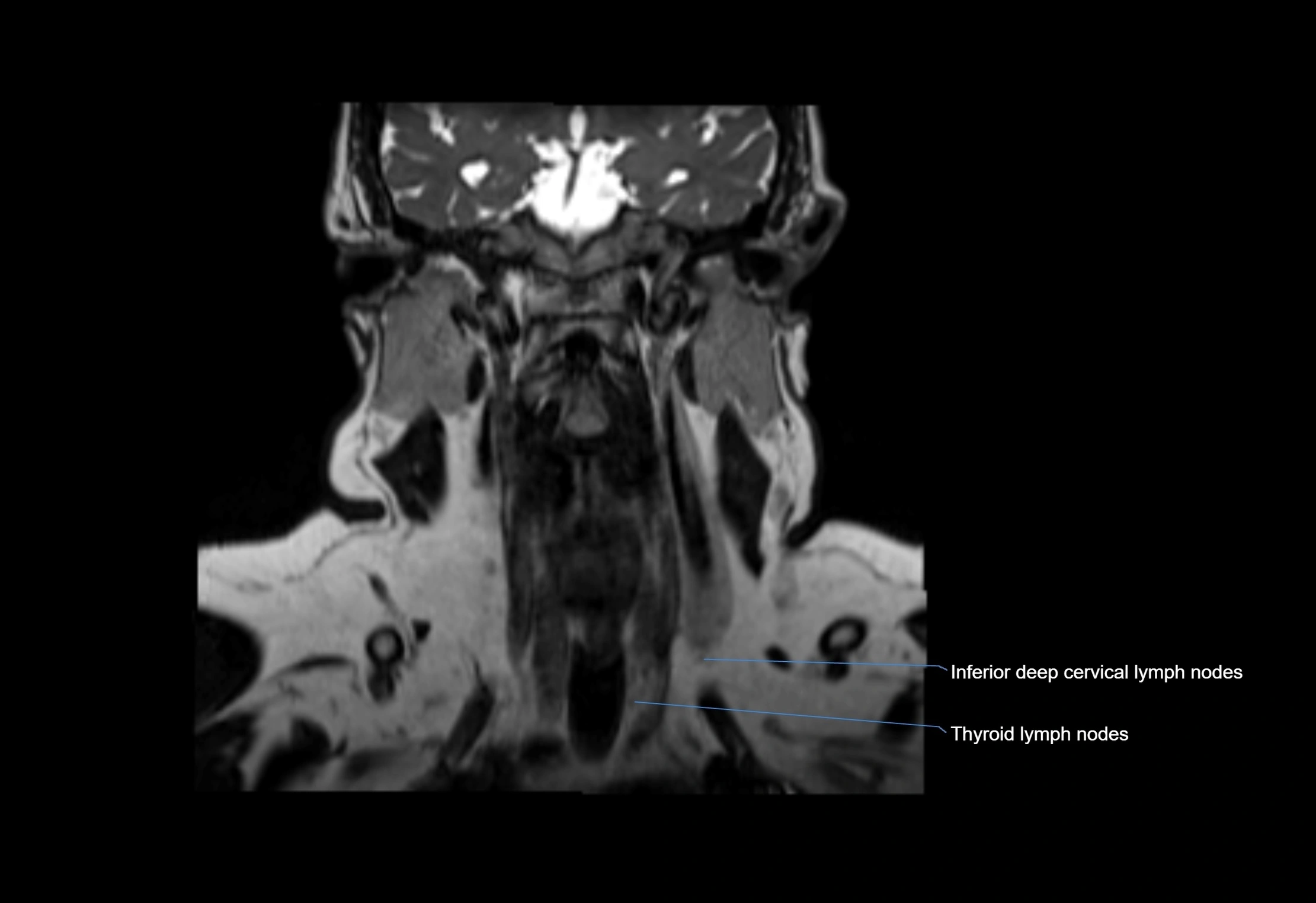
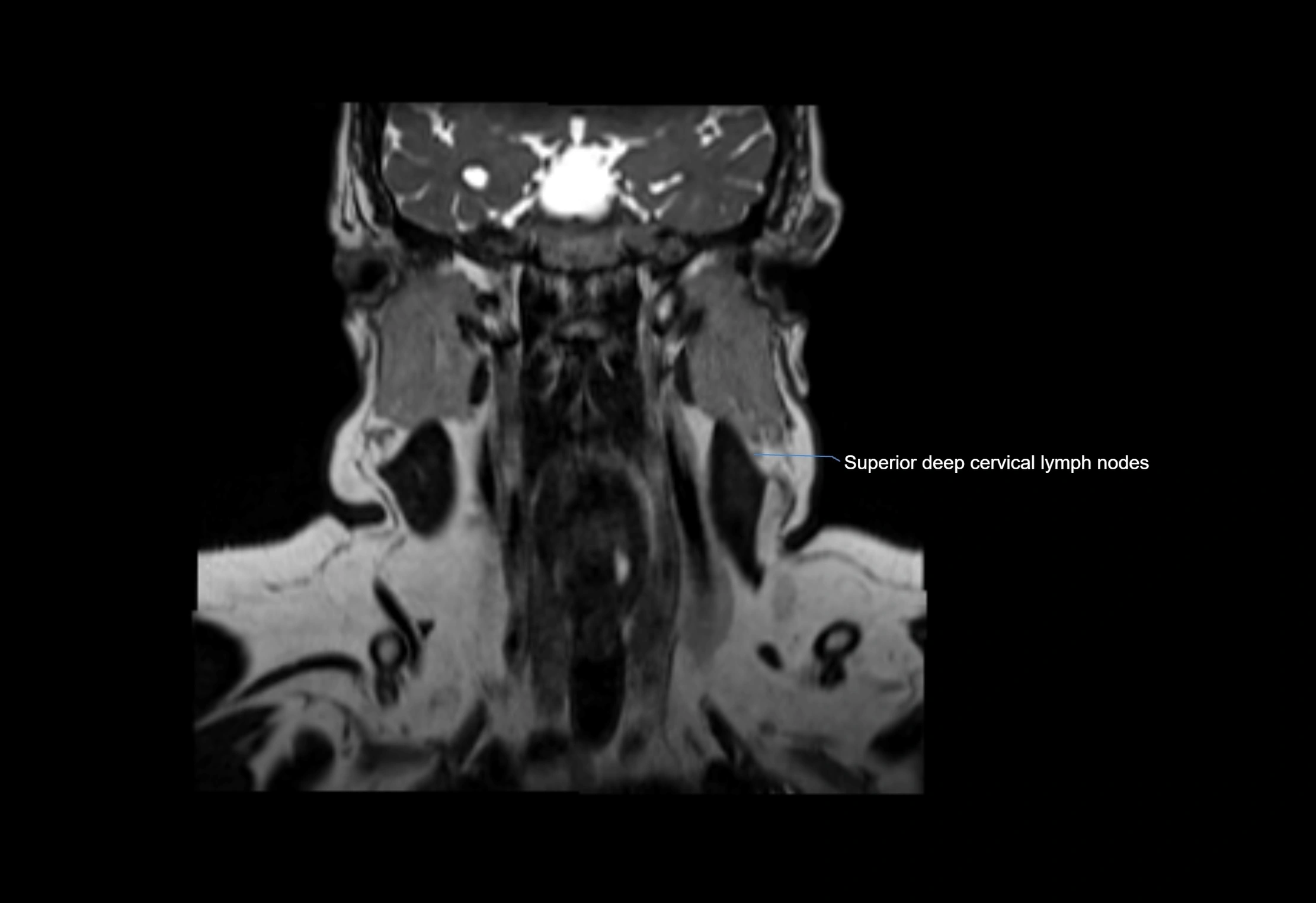
