


Topic
The anococcygeal nerve is a small sensory nerve derived from the coccygeal plexus, which itself is formed by the ventral rami of S4, S5, and the coccygeal nerve (Co1). Although tiny, this nerve plays an important role in supplying the skin of the coccyx and the area between the anus and coccyx. It passes through the sacrotuberous ligament and runs in the midline behind the coccyx.
Despite its small size, the anococcygeal nerve is clinically important because of its involvement in coccygodynia (coccyx pain) and perineal pain syndromes.
Synonyms
-
Coccygeal cutaneous nerve
-
Terminal branch of coccygeal plexus
Origin, Course, and Branches
-
Origin:
-
Arises from the coccygeal plexus, formed by ventral rami of S4, S5, and Co1
-
-
Course:
-
Emerges through the sacrotuberous ligament near the coccyx
-
Runs in the midline posterior to the coccyx
-
Passes forward into the small space between anus and coccyx
-
-
Branches:
-
Small cutaneous branches that supply the skin between the coccyx and anus
-
Relations
-
Anteriorly: Coccyx and sacrococcygeal joint
-
Posteriorly: Skin of sacrococcygeal region
-
Laterally: Sacrotuberous ligaments
-
Inferiorly: Perianal skin and pelvic floor muscles
Function
-
Provides sensory innervation to the skin of the coccyx
-
Supplies sensation to the small perianal area between anus and coccyx
-
Contributes to sensory input involved in pain syndromes of the coccygeal region
Clinical Significance
-
Involved in coccygodynia (tailbone pain)
-
Can be damaged during coccyx fractures, childbirth trauma, or pelvic surgery
-
Target for nerve blocks in chronic coccygeal pain
-
May mimic or be involved in perineal neuralgias
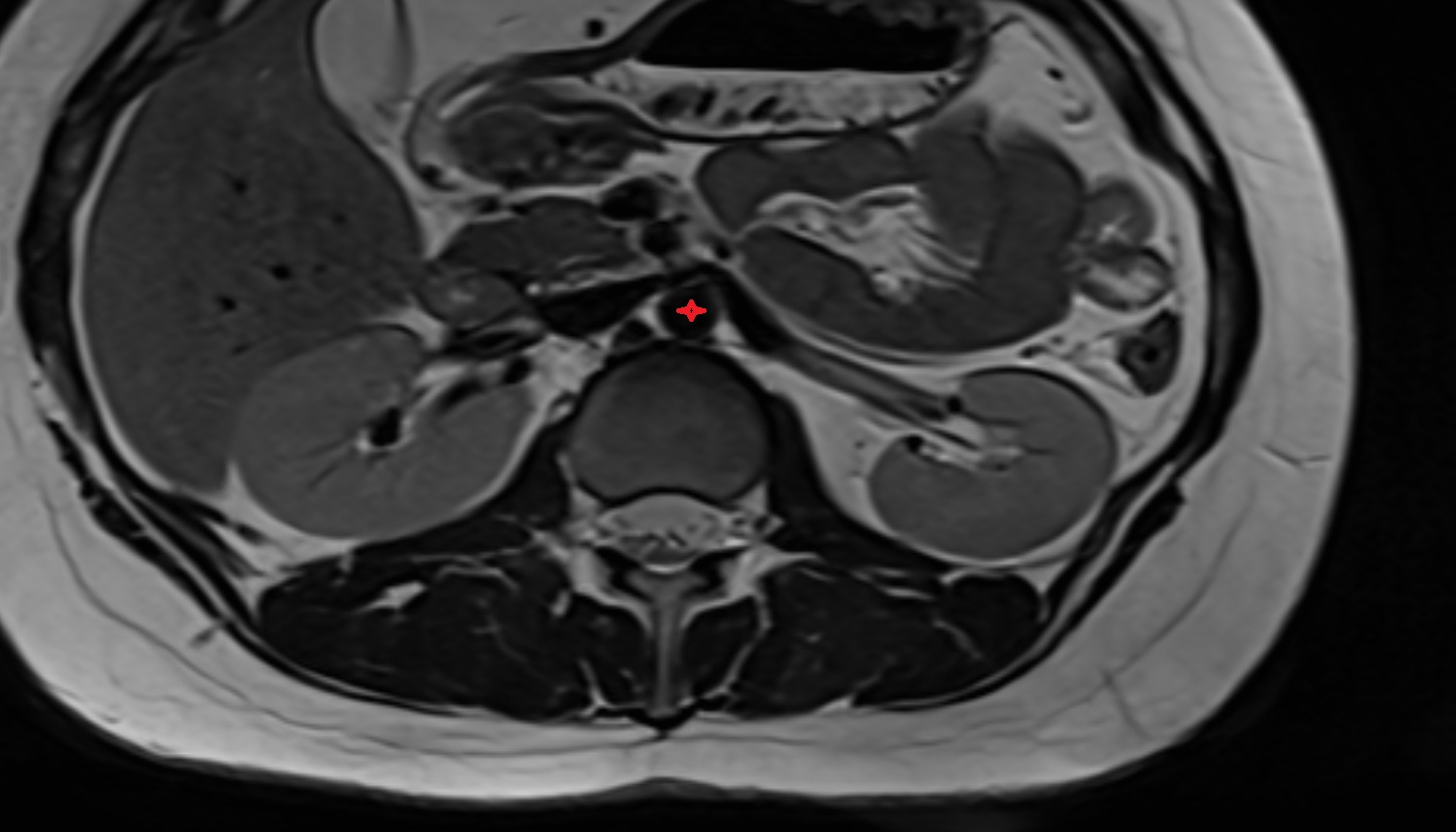
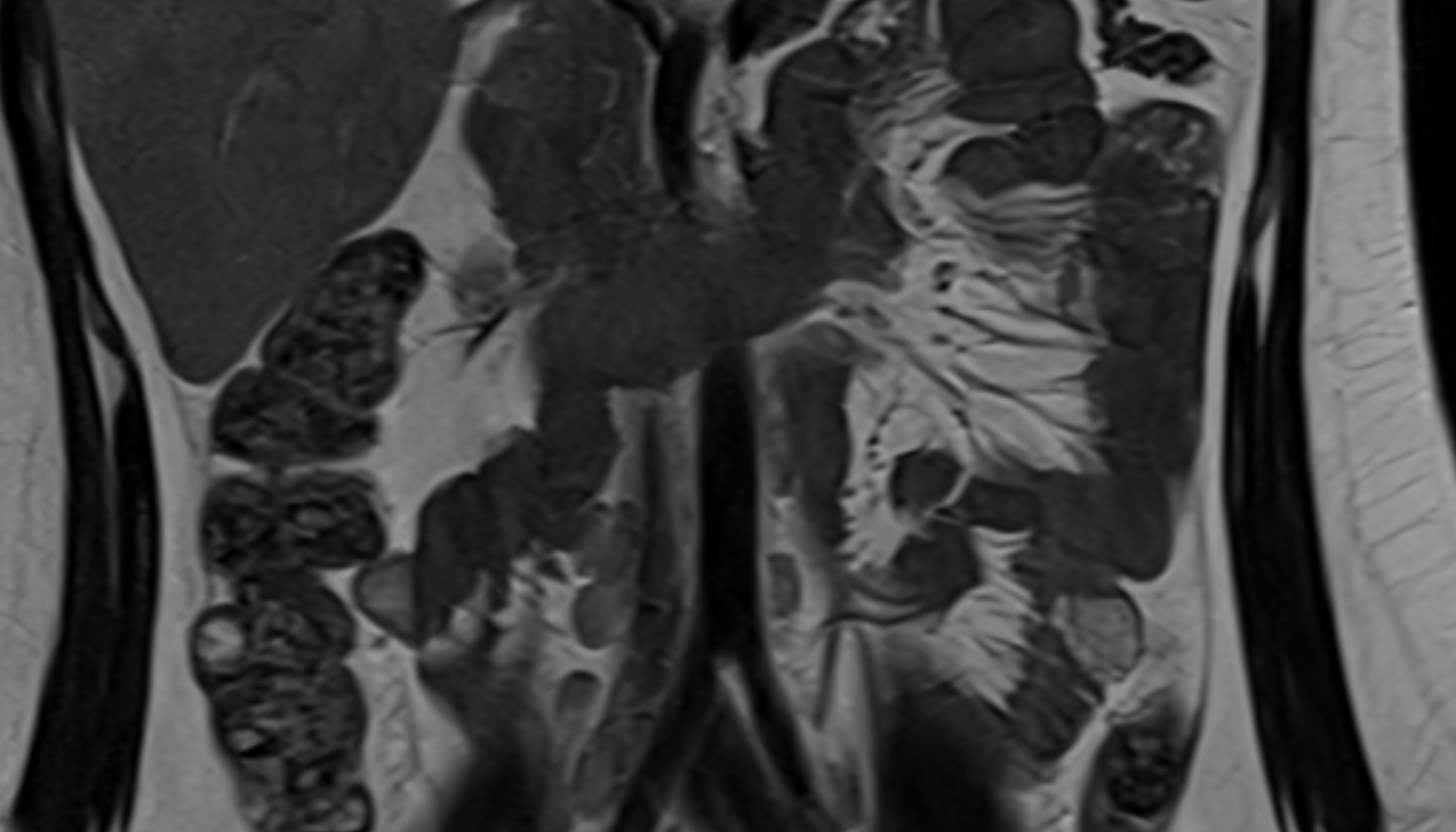
MRI Appearance
T1-weighted images:
-
Nerve appears as a very thin low-to-intermediate signal intensity structure
-
Surrounded by bright fat, aiding visualization
T2-weighted images:
-
Nerve shows intermediate to mildly hyperintense signal compared to muscle
-
Pathological involvement appears brighter
STIR (Short Tau Inversion Recovery):
-
Normal nerve appears dark
-
Inflamed or entrapped nerve appears bright hyperintense
T1 Fat-Sat Post-Contrast:
-
Normal nerve enhances minimally
-
Pathologic nerve (neuritis, entrapment, tumor infiltration) shows focal or diffuse enhancement
3D T2 SPACE / CISS:
-
Nerve appears intermediate to mildly hyperintense compared to muscle
-
Surrounded by bright fat or CSF, improving visualization
-
Best sequence for mapping small pelvic nerves such as the anococcygeal
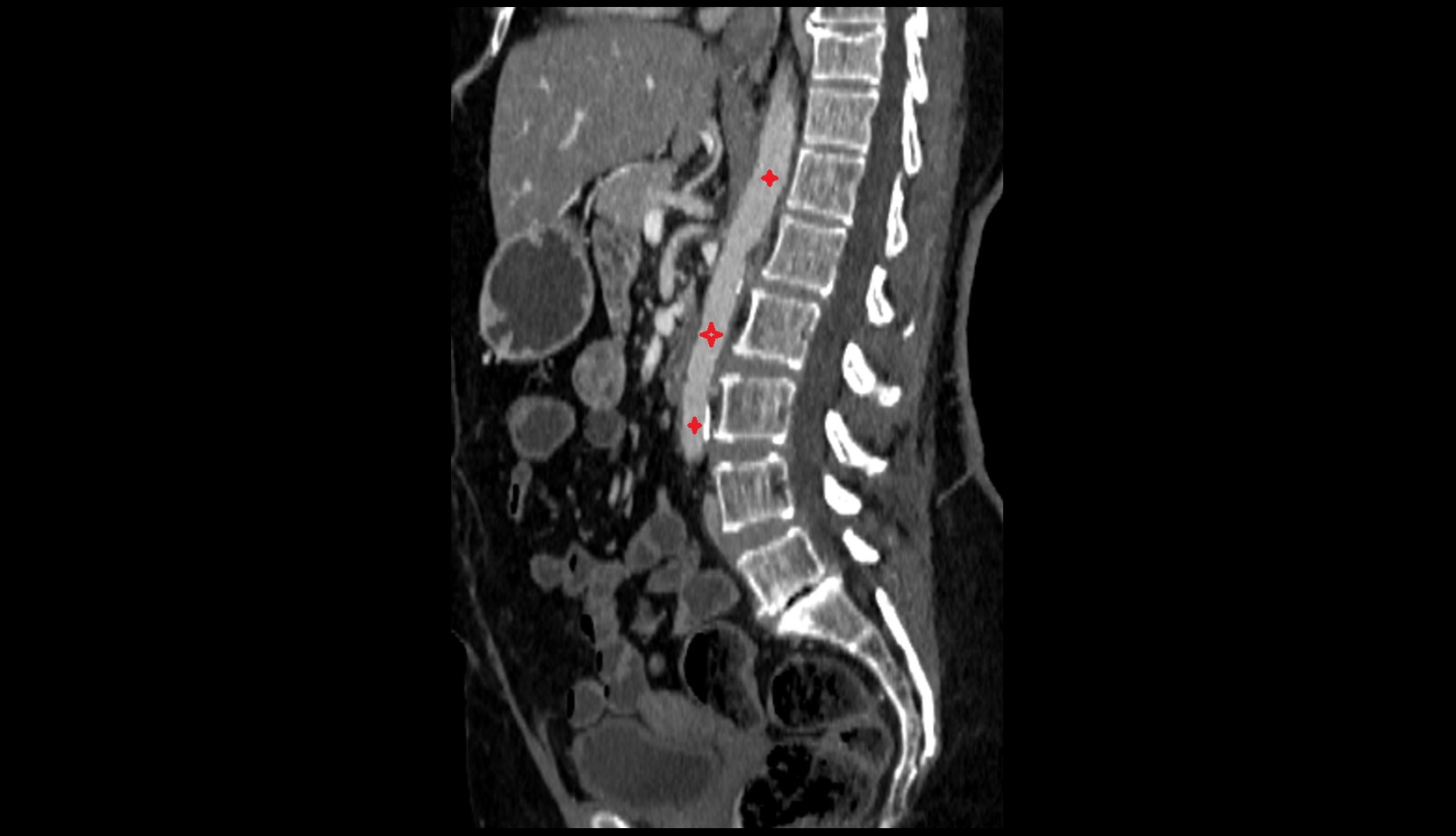