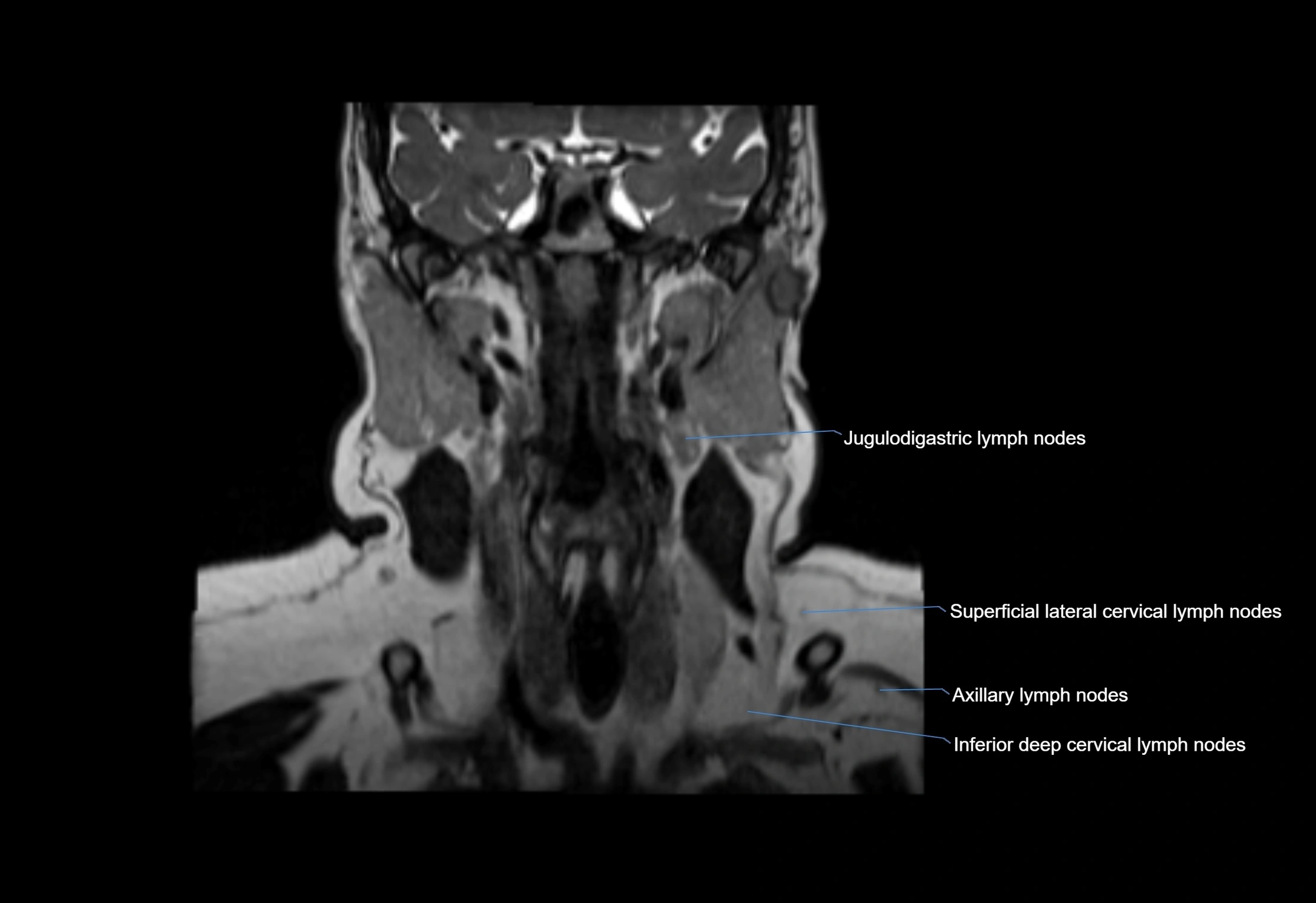
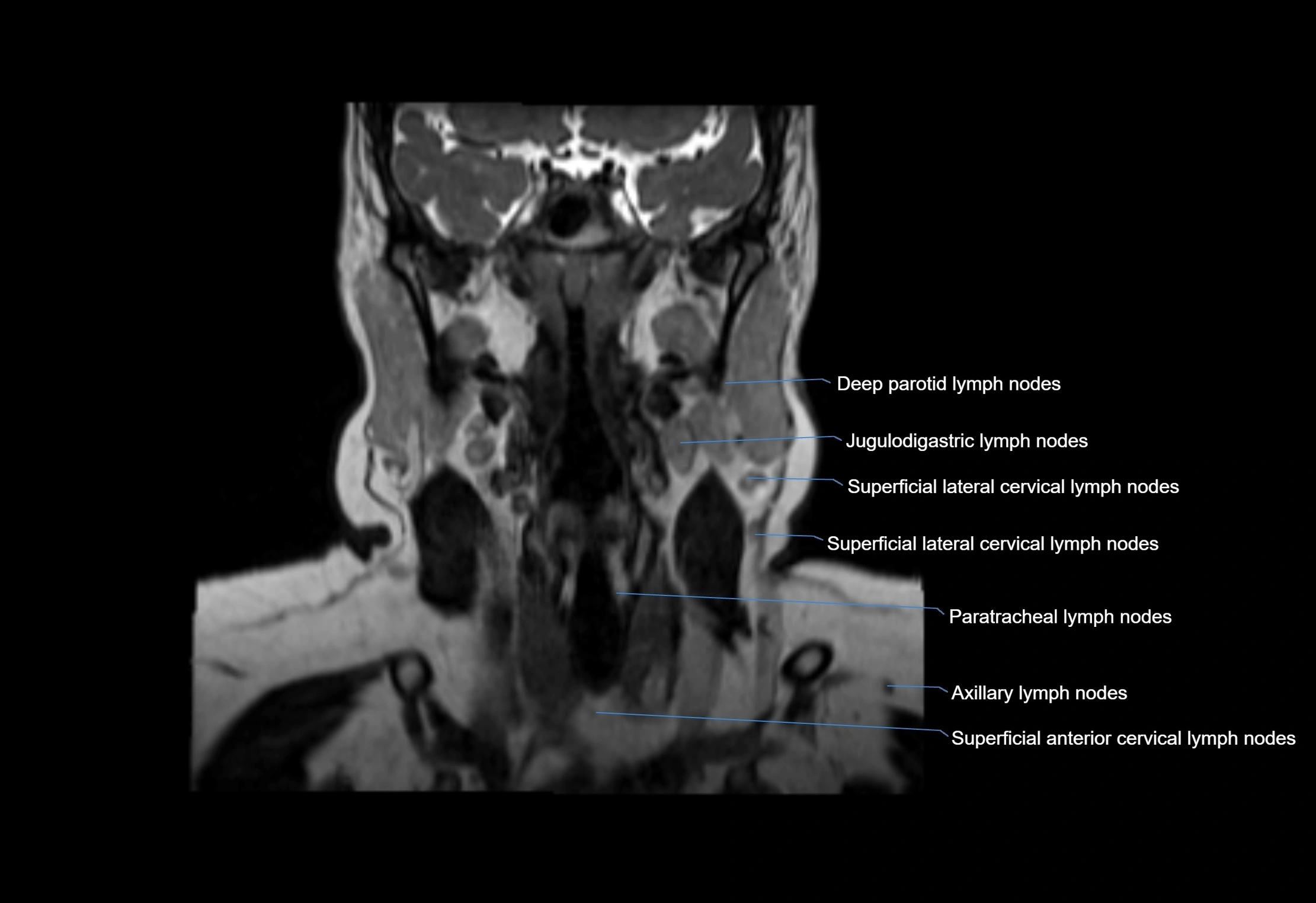
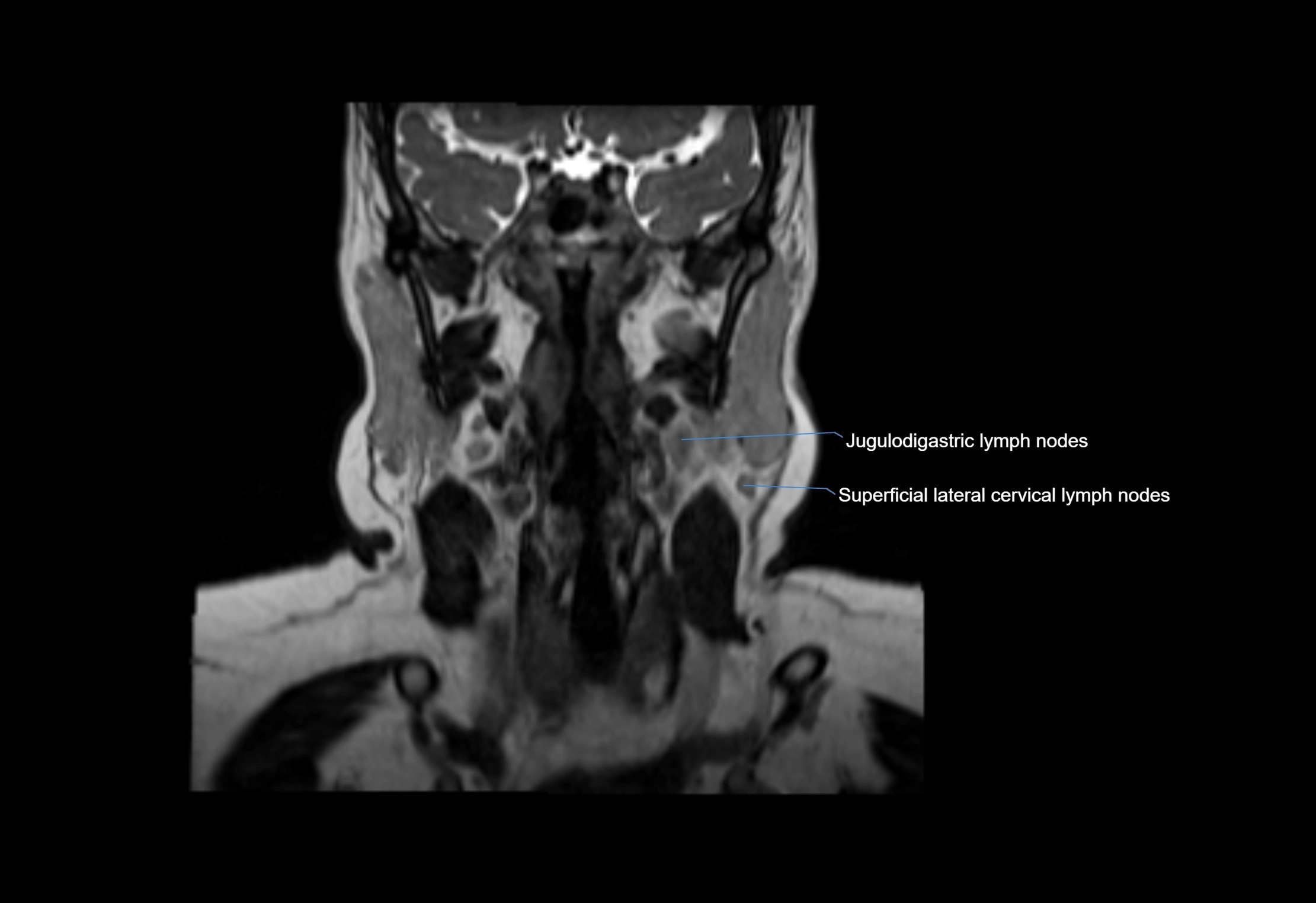