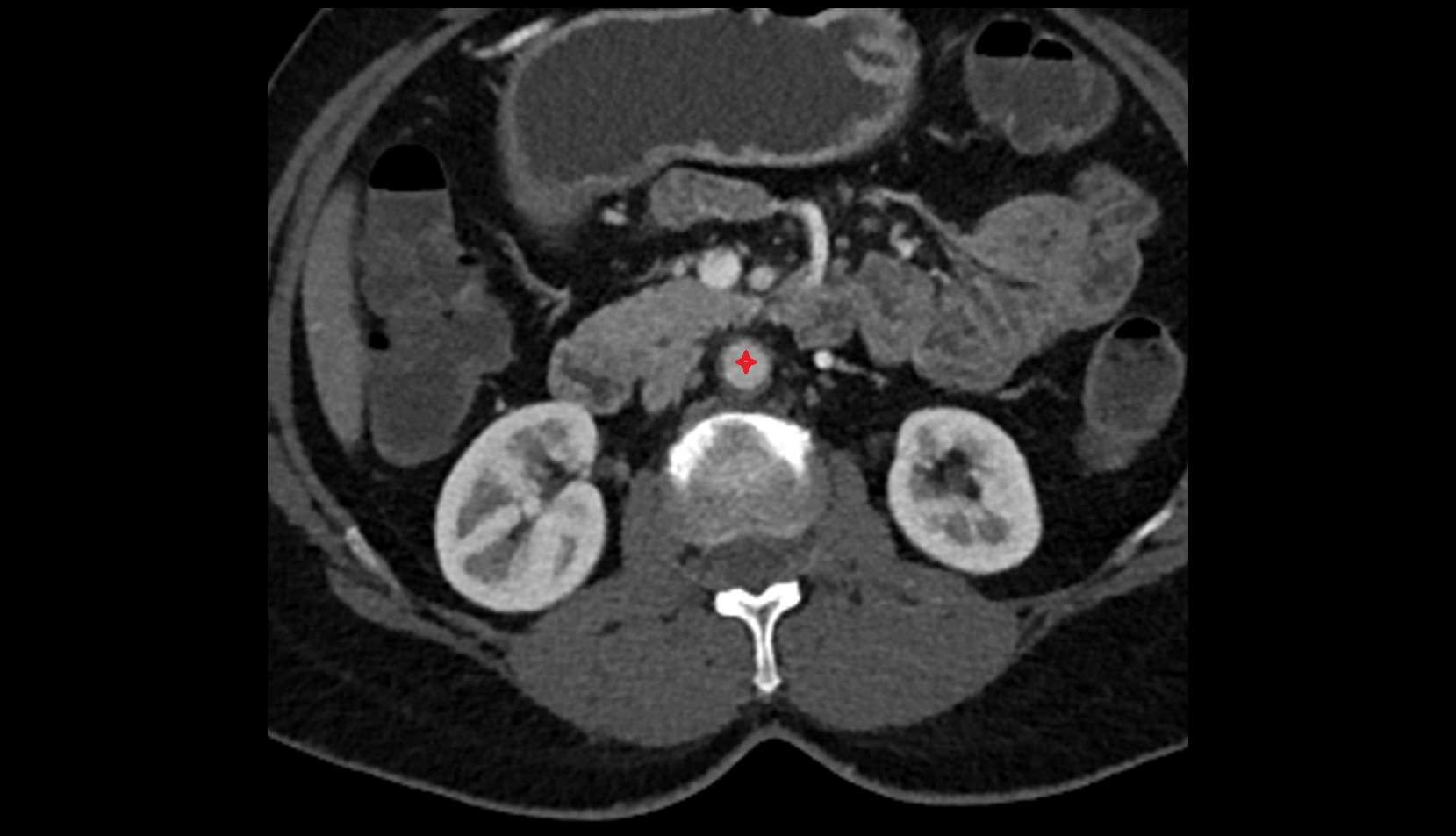
CT Appearance
Non-Contrast CT:
-
Nerve not directly visualized; location inferred posterior to coccyx within fat plane
-
Coccygeal fractures or bony spurs may impinge on its course
Post-Contrast CT:
-
Nerve itself does not enhance
-
Pathology such as inflammatory infiltration or neoplasm may appear as enhancing soft tissue in region of nerve
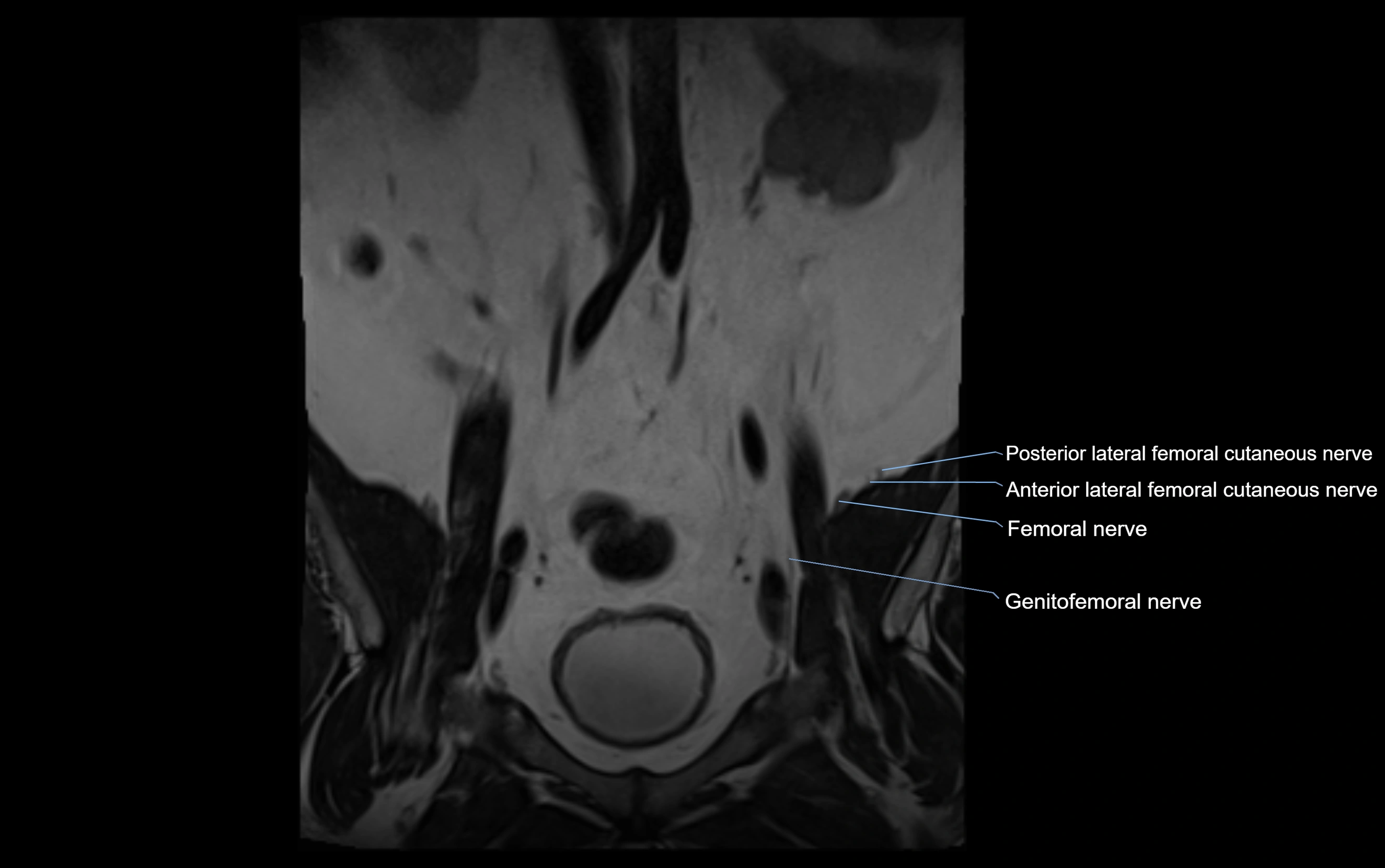
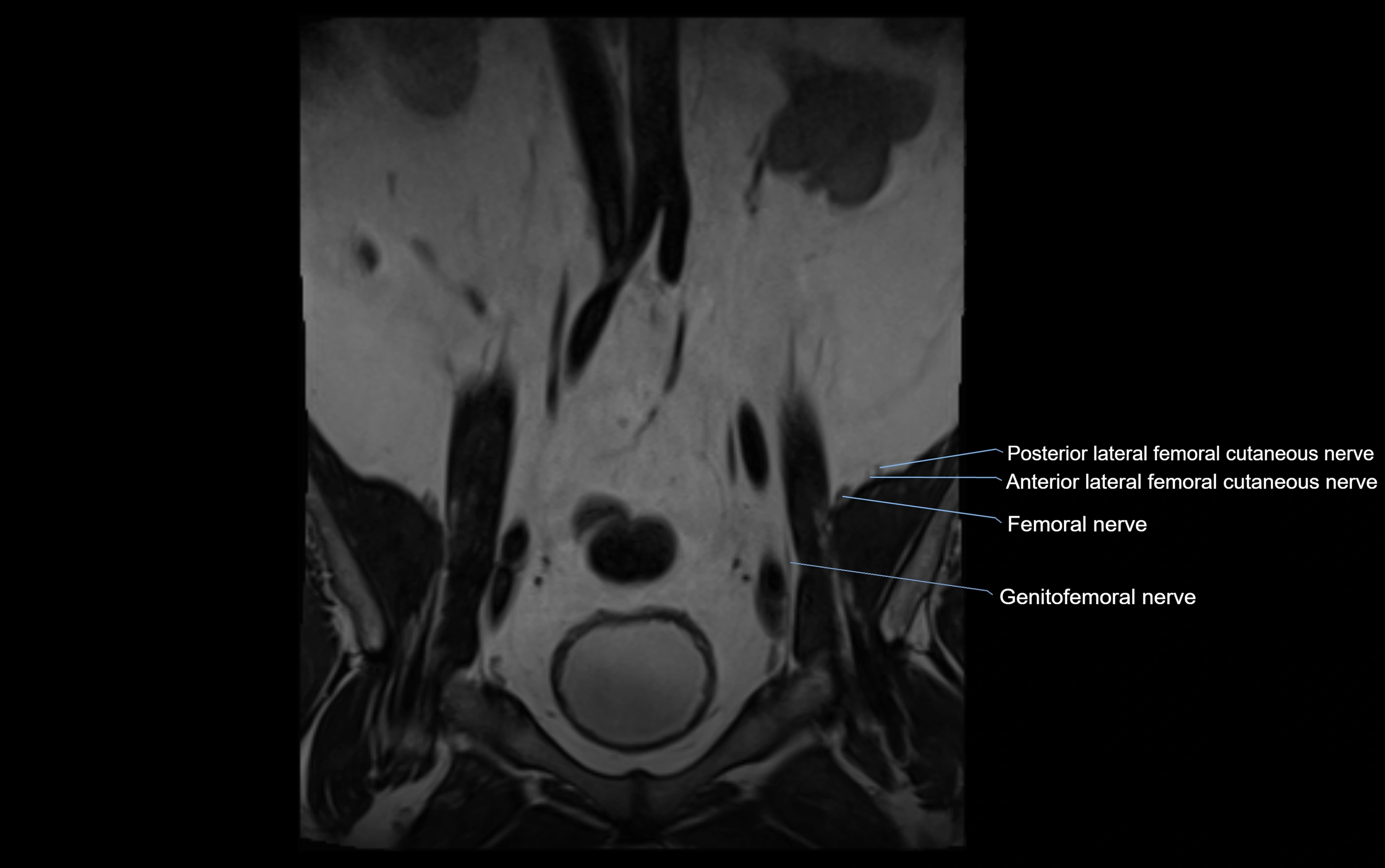
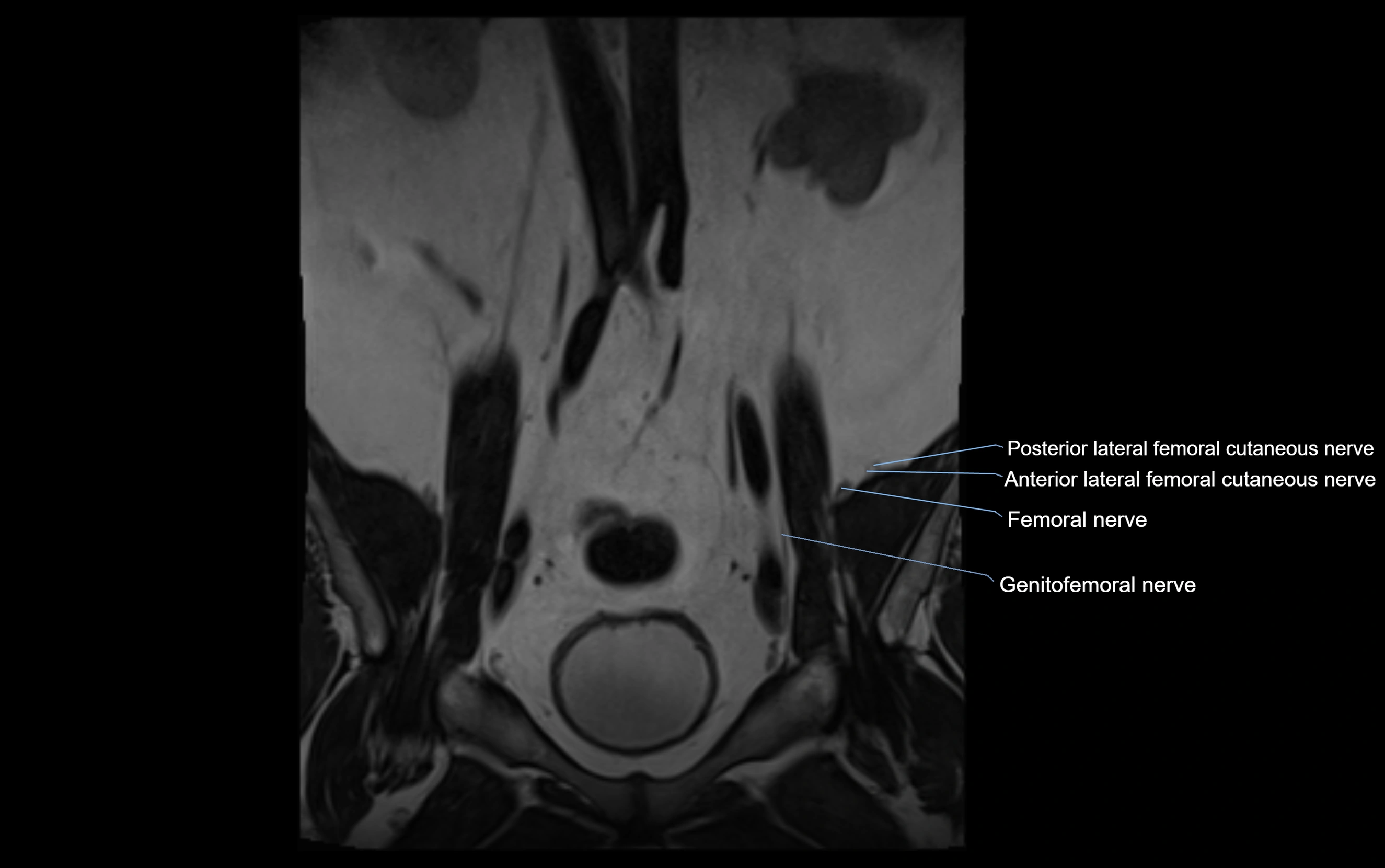
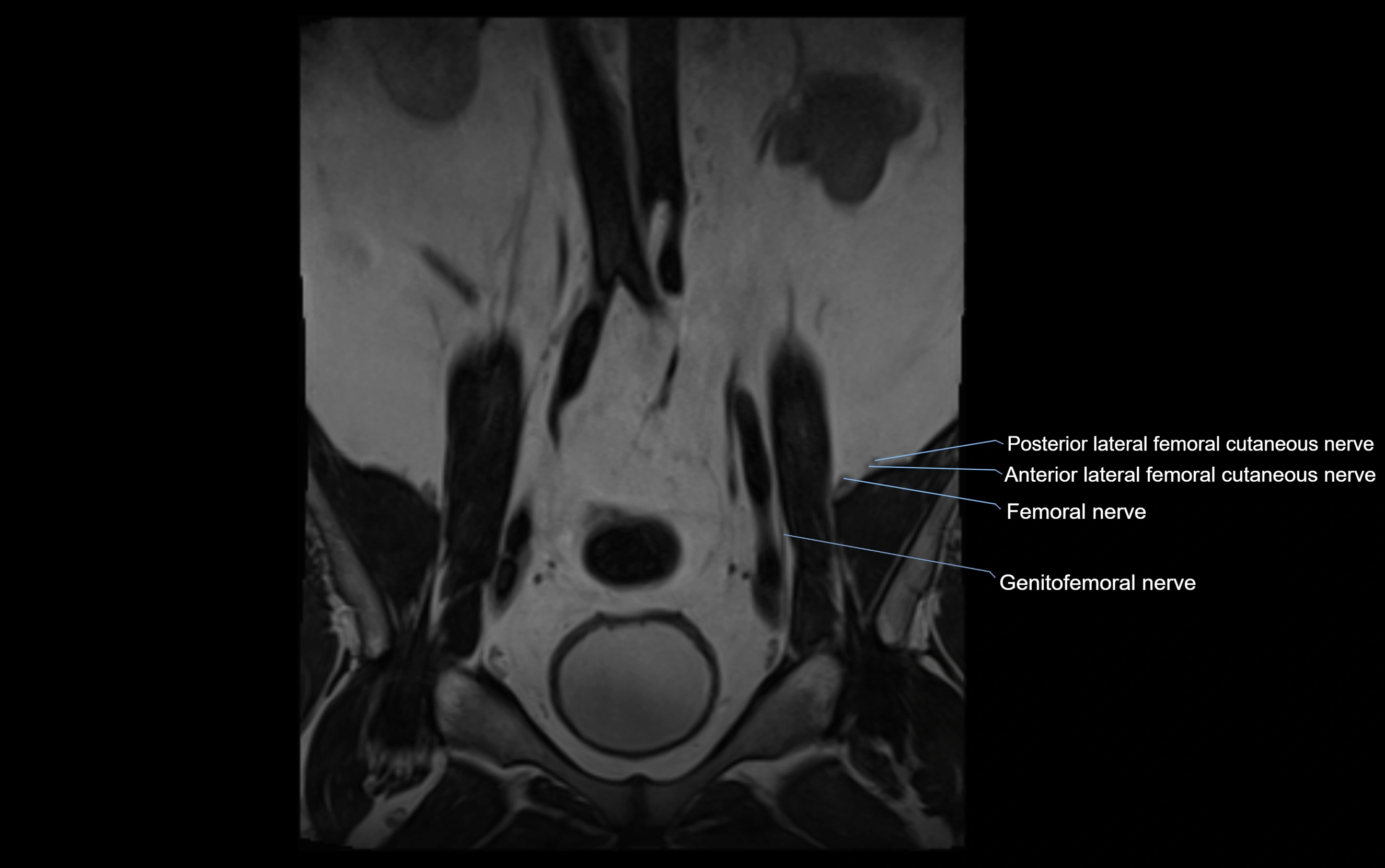
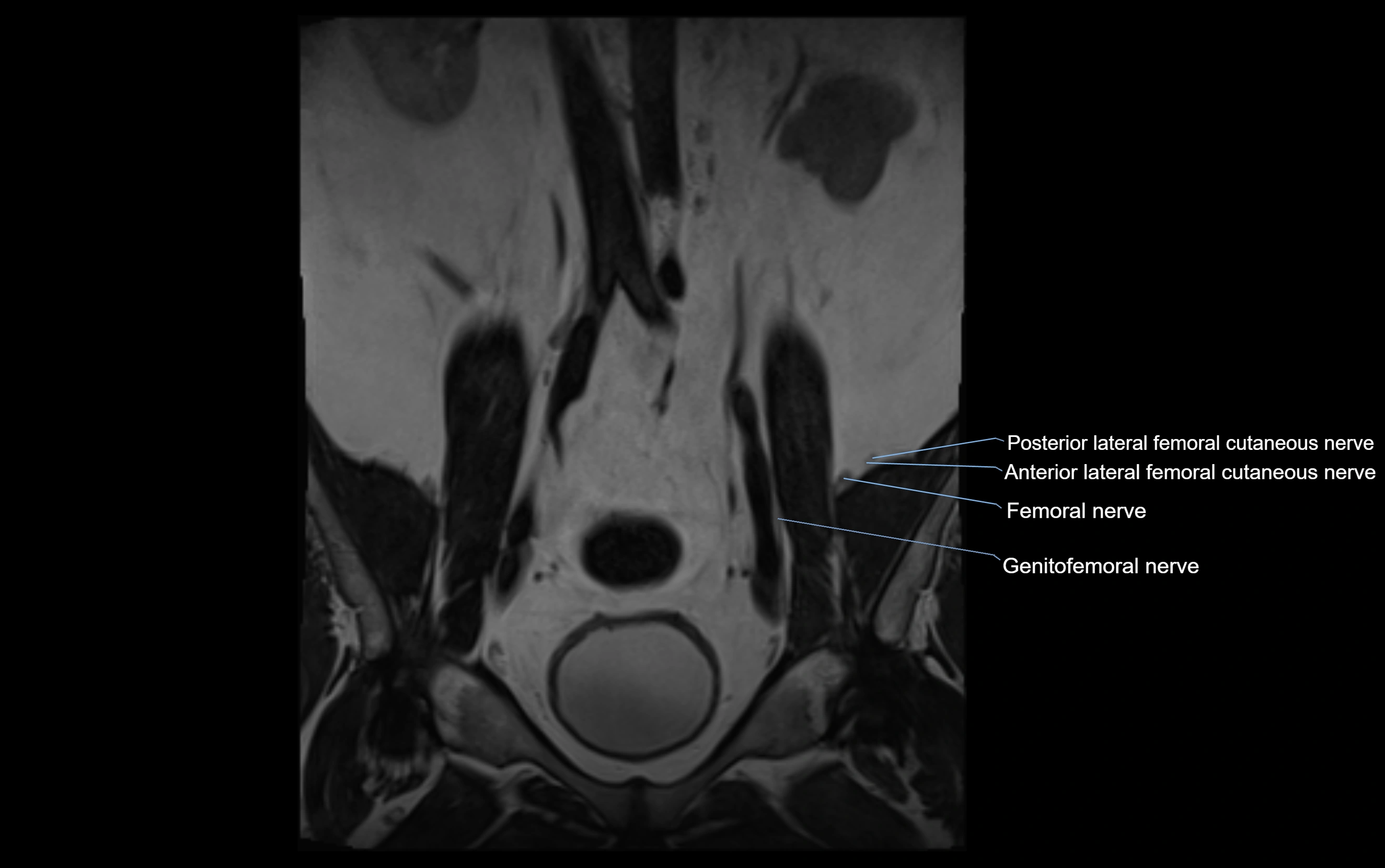
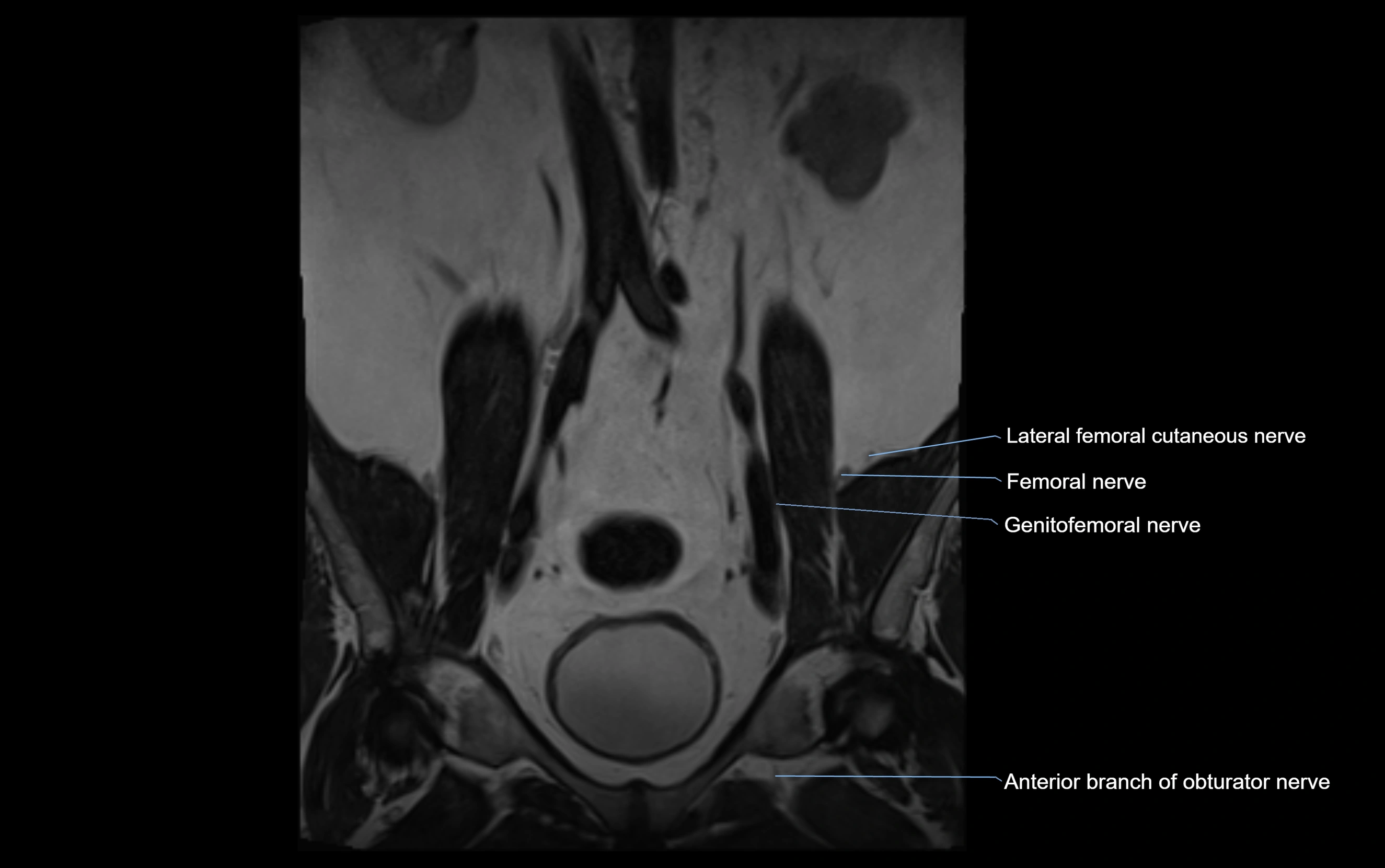
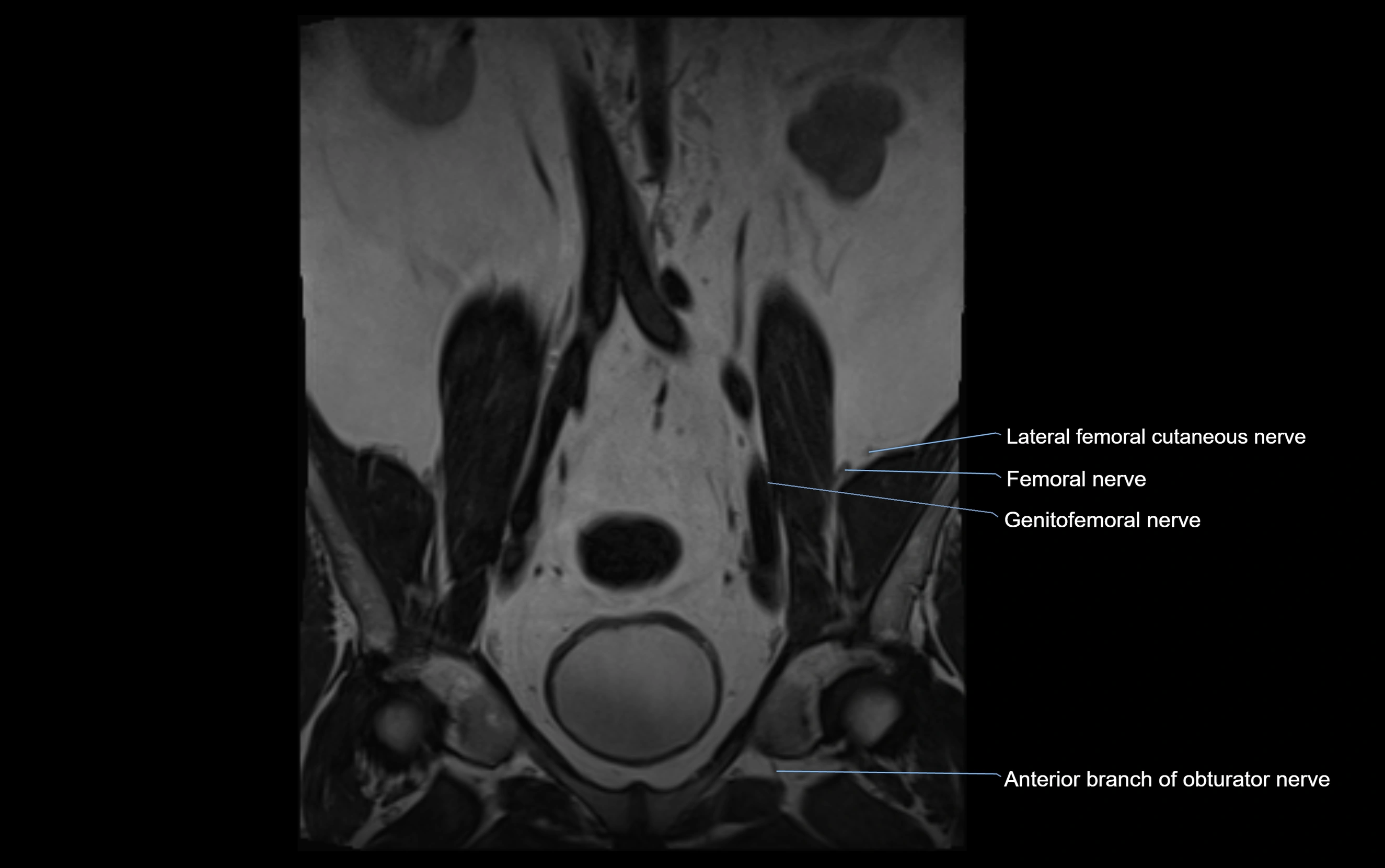
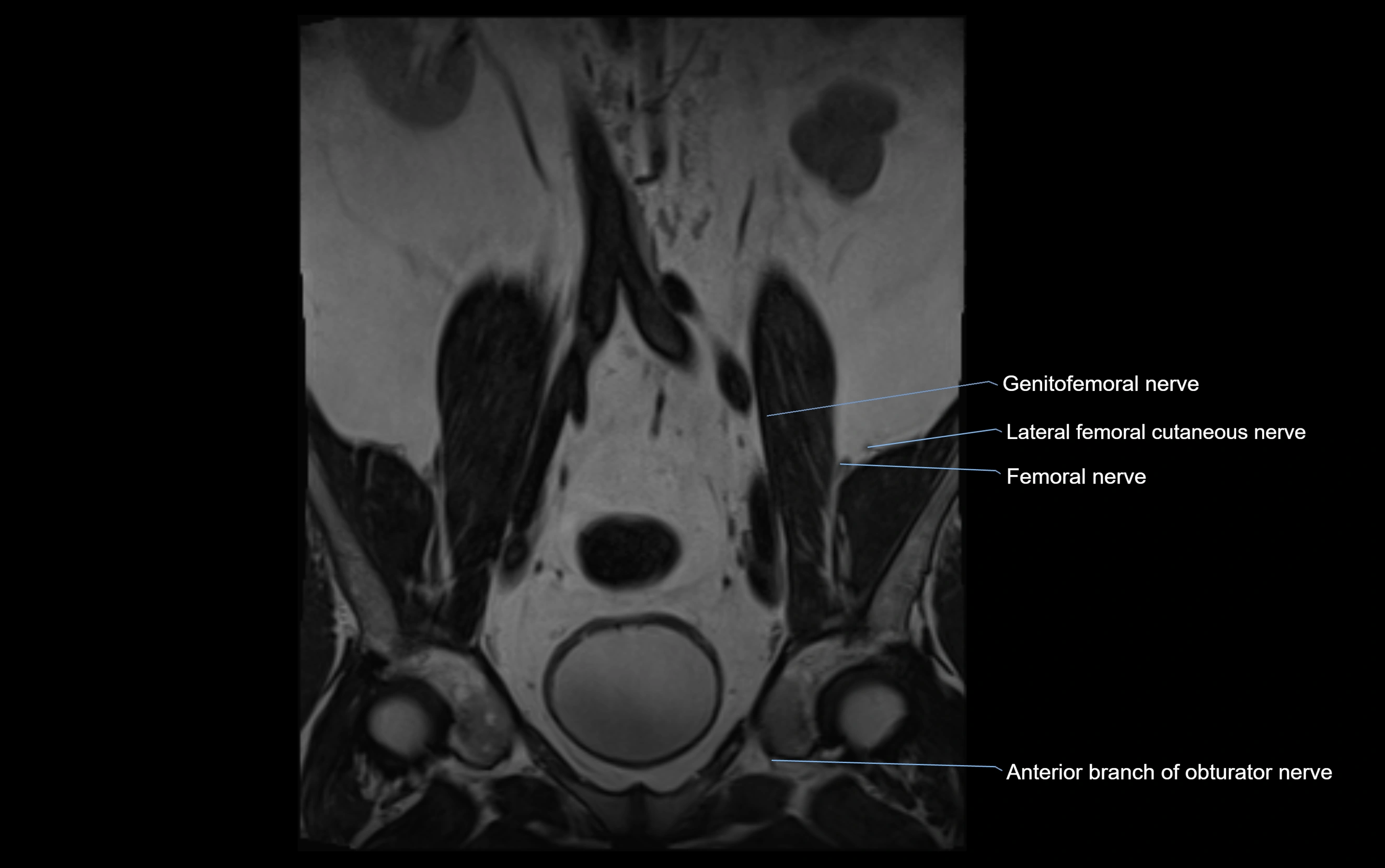
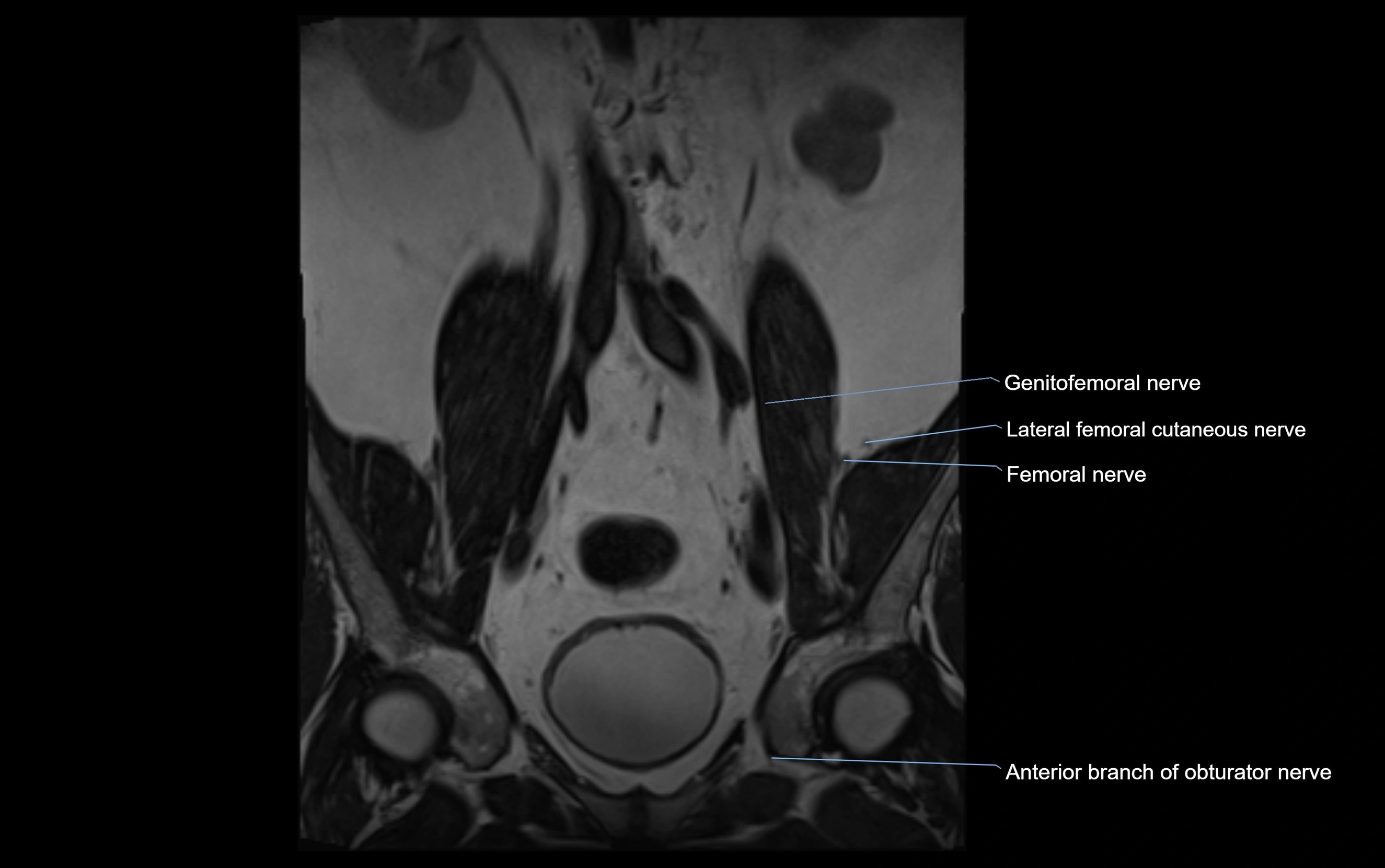
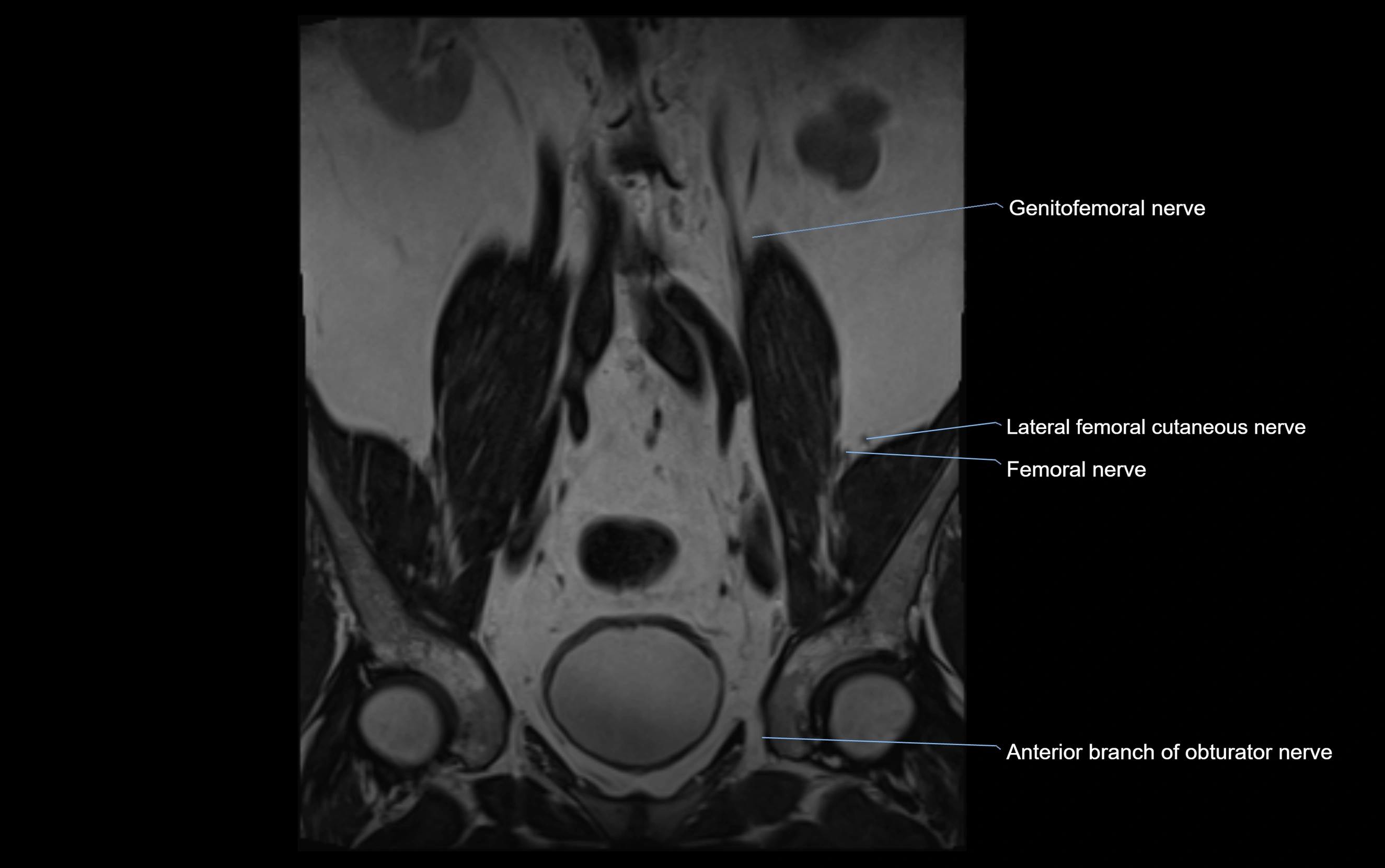
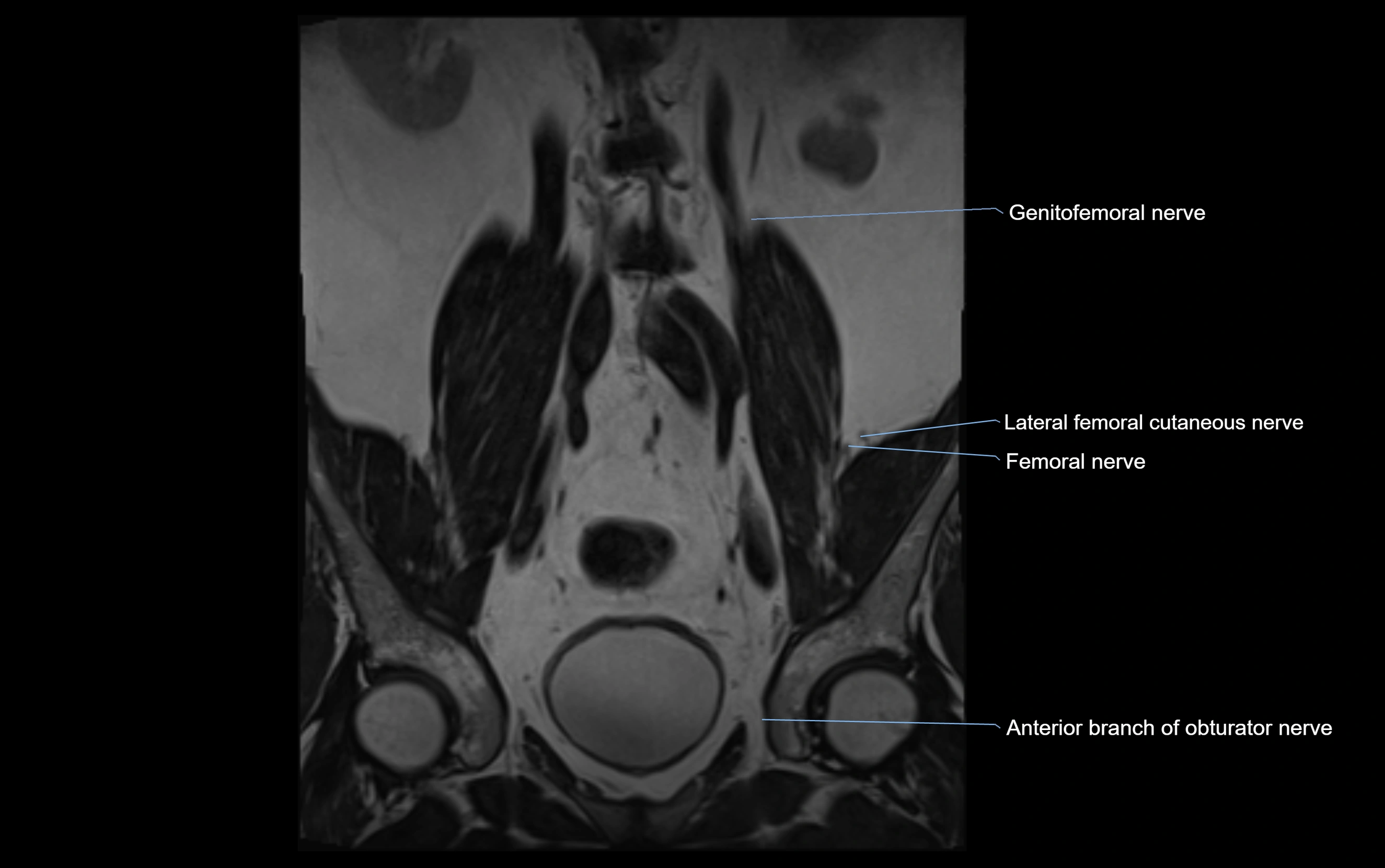
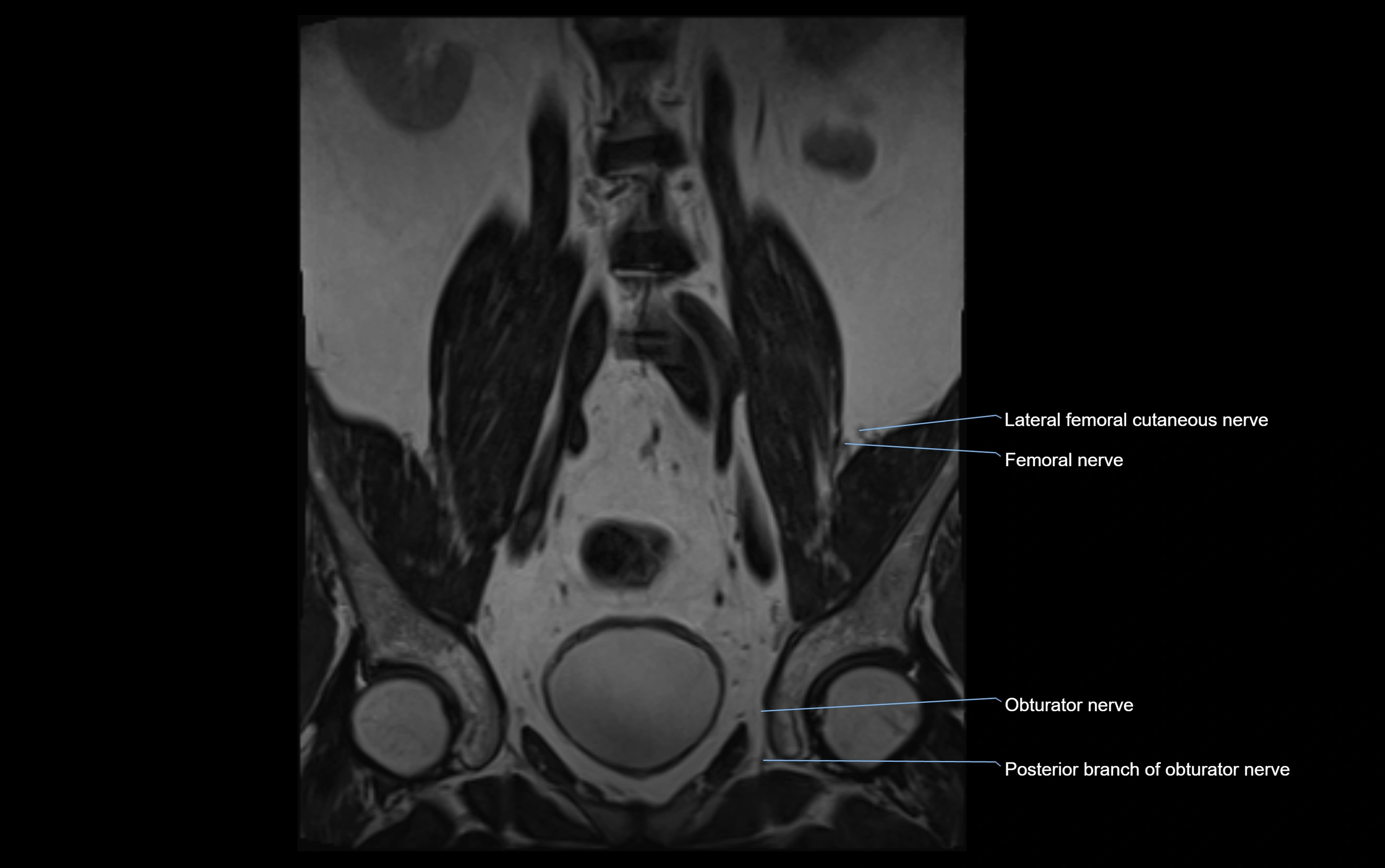
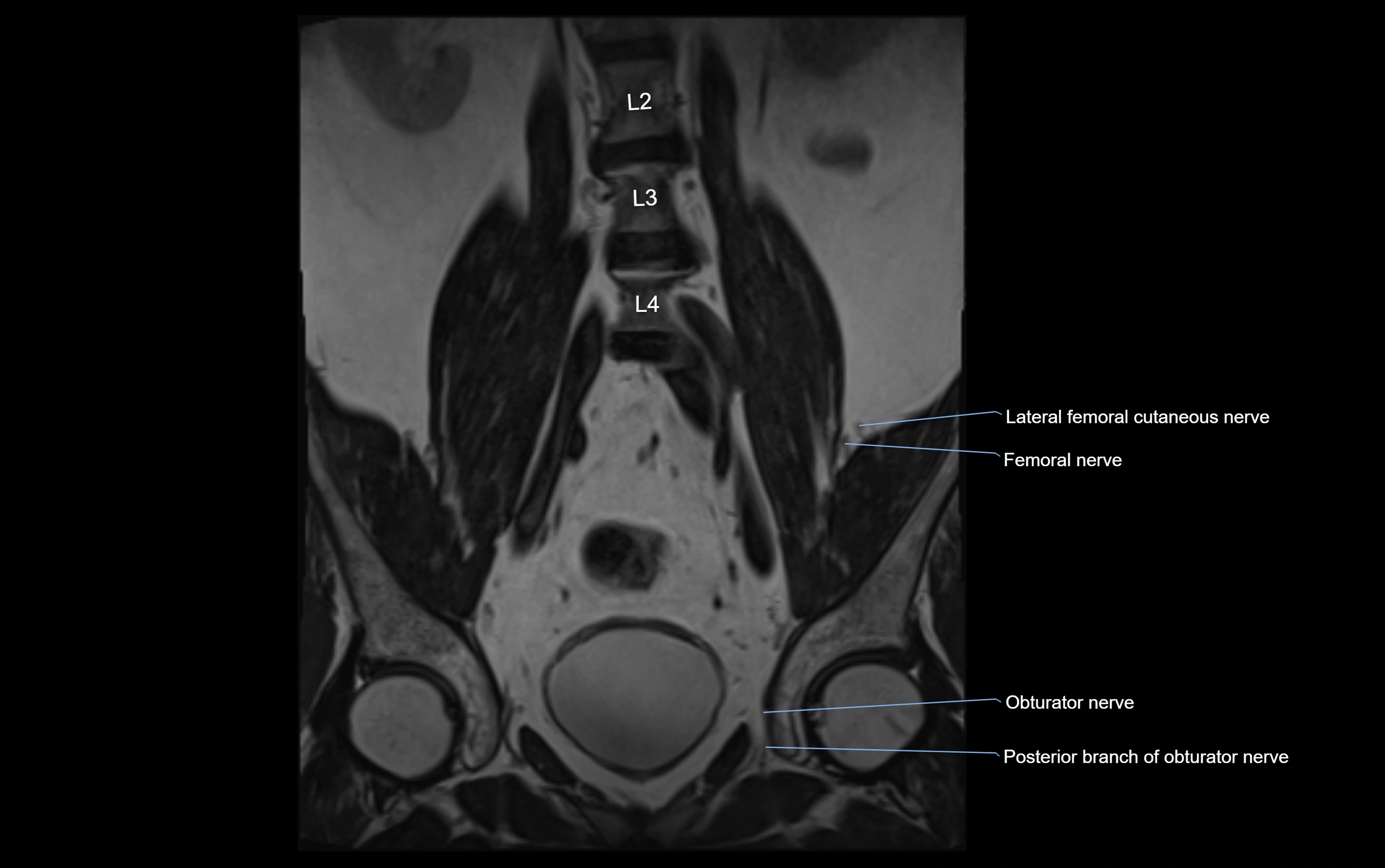
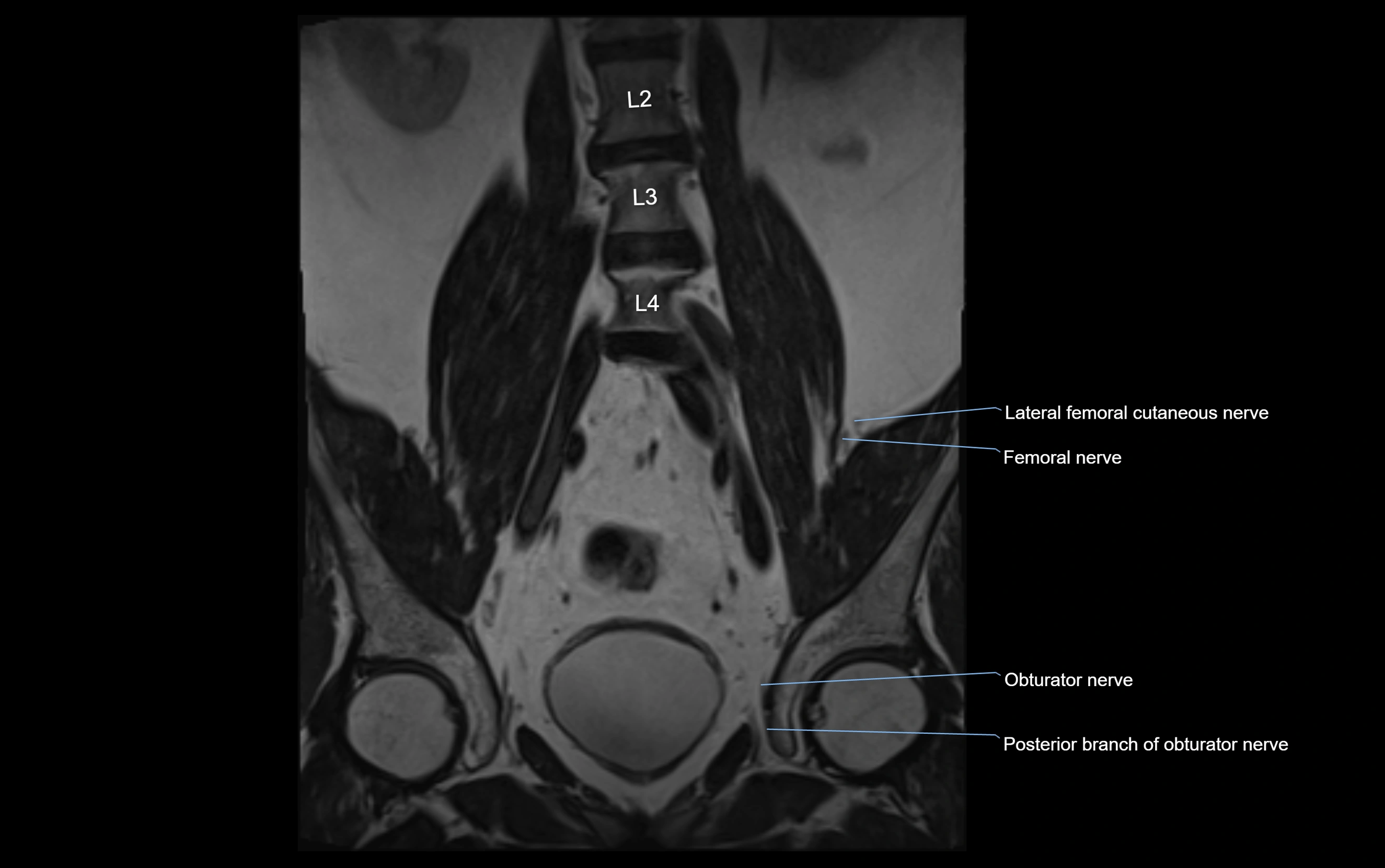
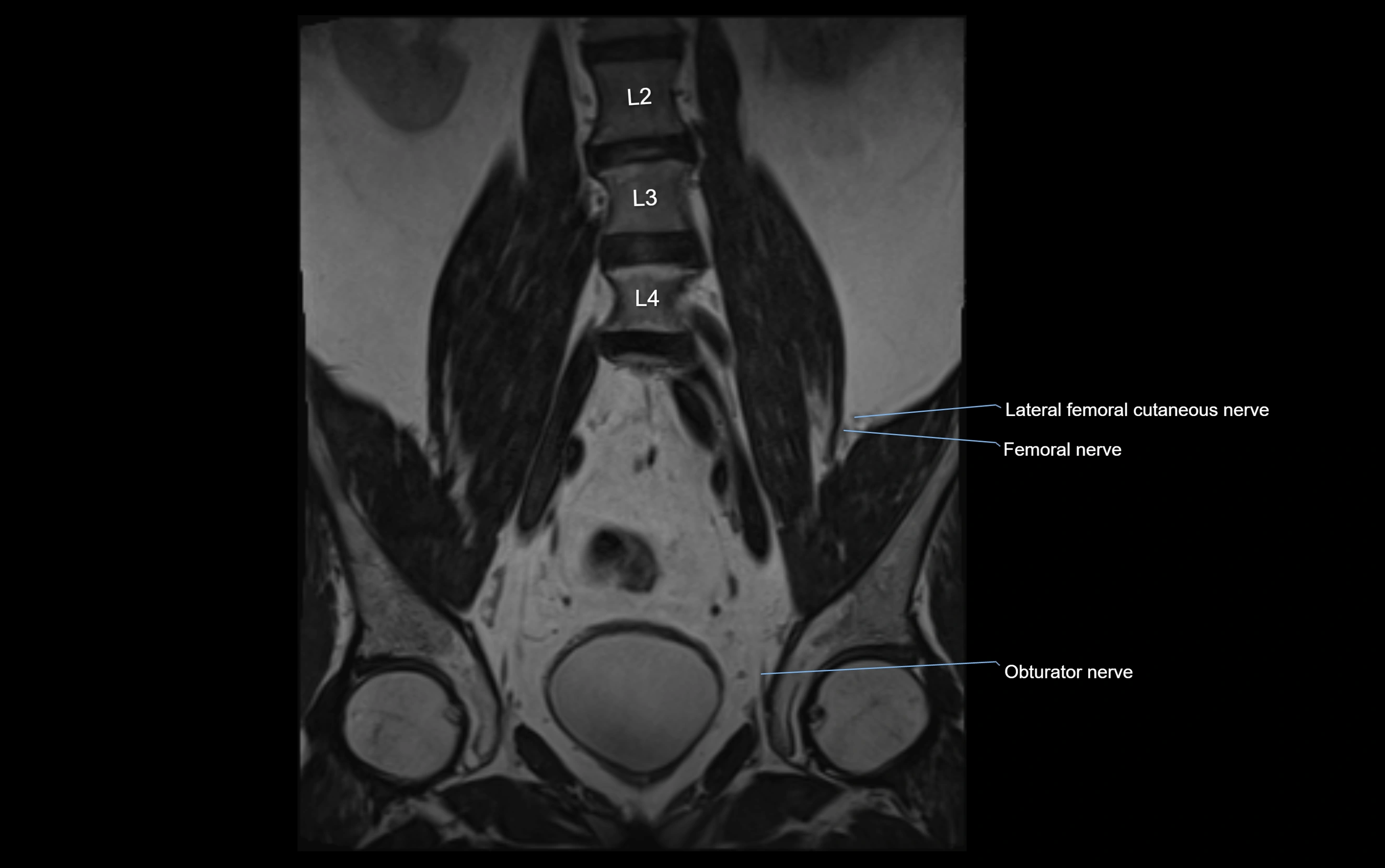
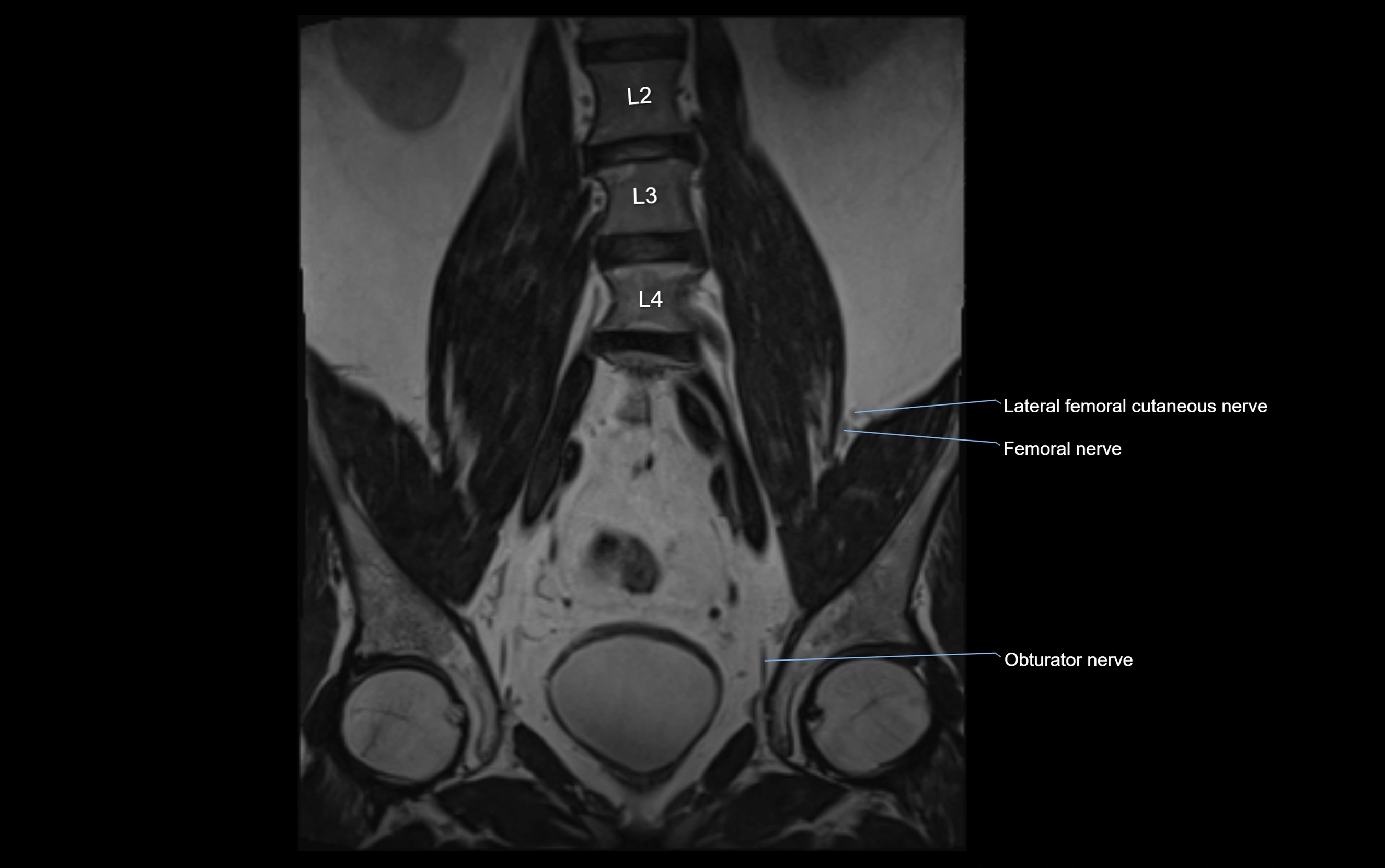
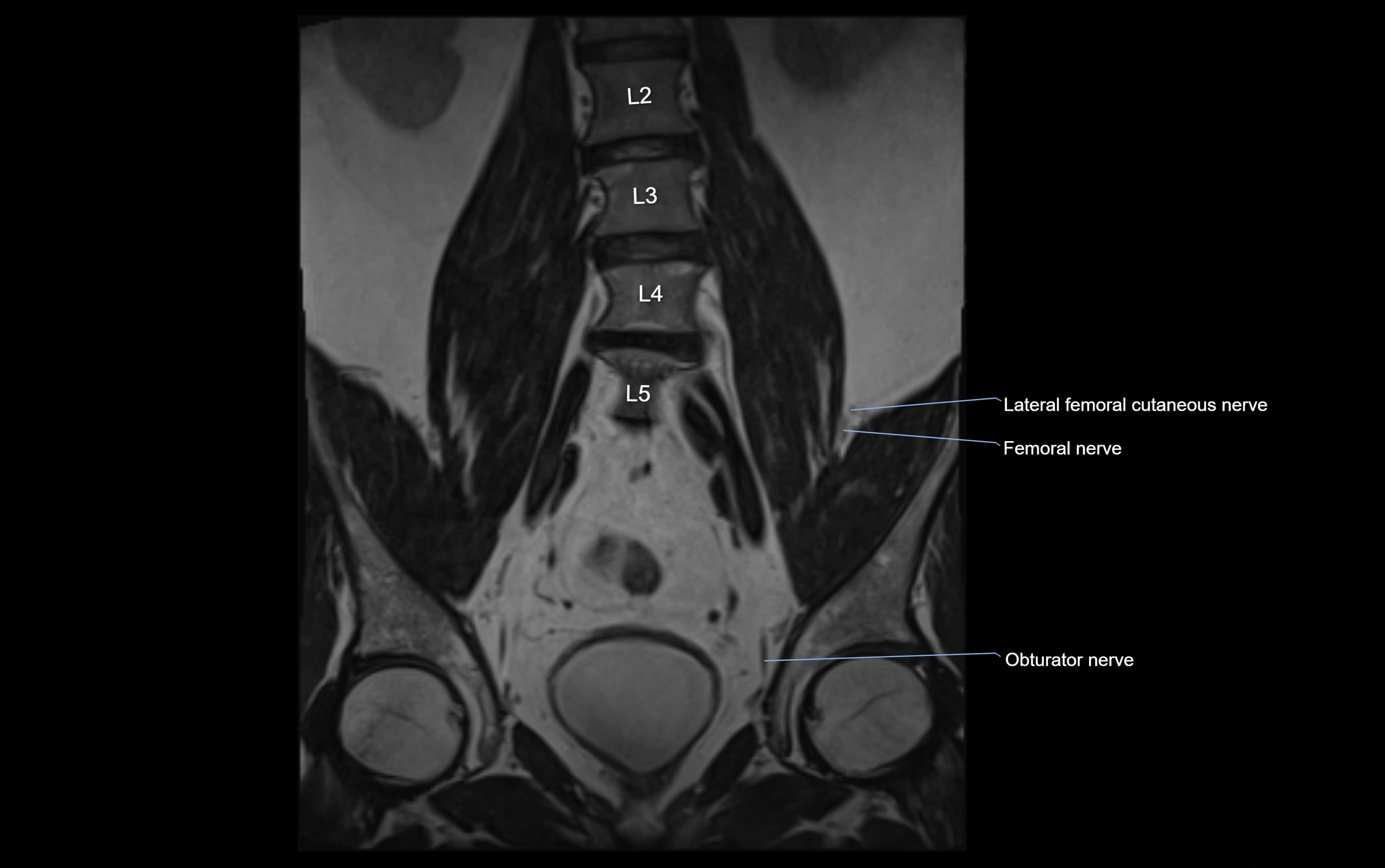
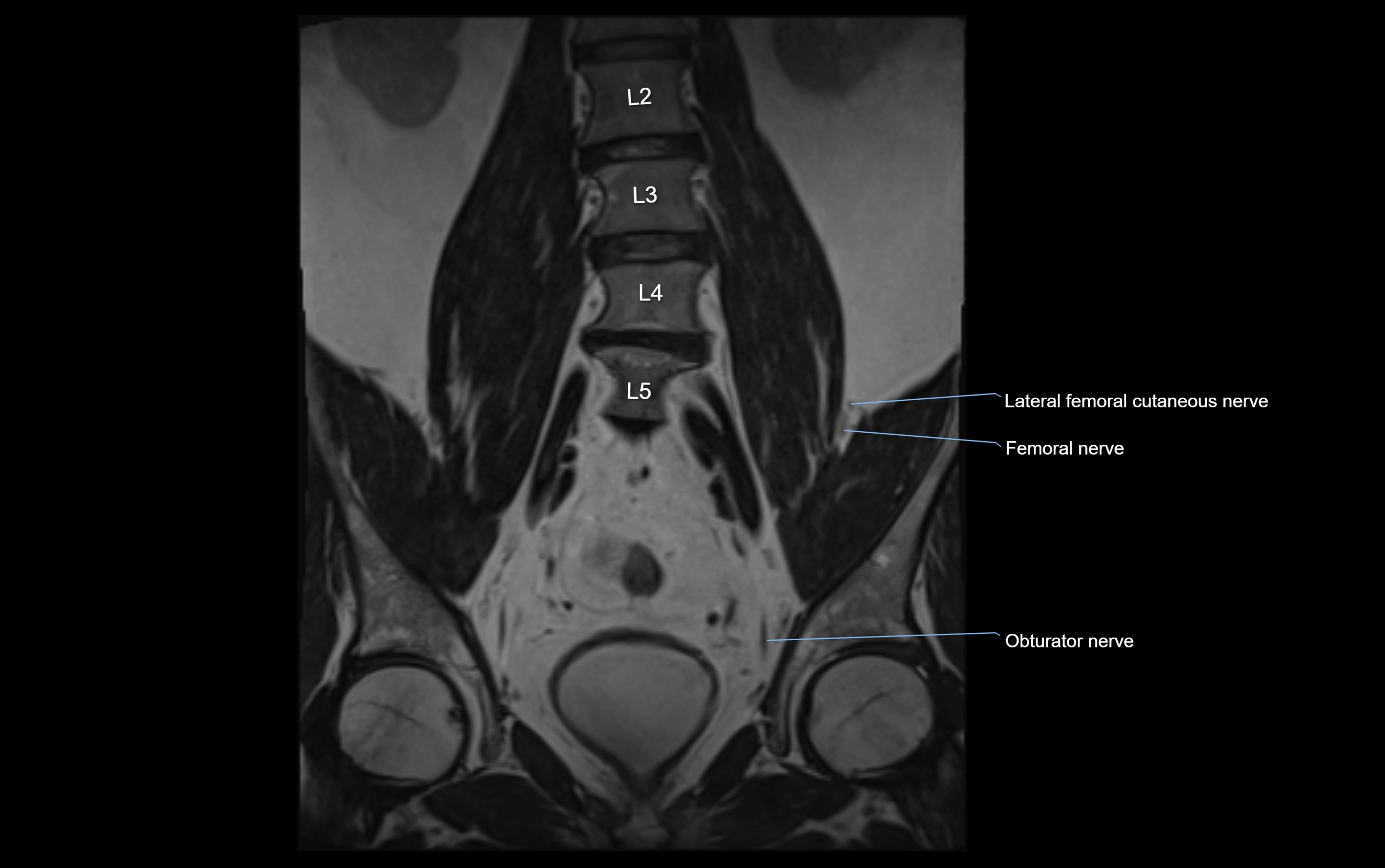
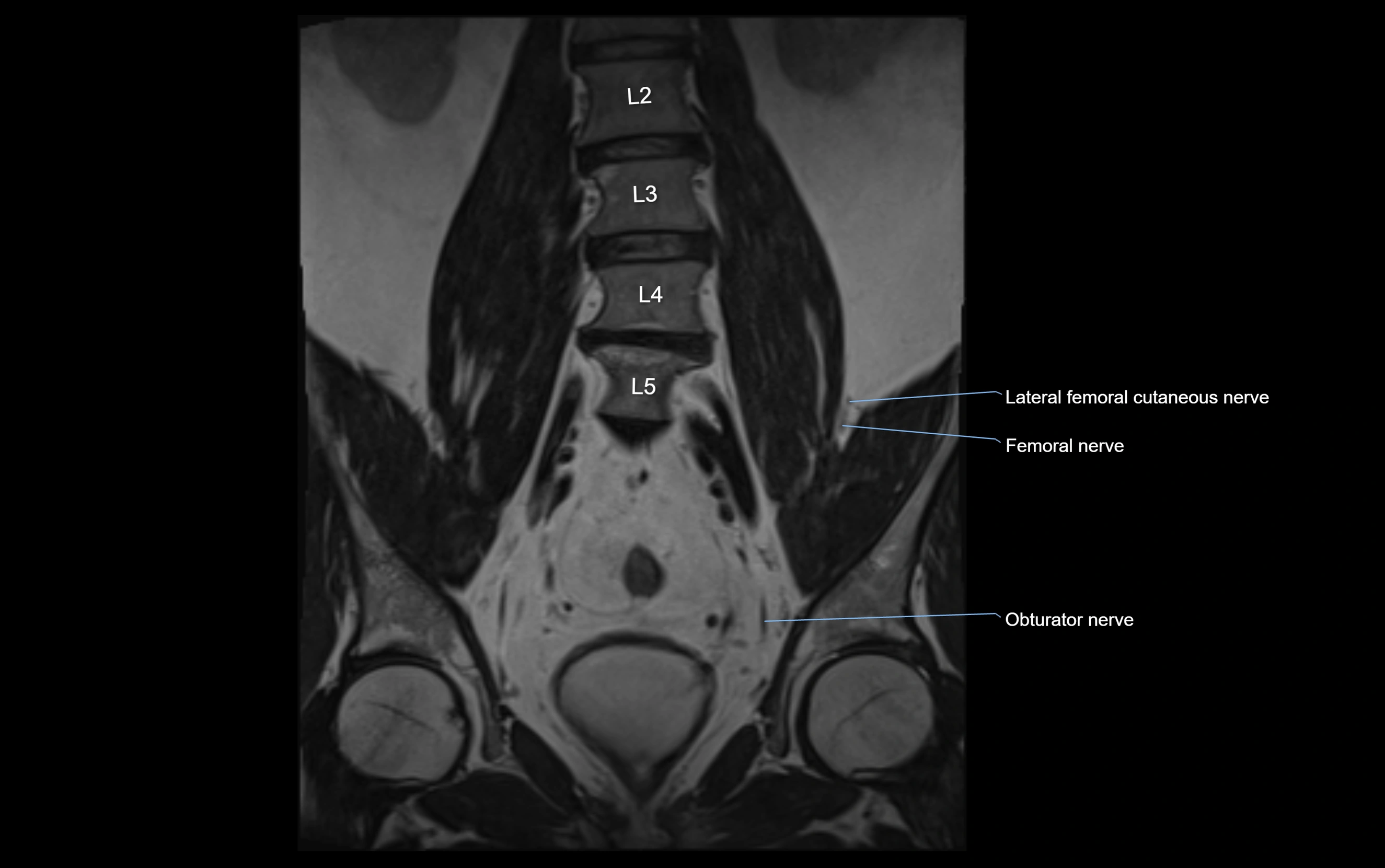
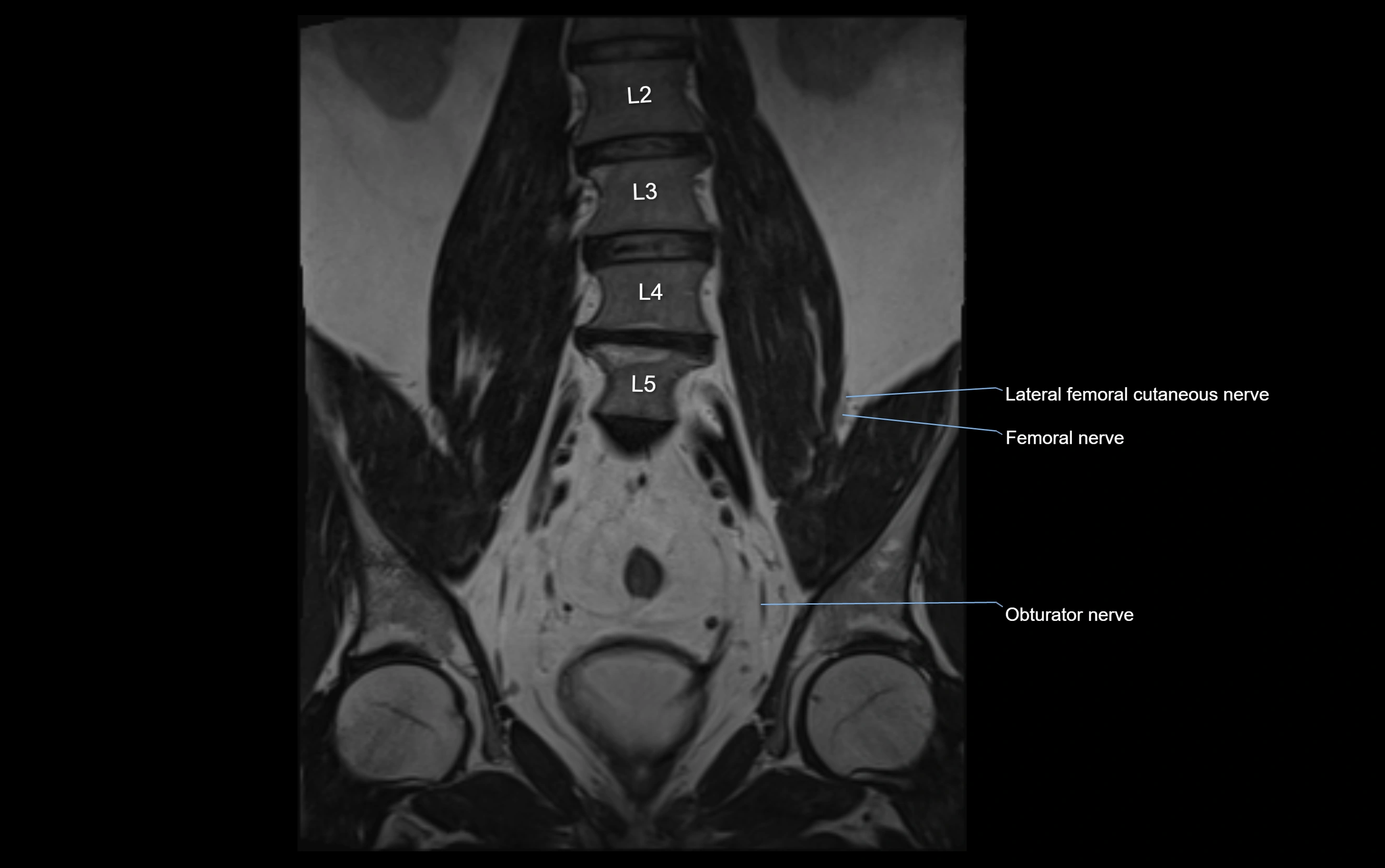
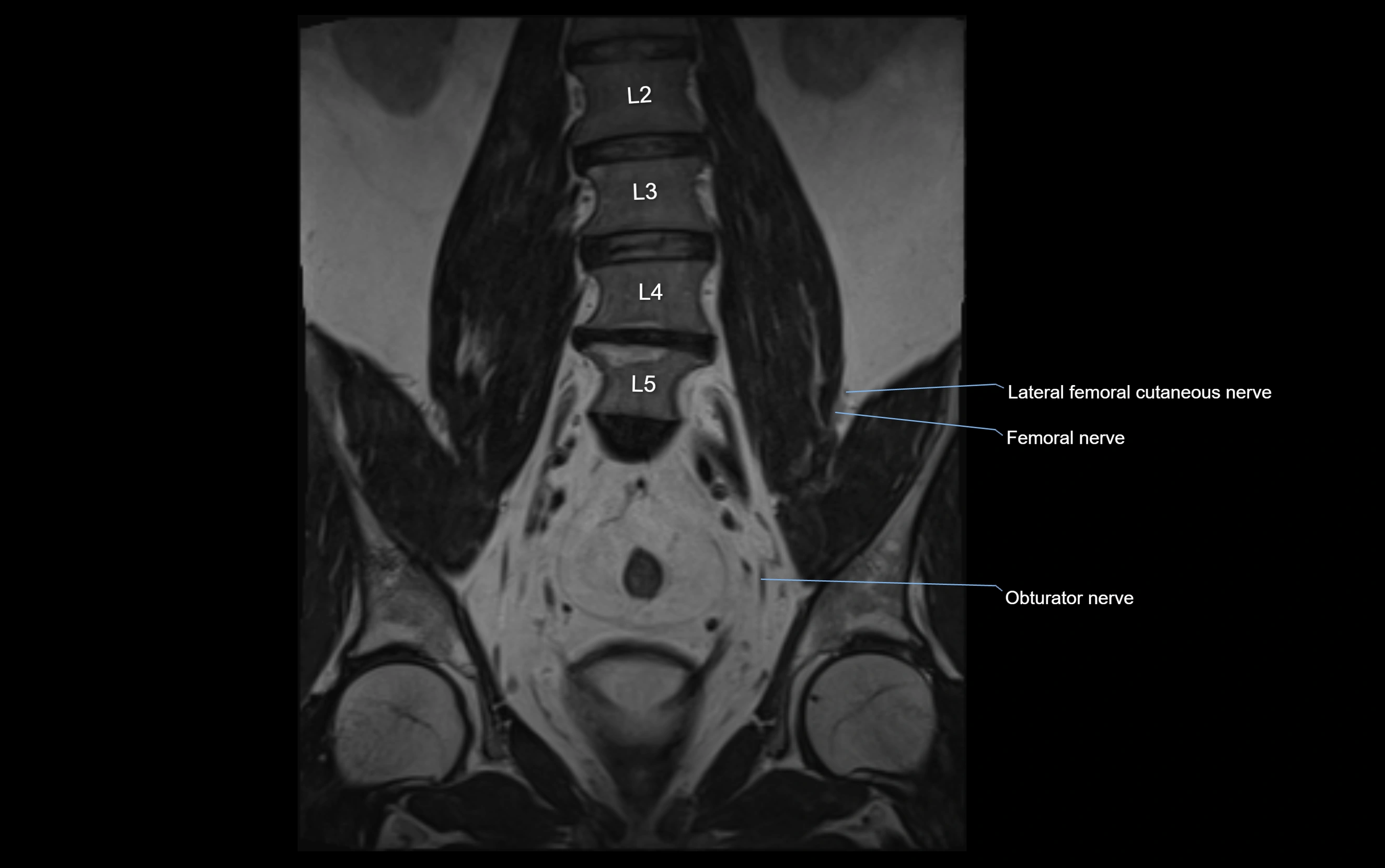
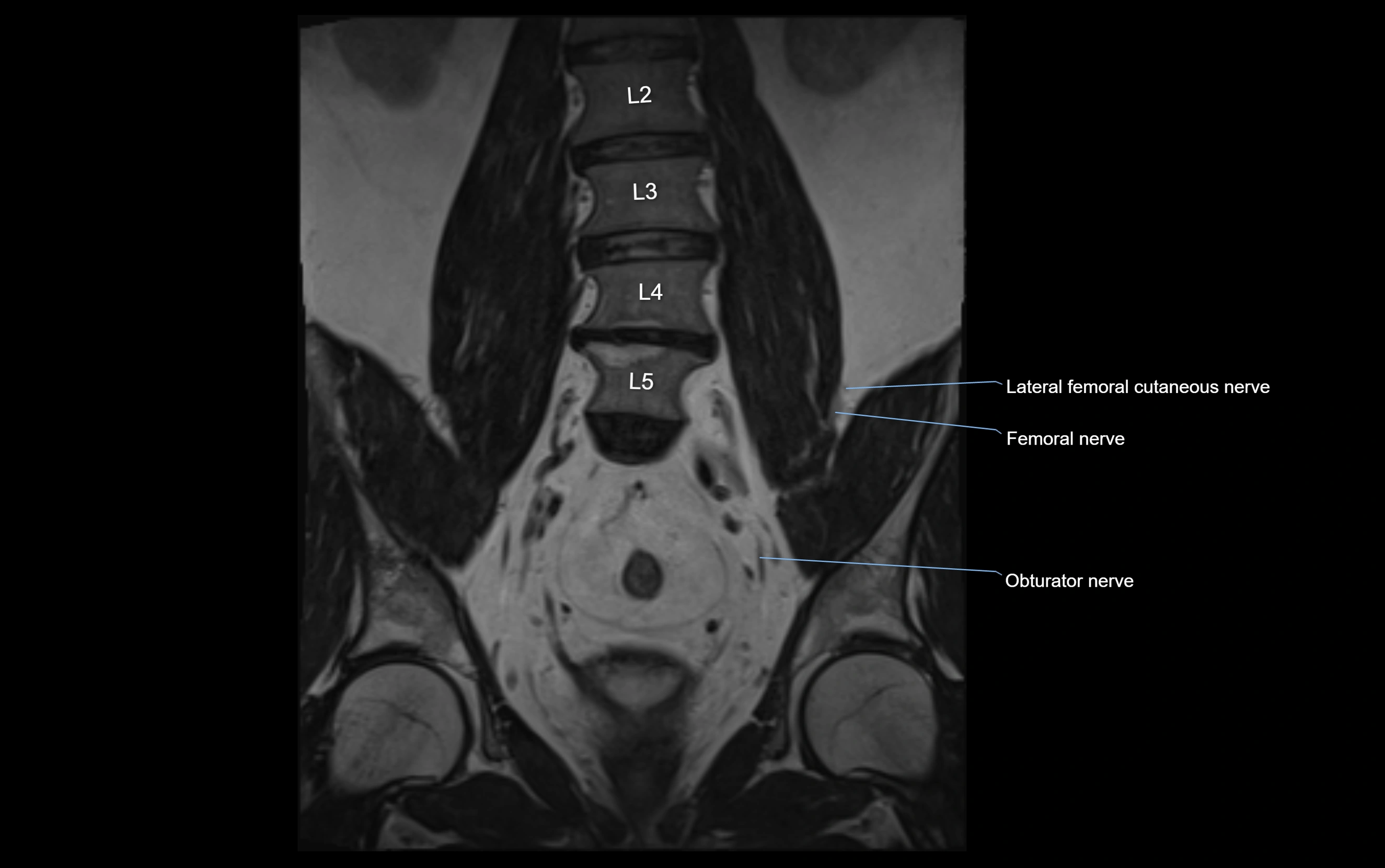
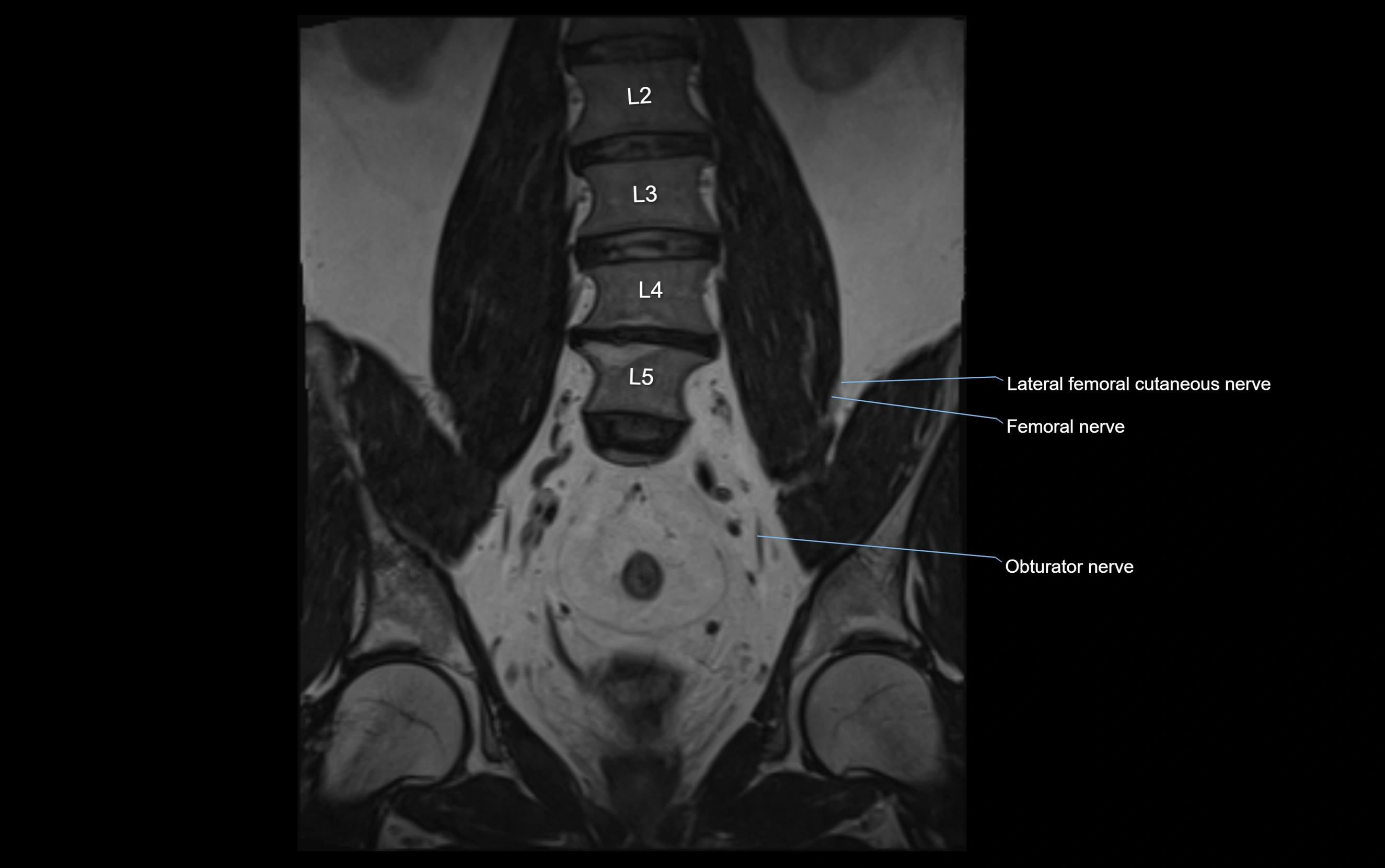
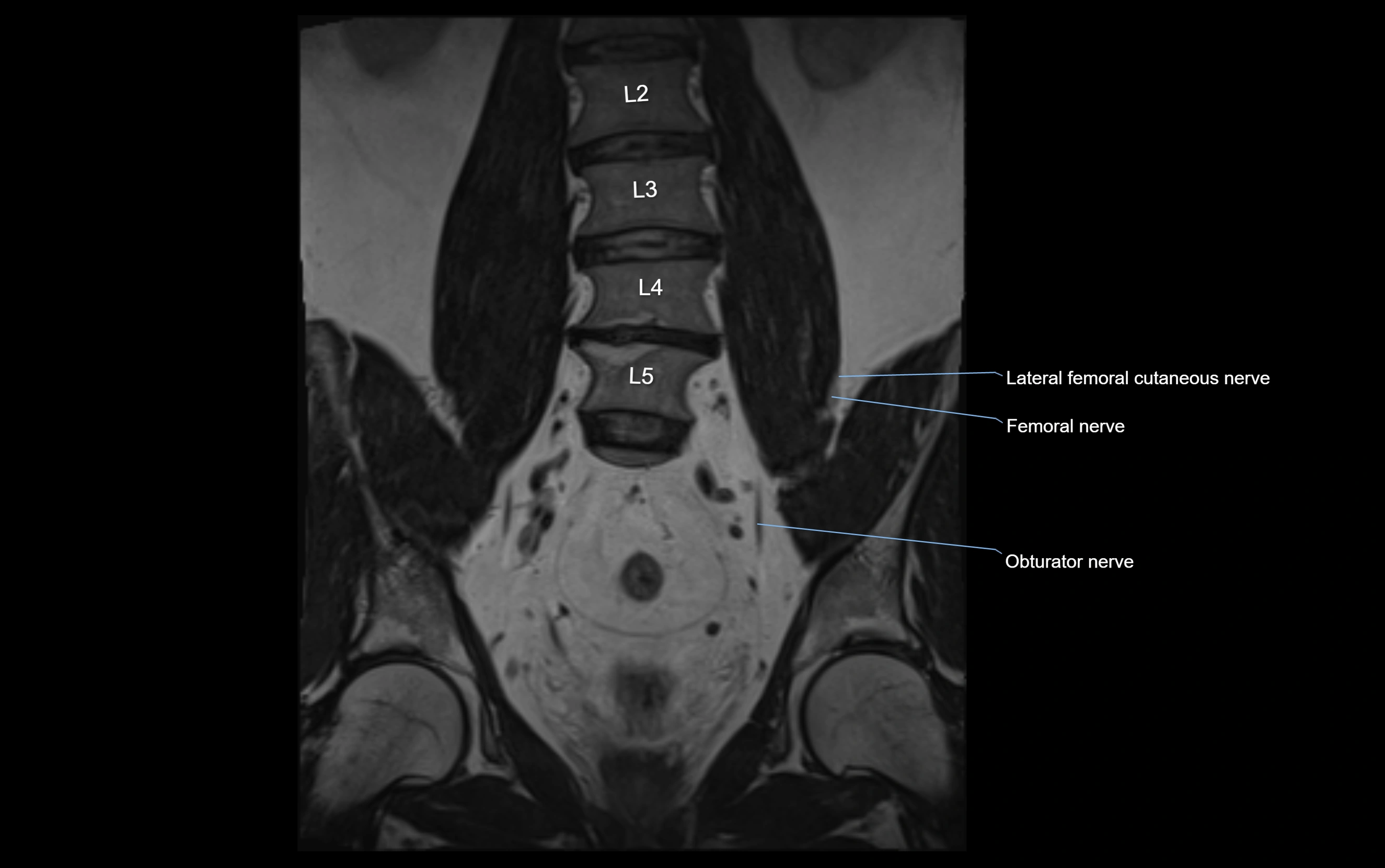
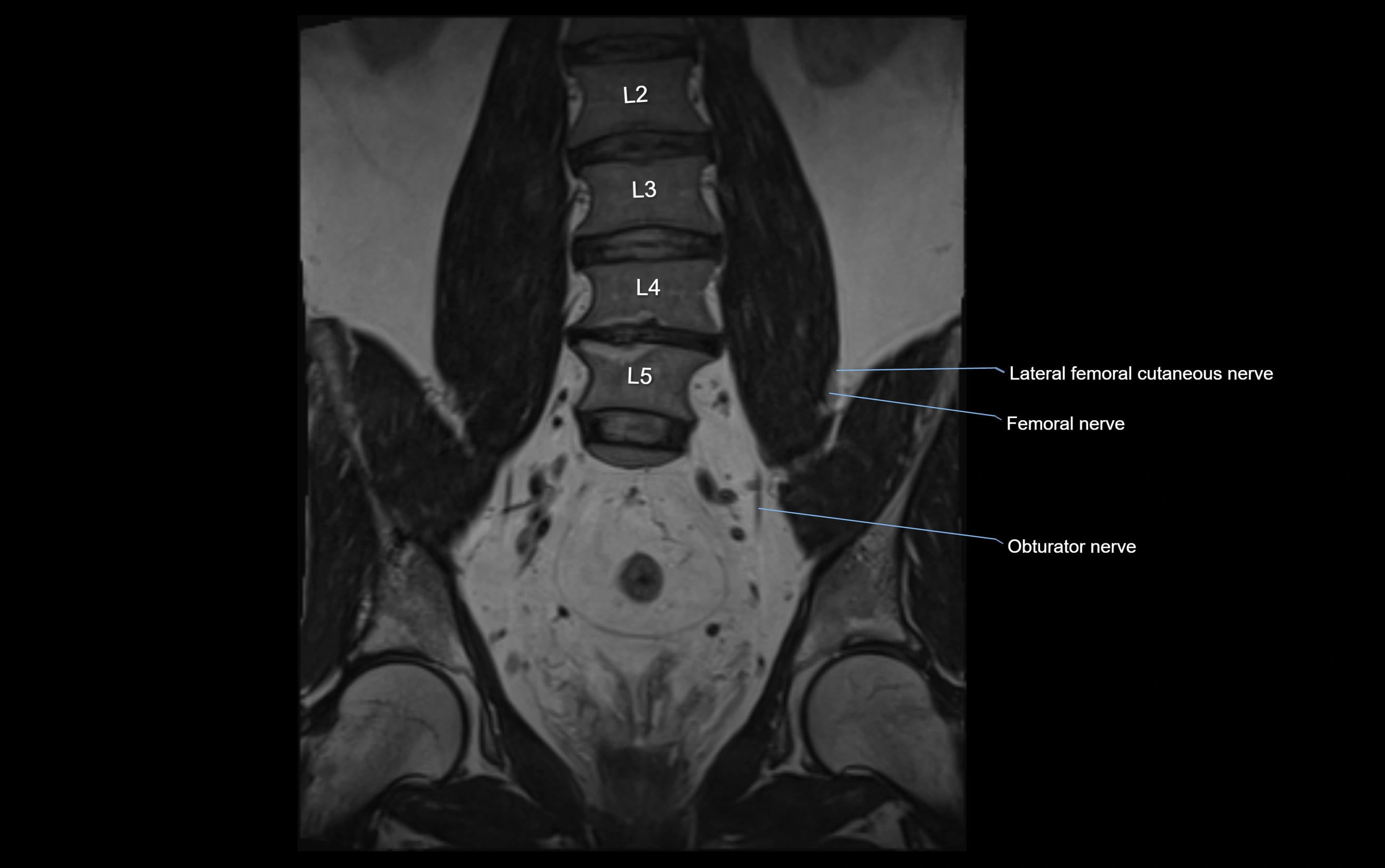
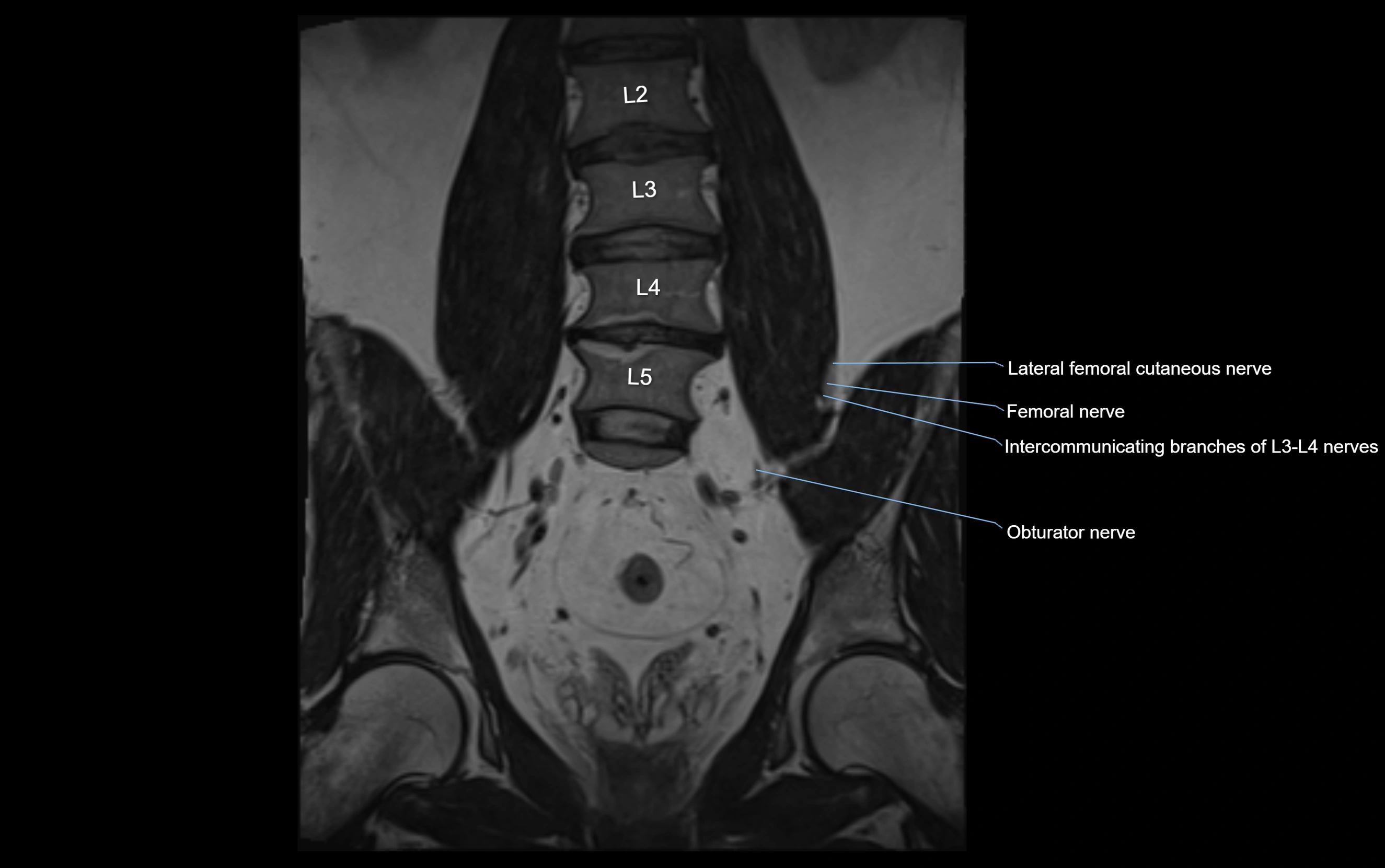
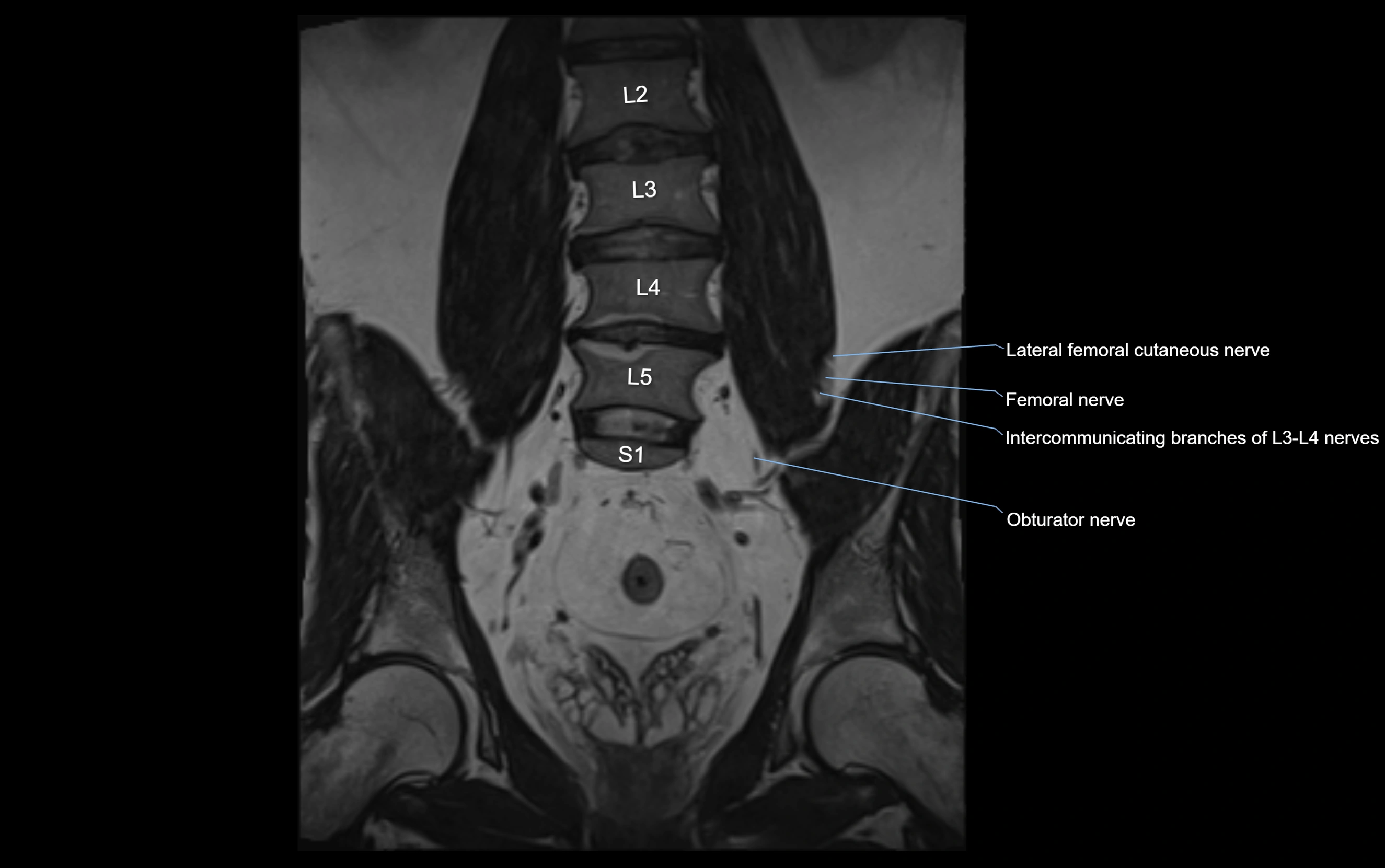
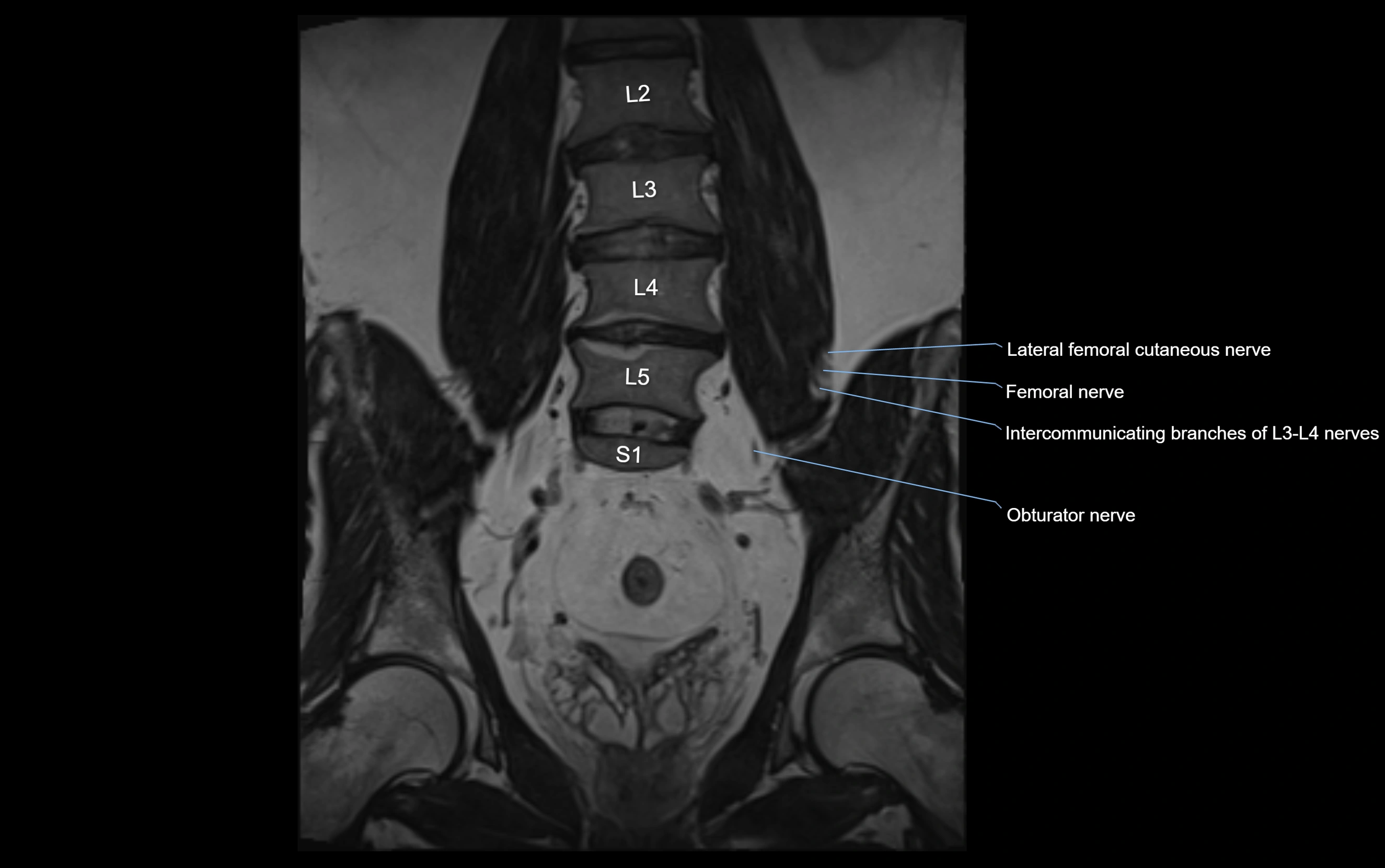
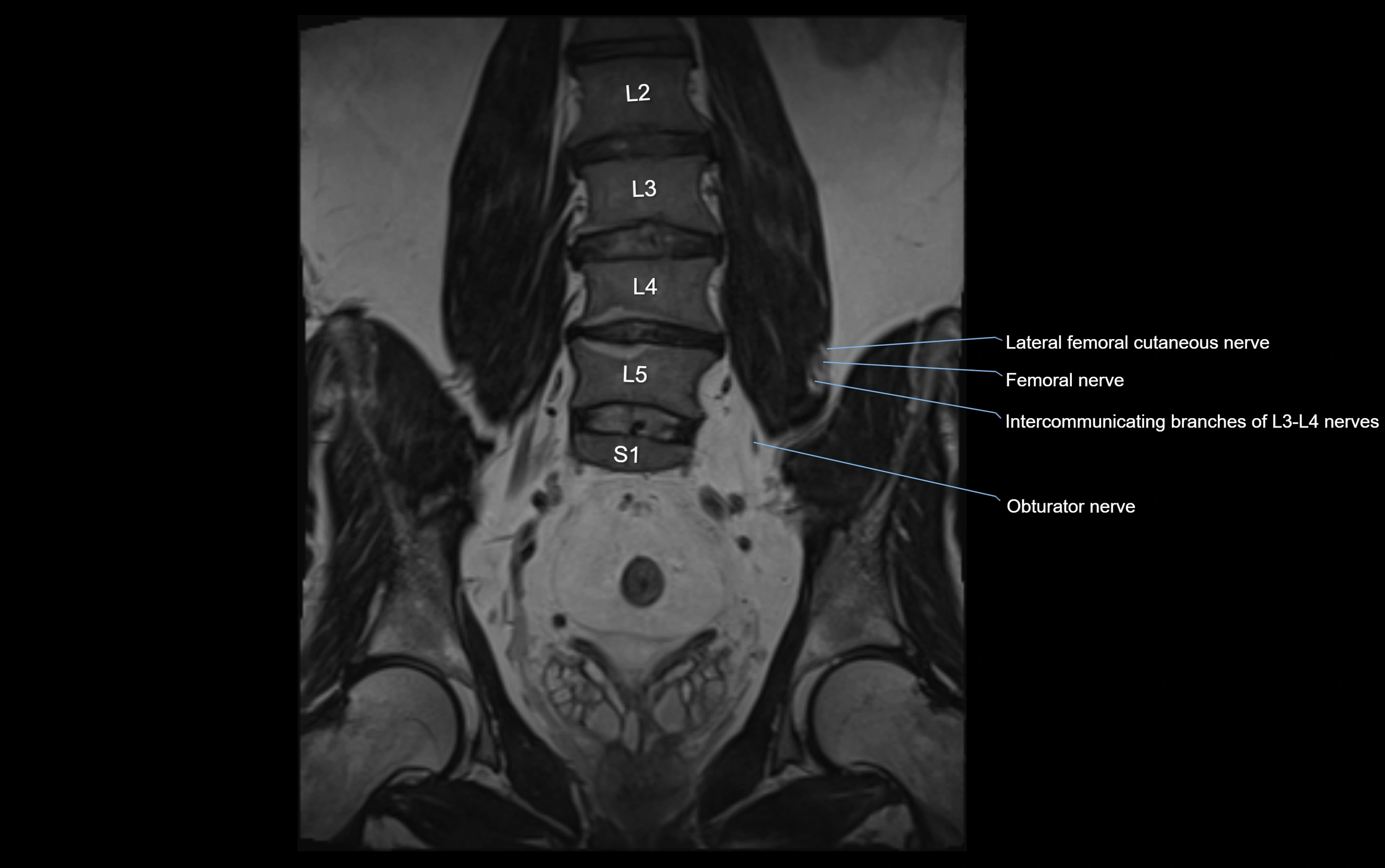
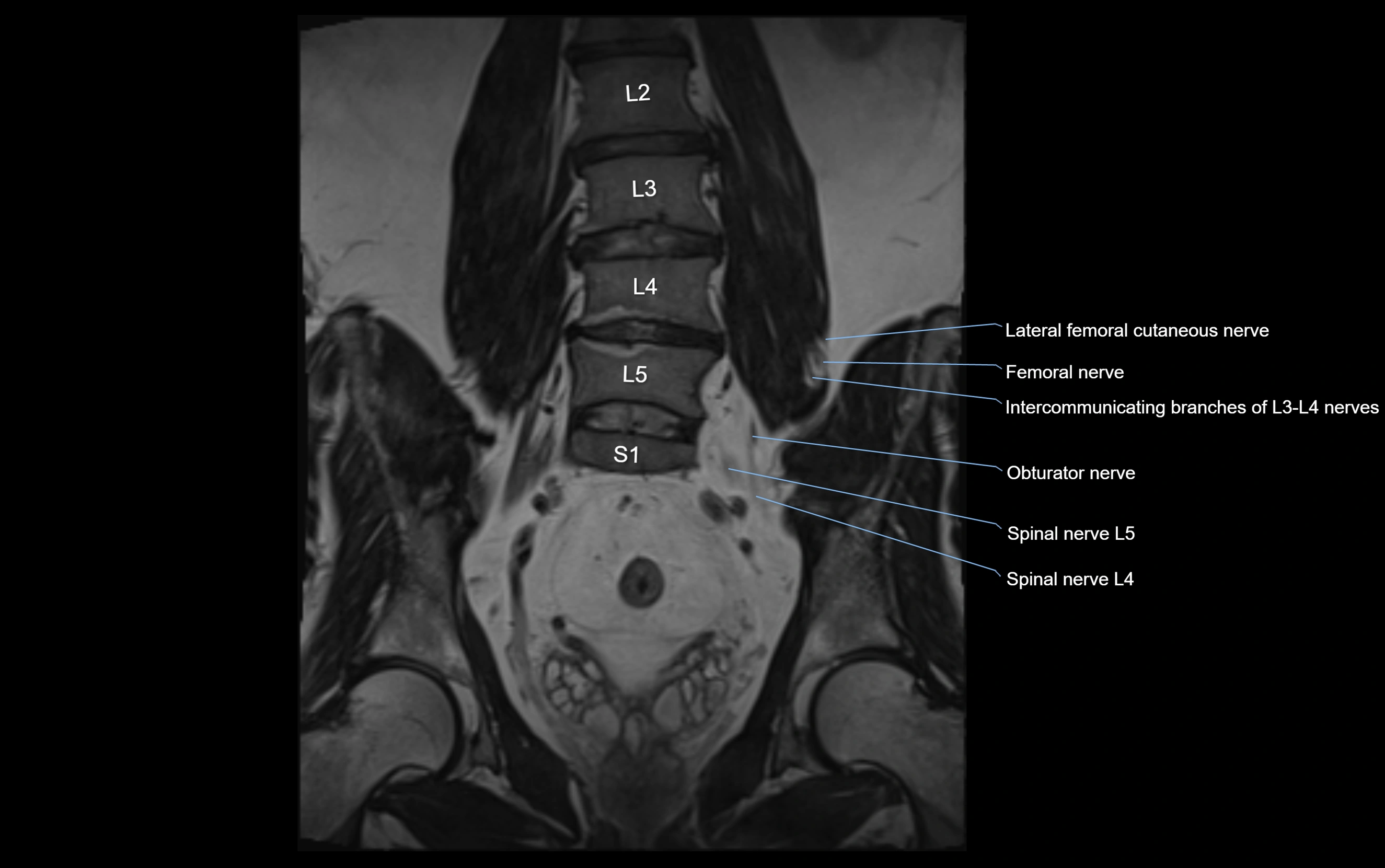
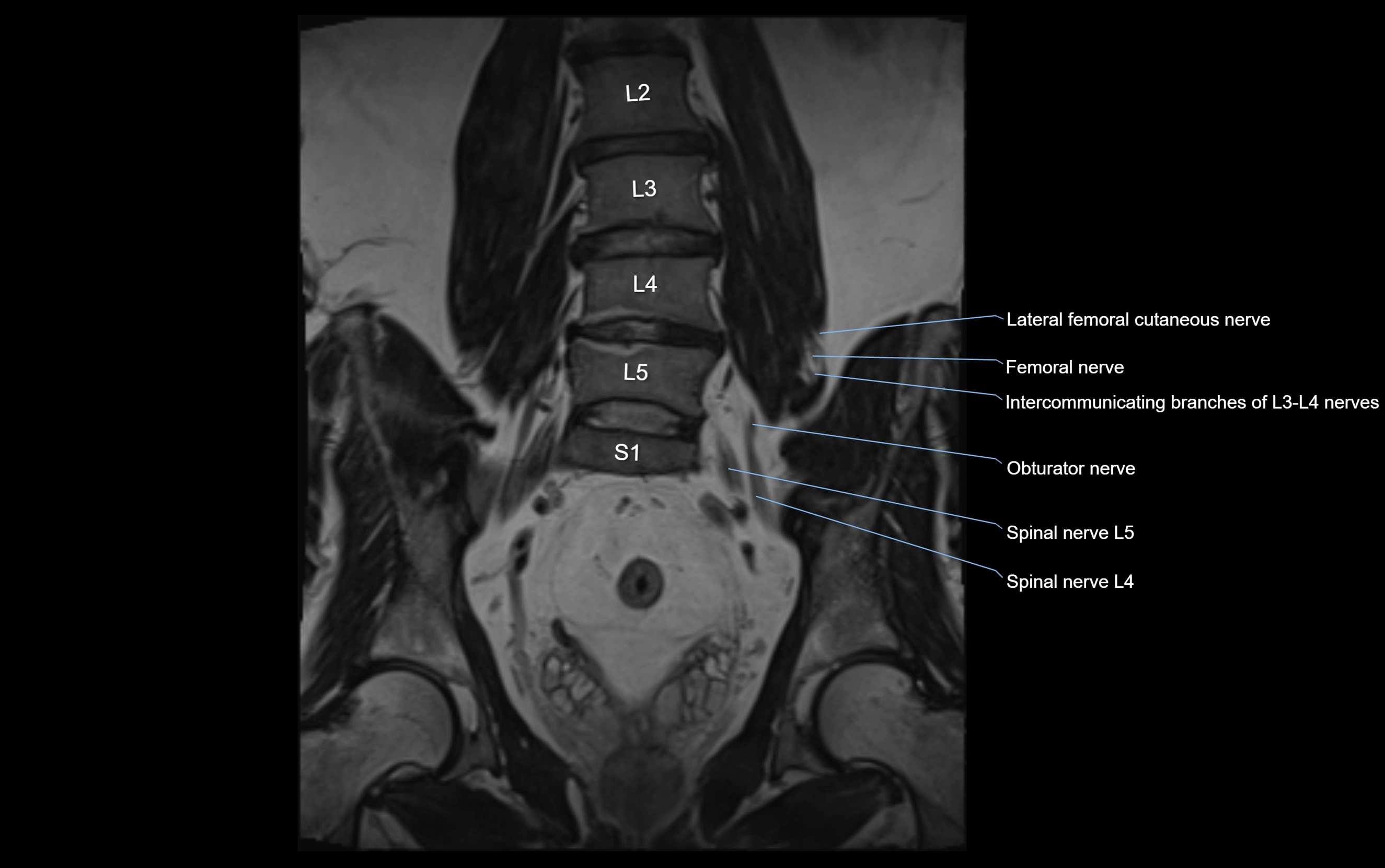
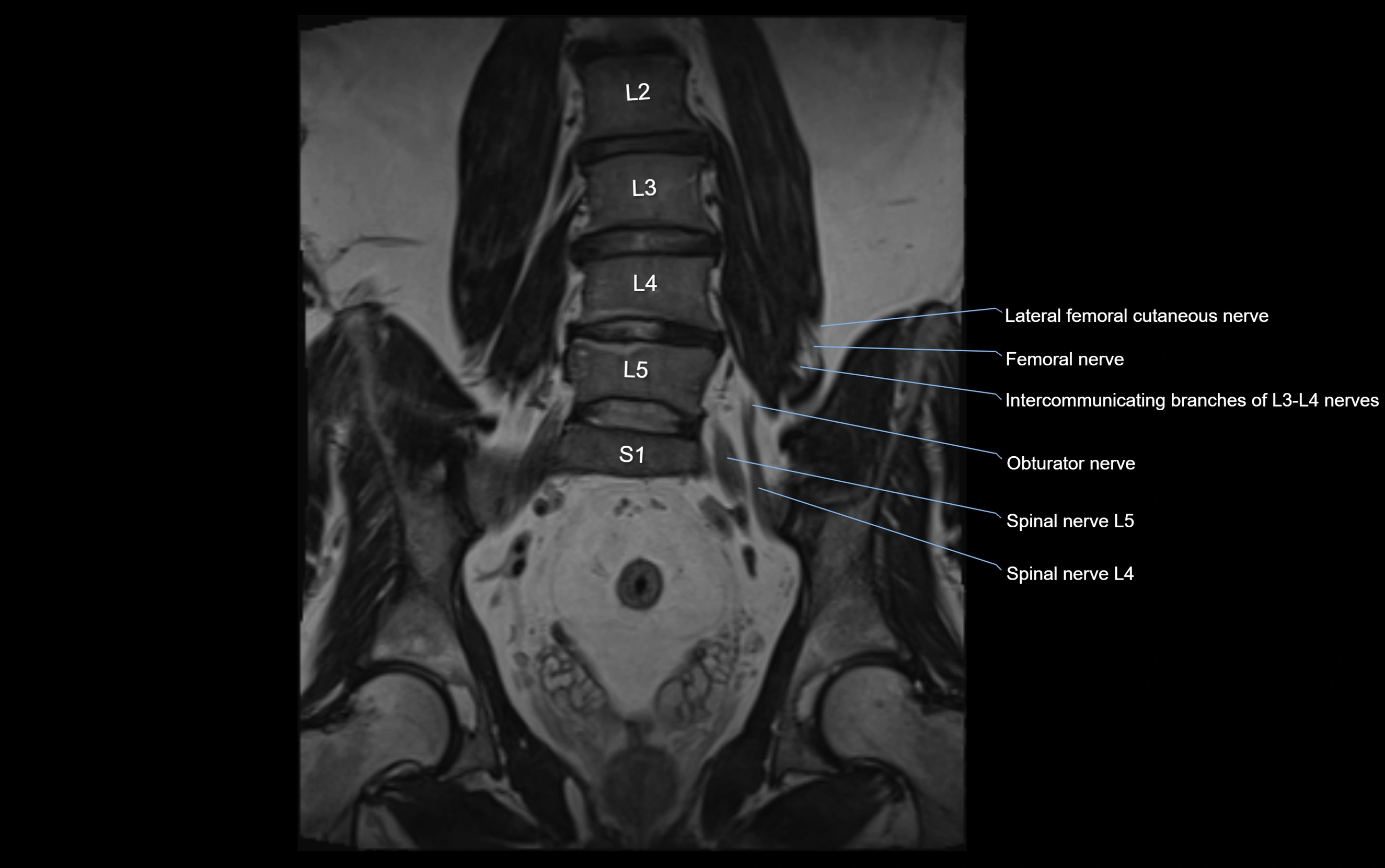
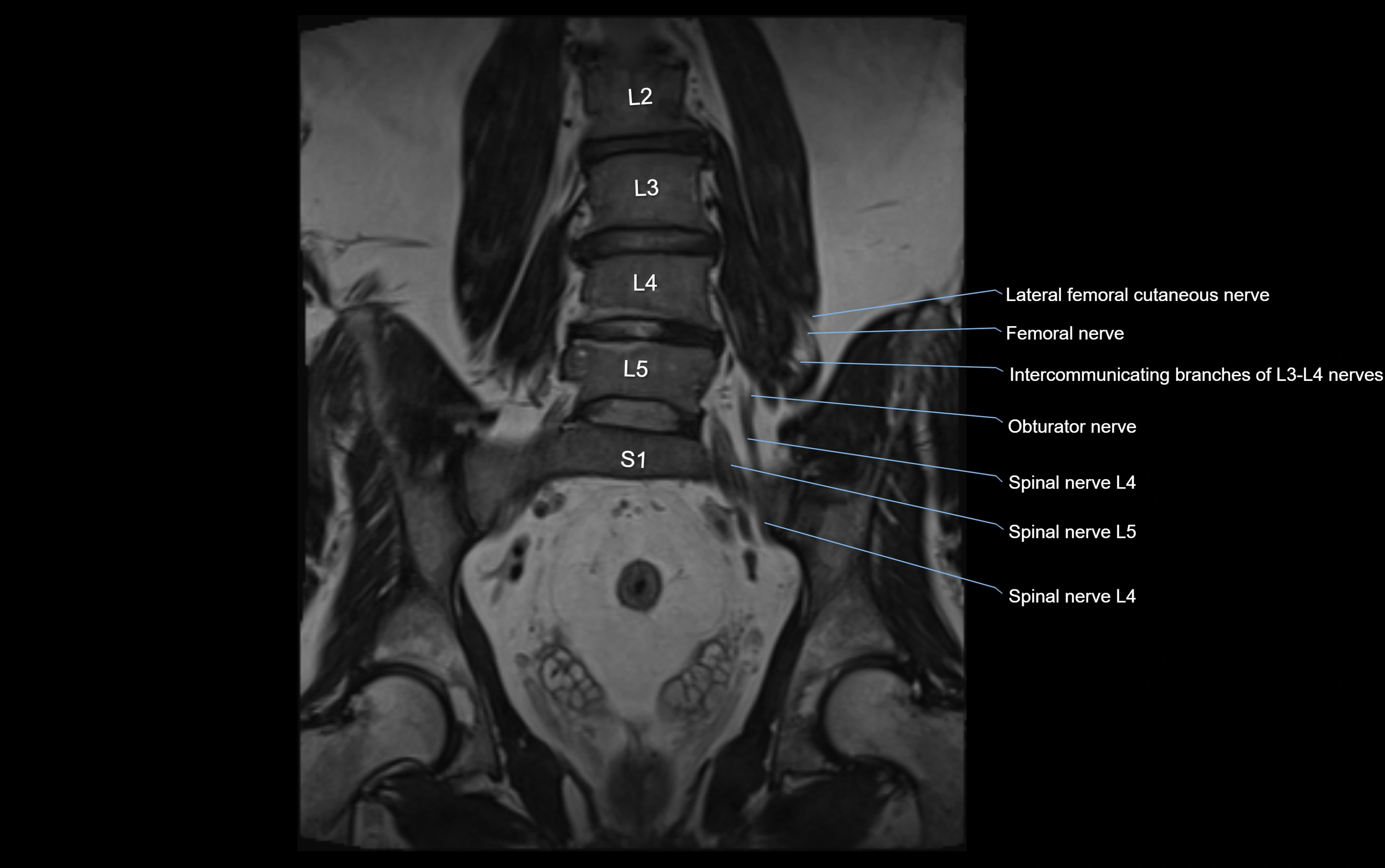