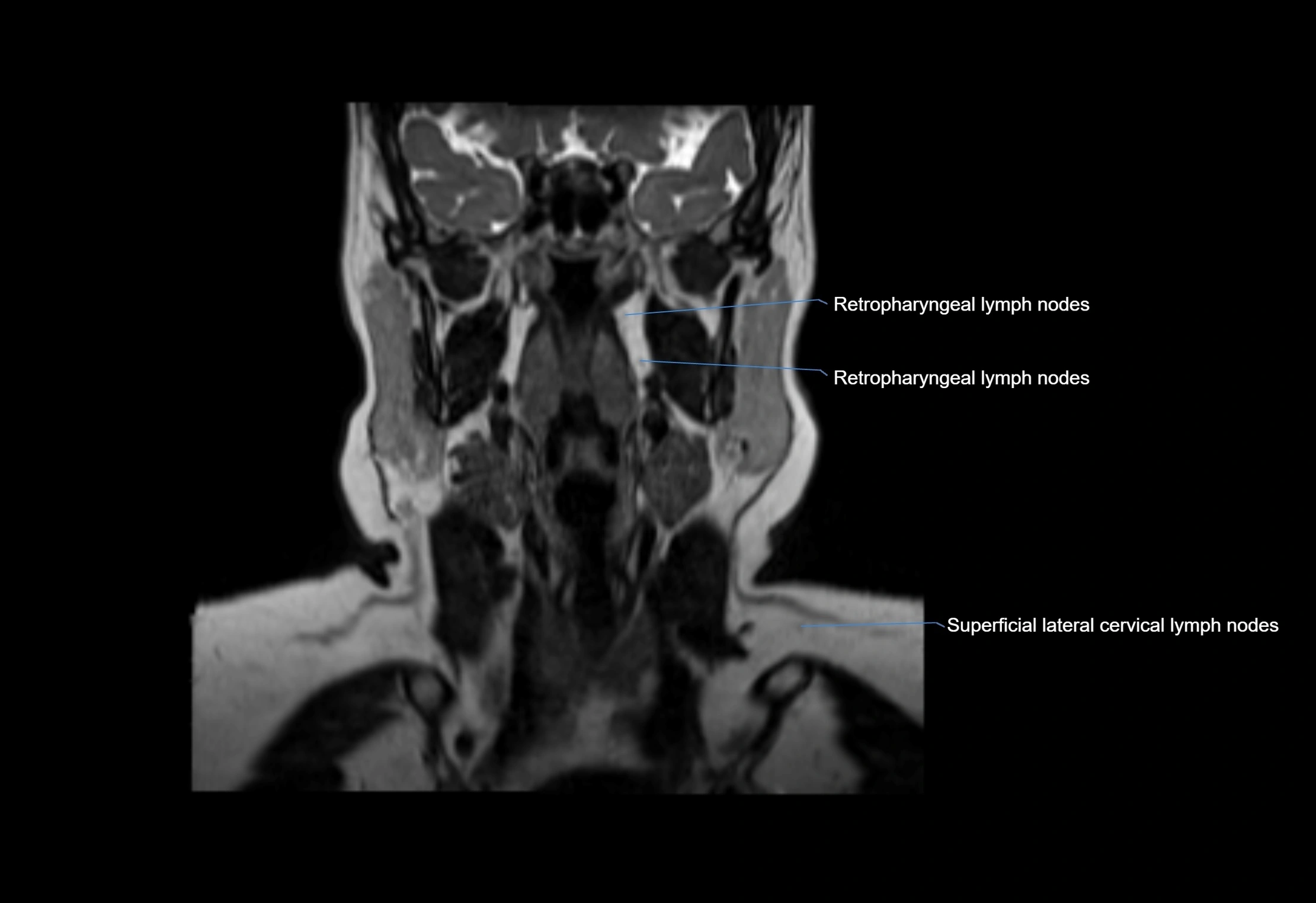
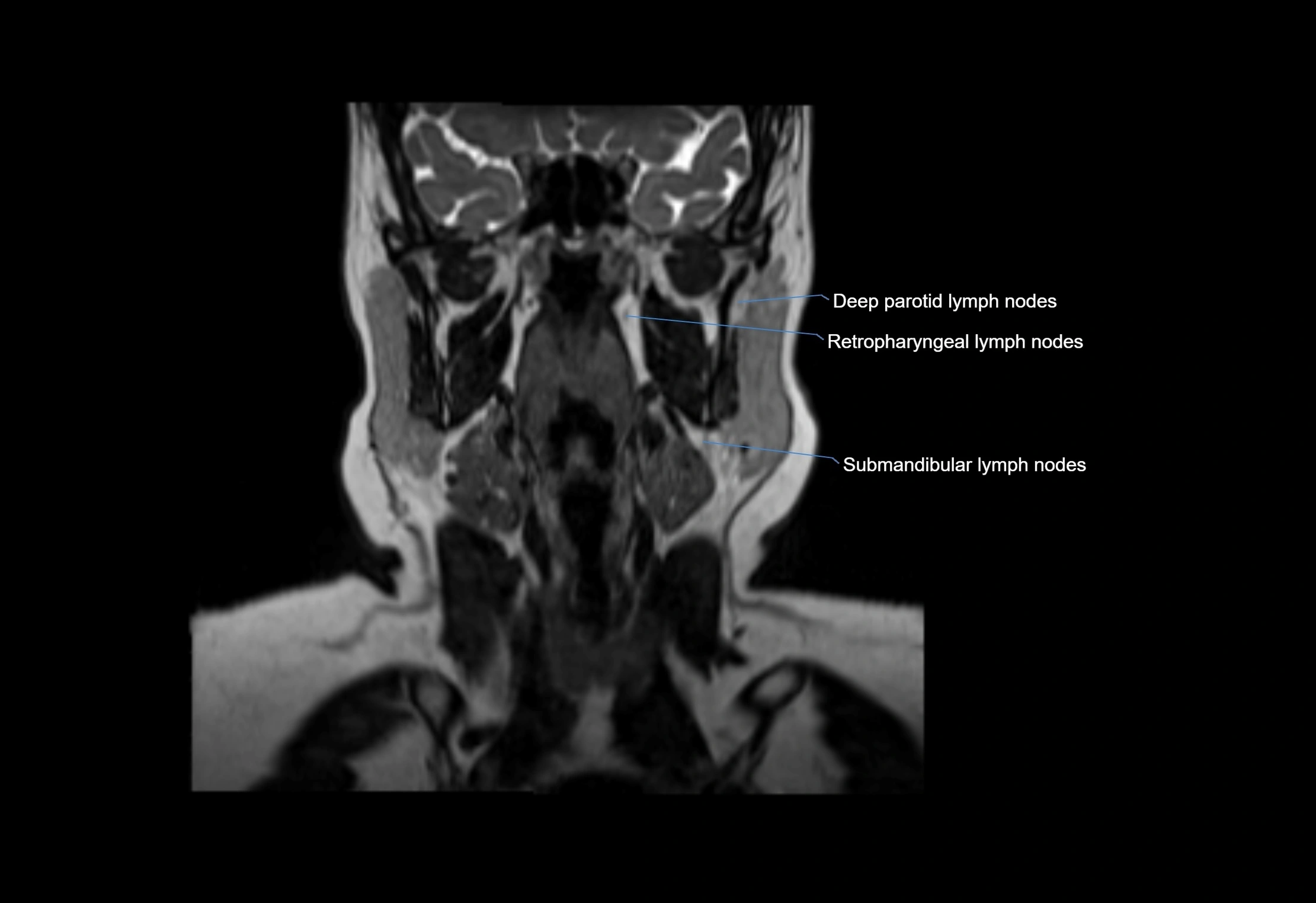