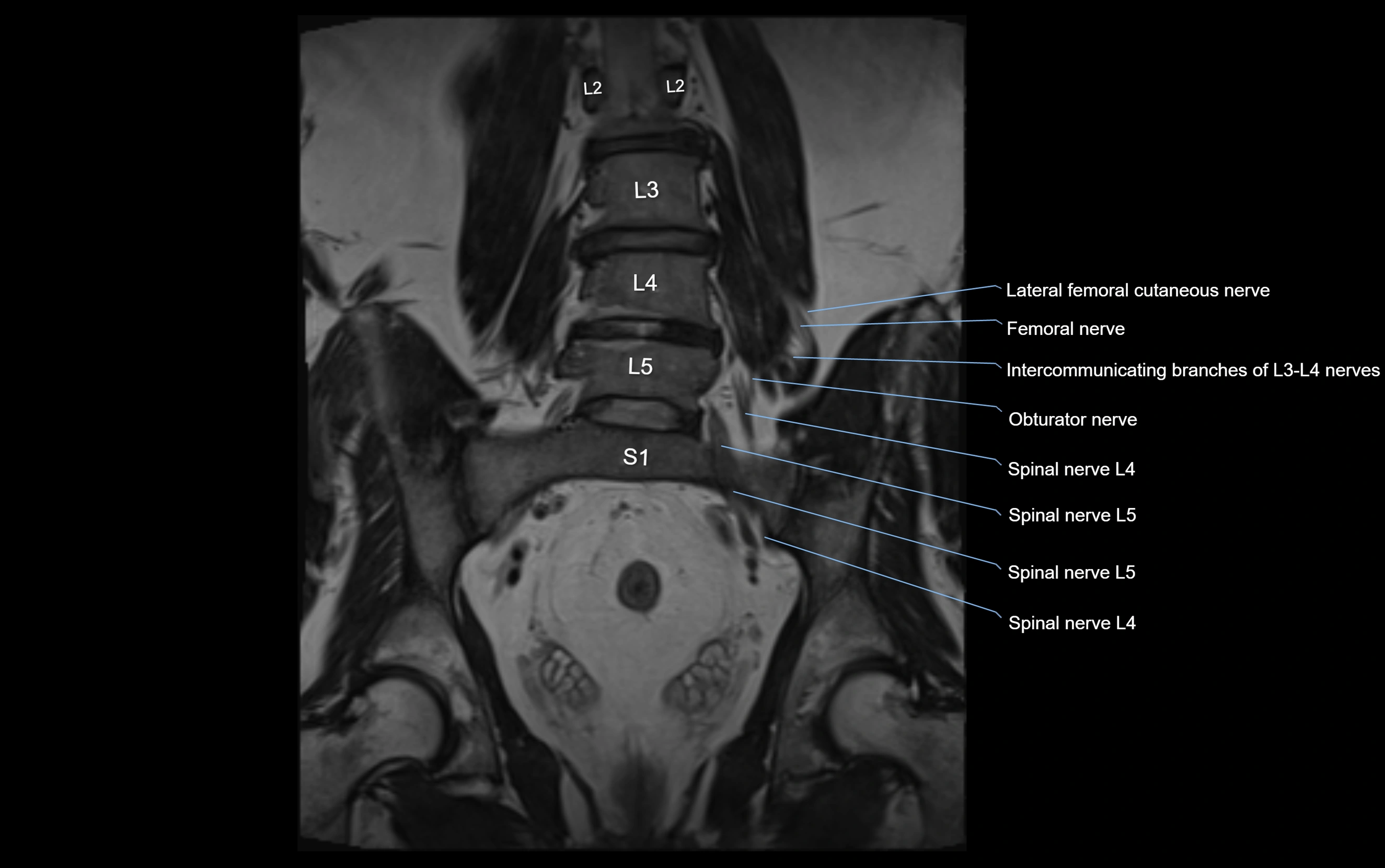
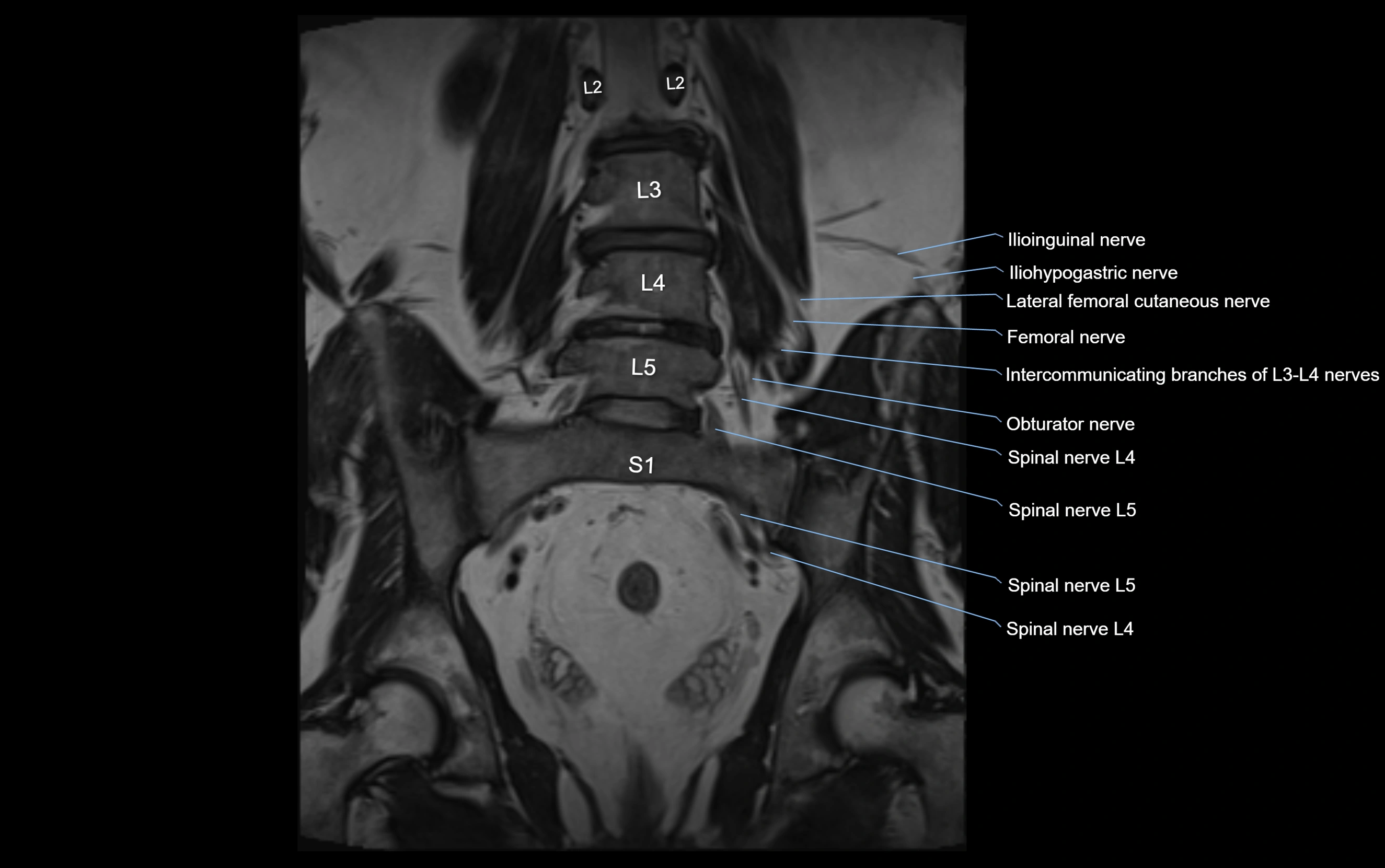
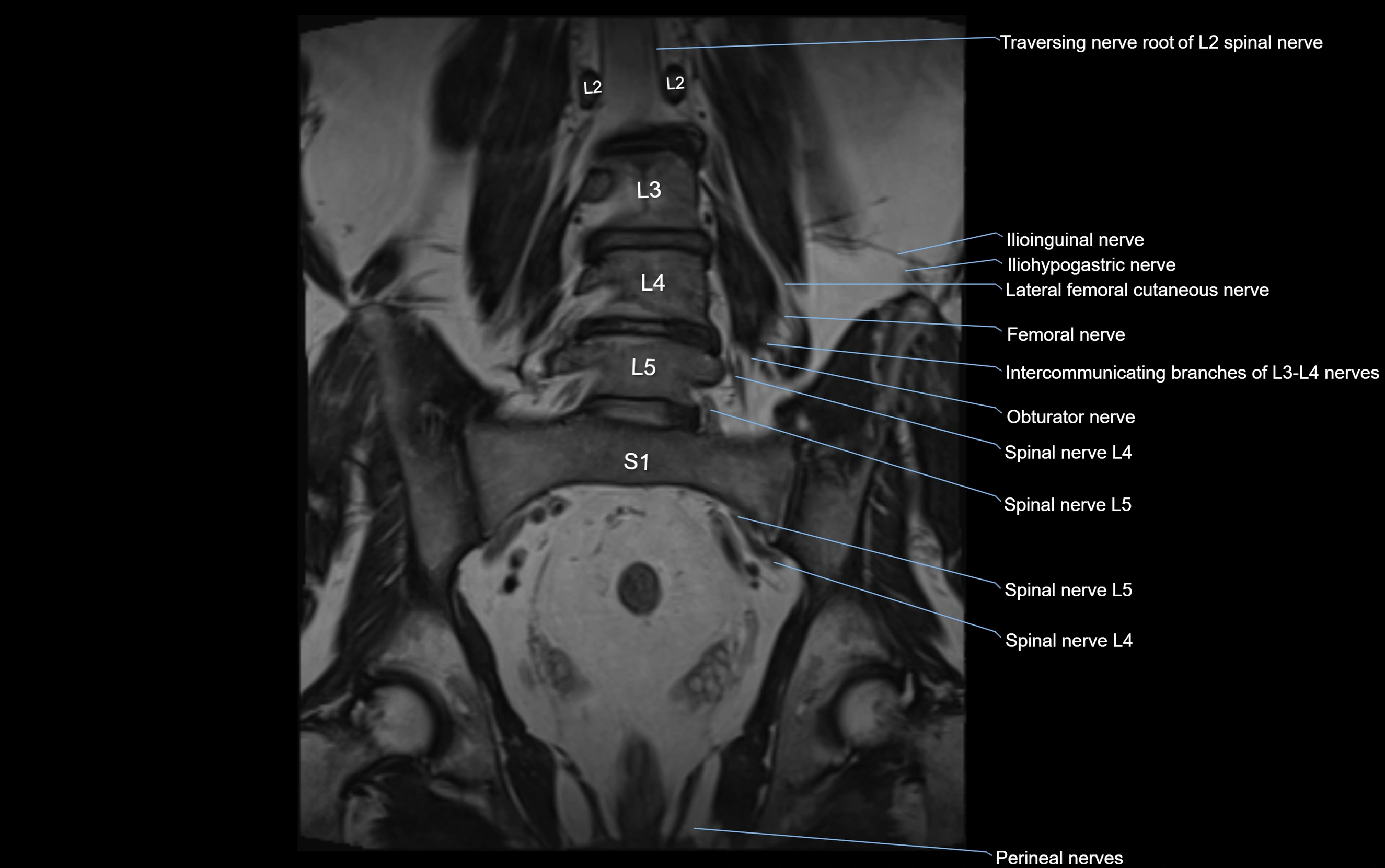
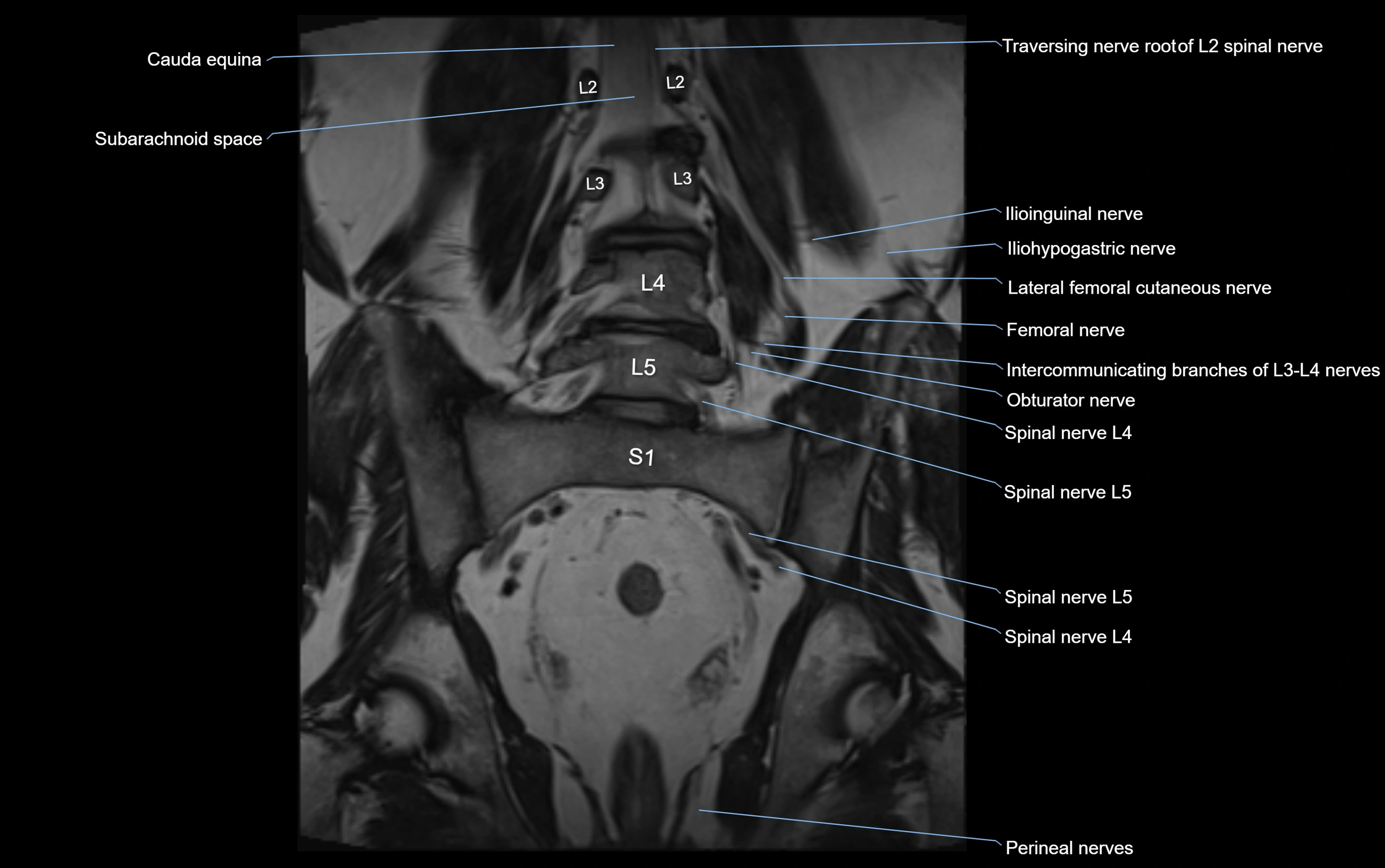
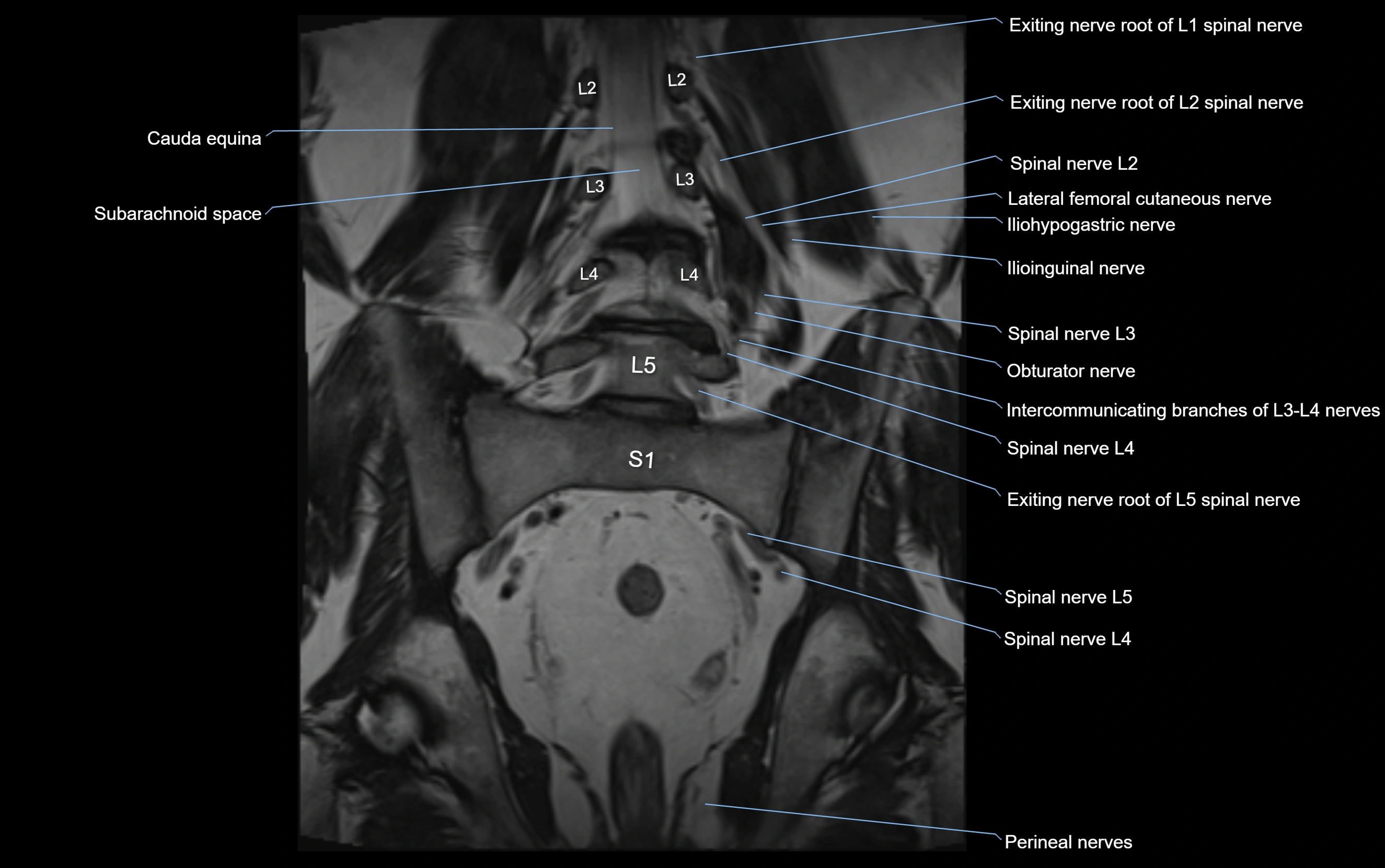
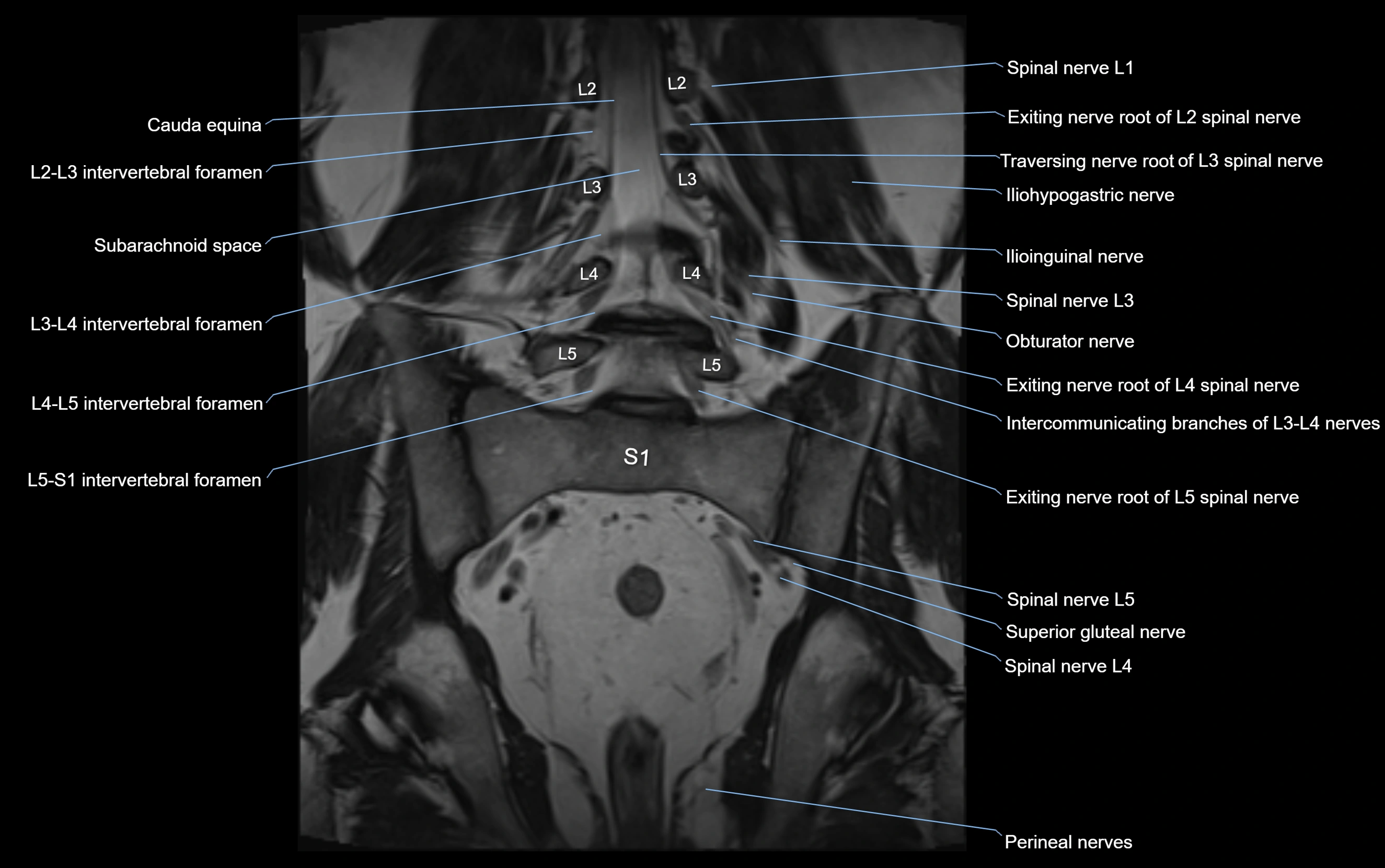
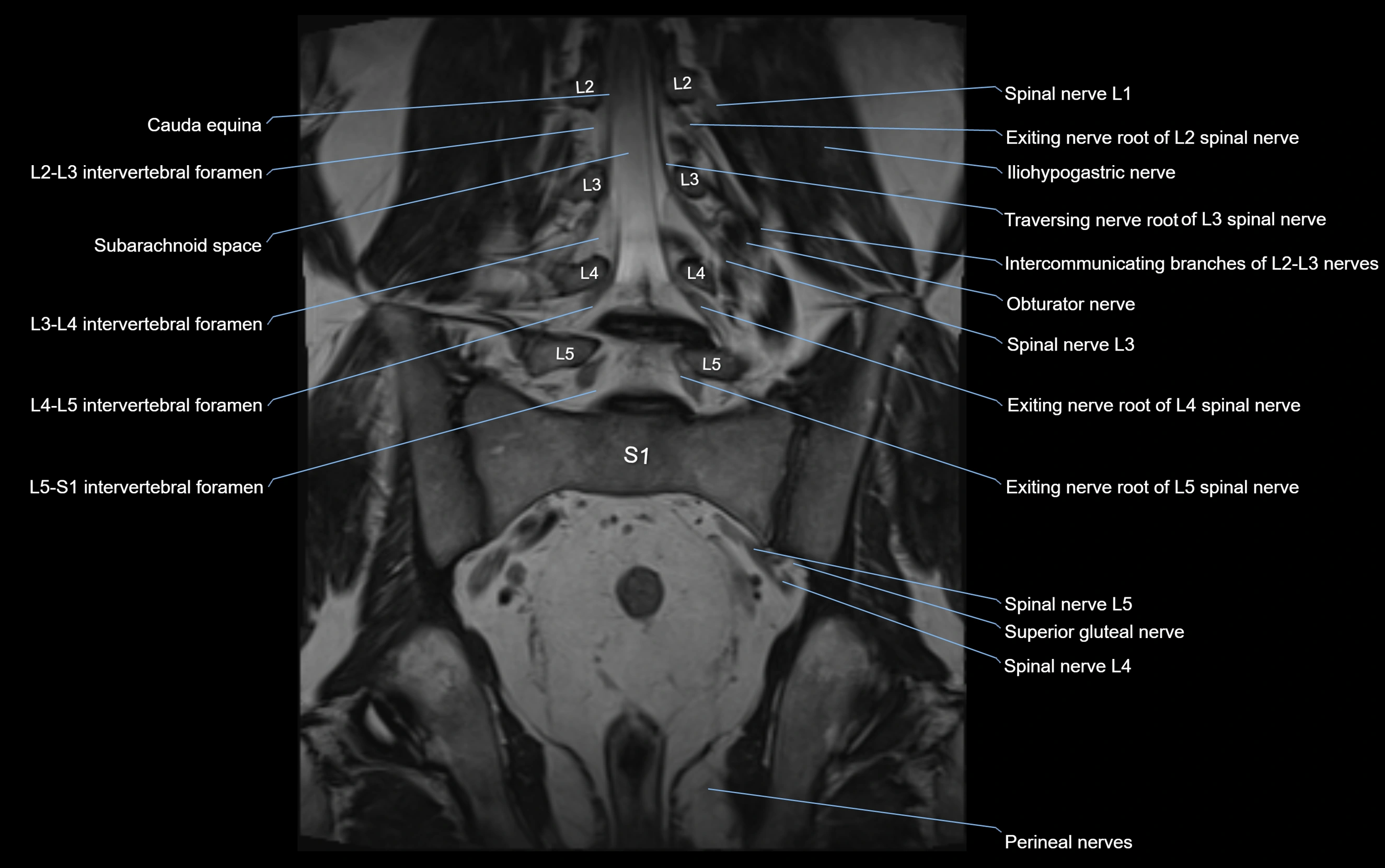
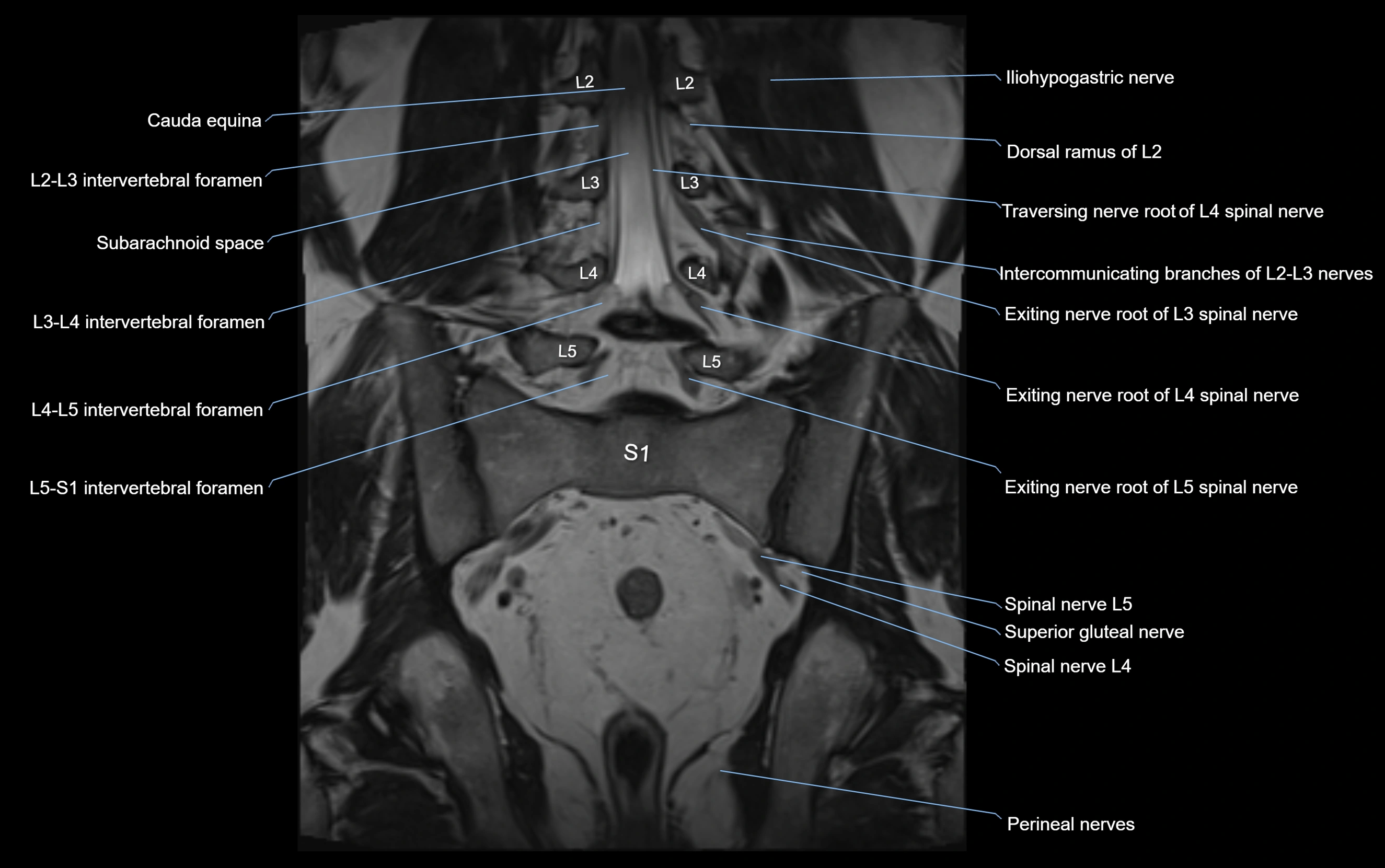
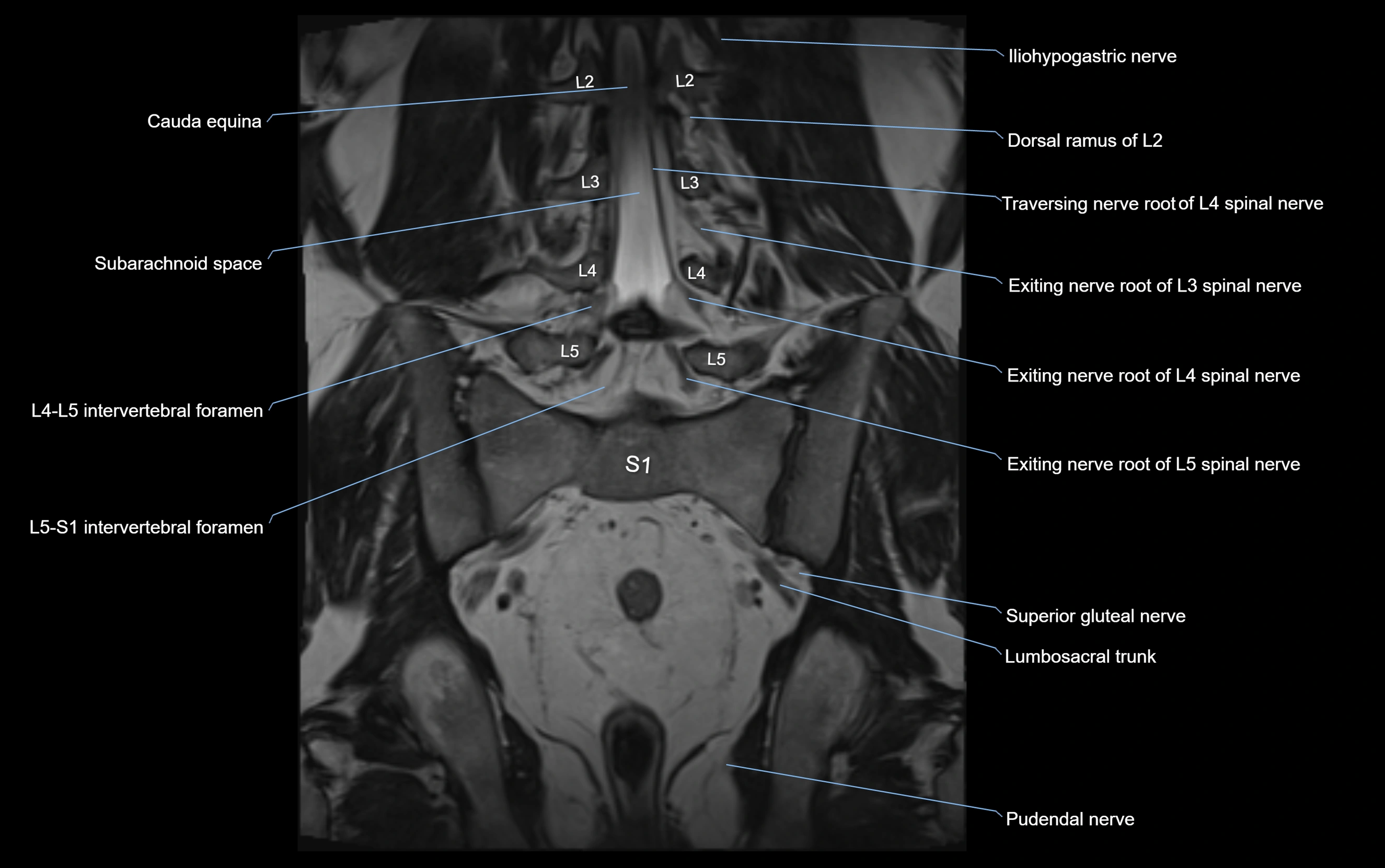
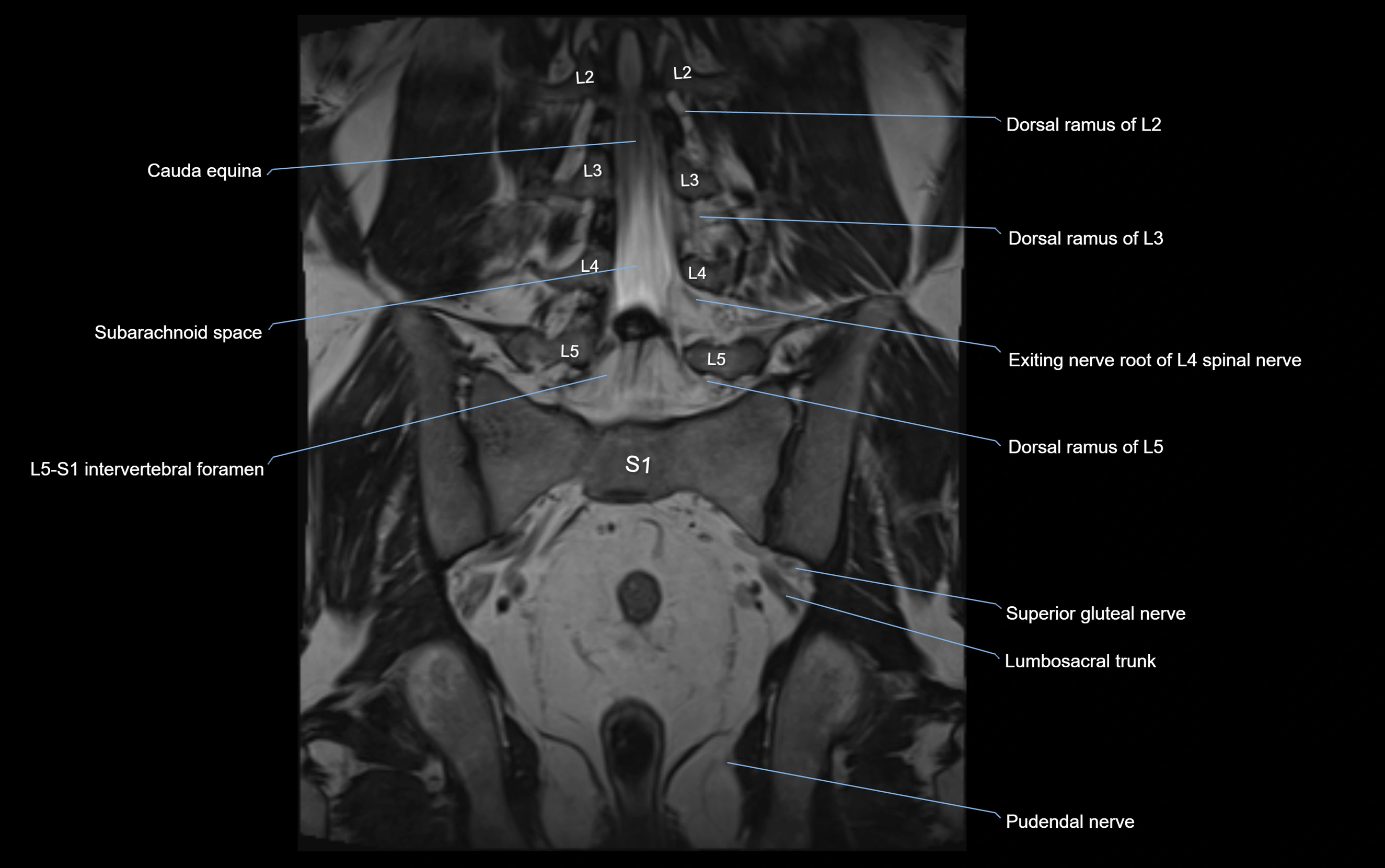
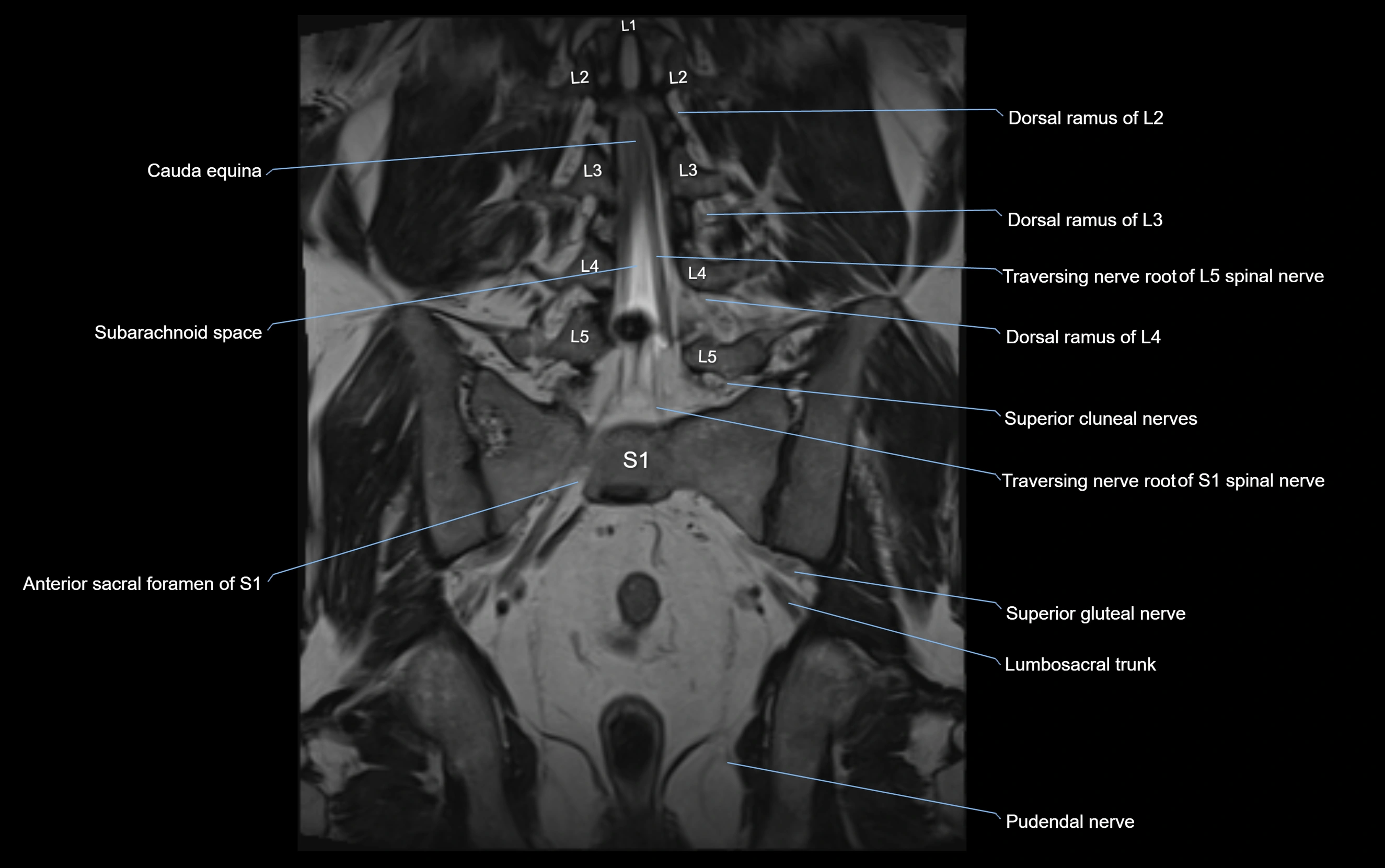
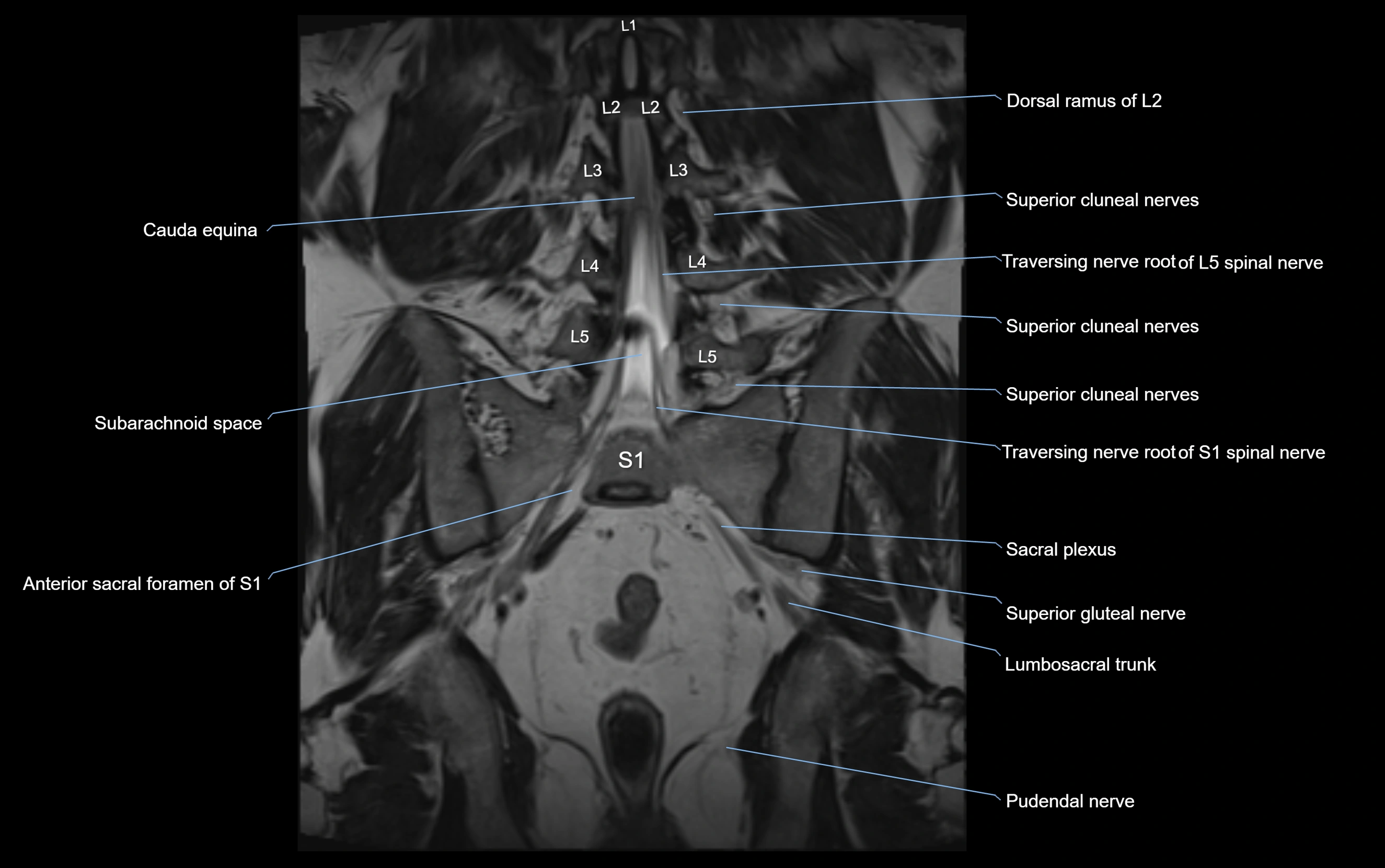
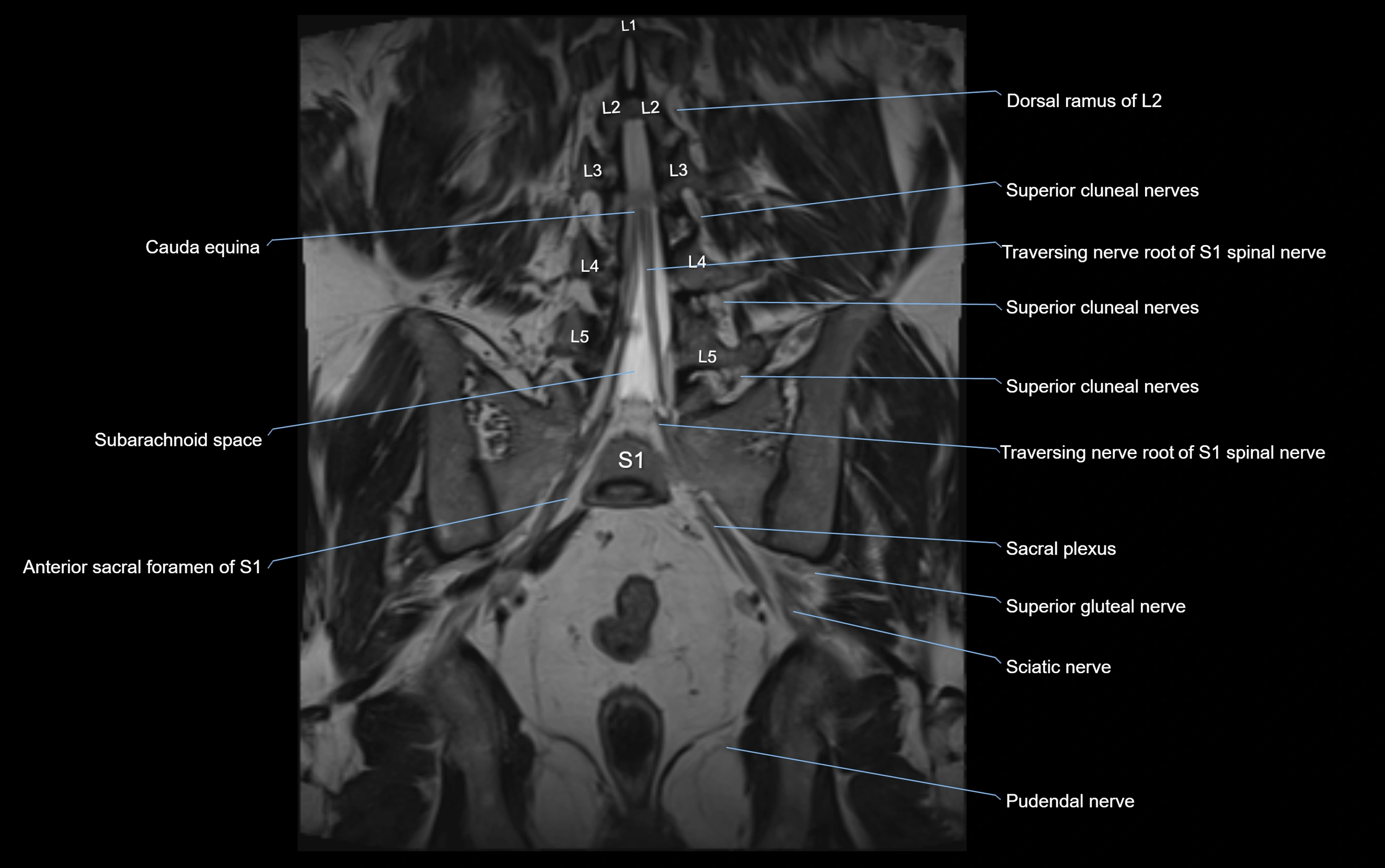
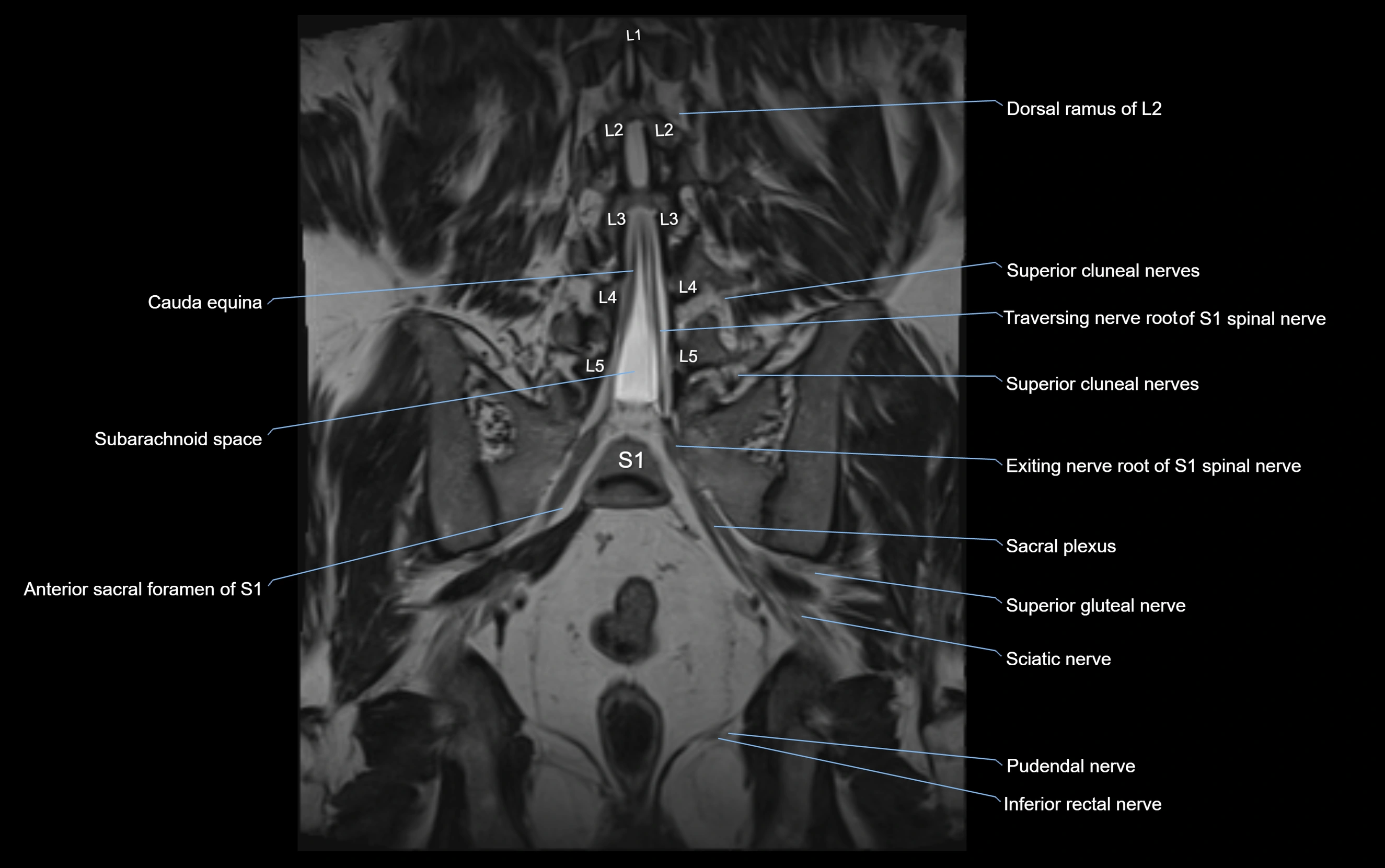
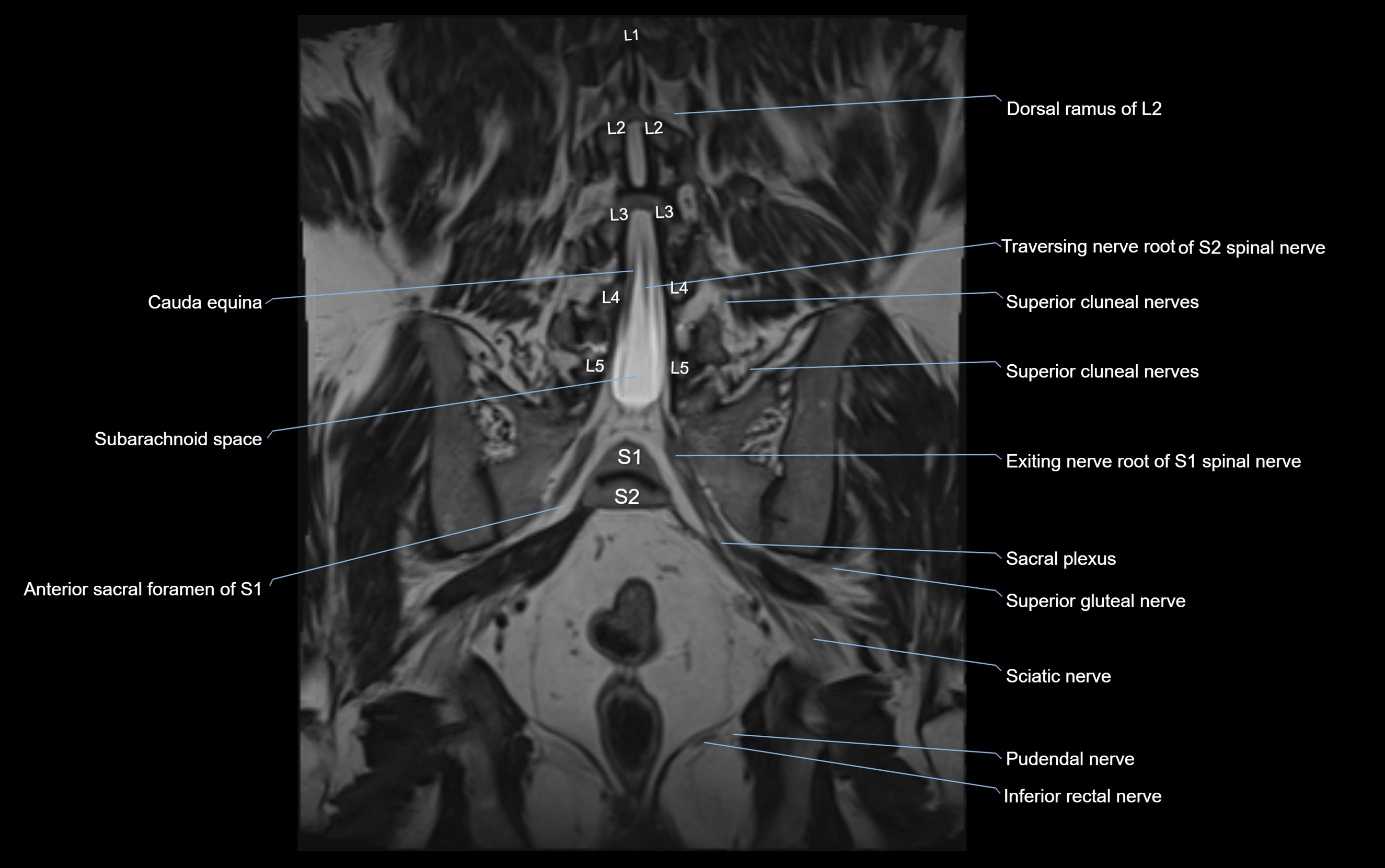
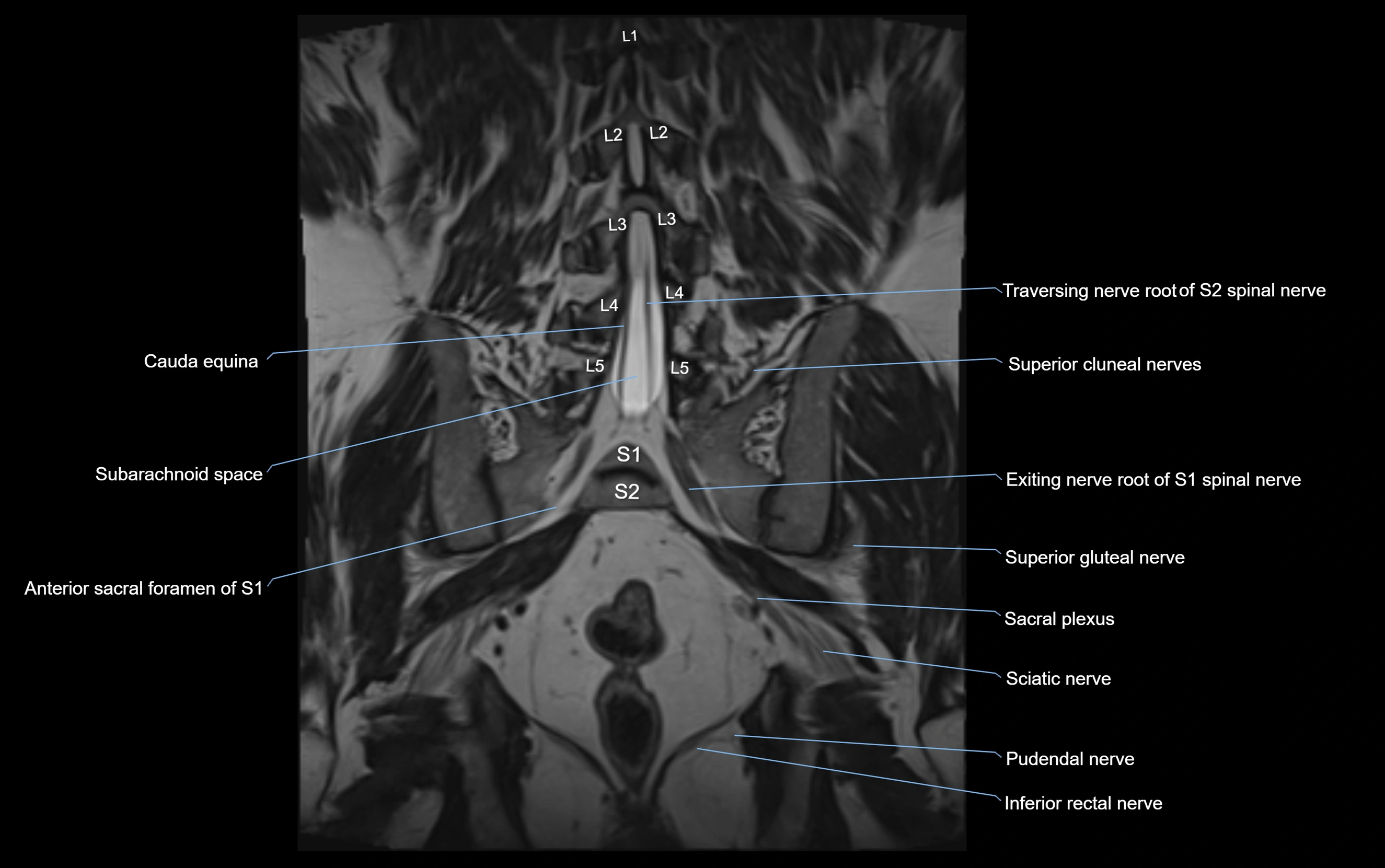
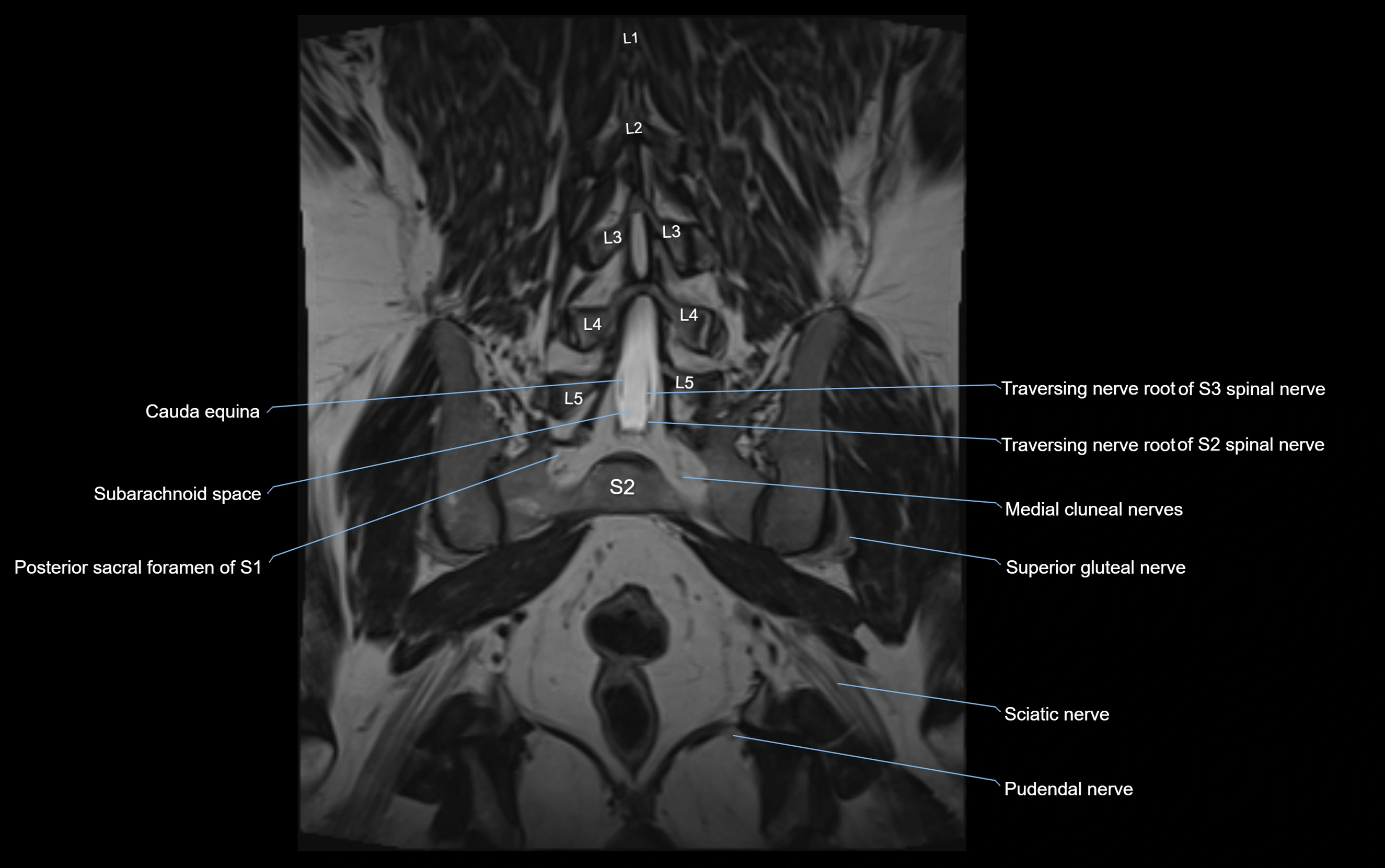
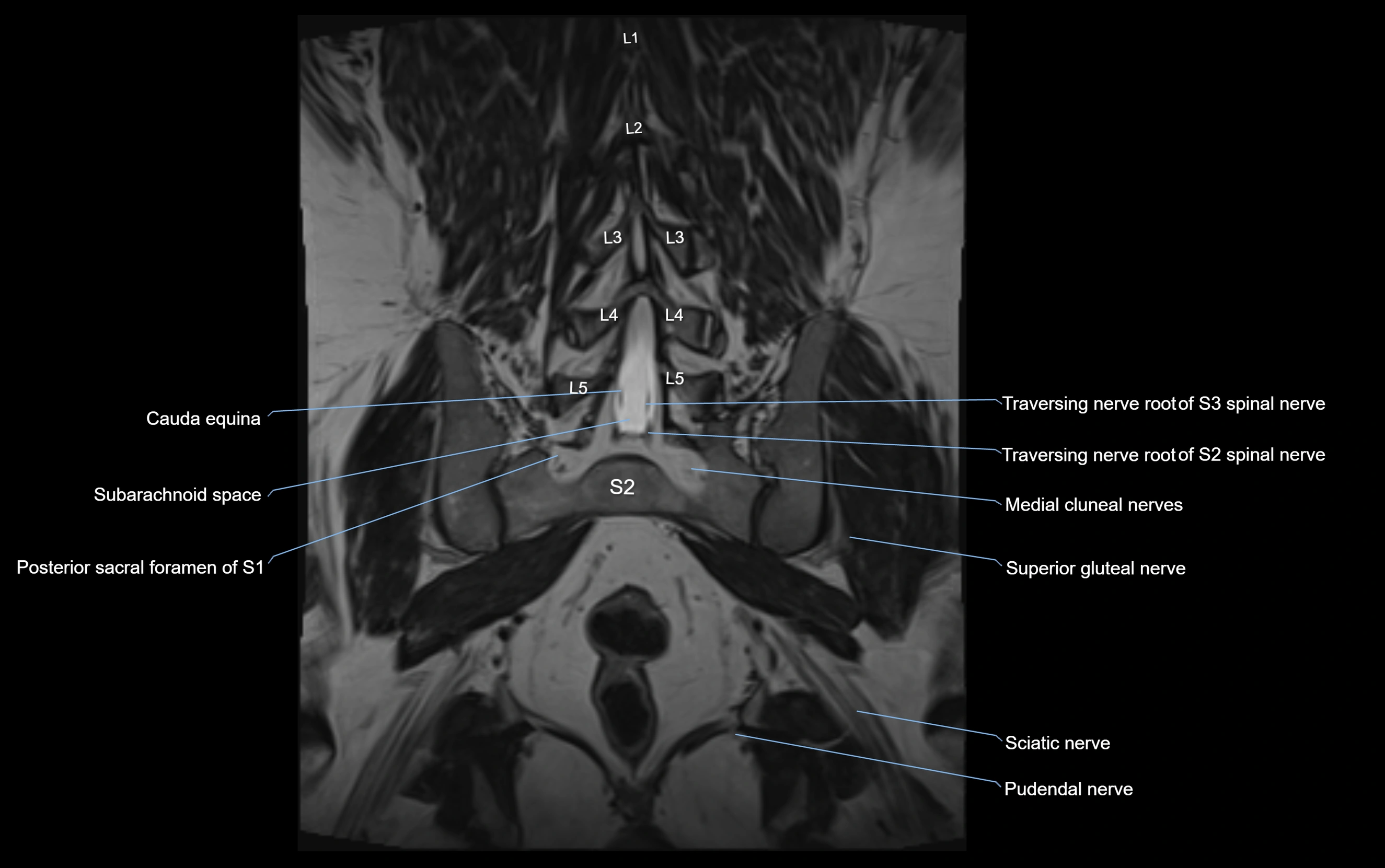
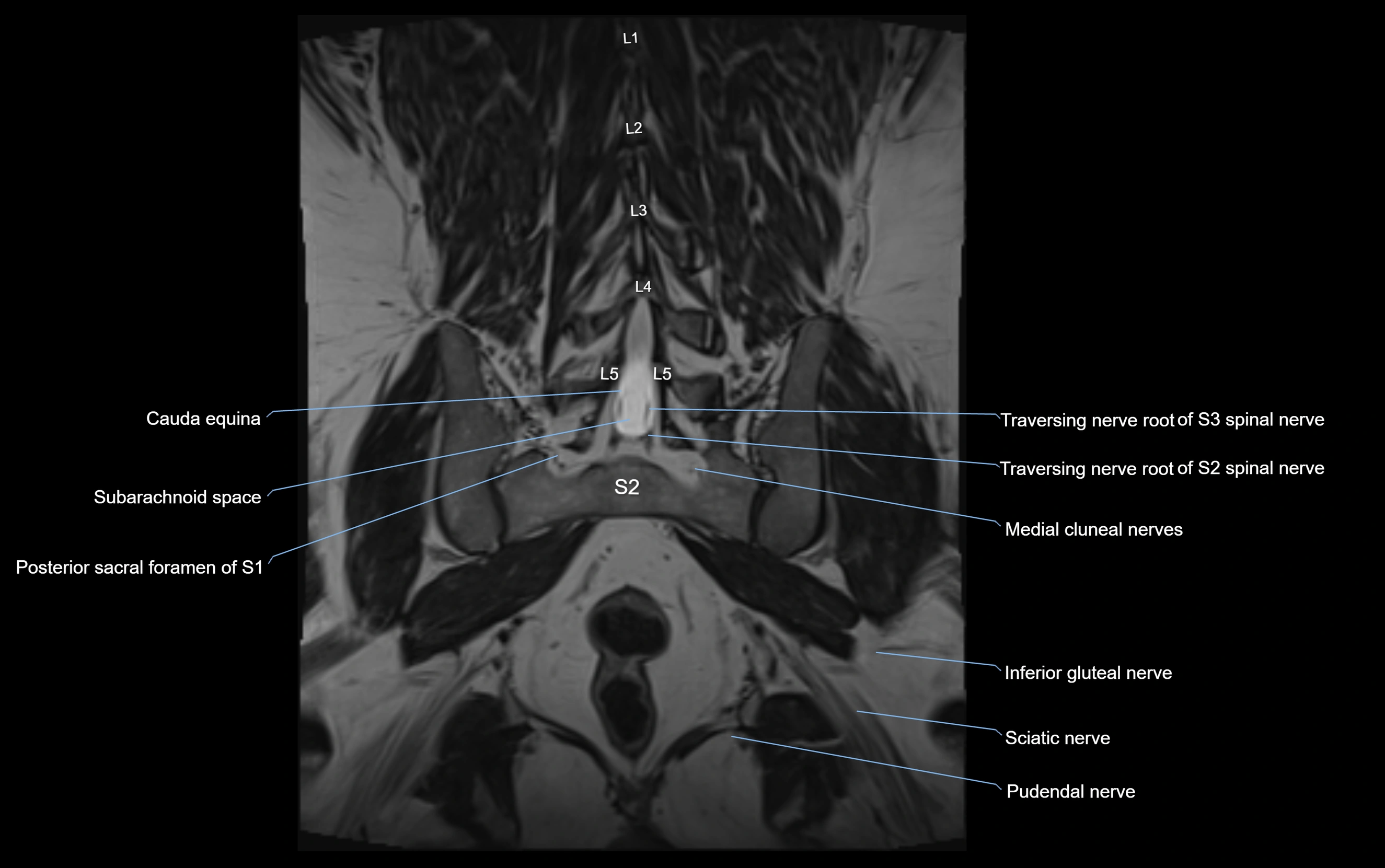
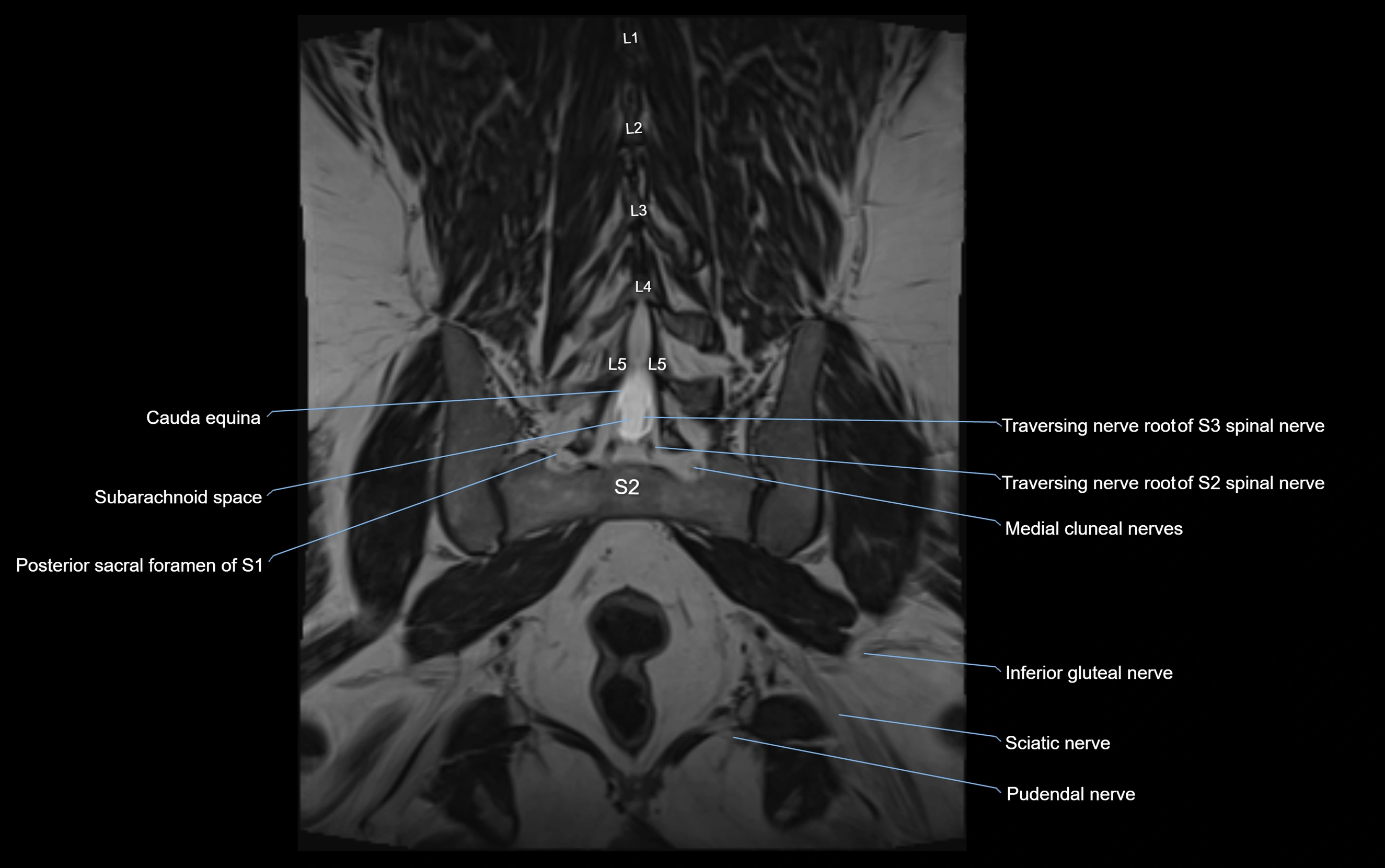
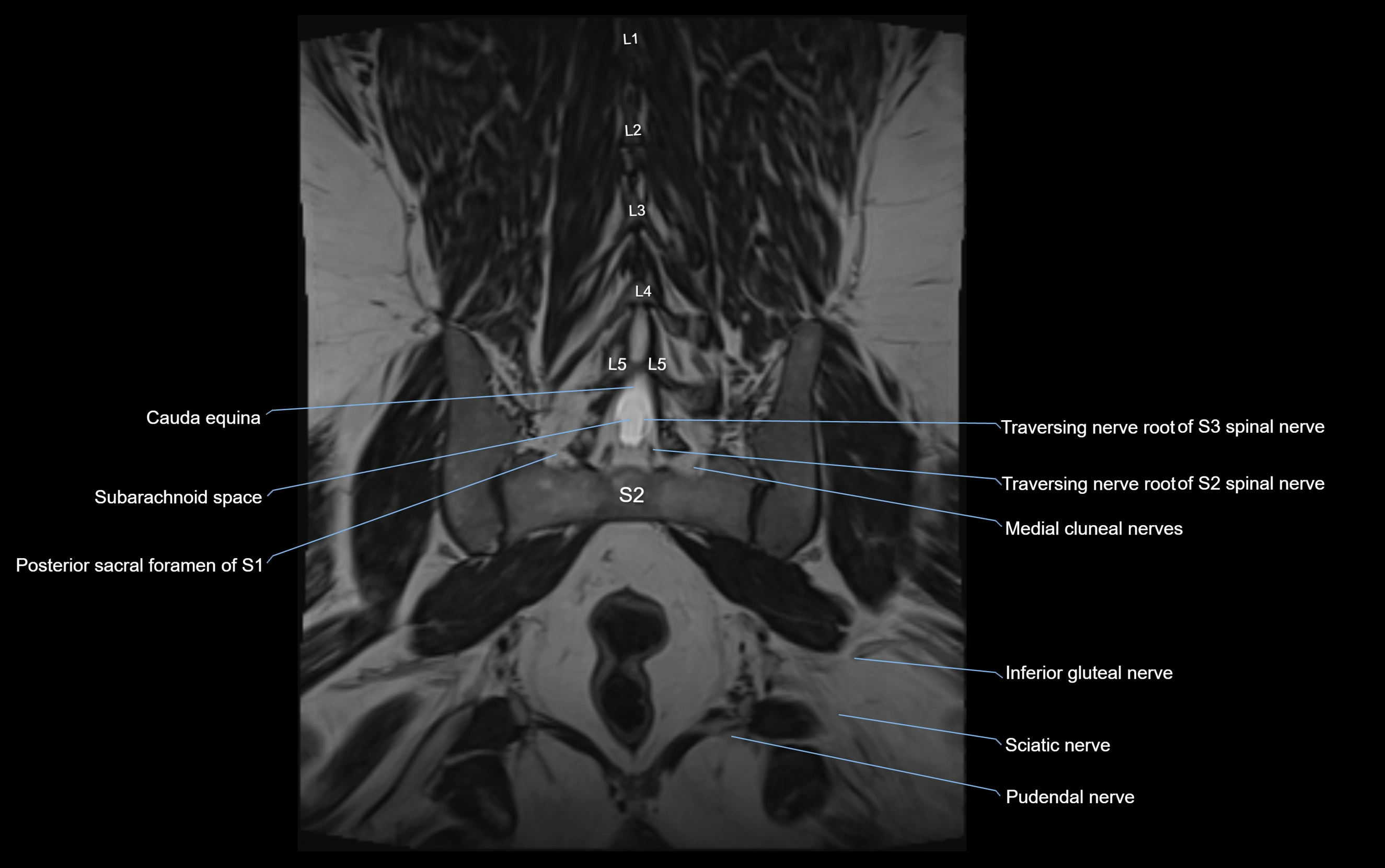
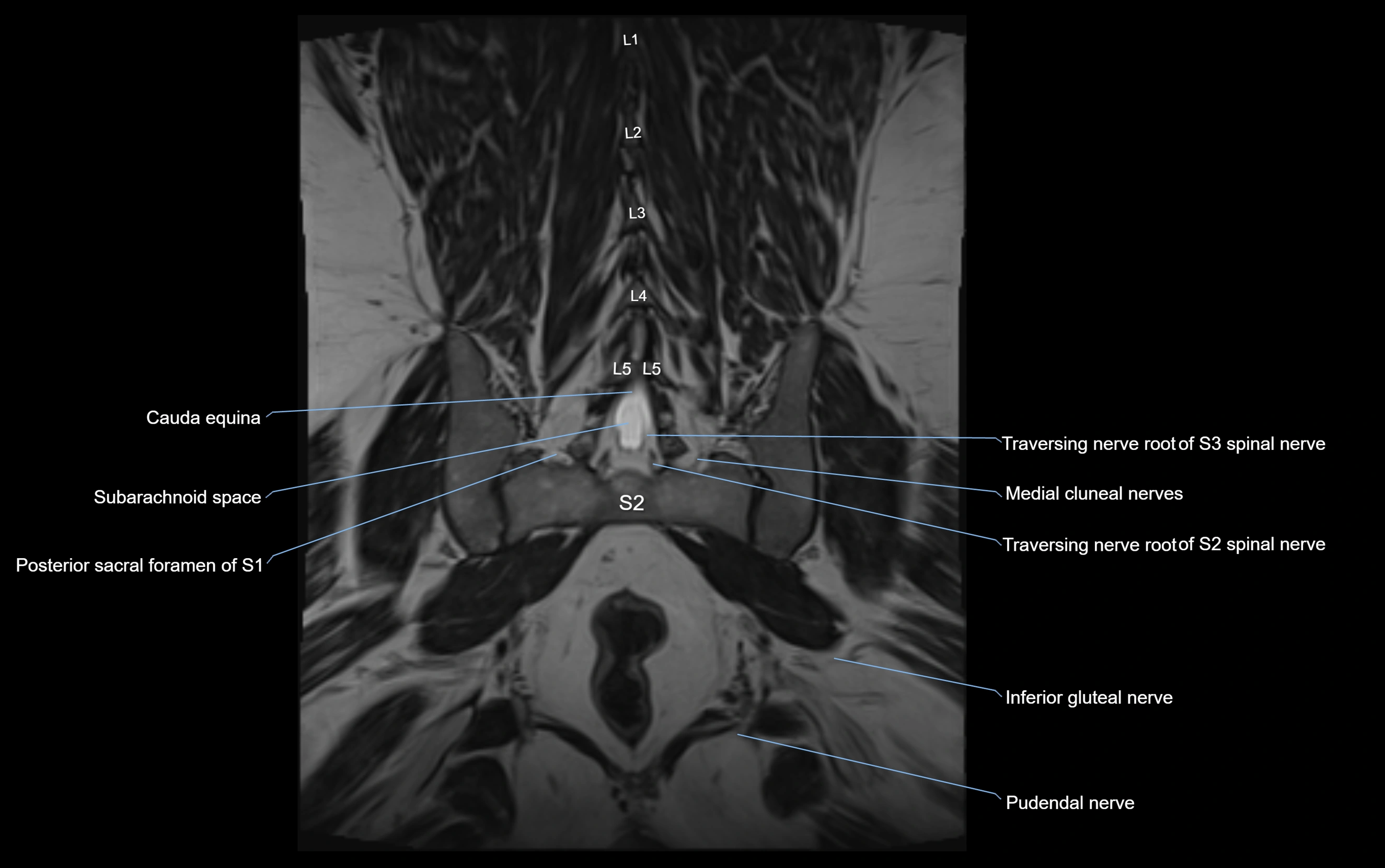