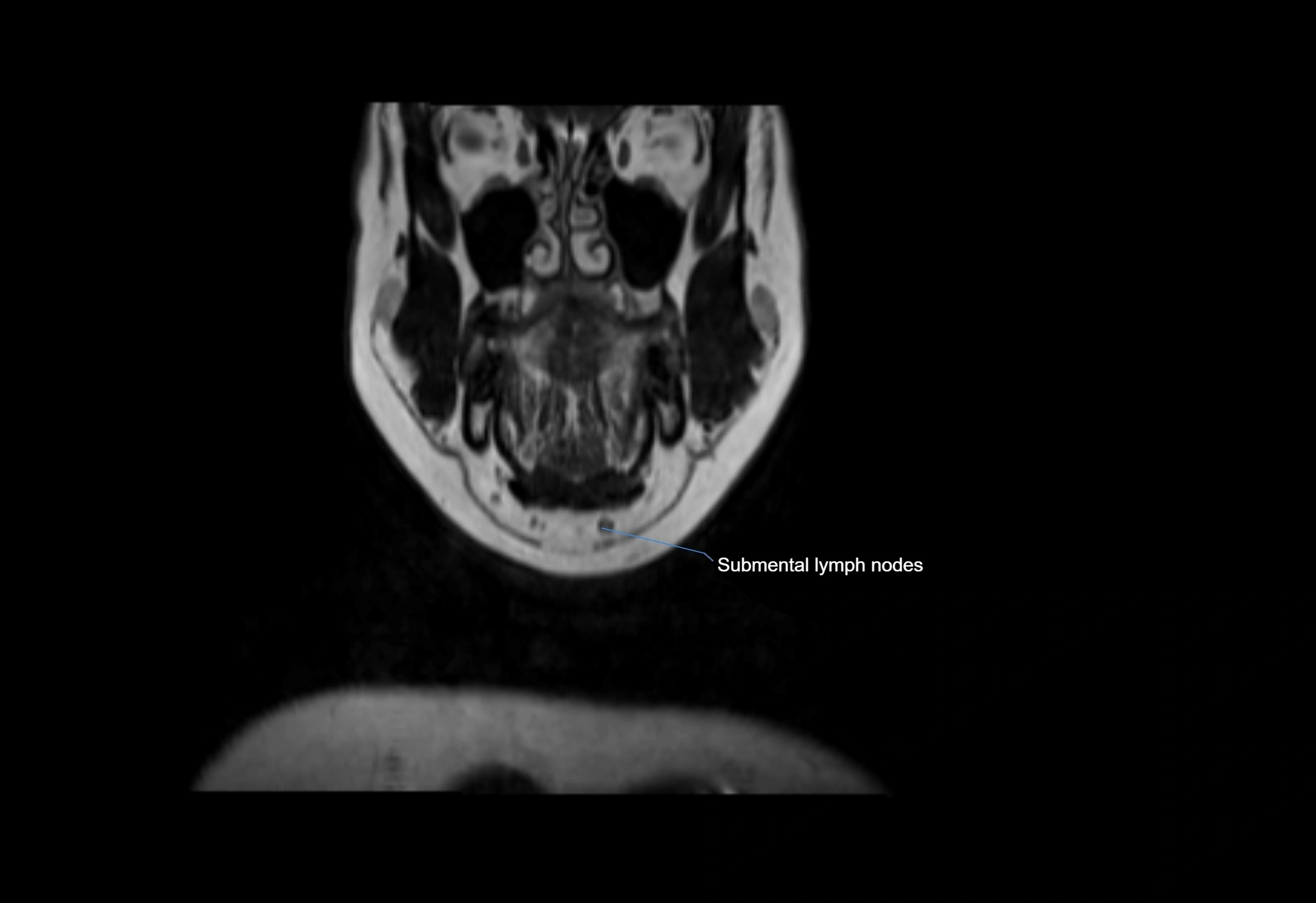
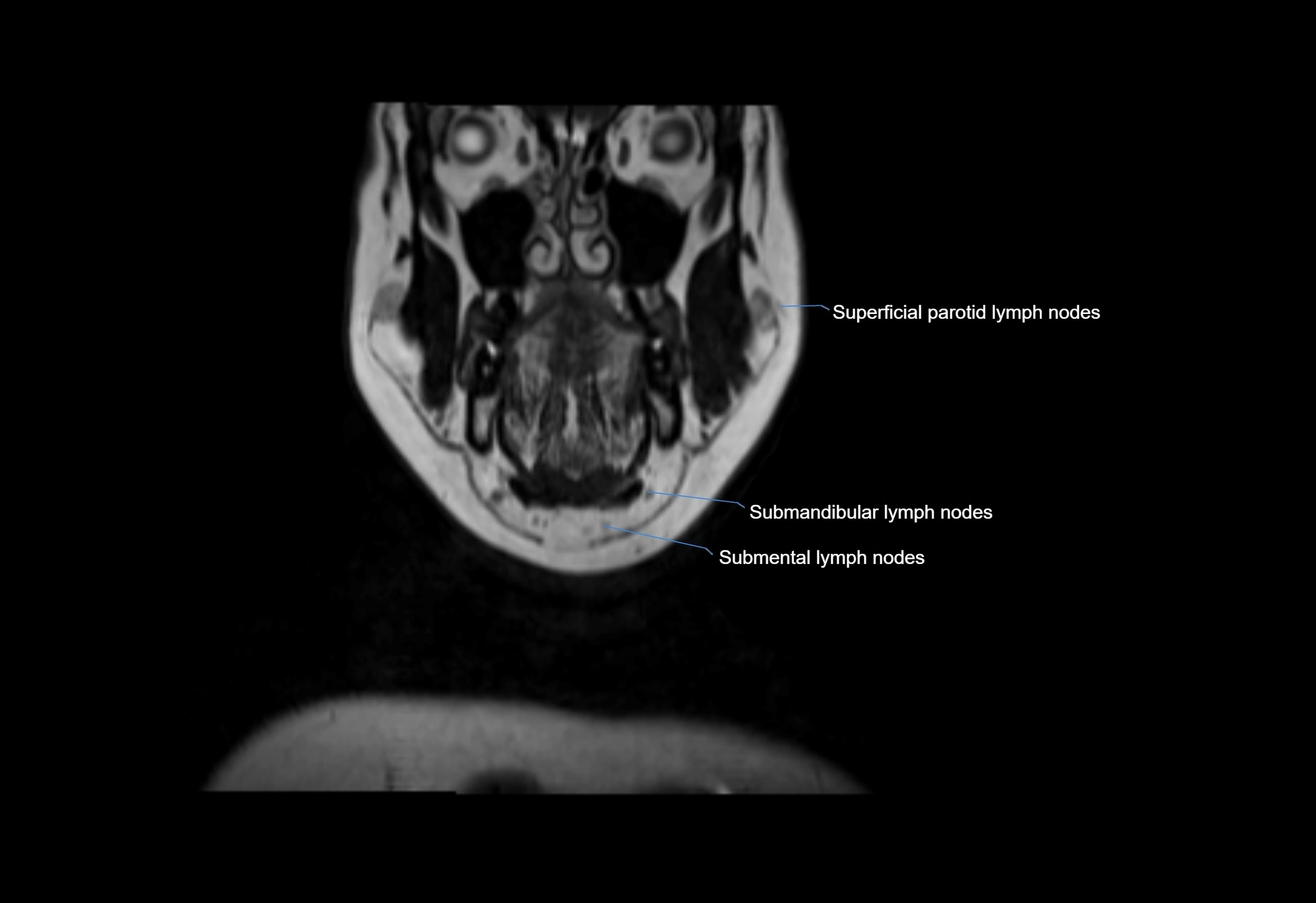
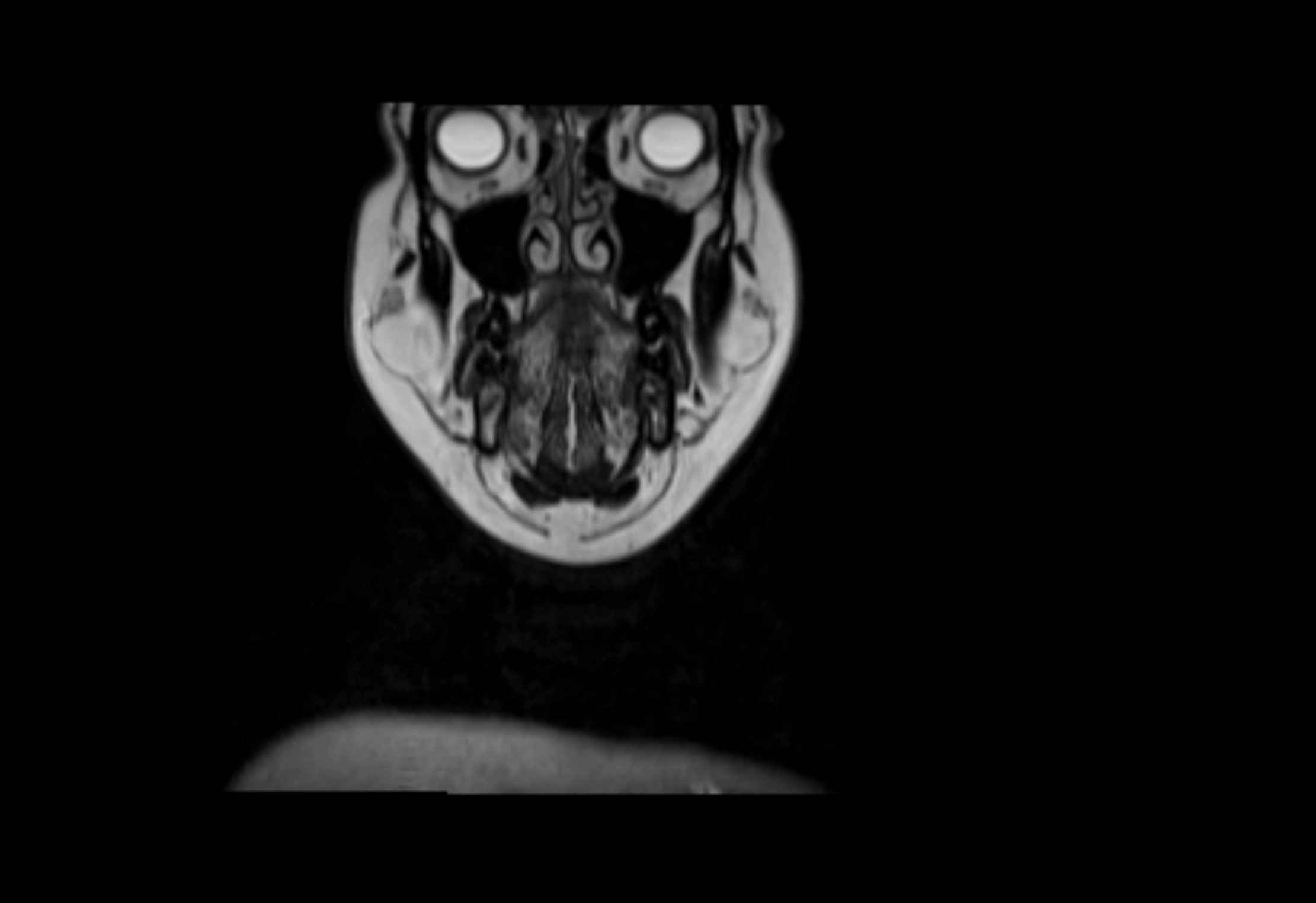
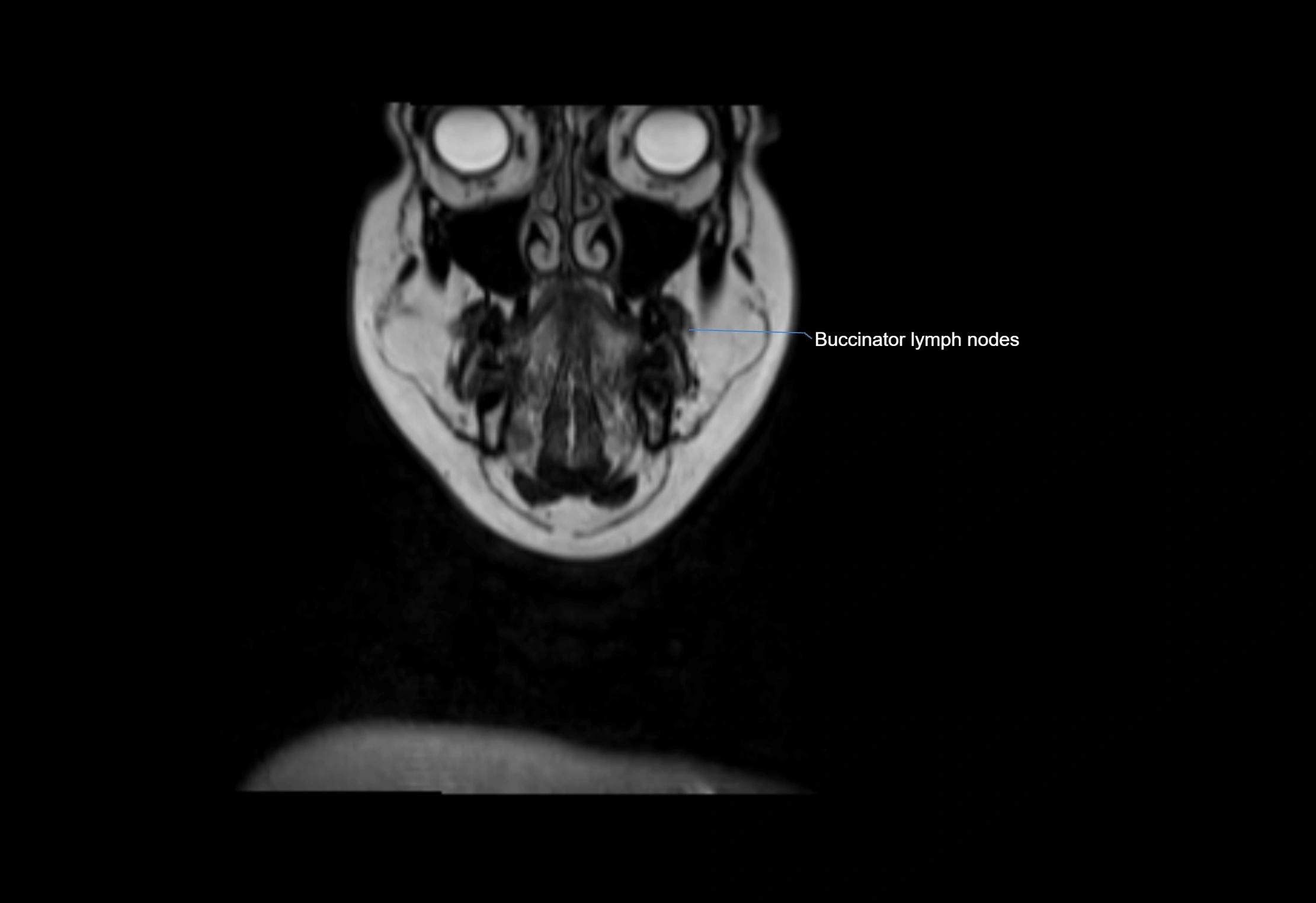