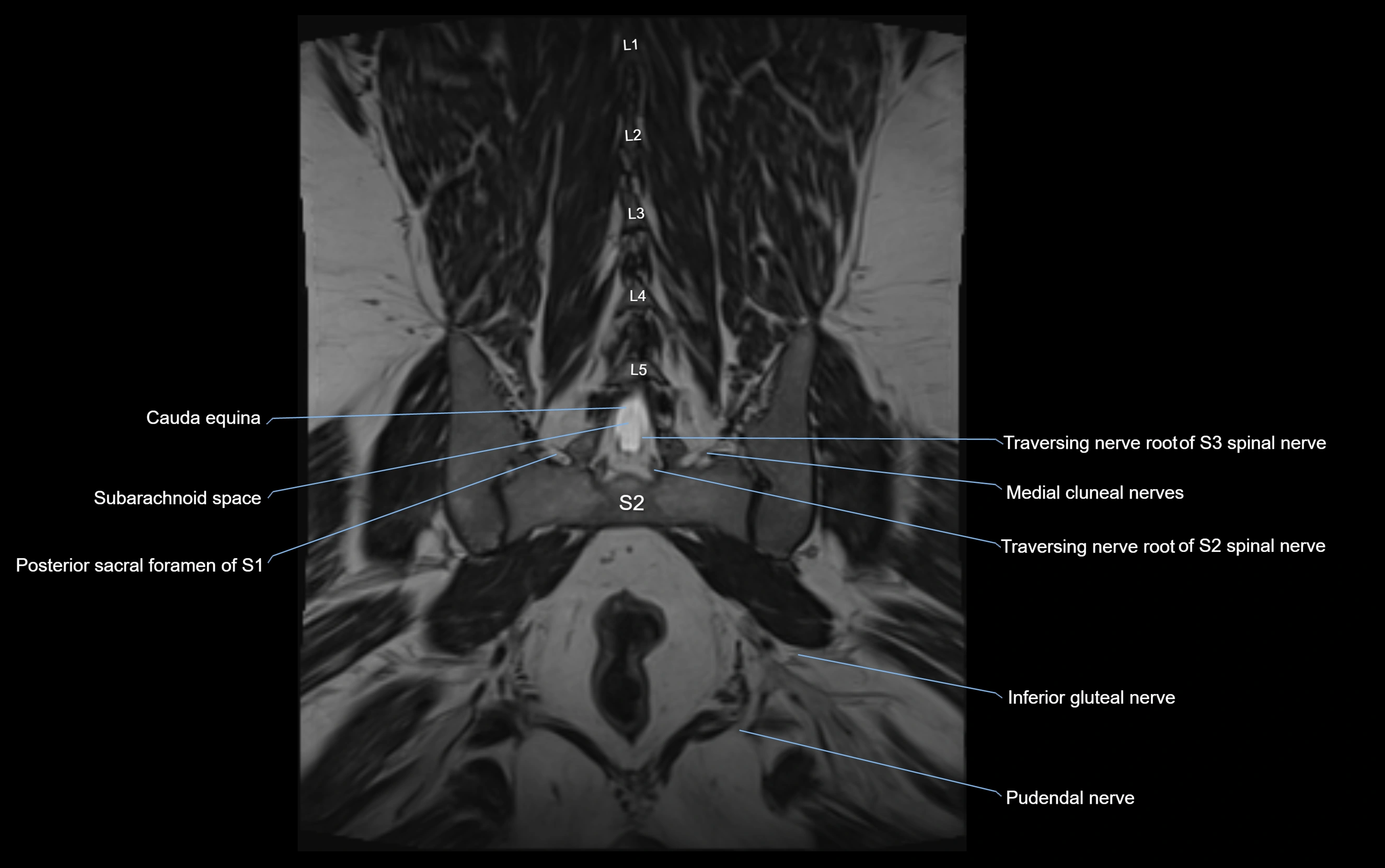
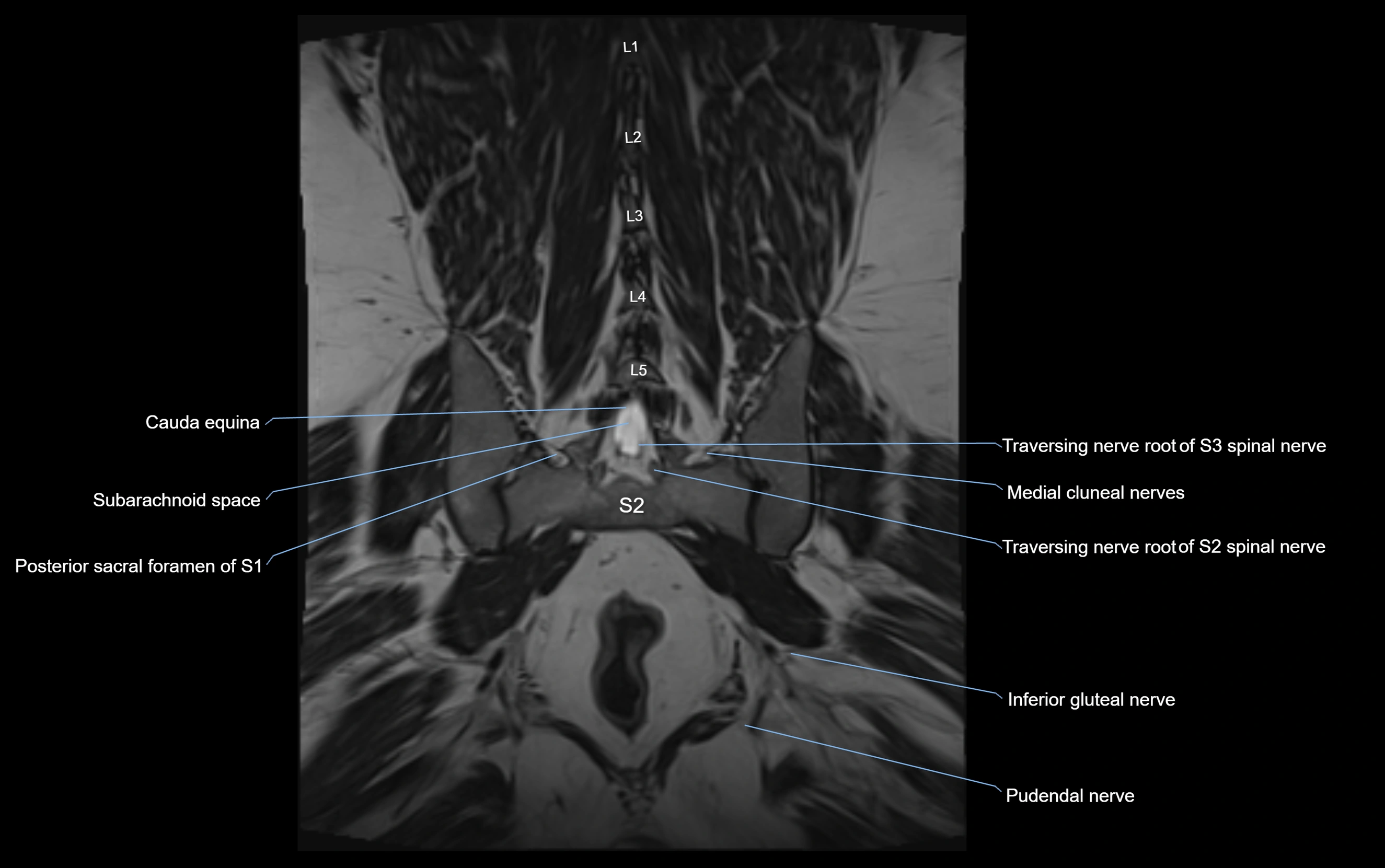
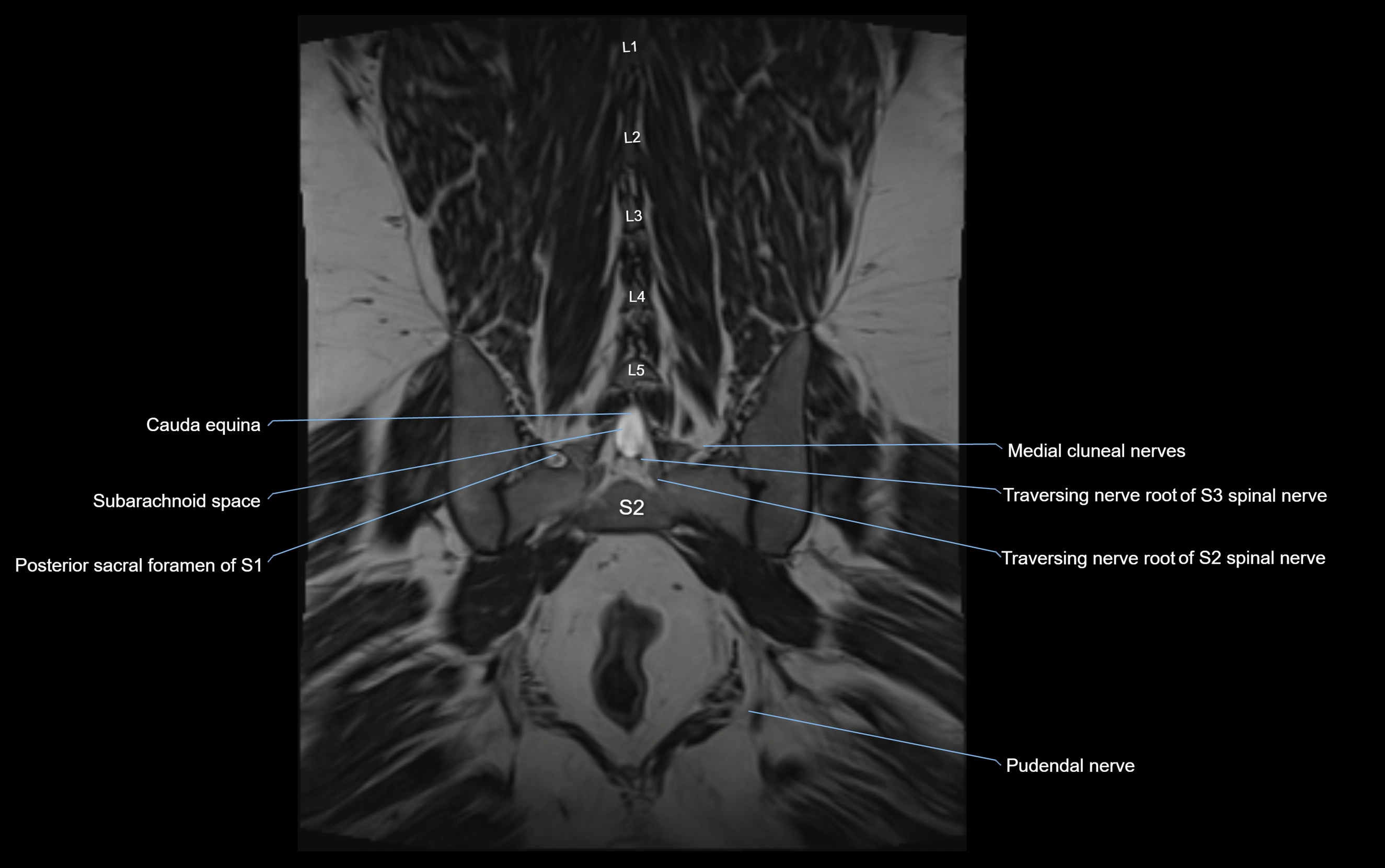
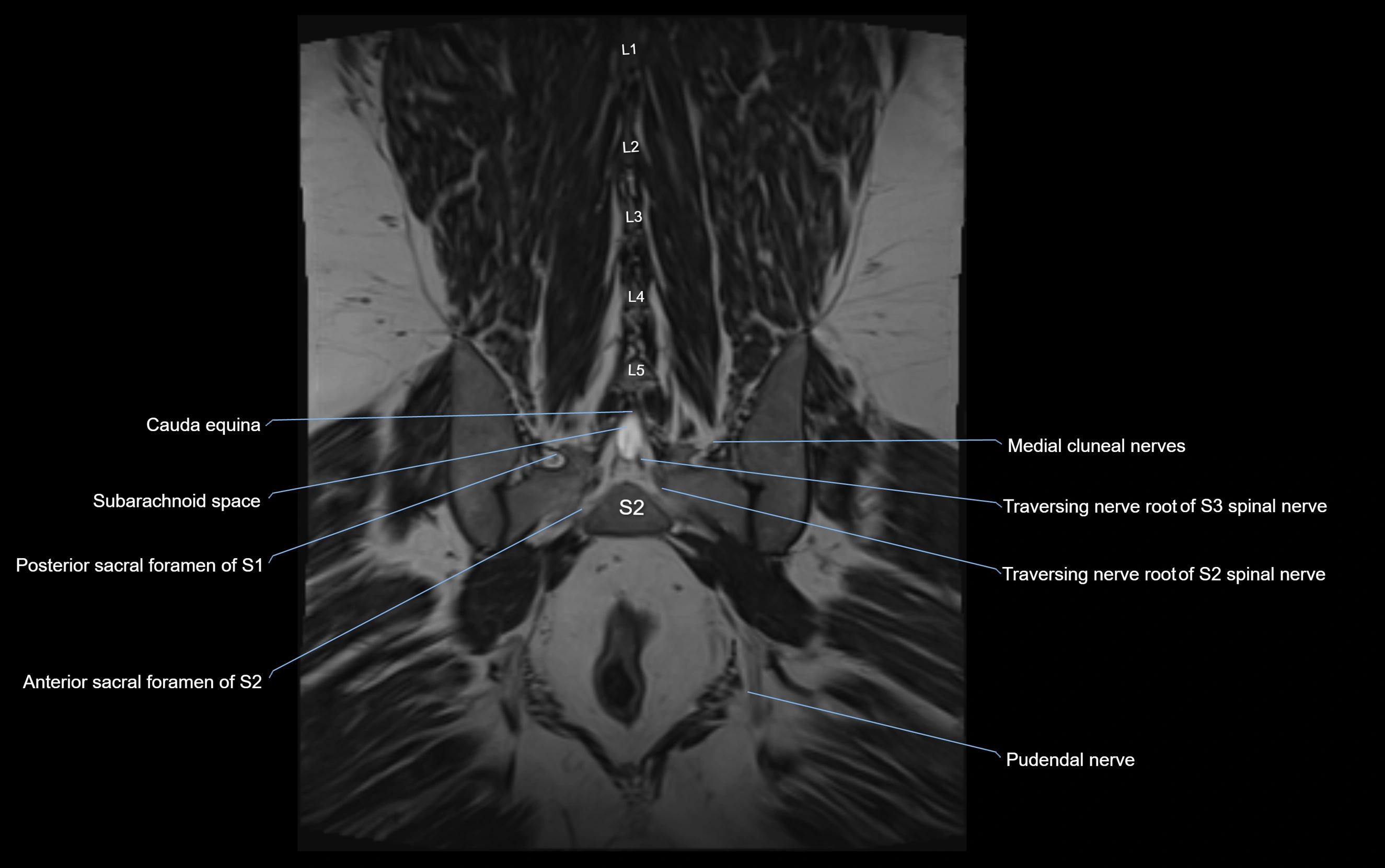
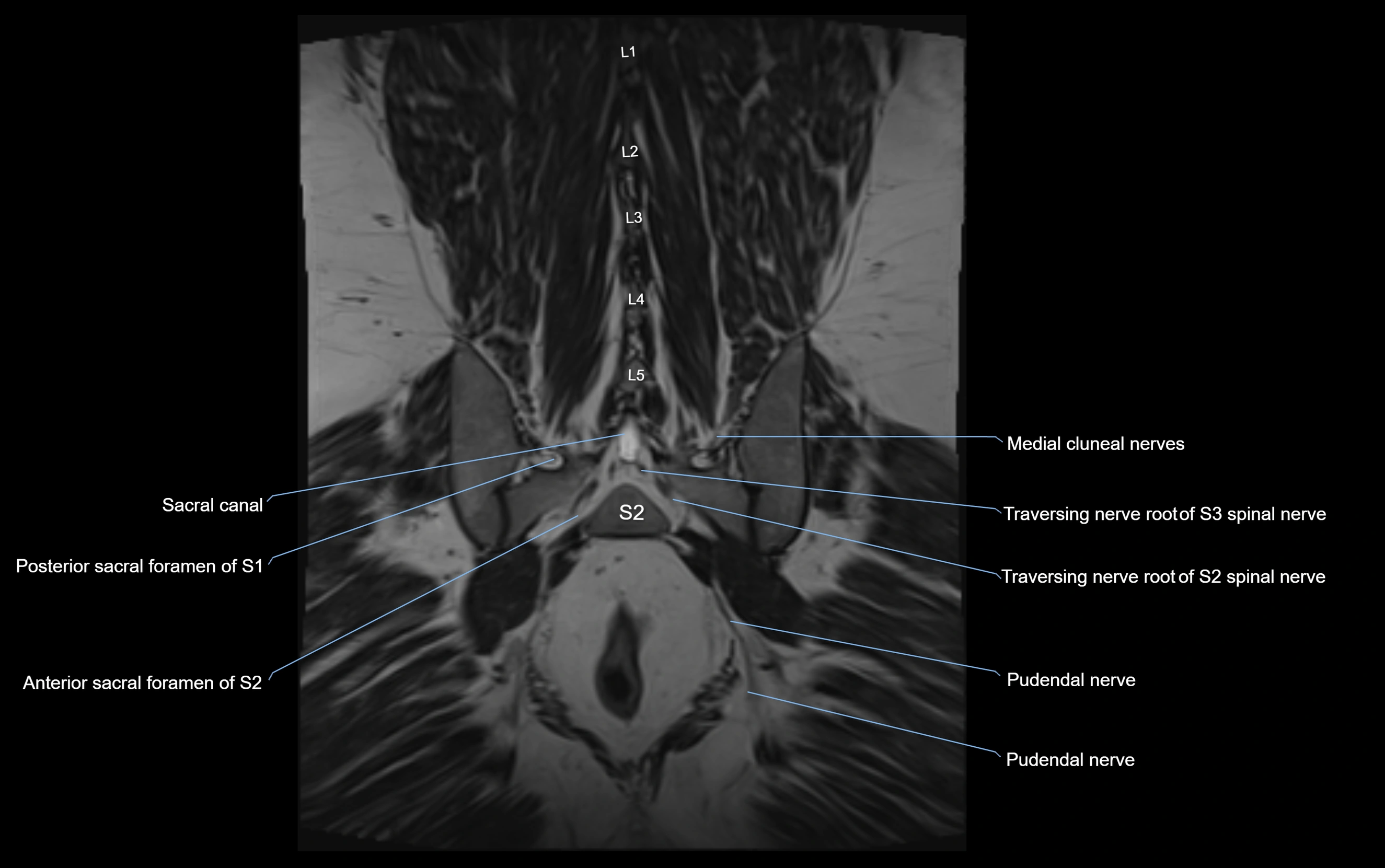
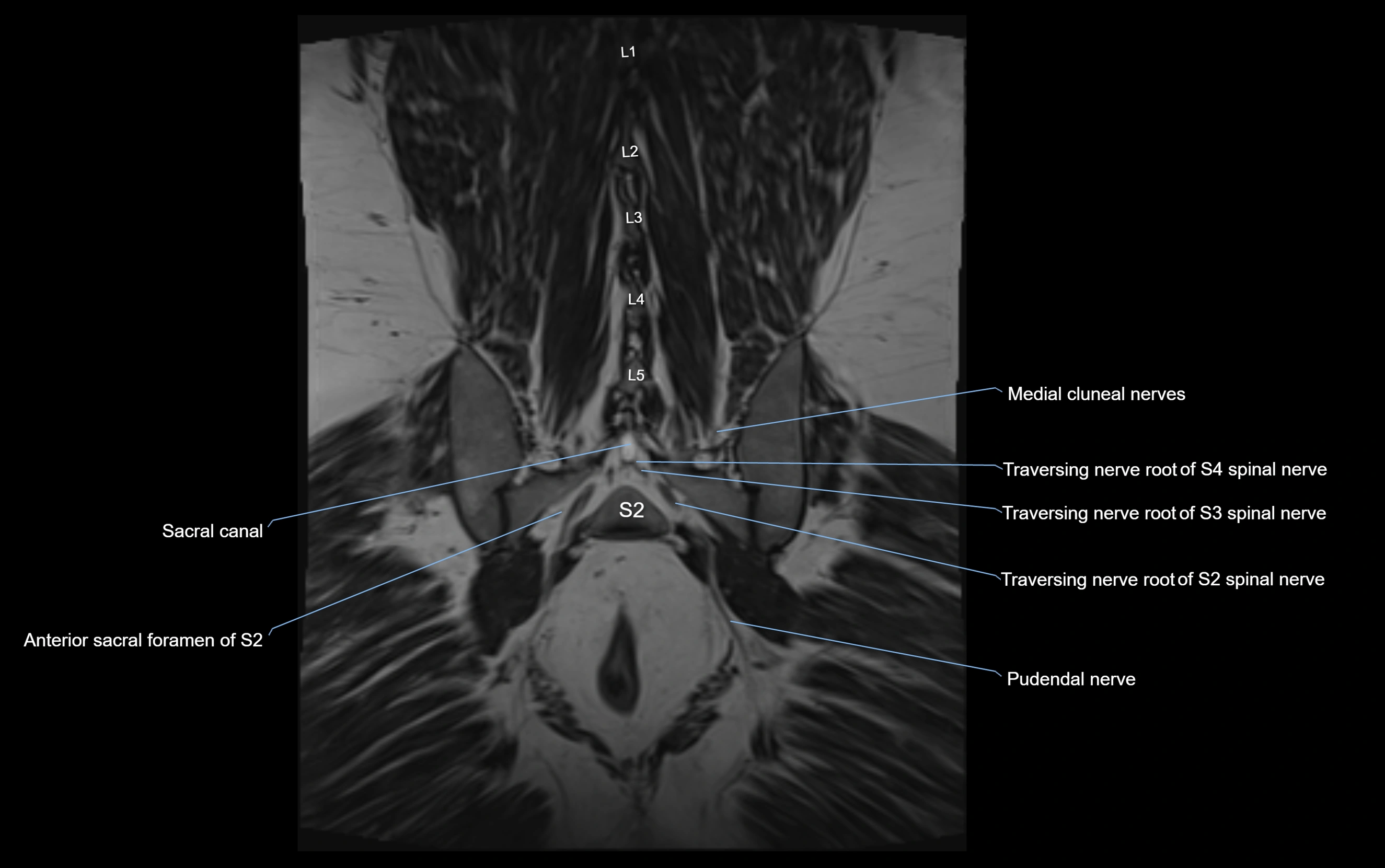
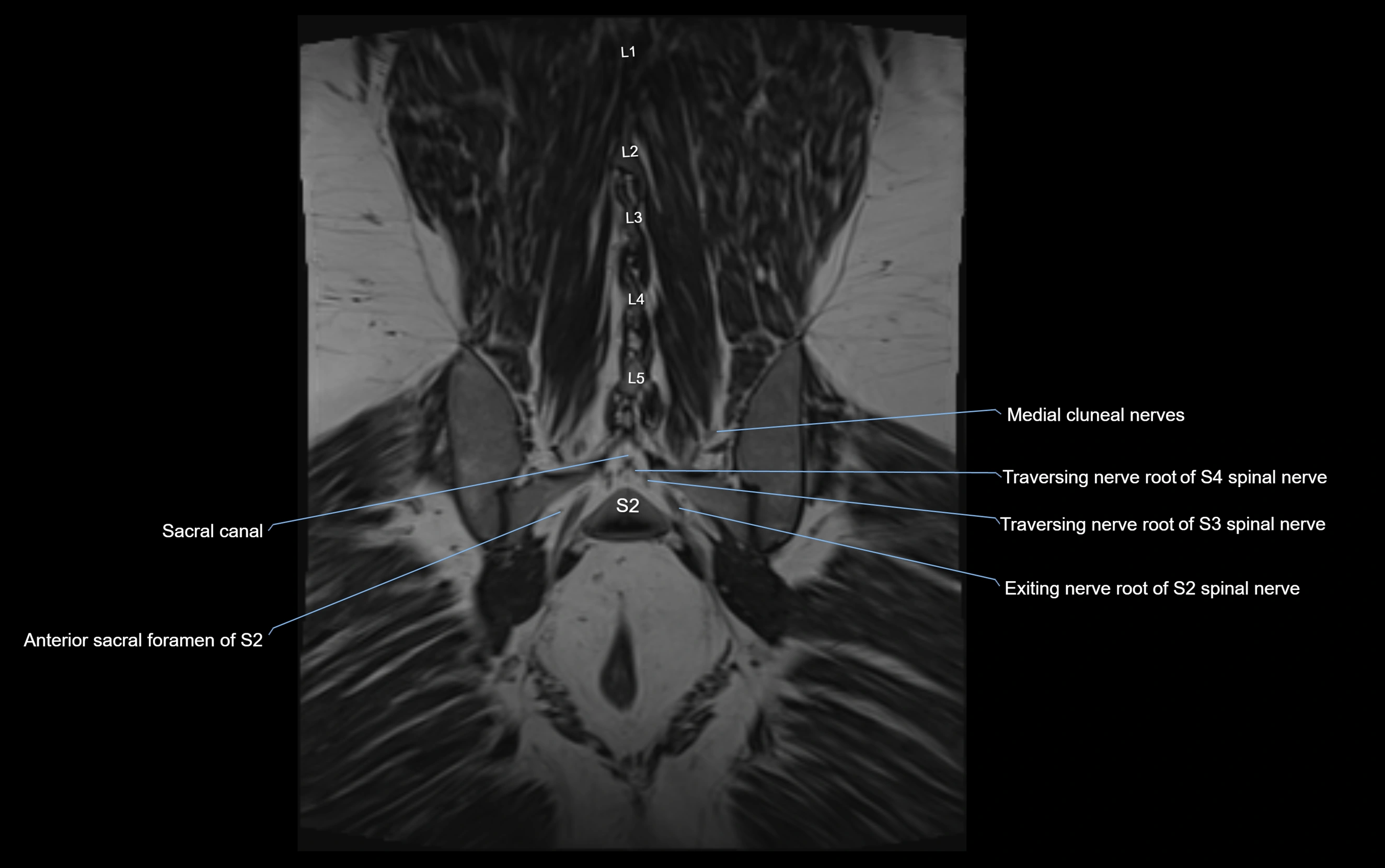
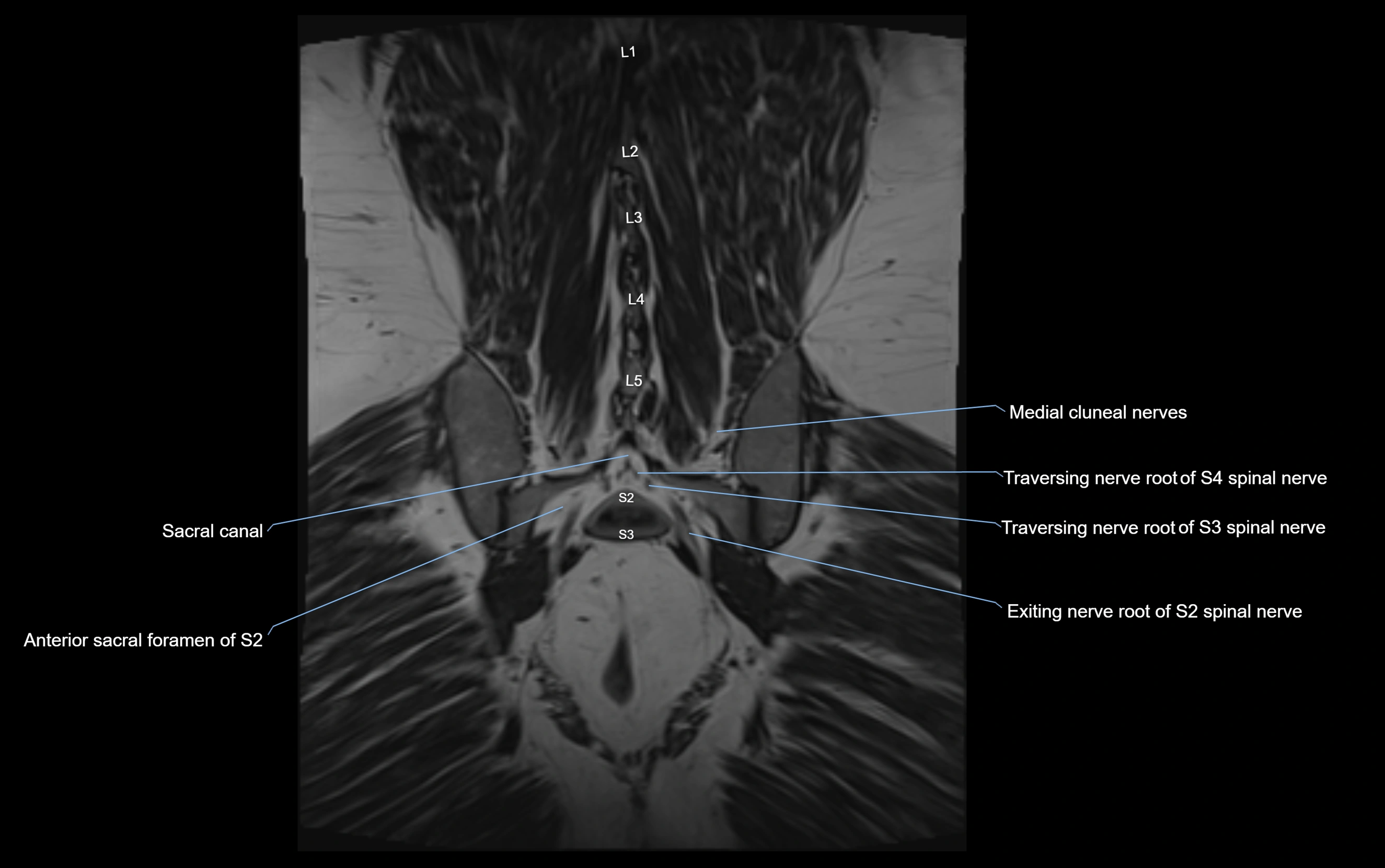
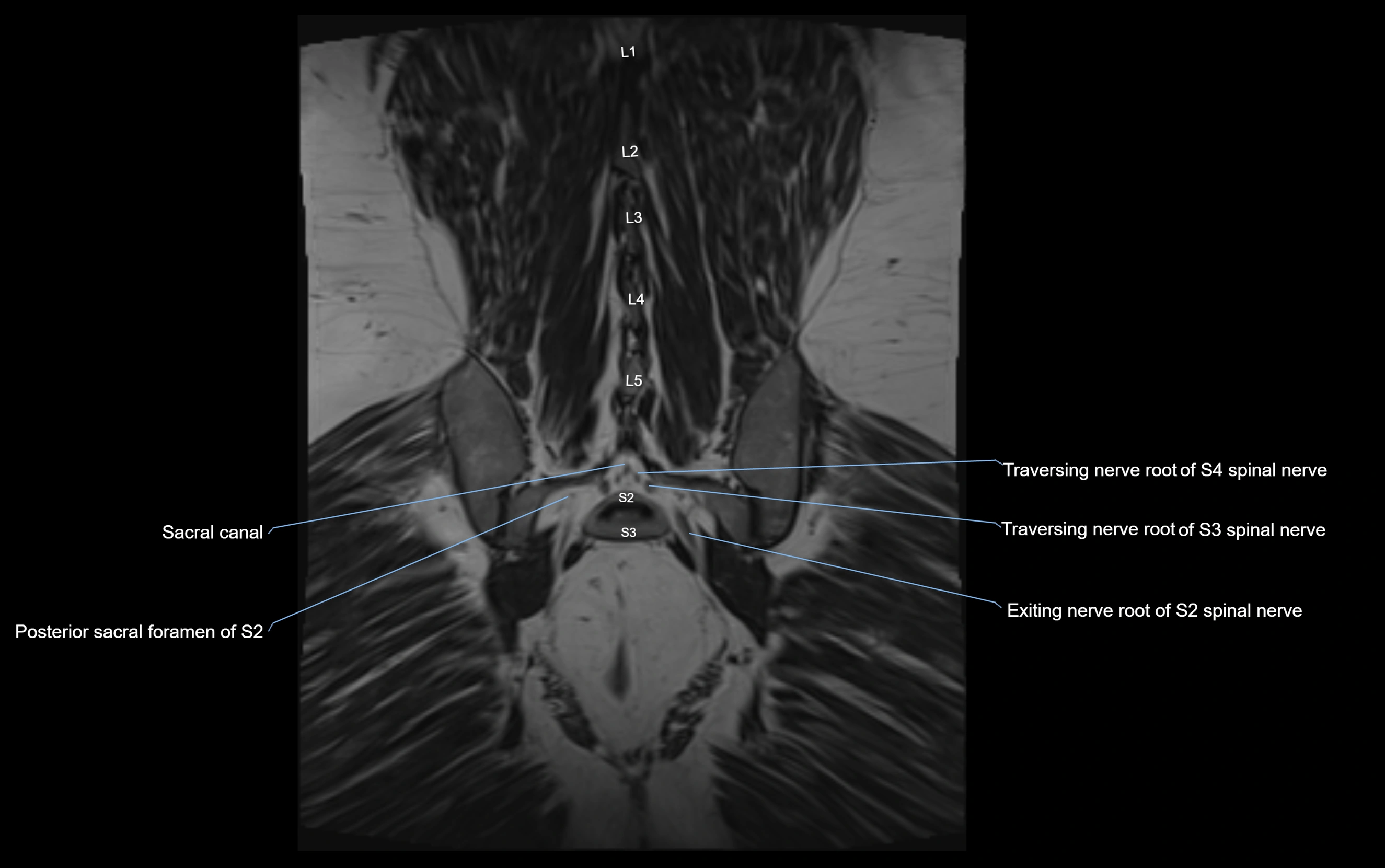
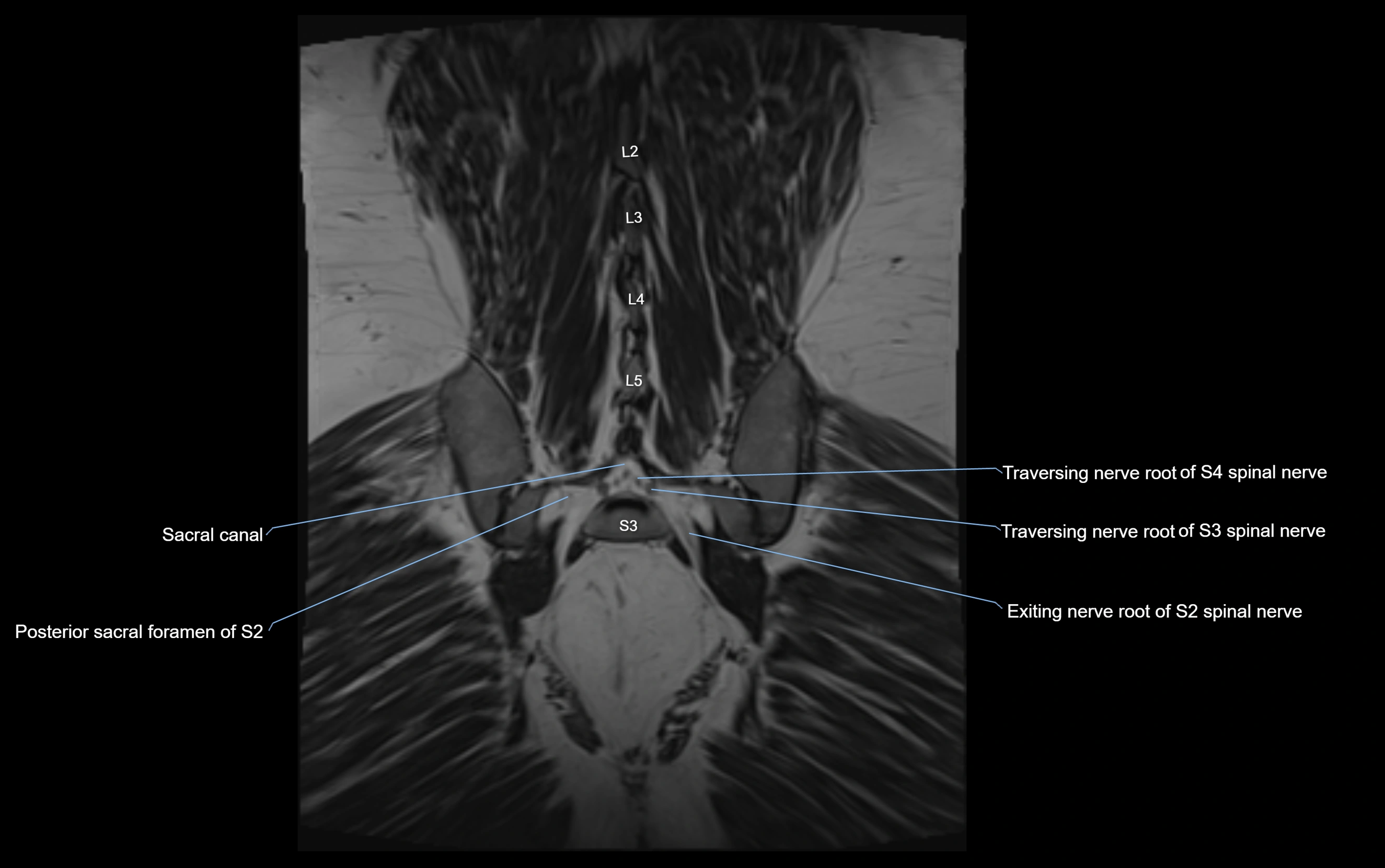
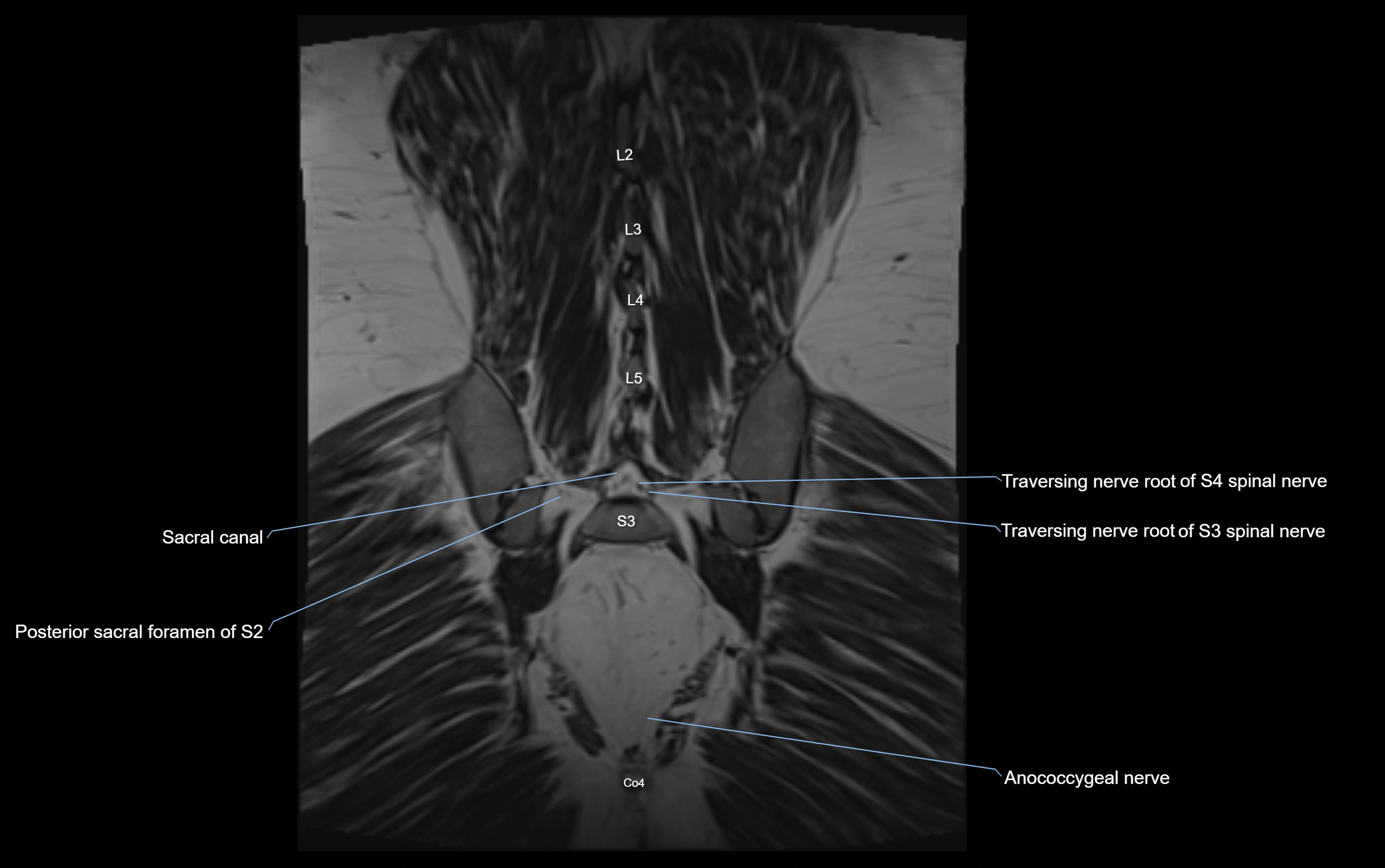
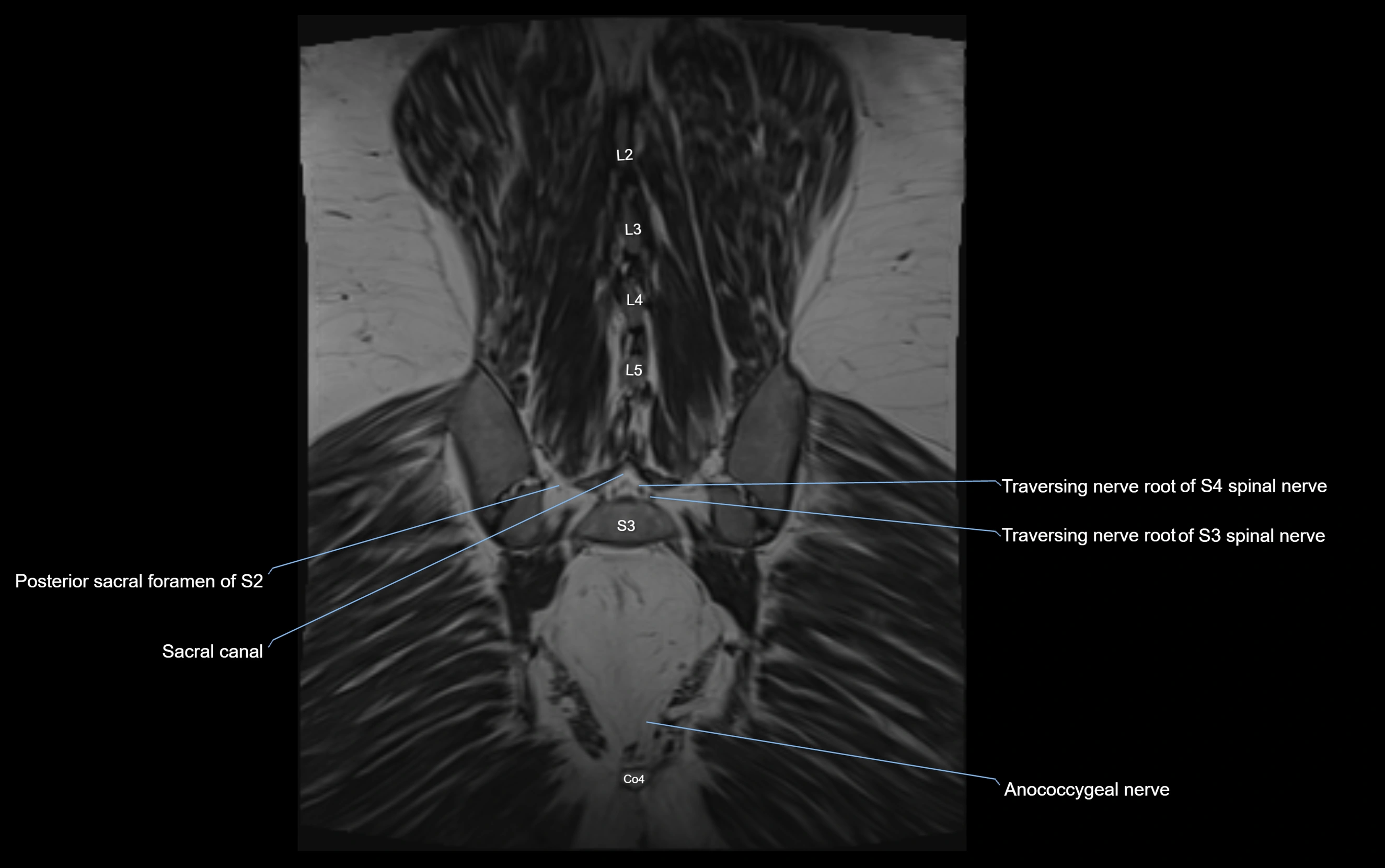
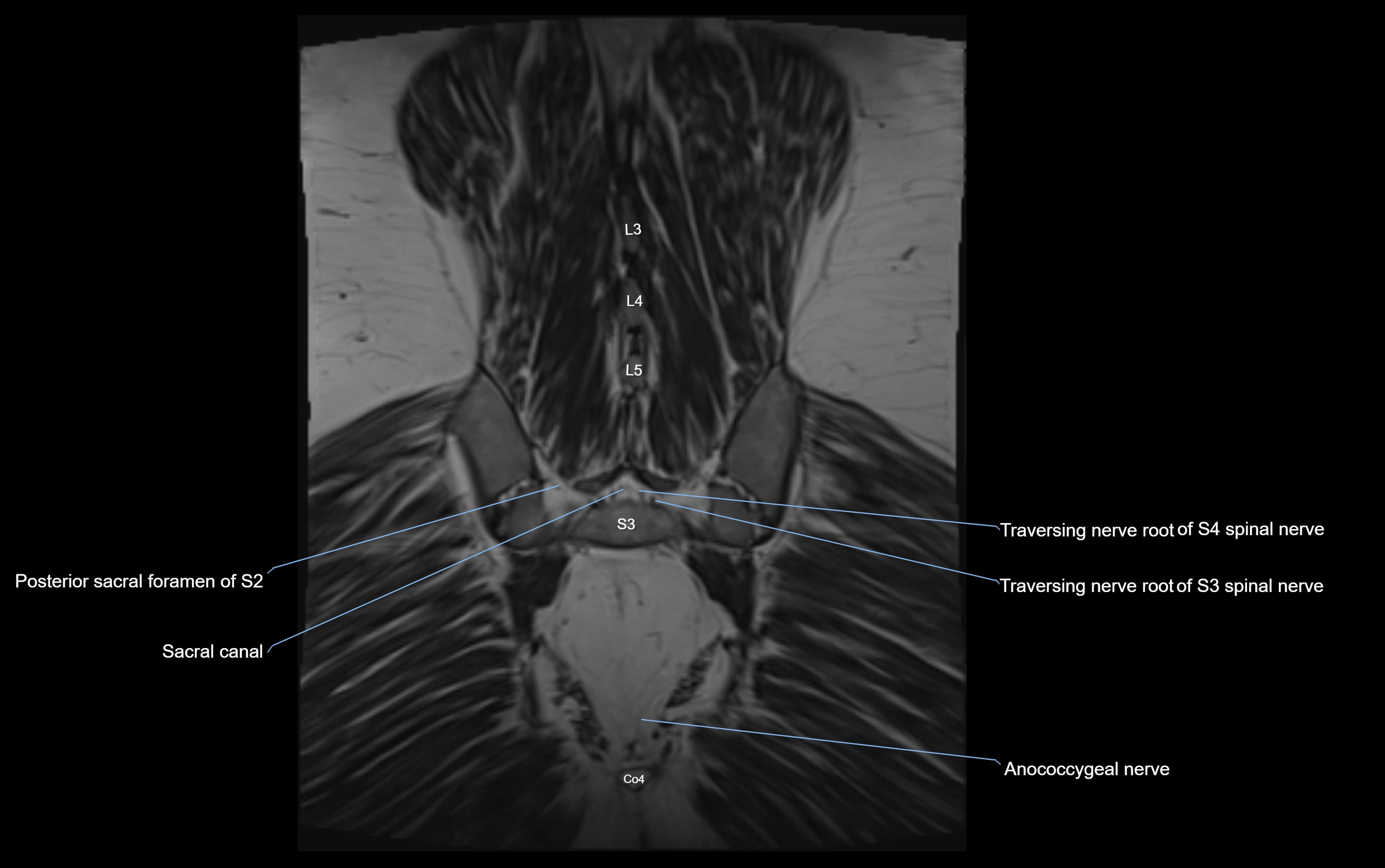
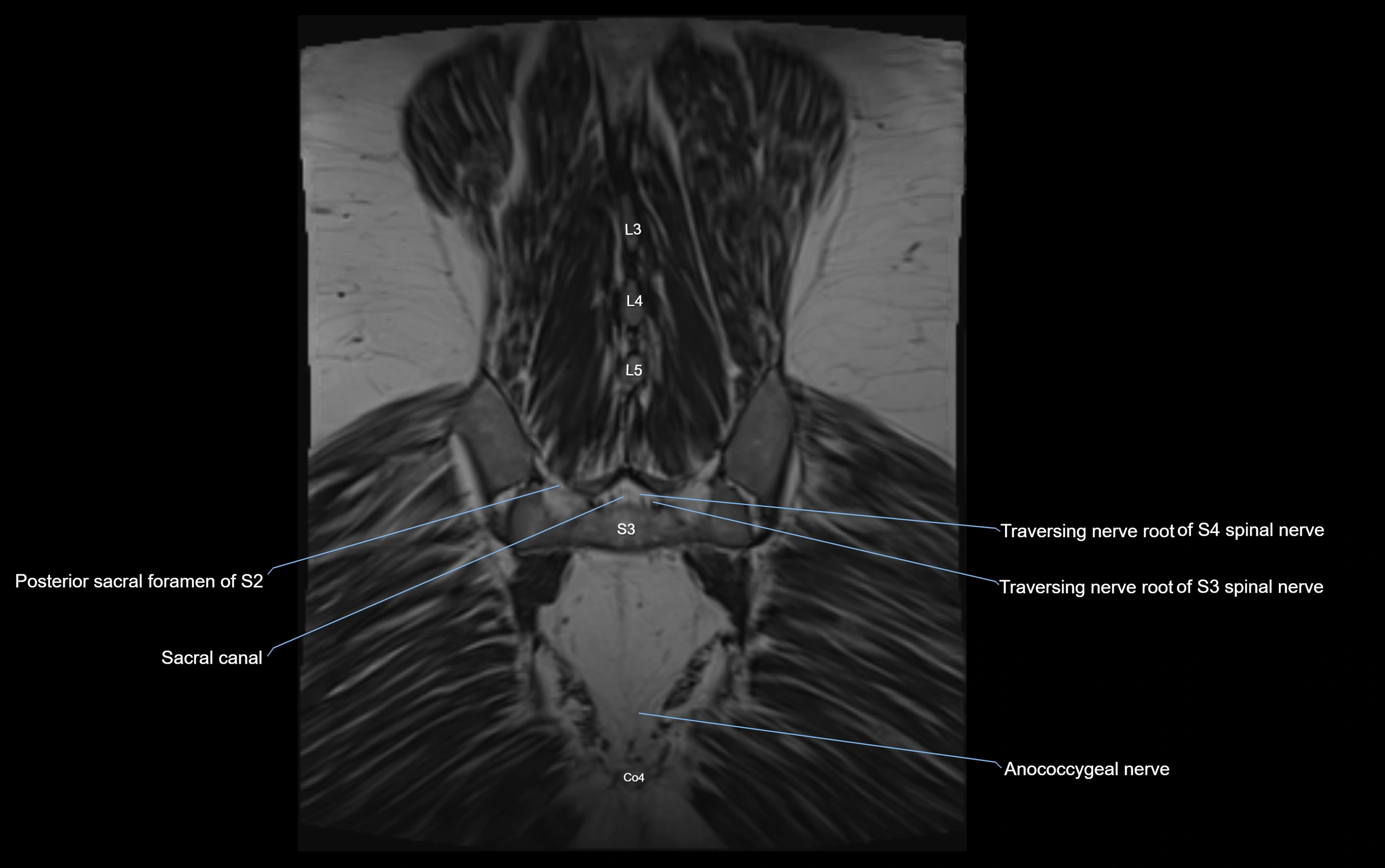
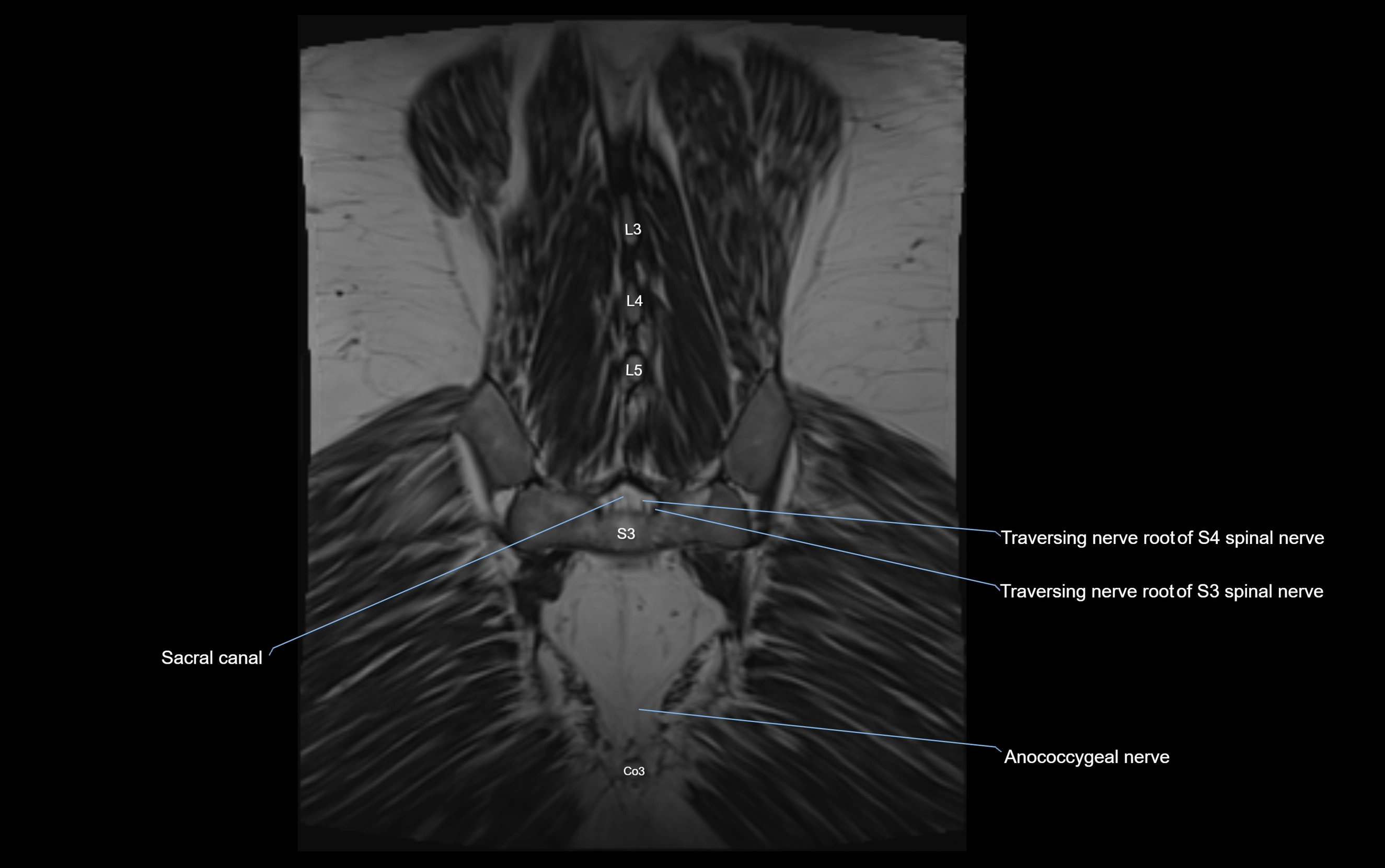
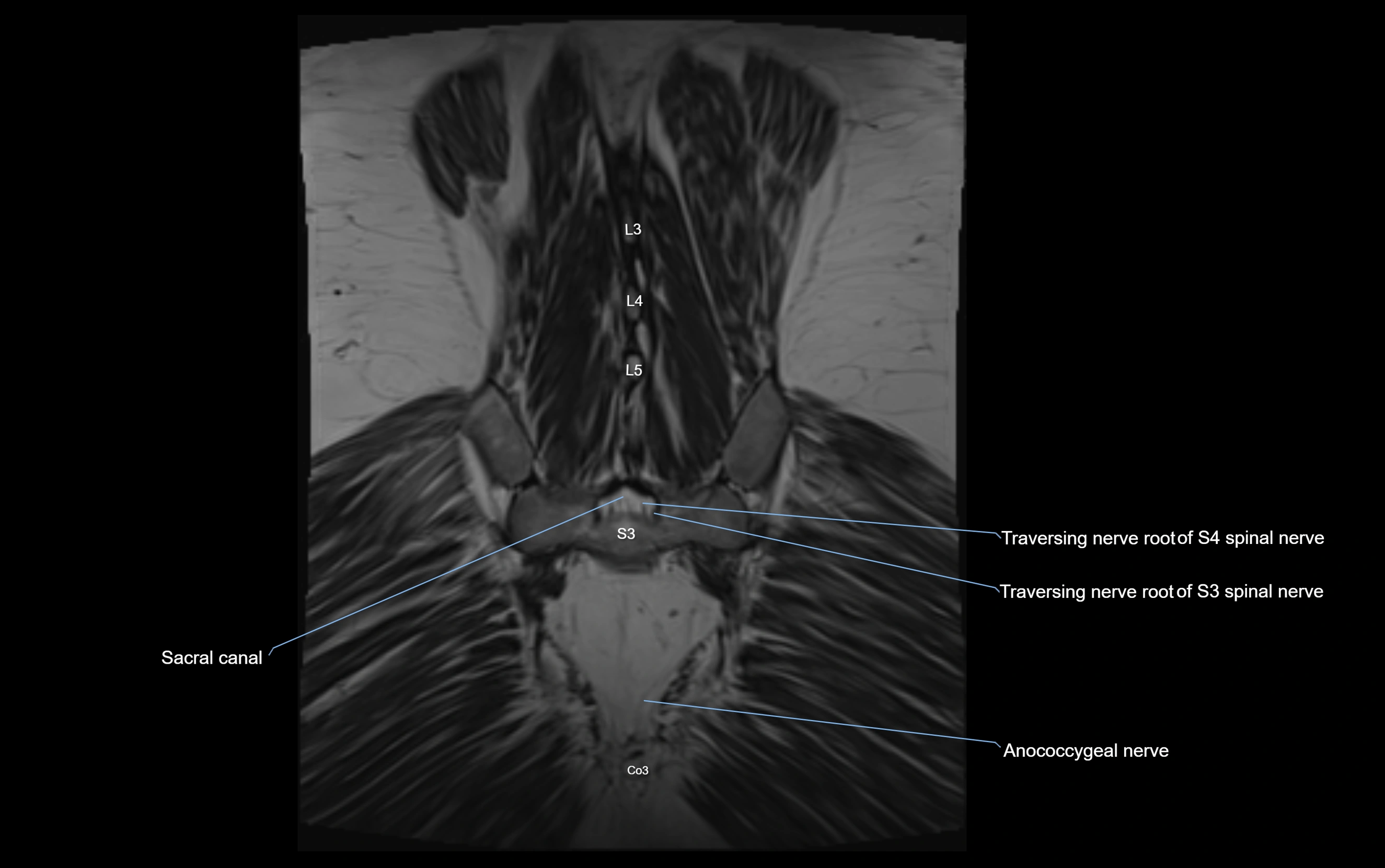
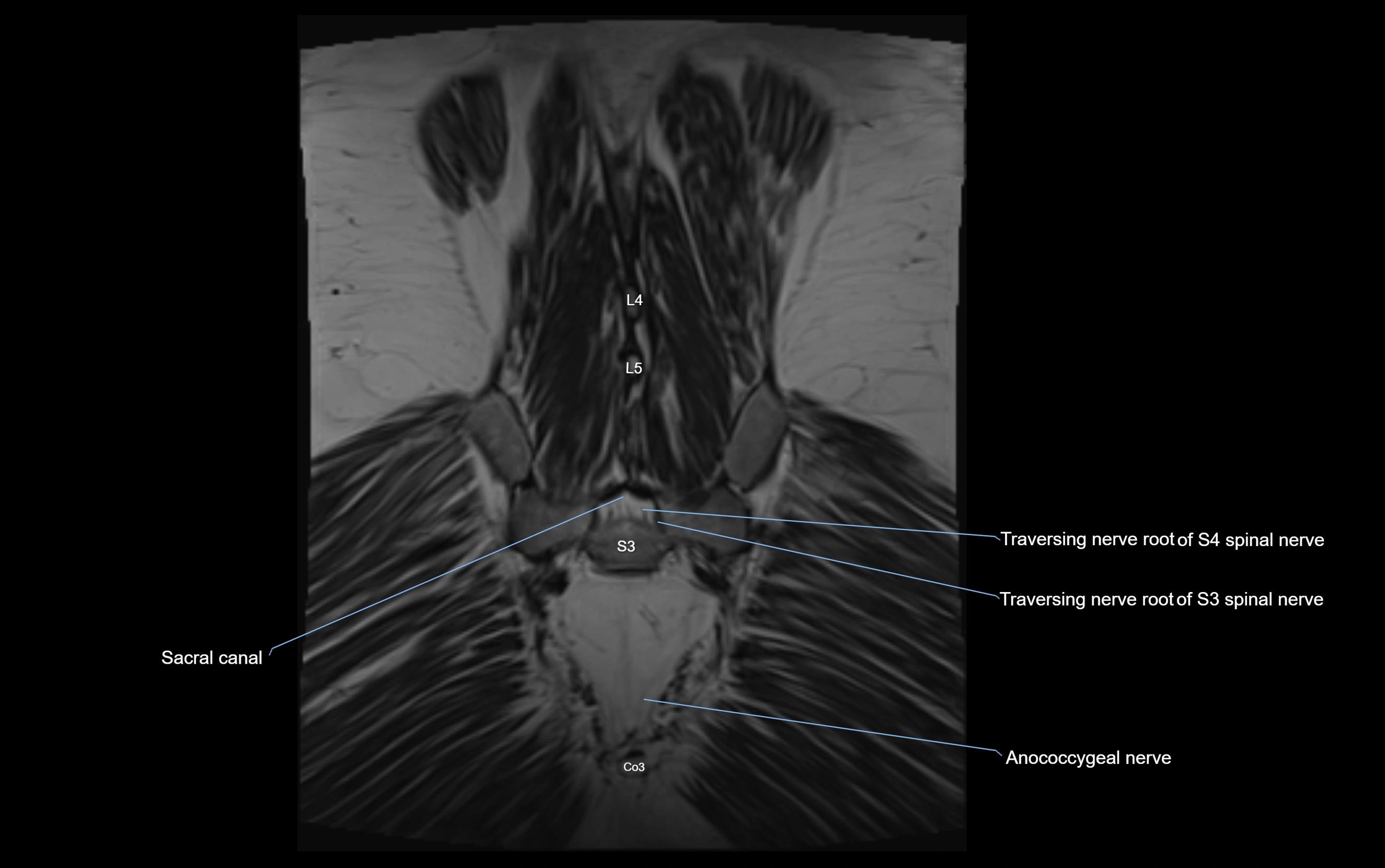
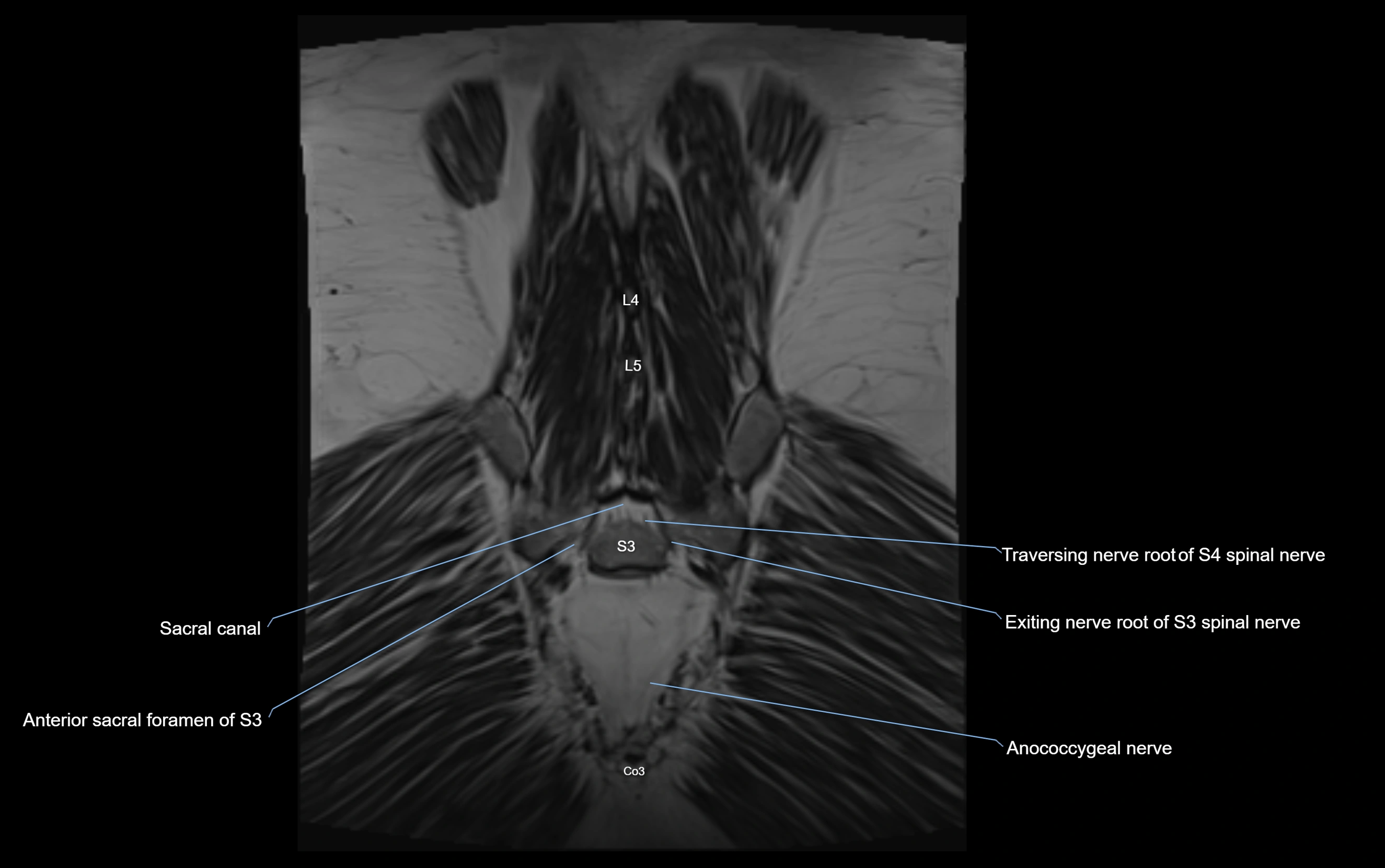
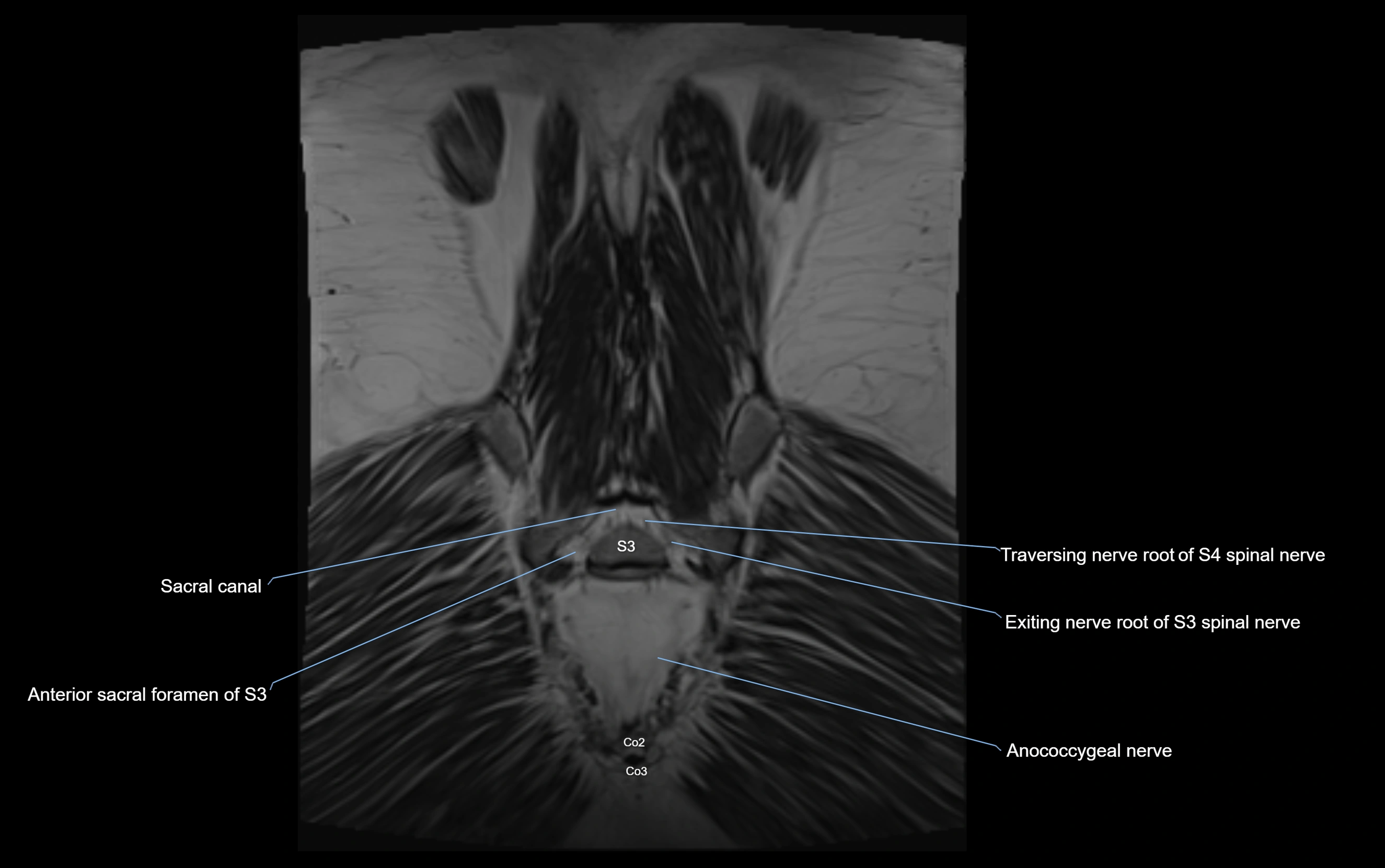
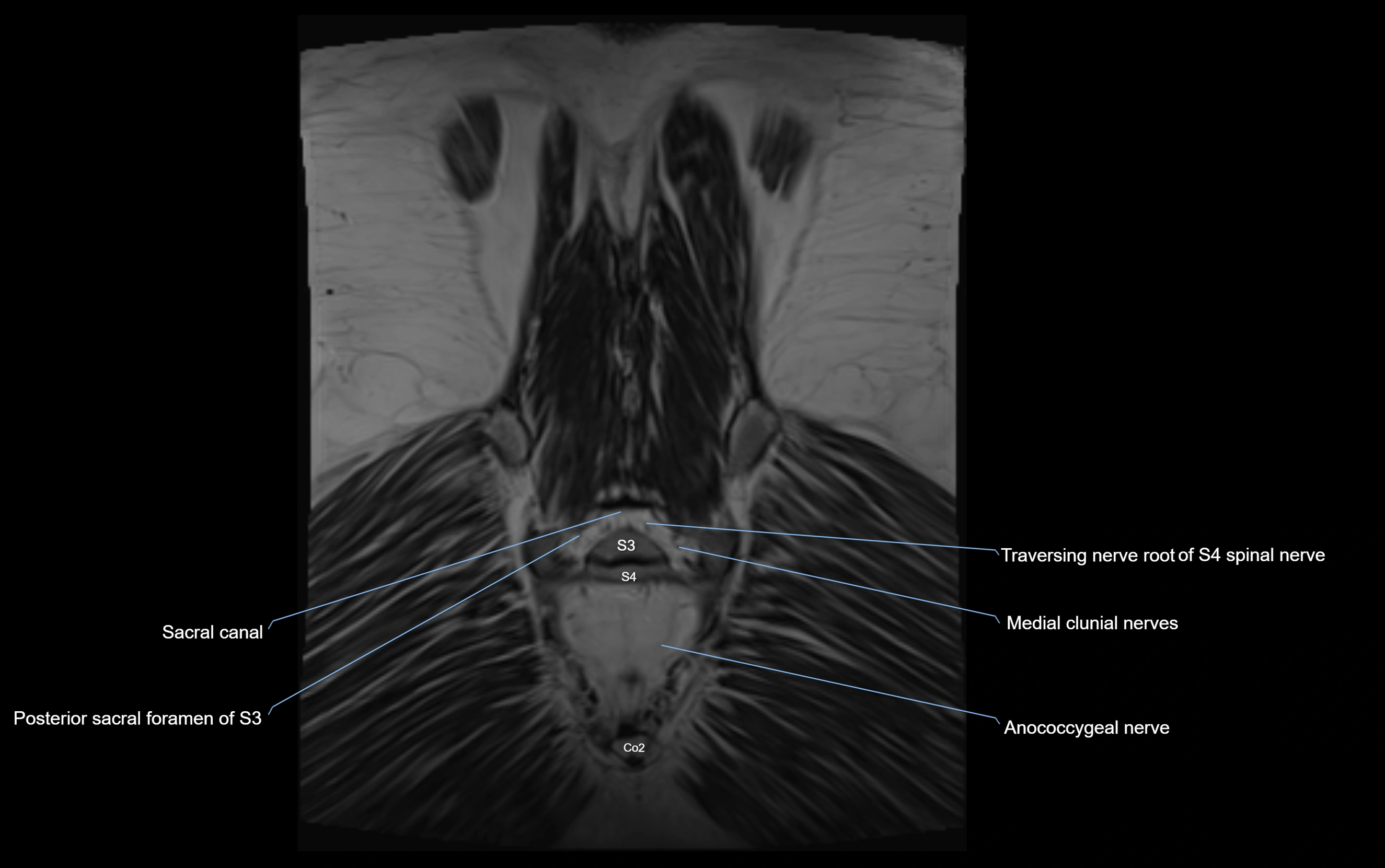
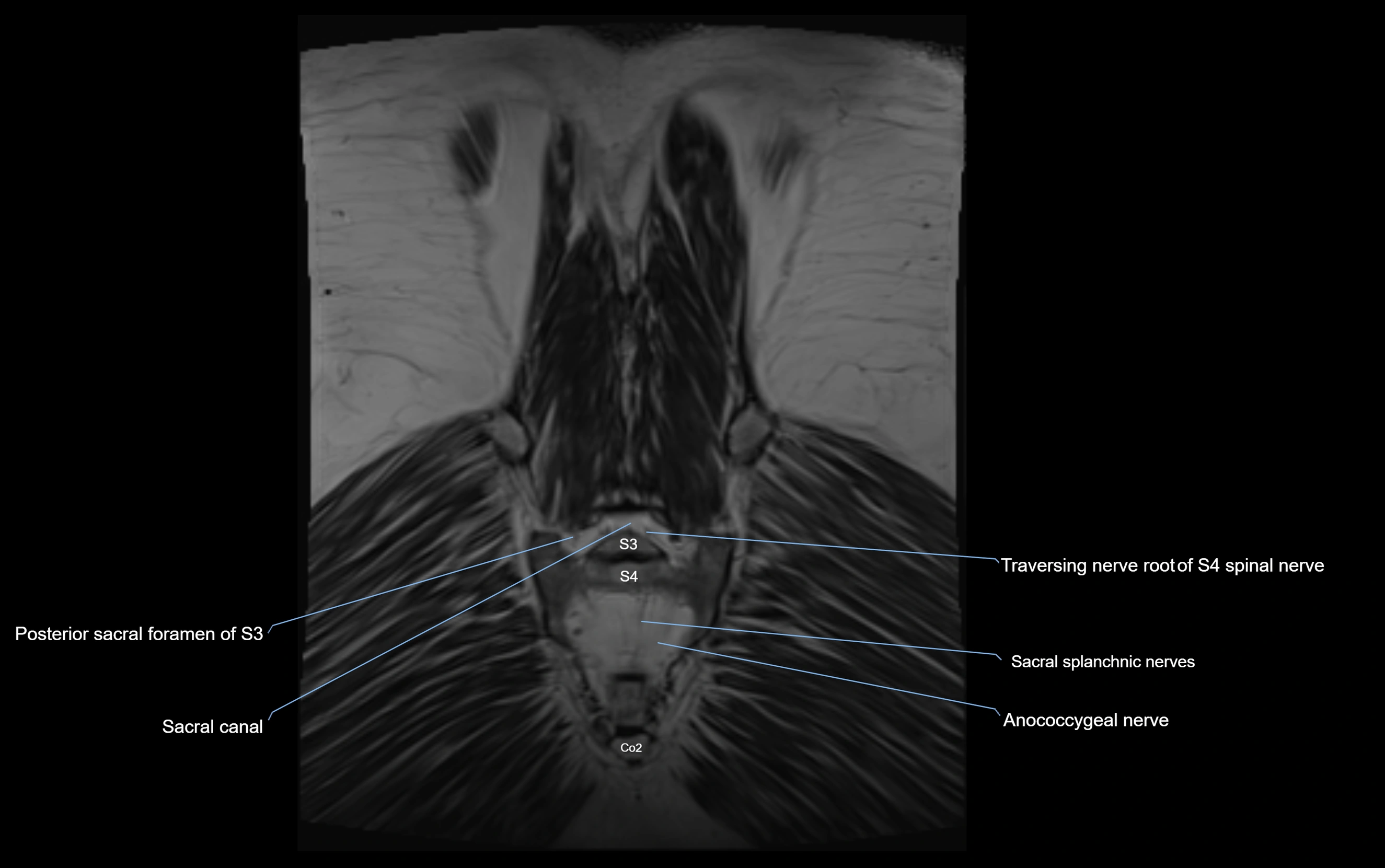