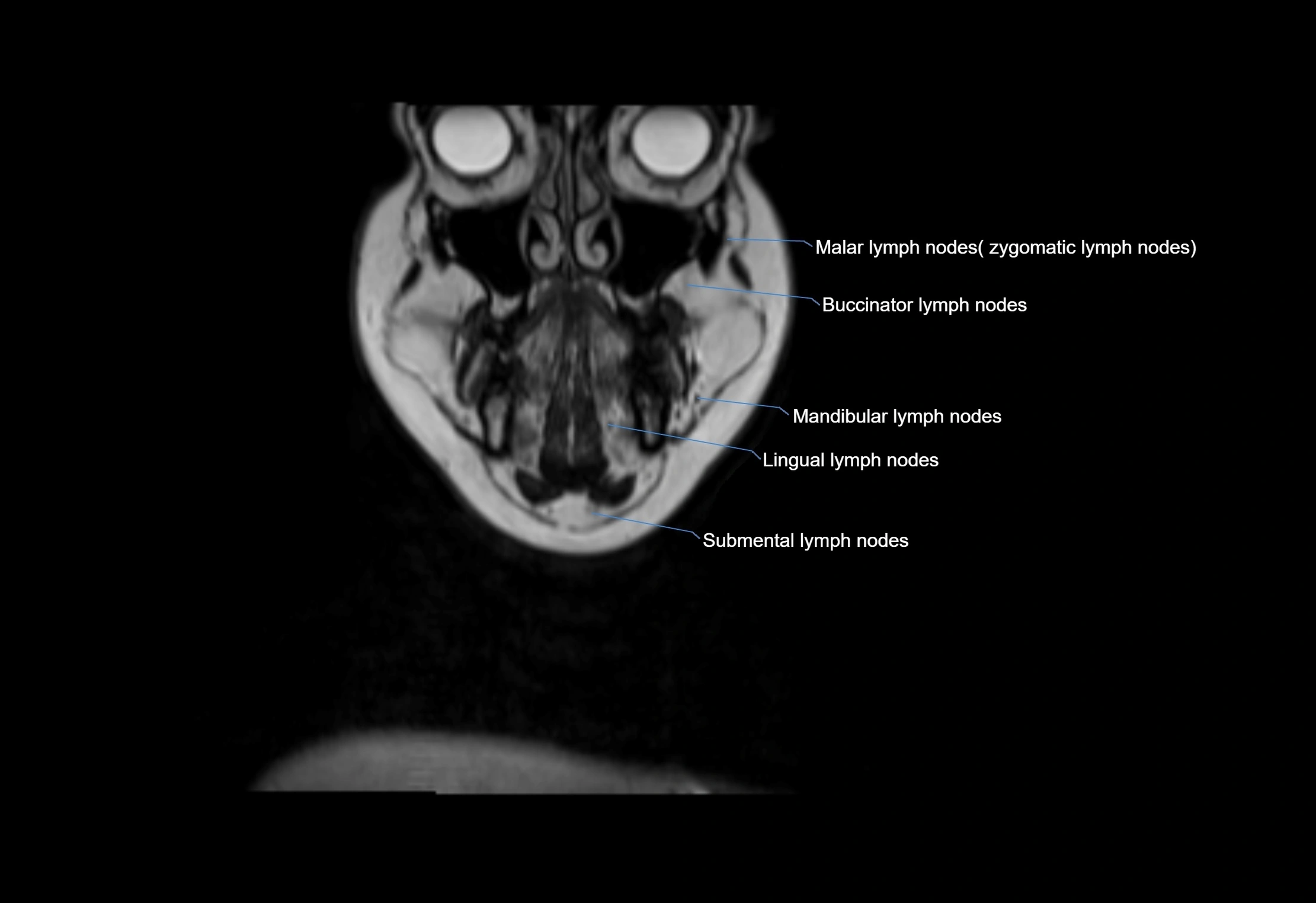
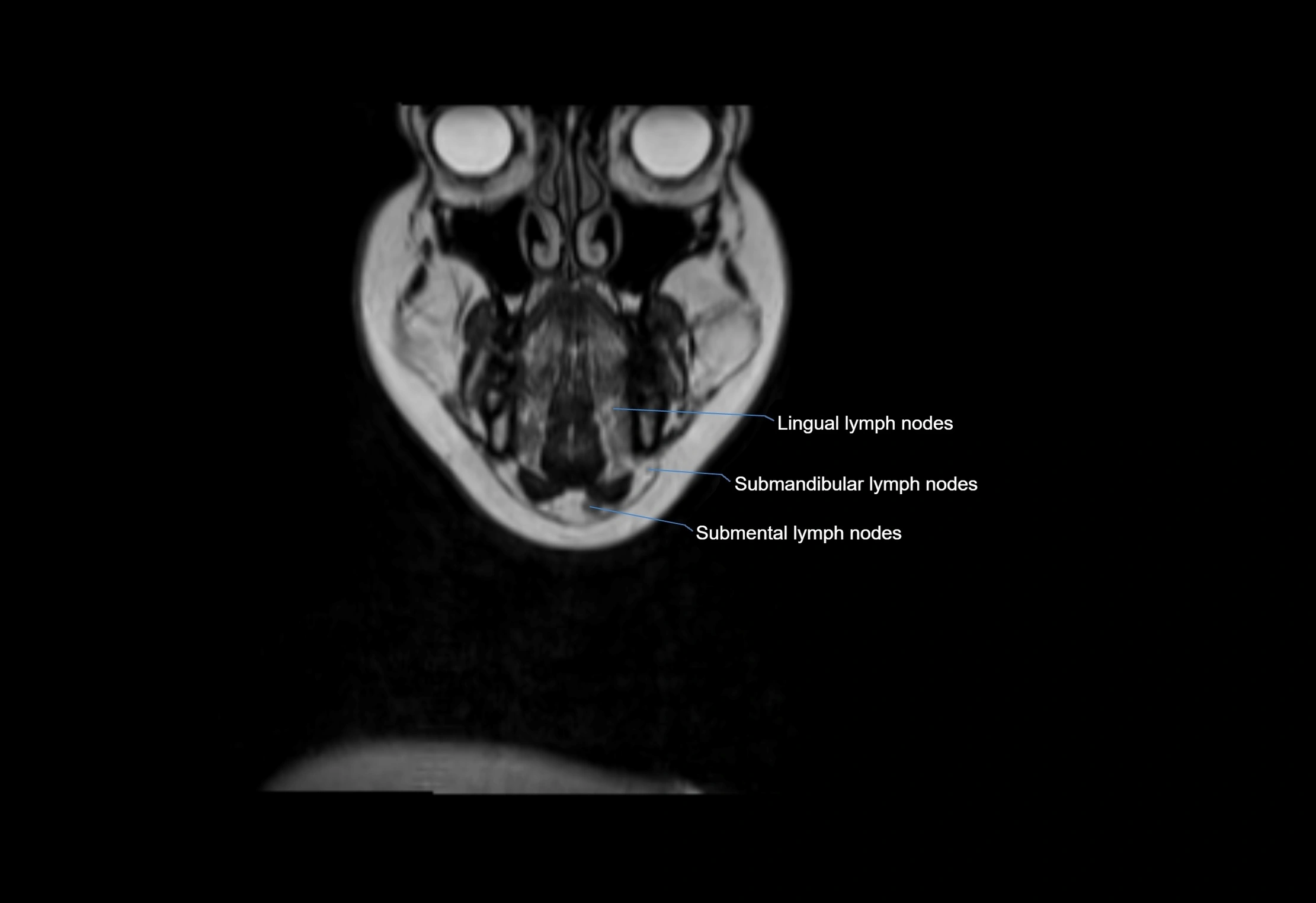
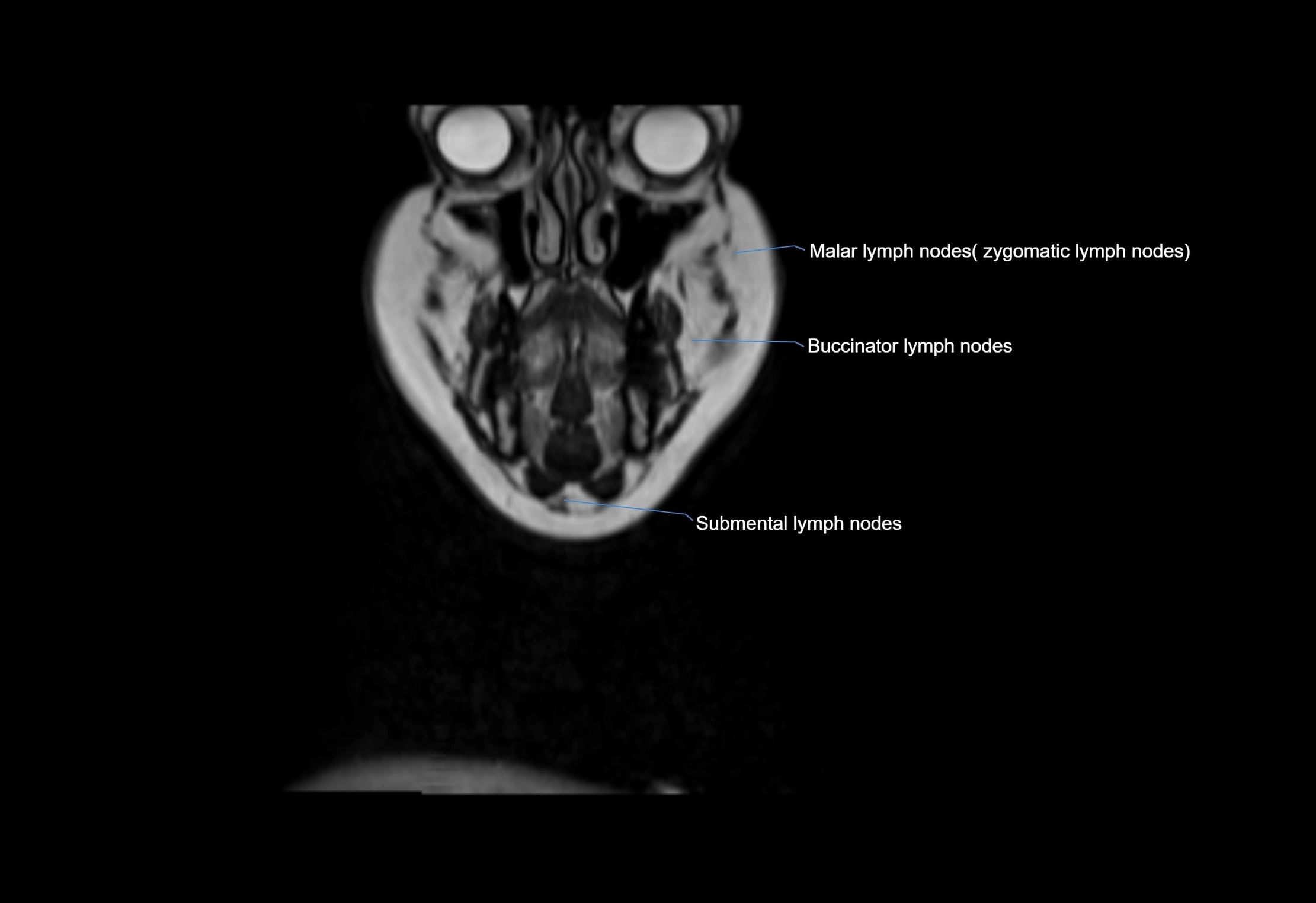
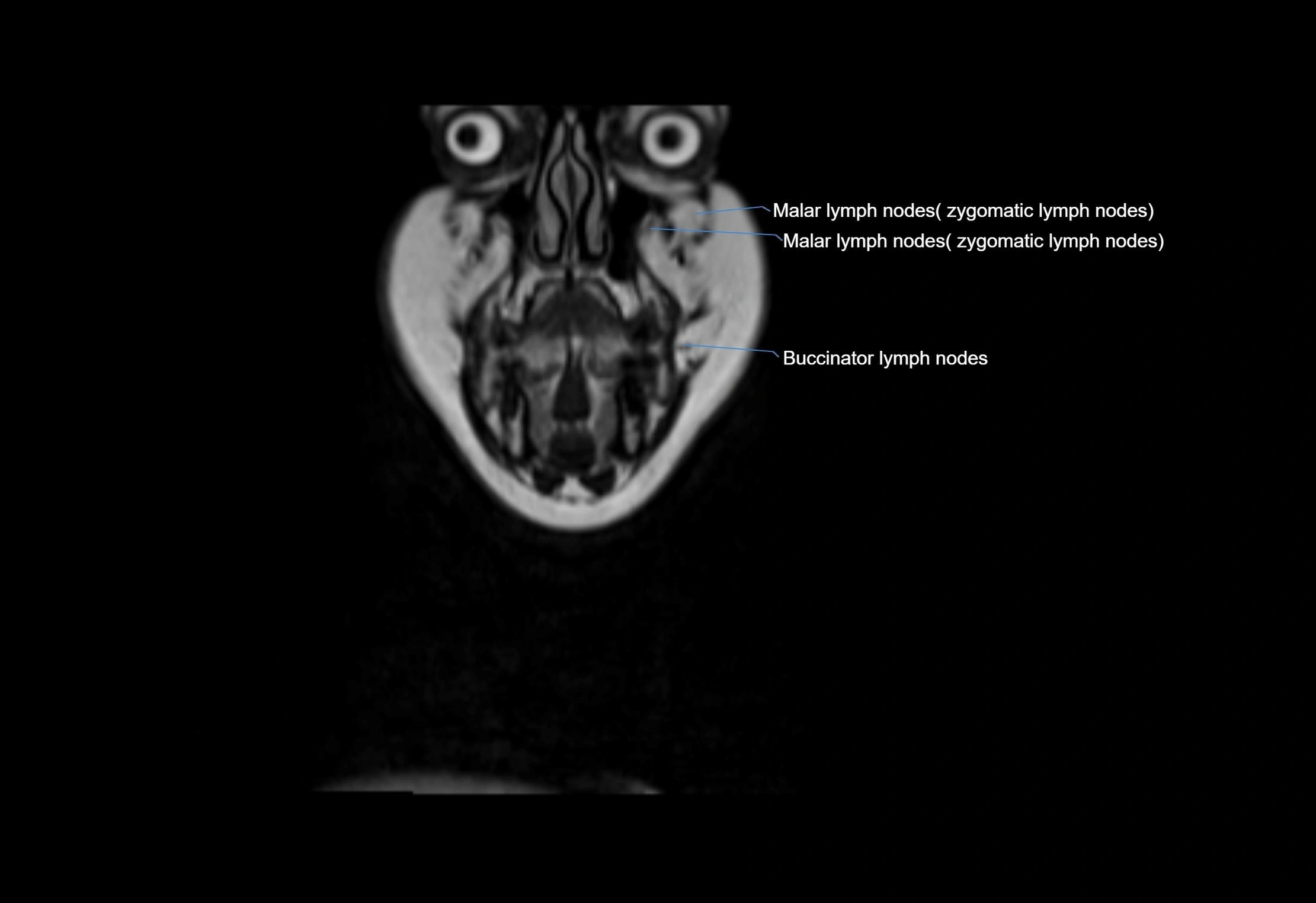
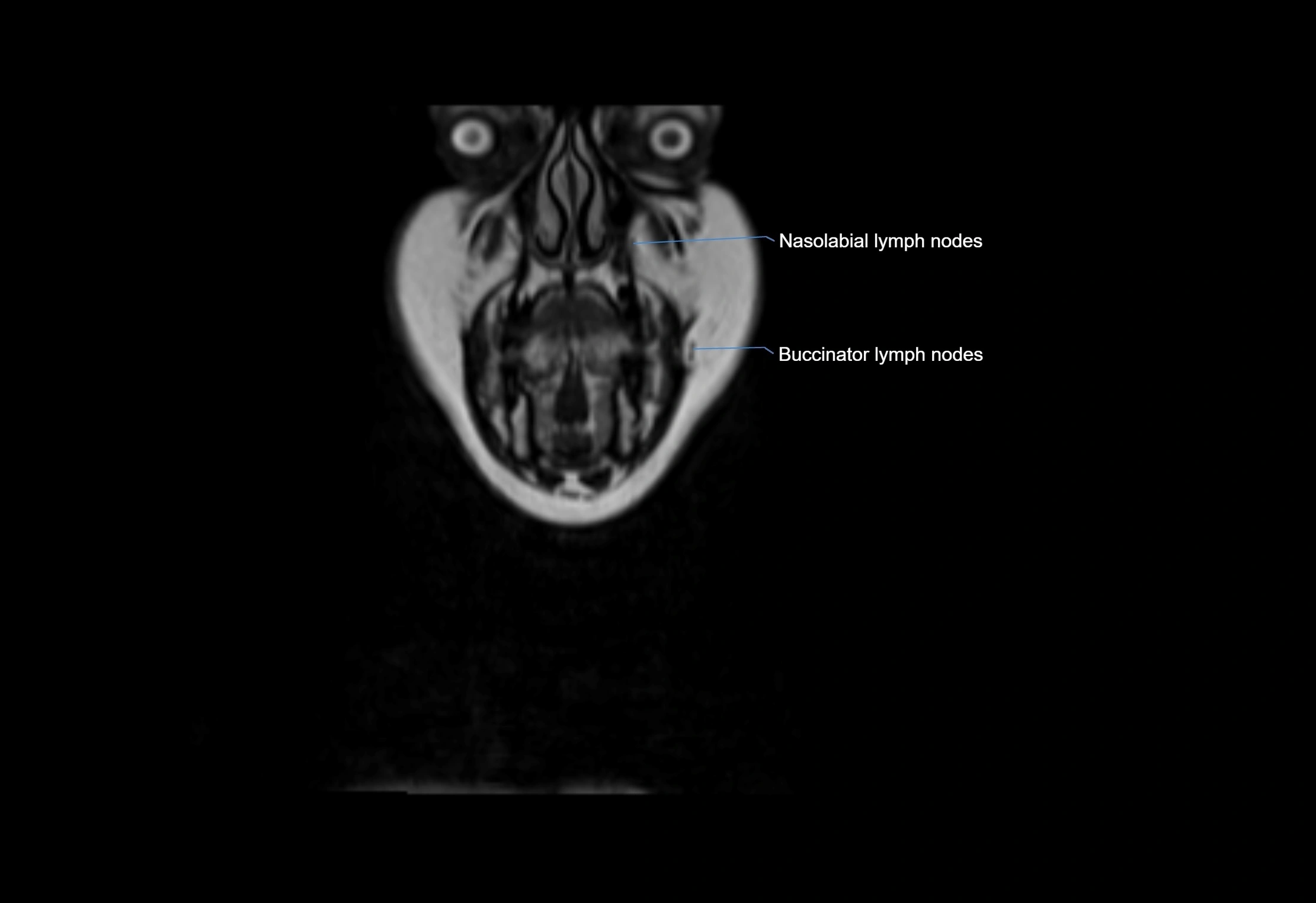
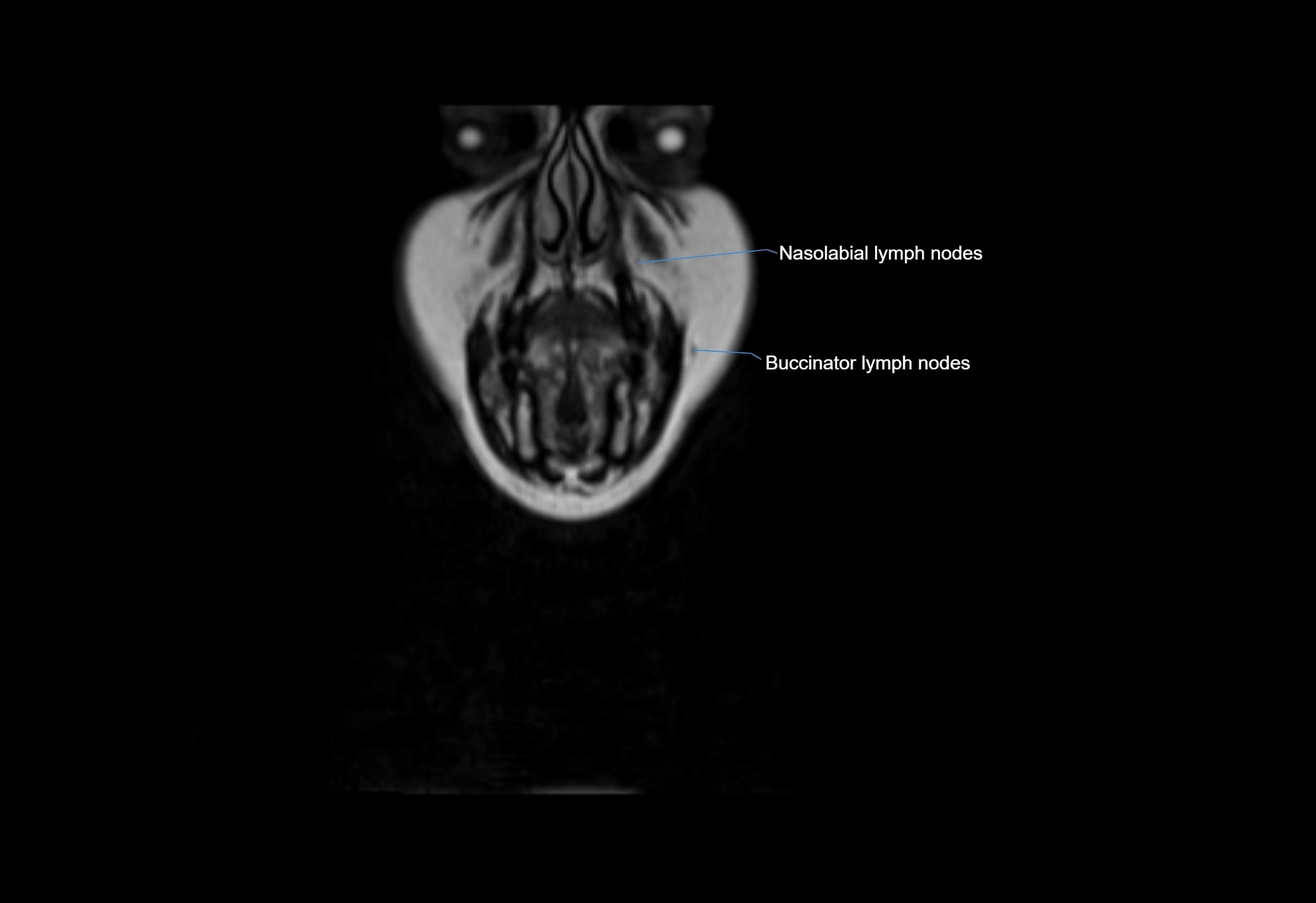
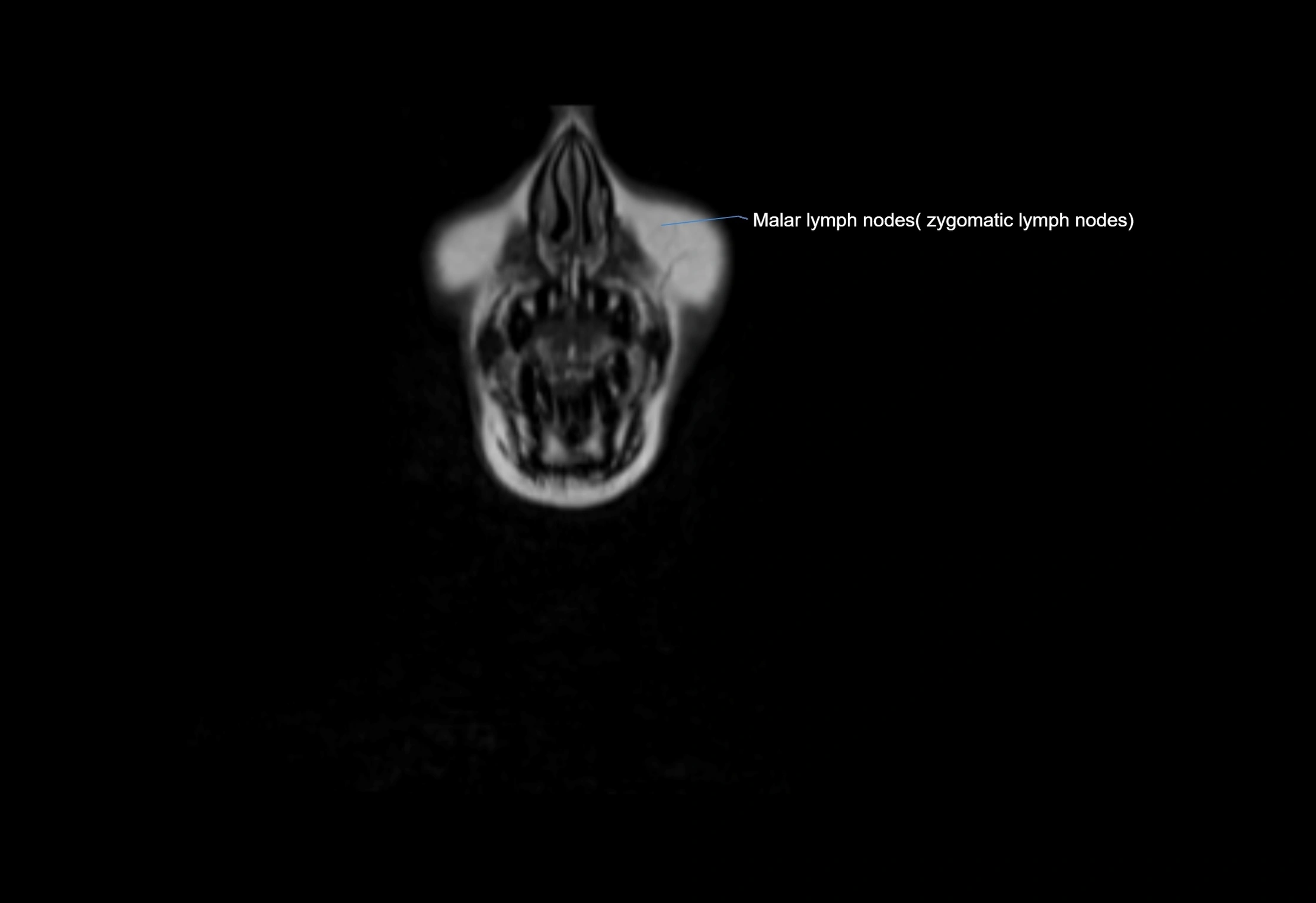
MRI images