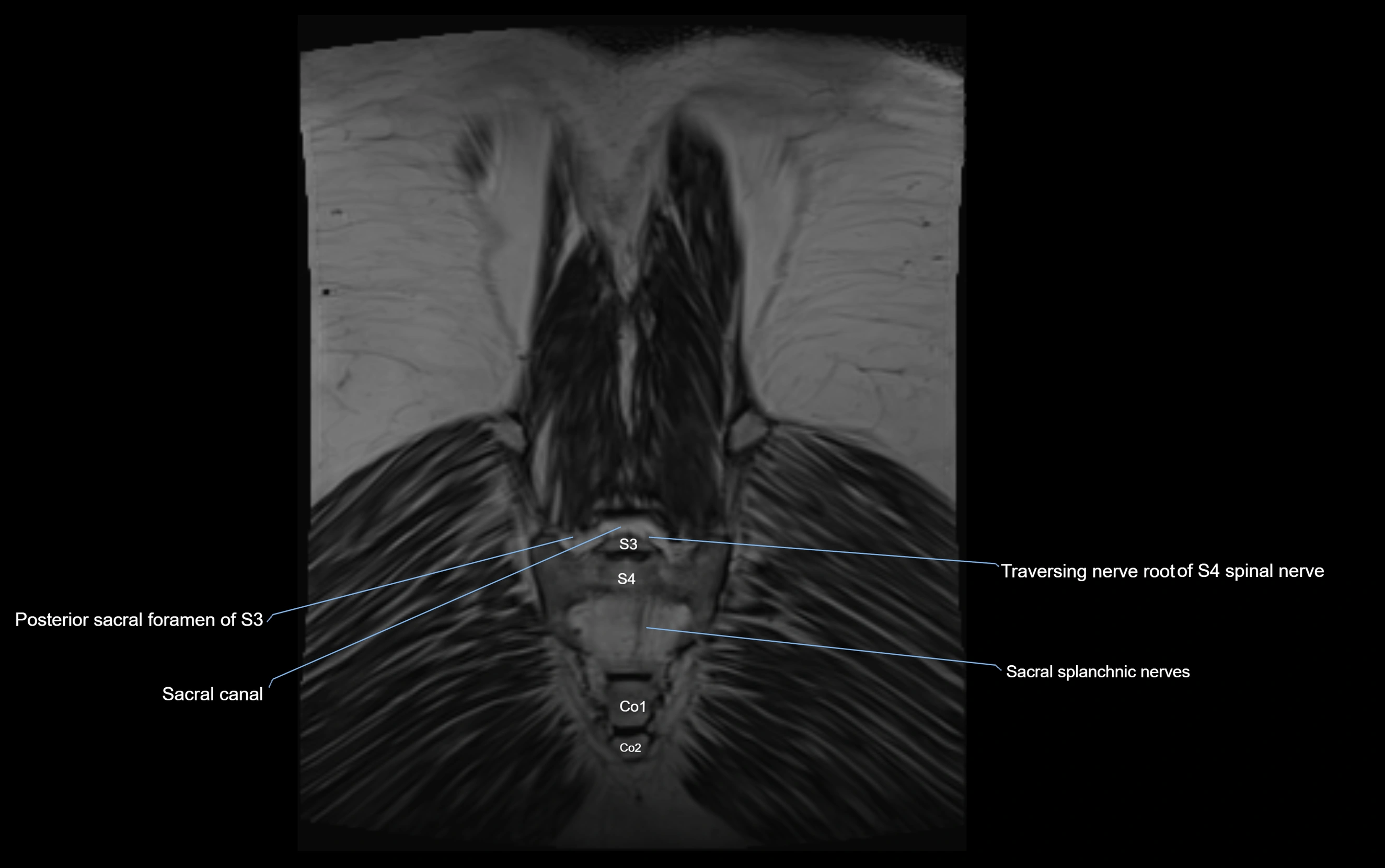
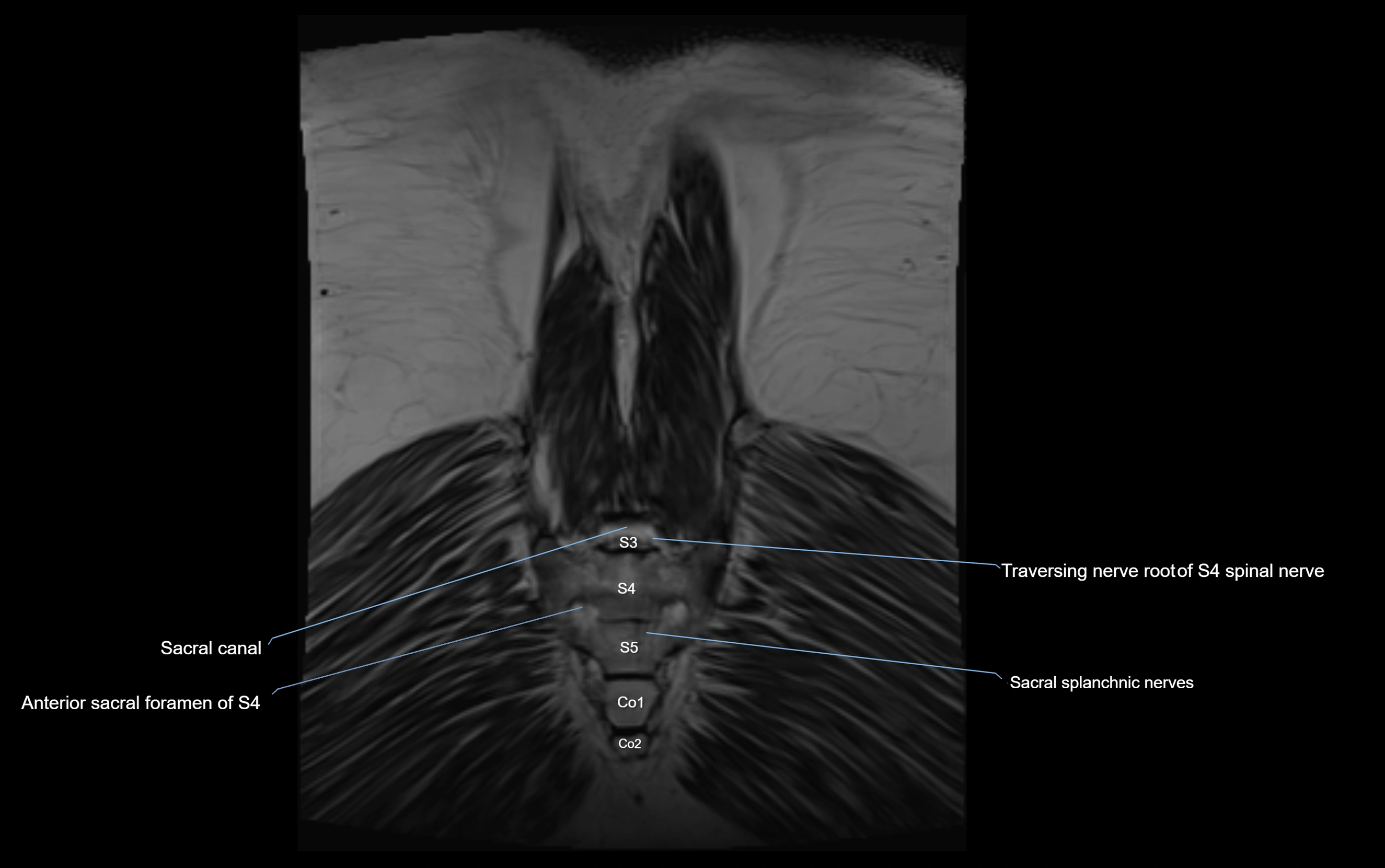
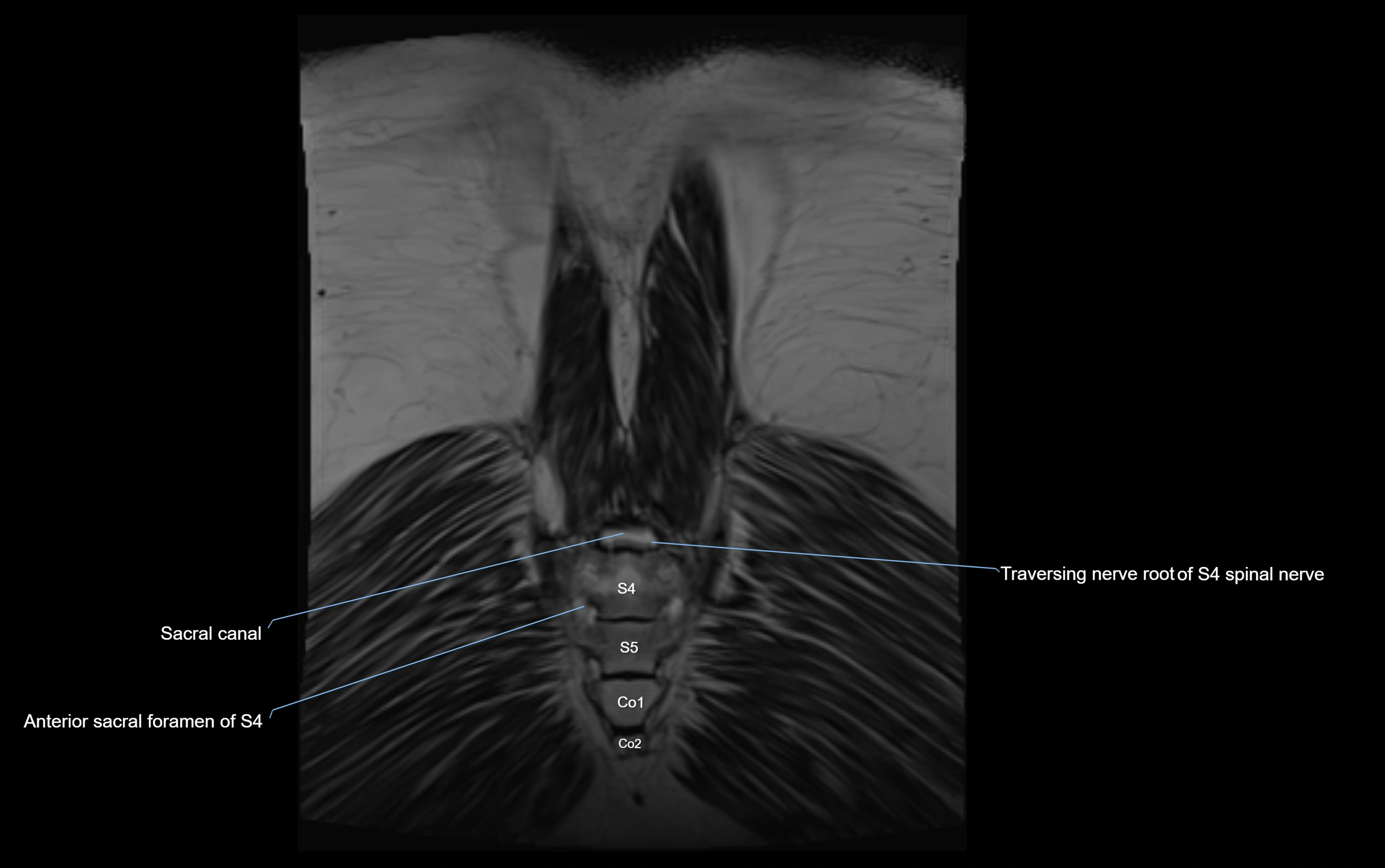
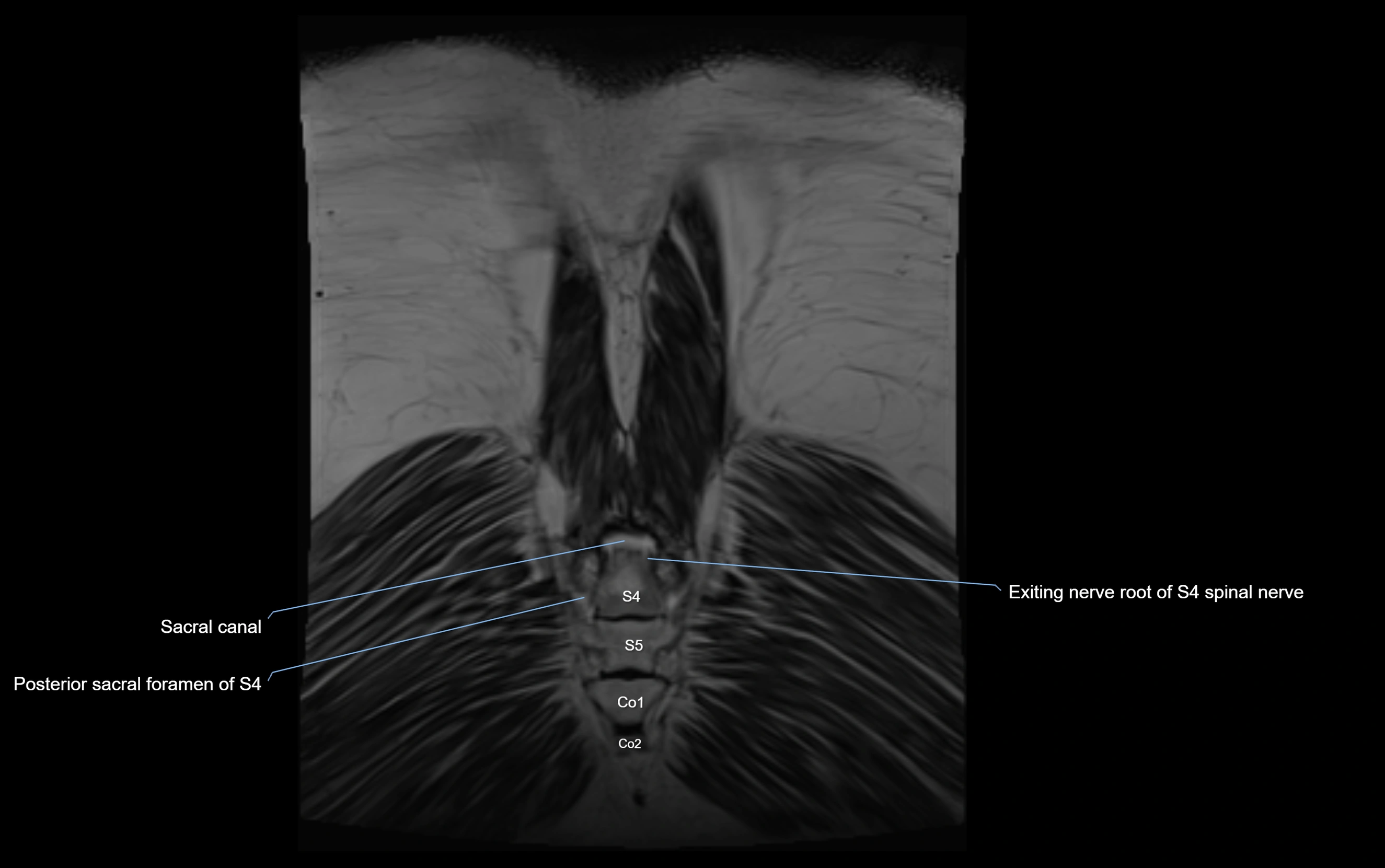
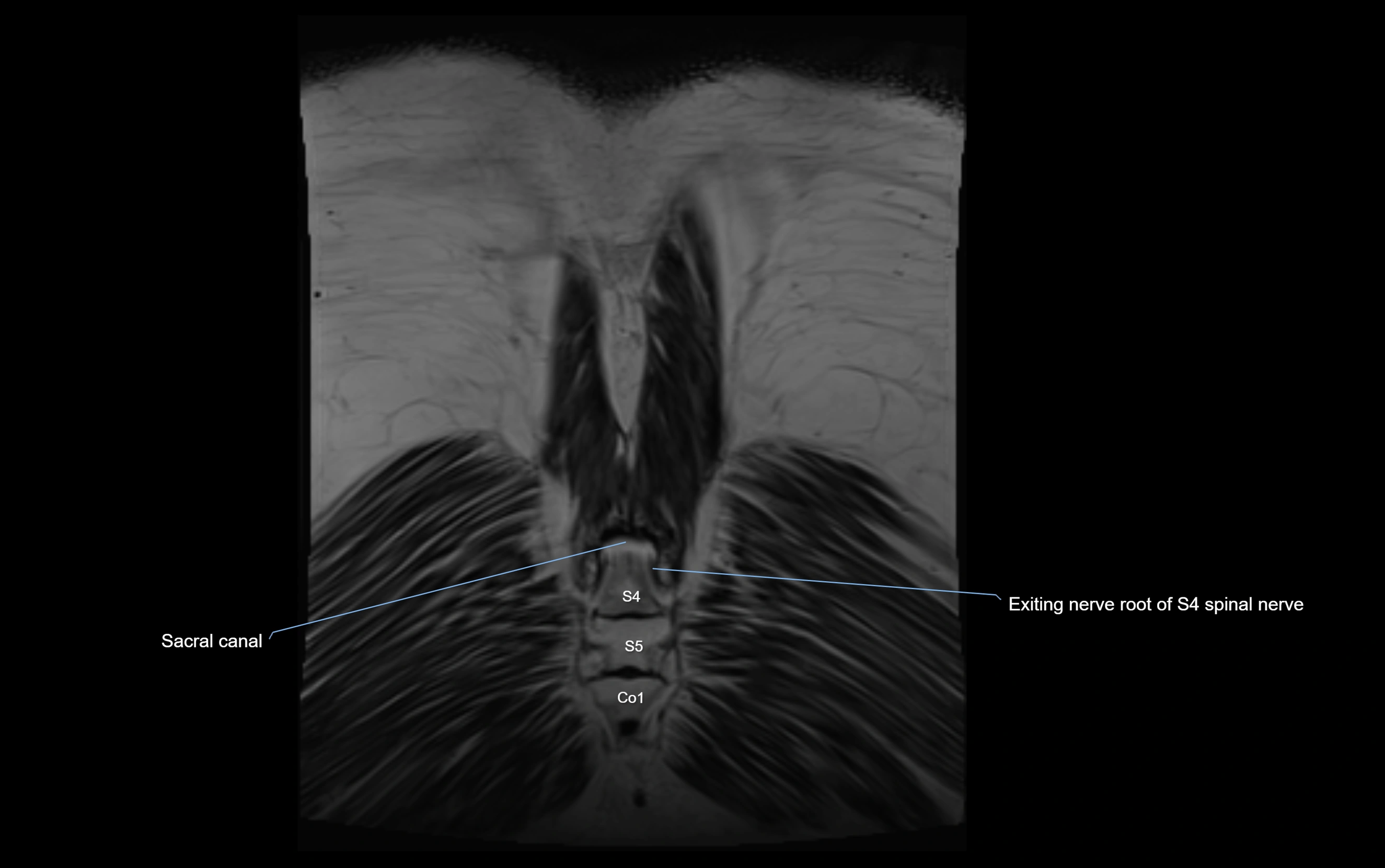
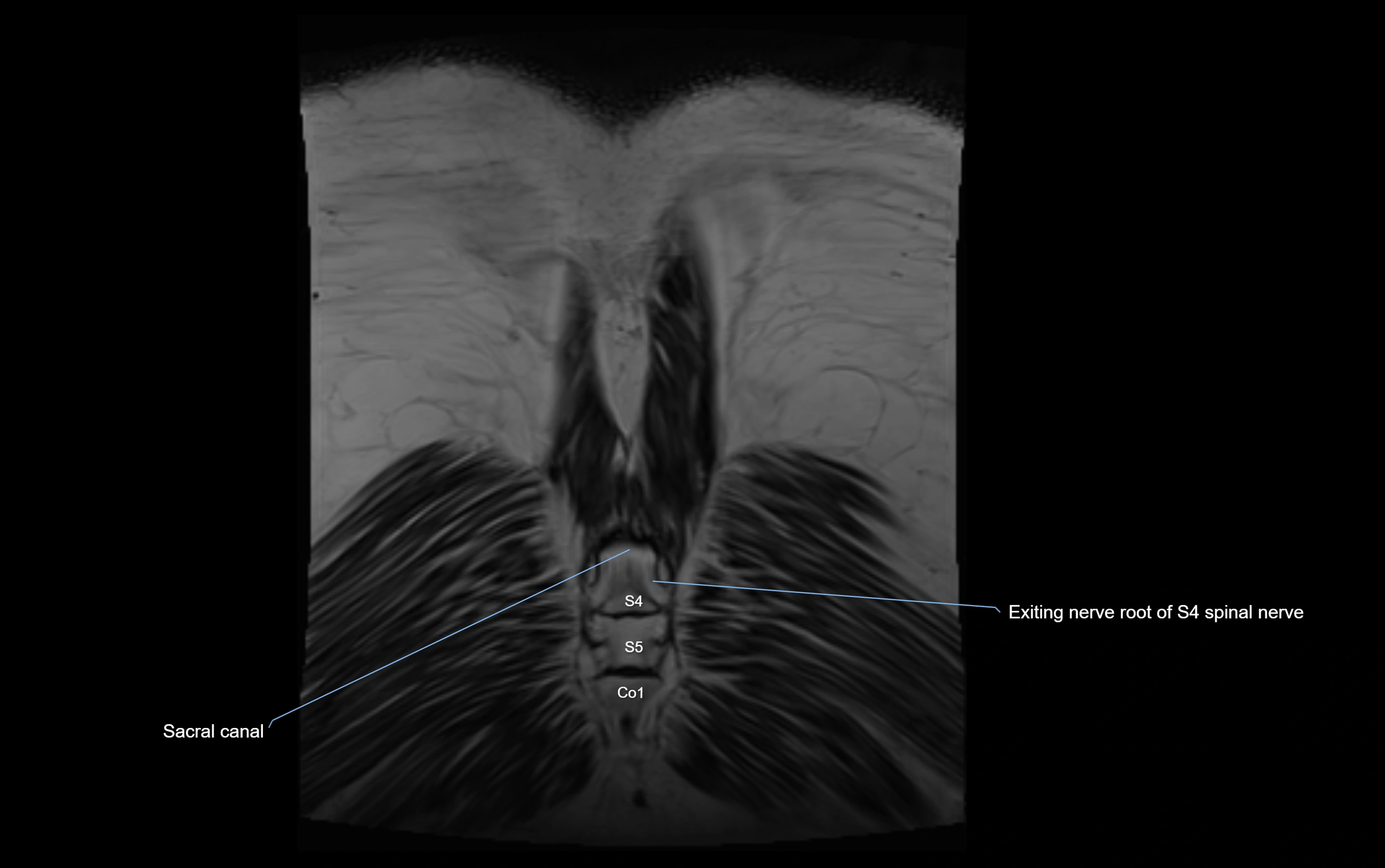
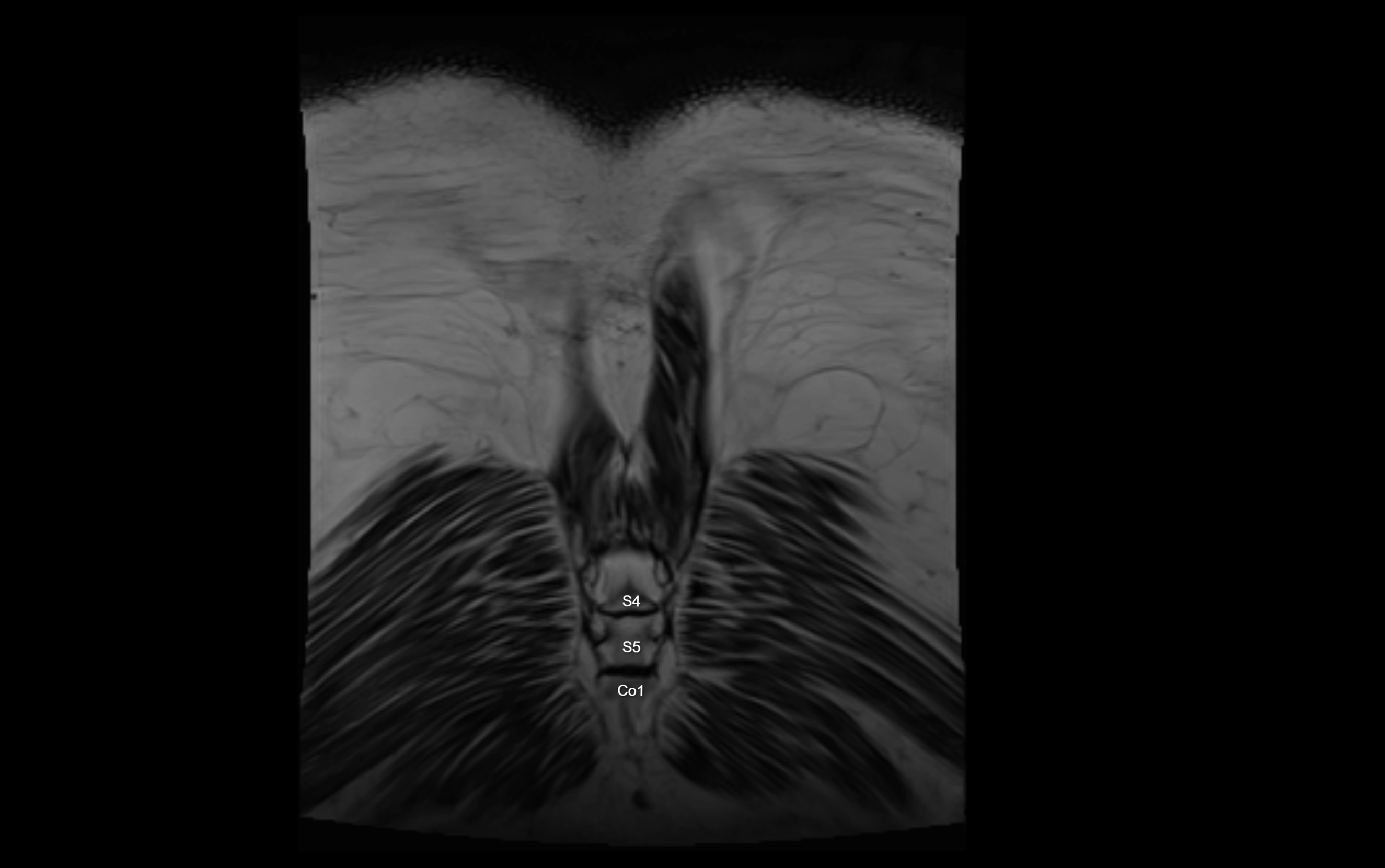
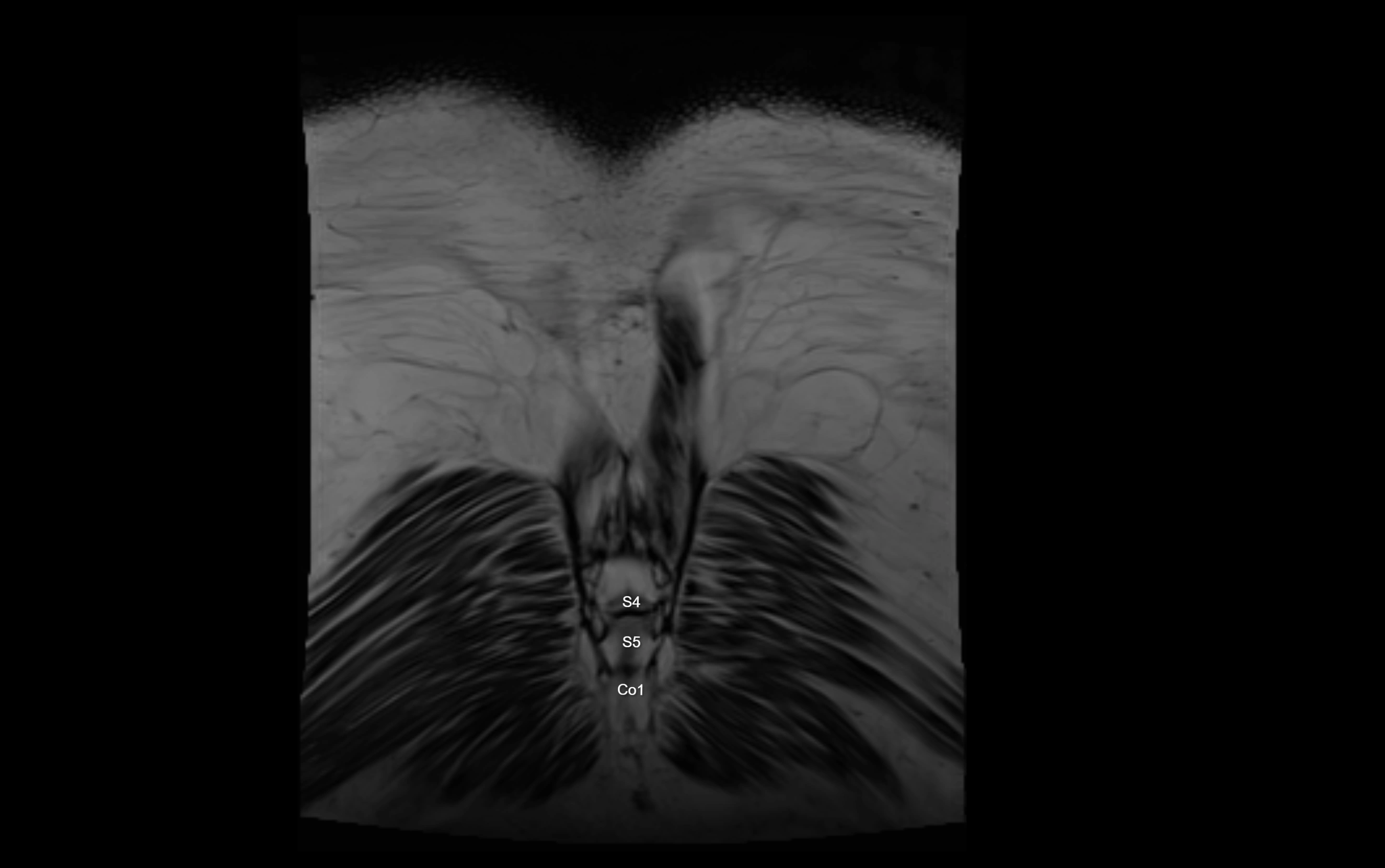
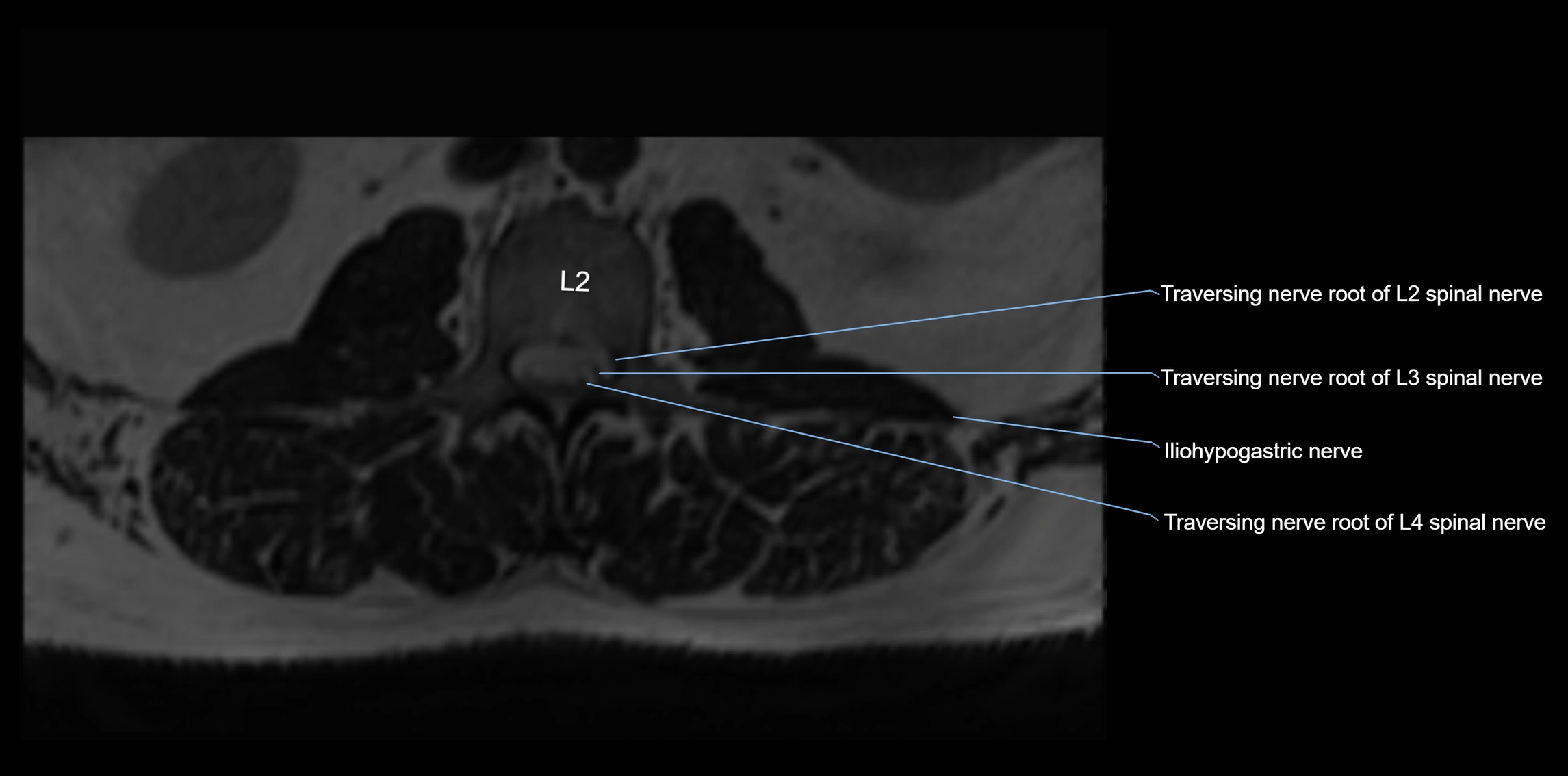
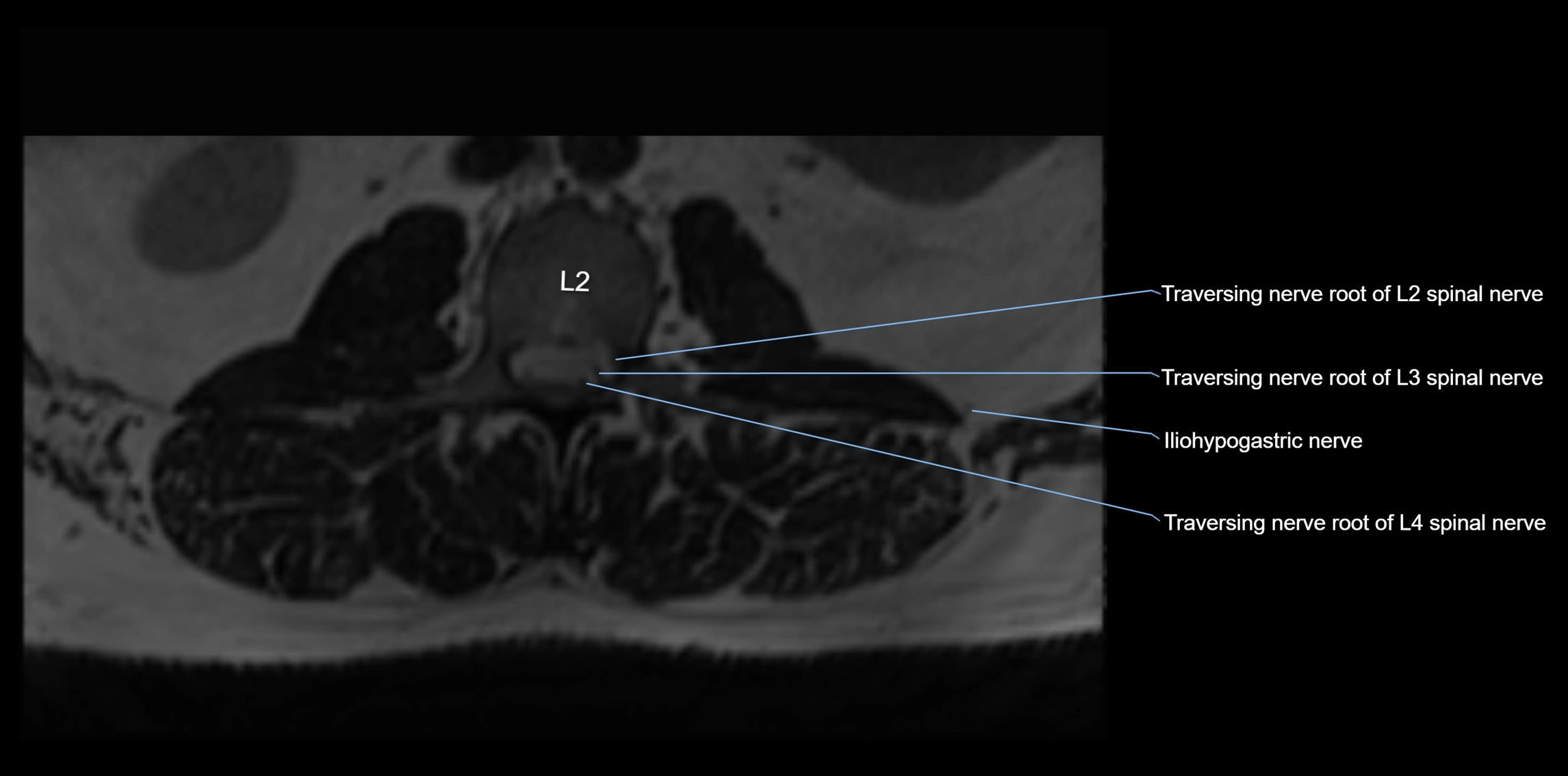
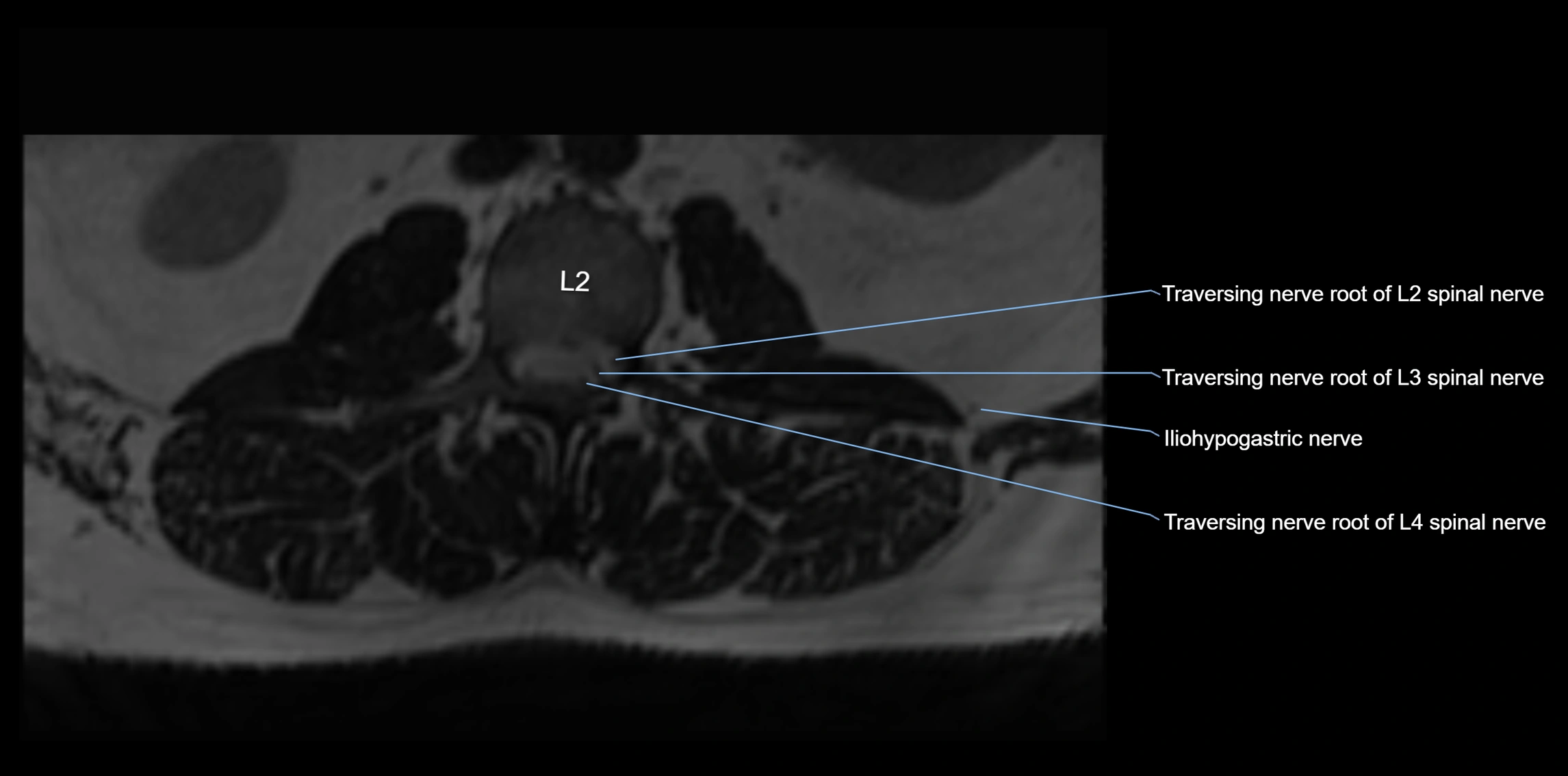
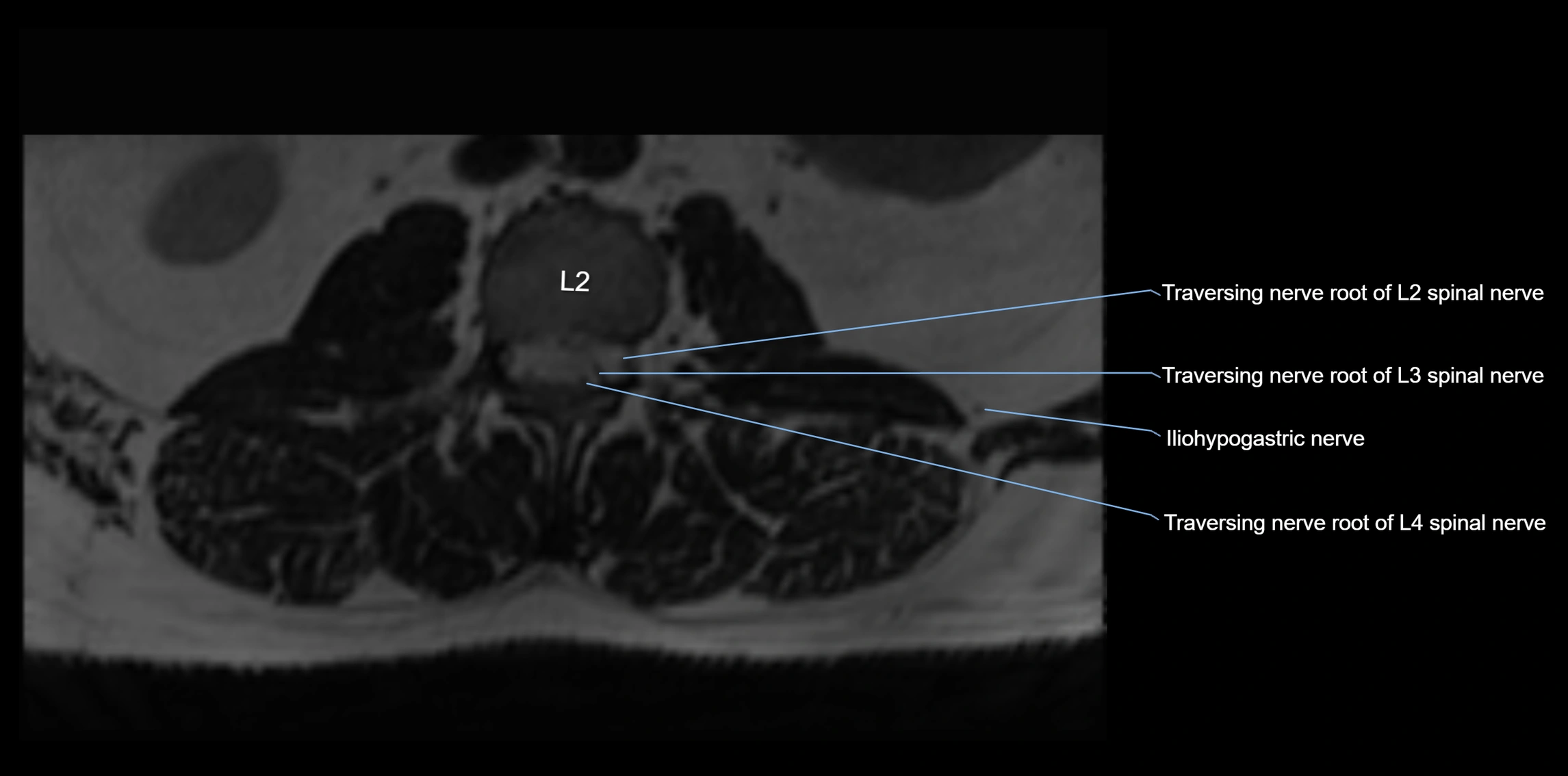
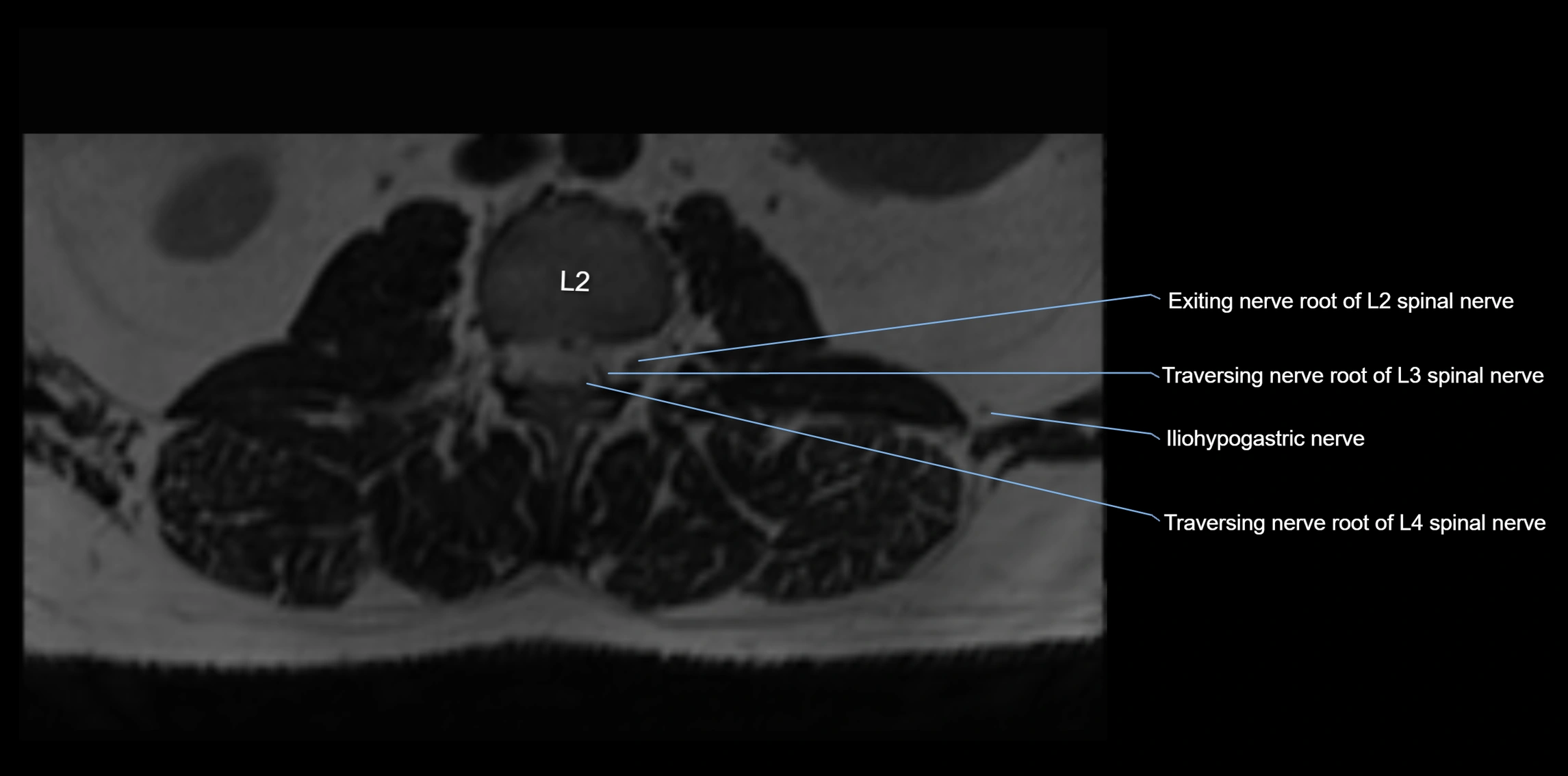
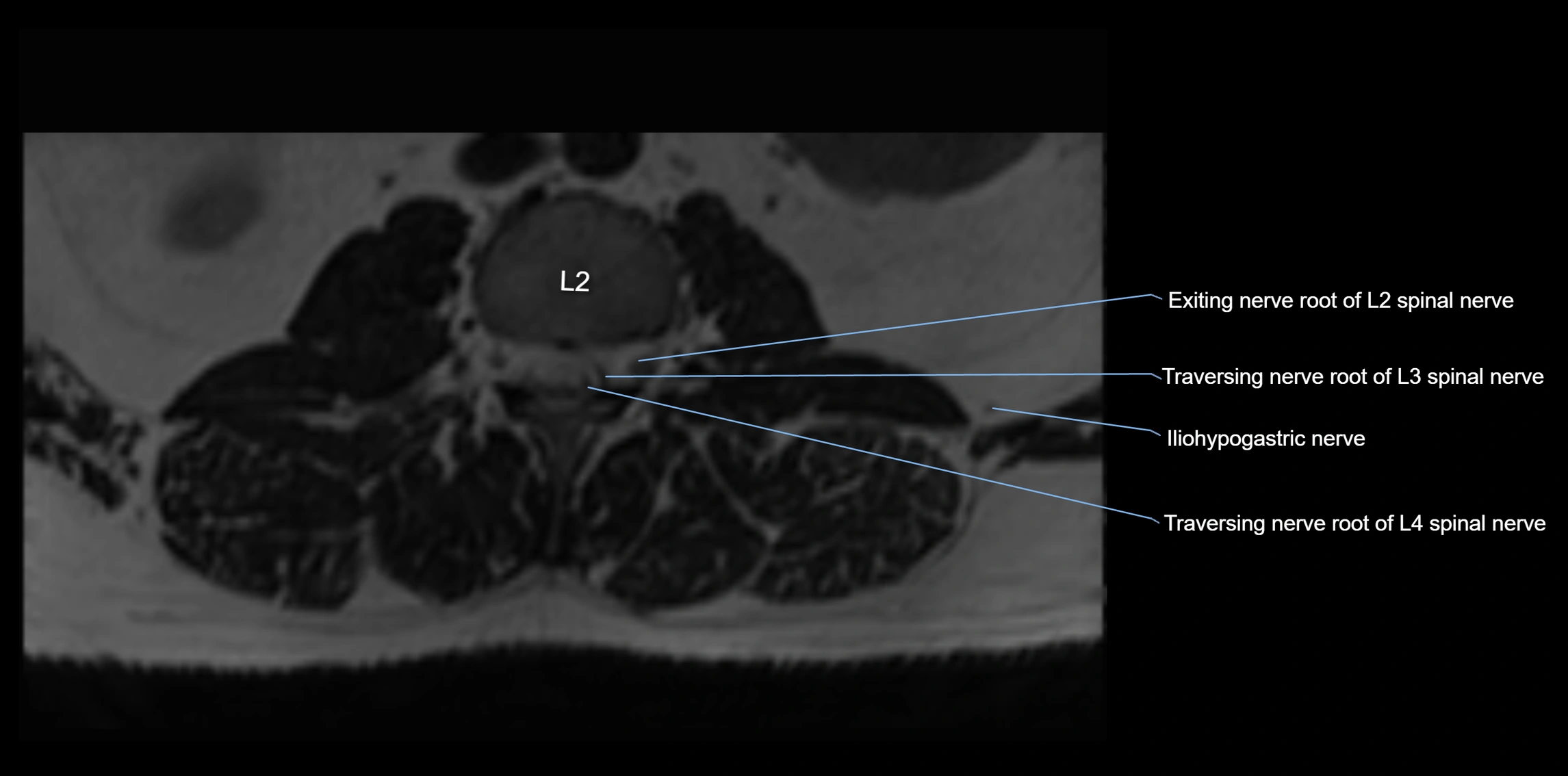
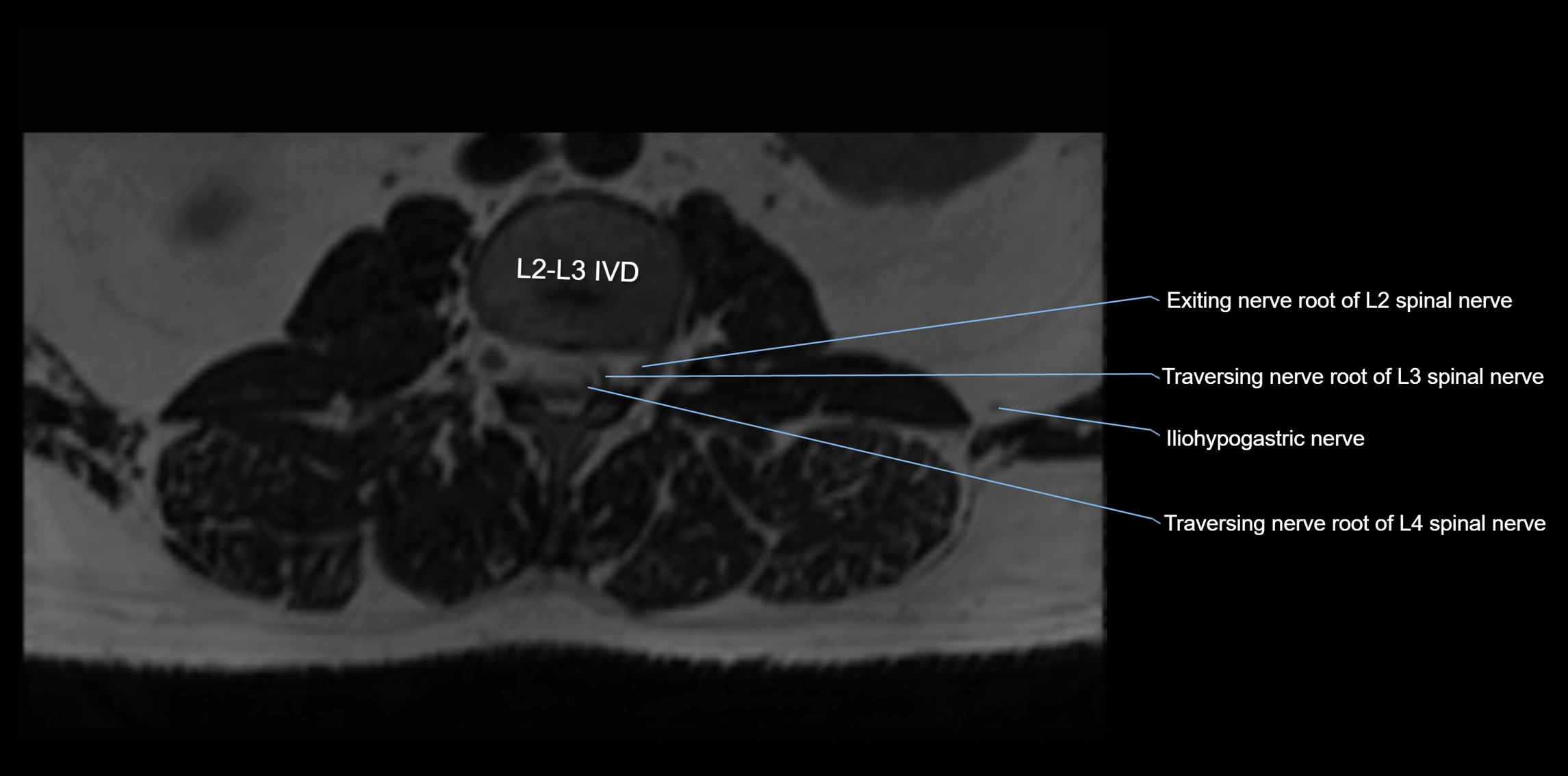
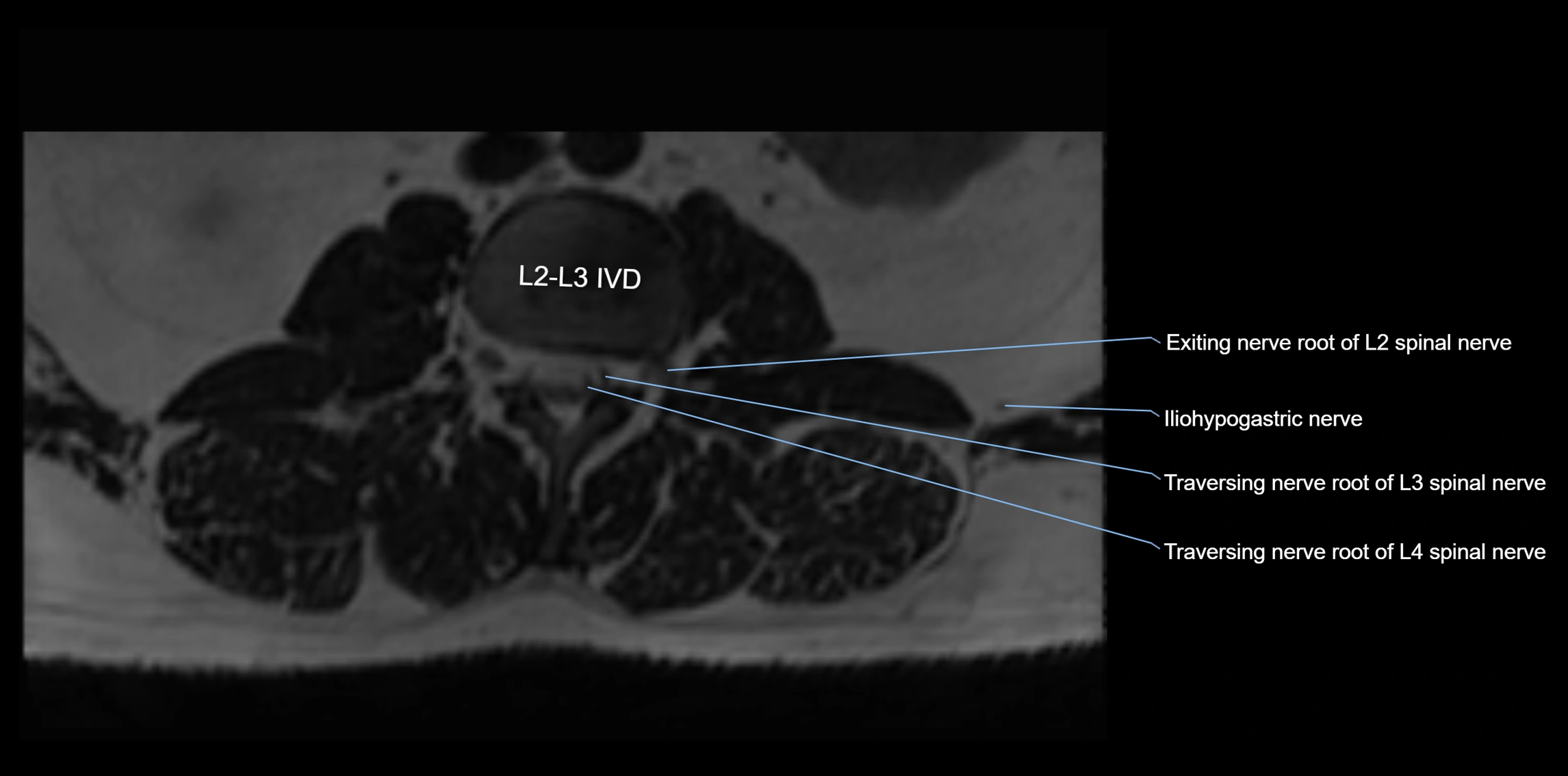
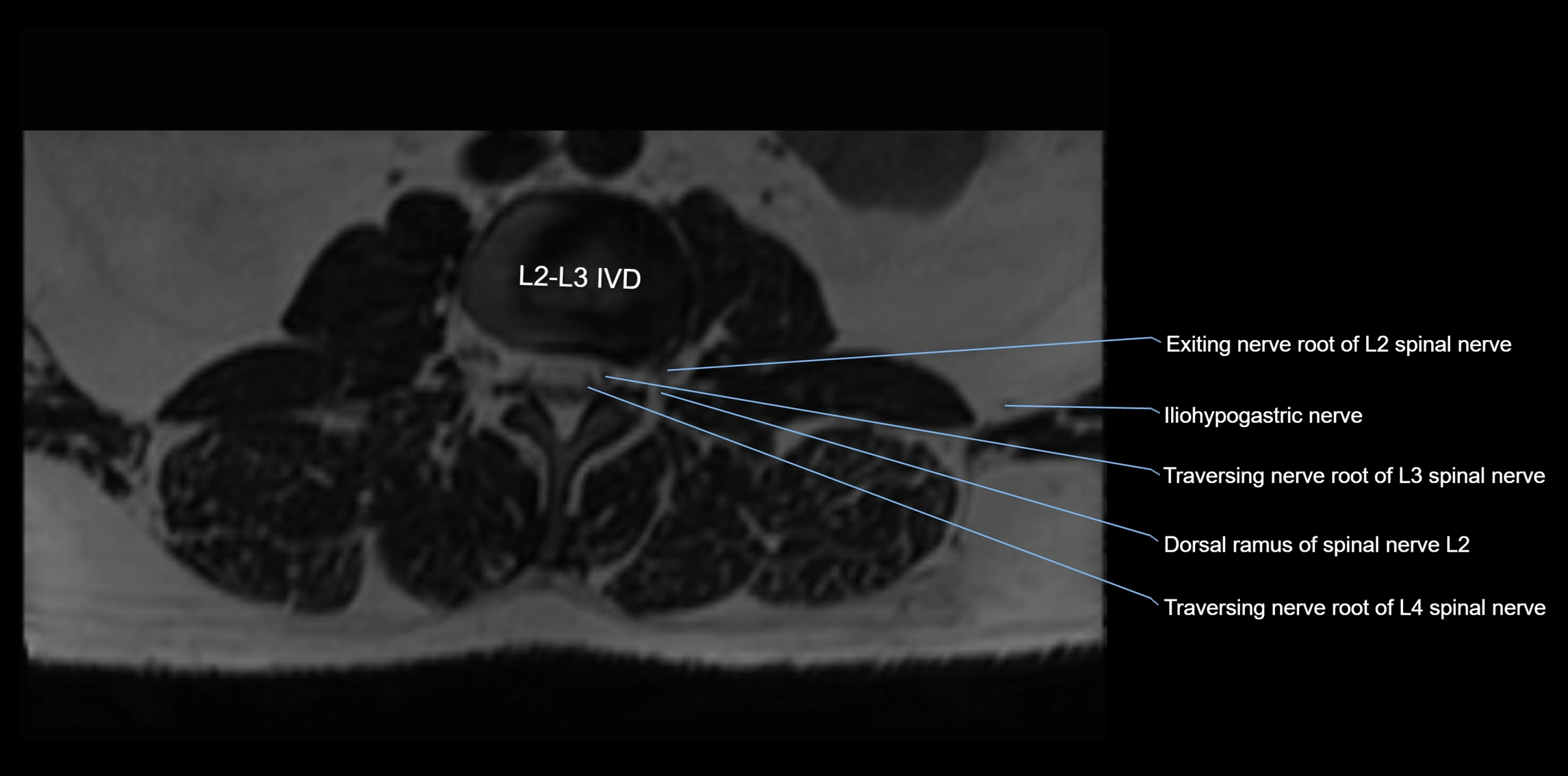
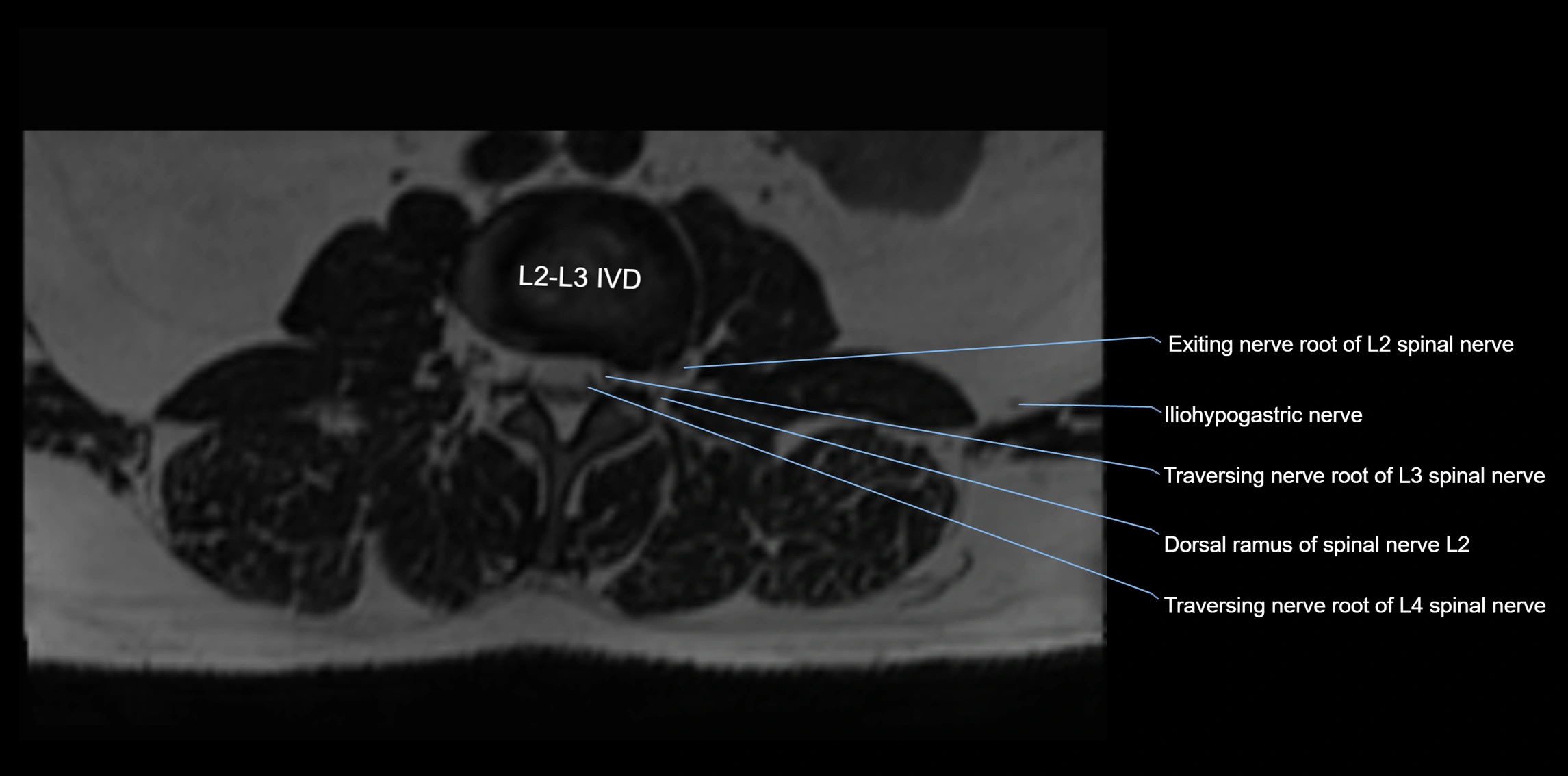
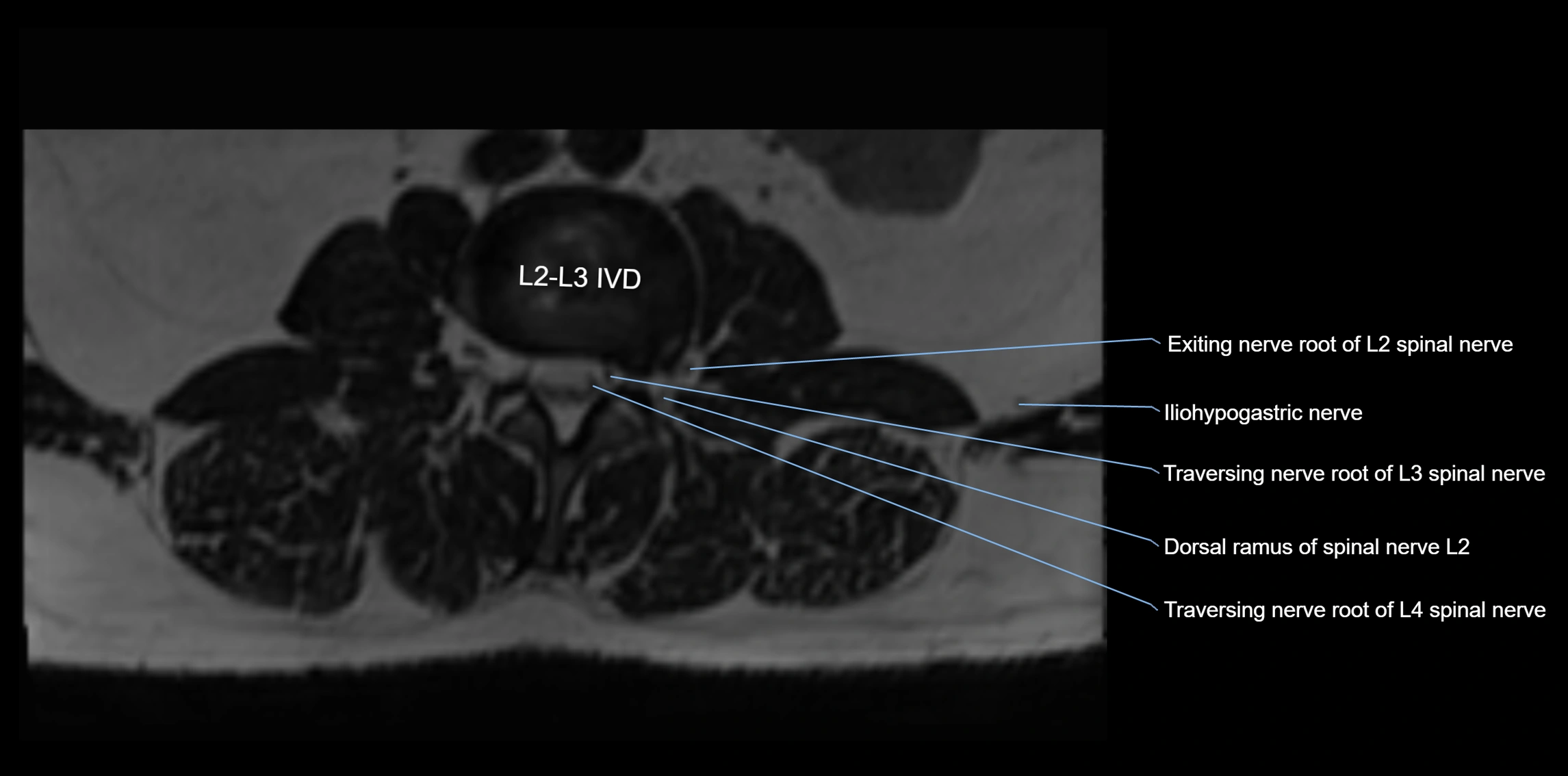
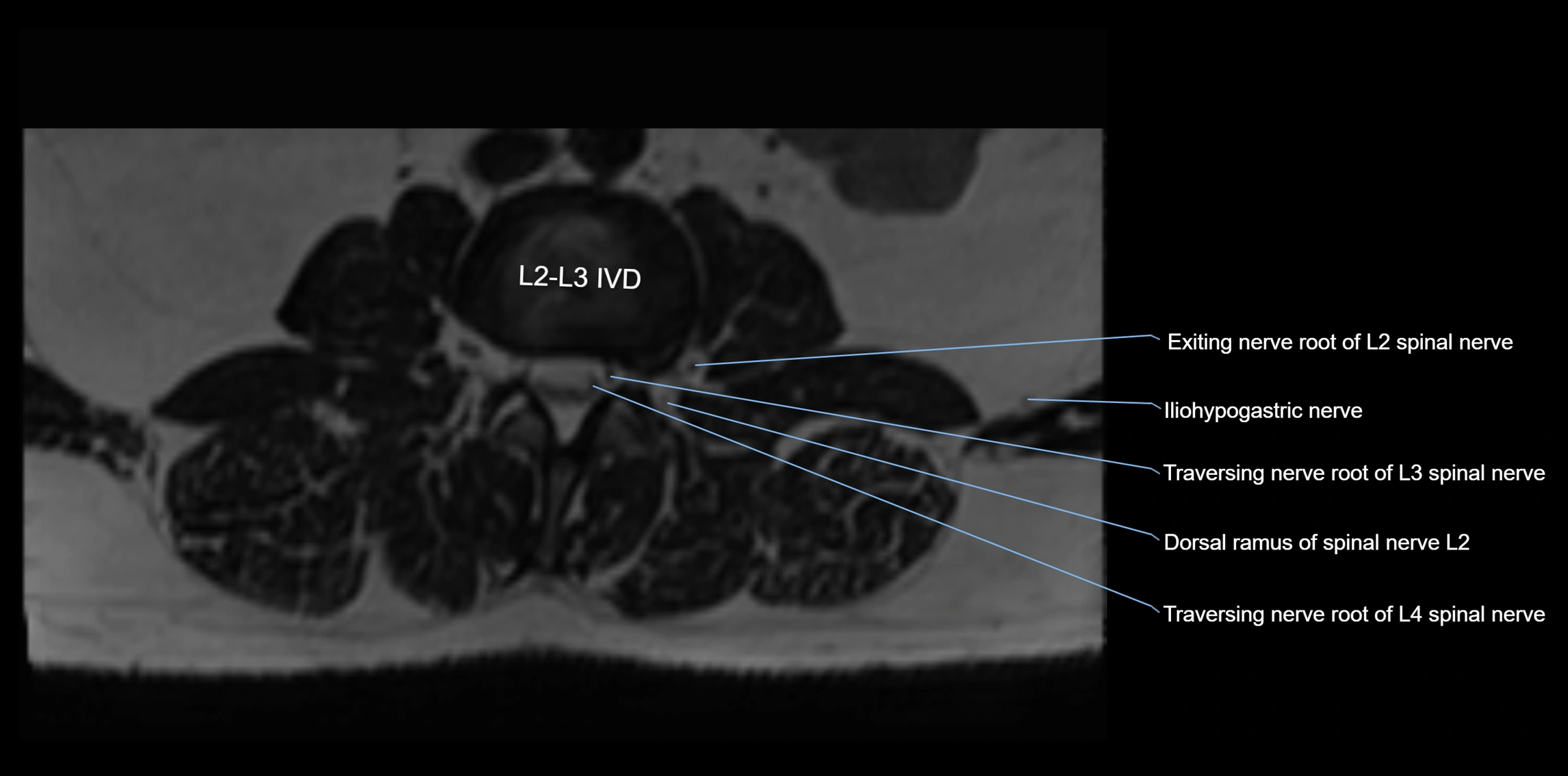
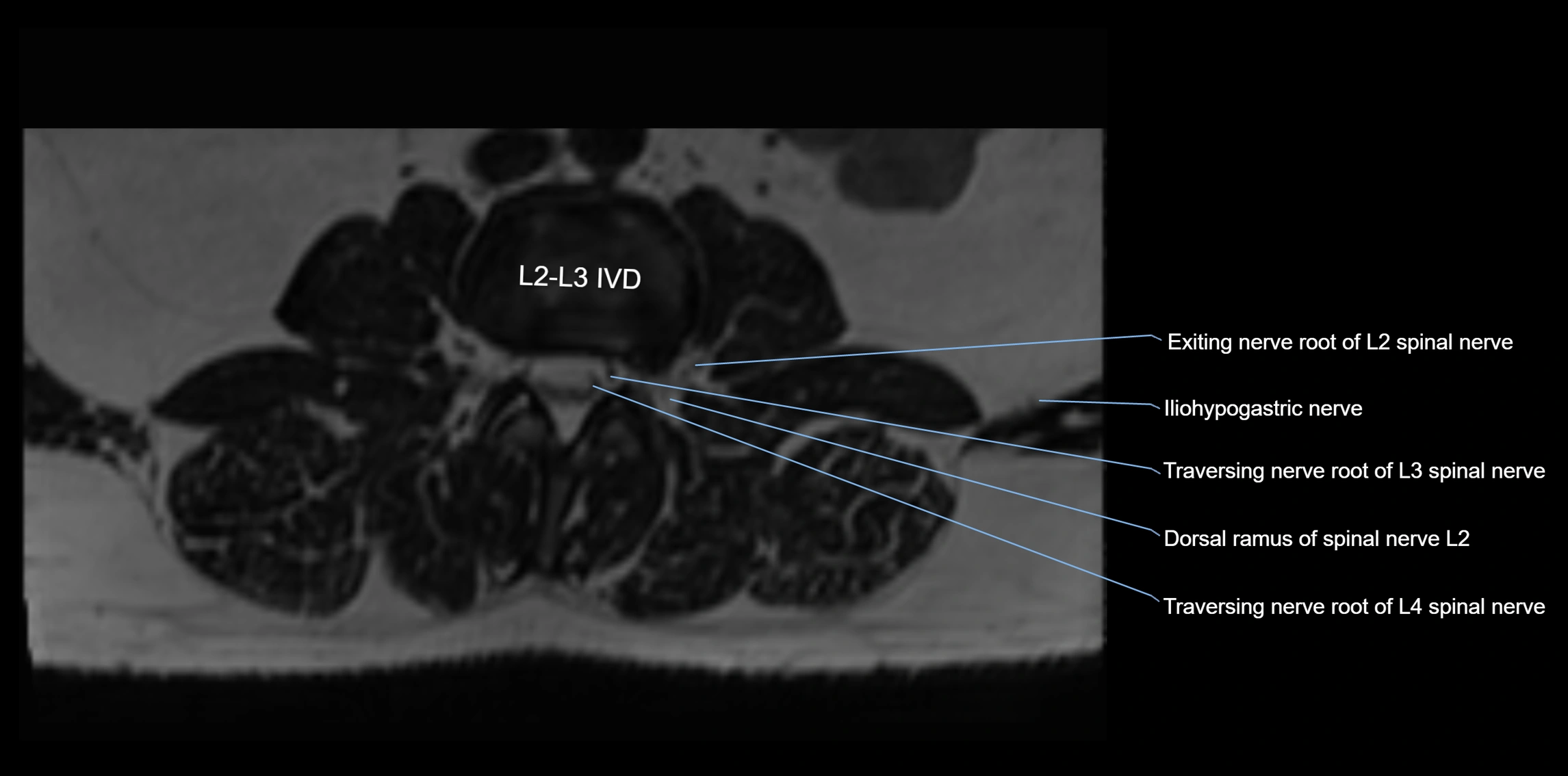
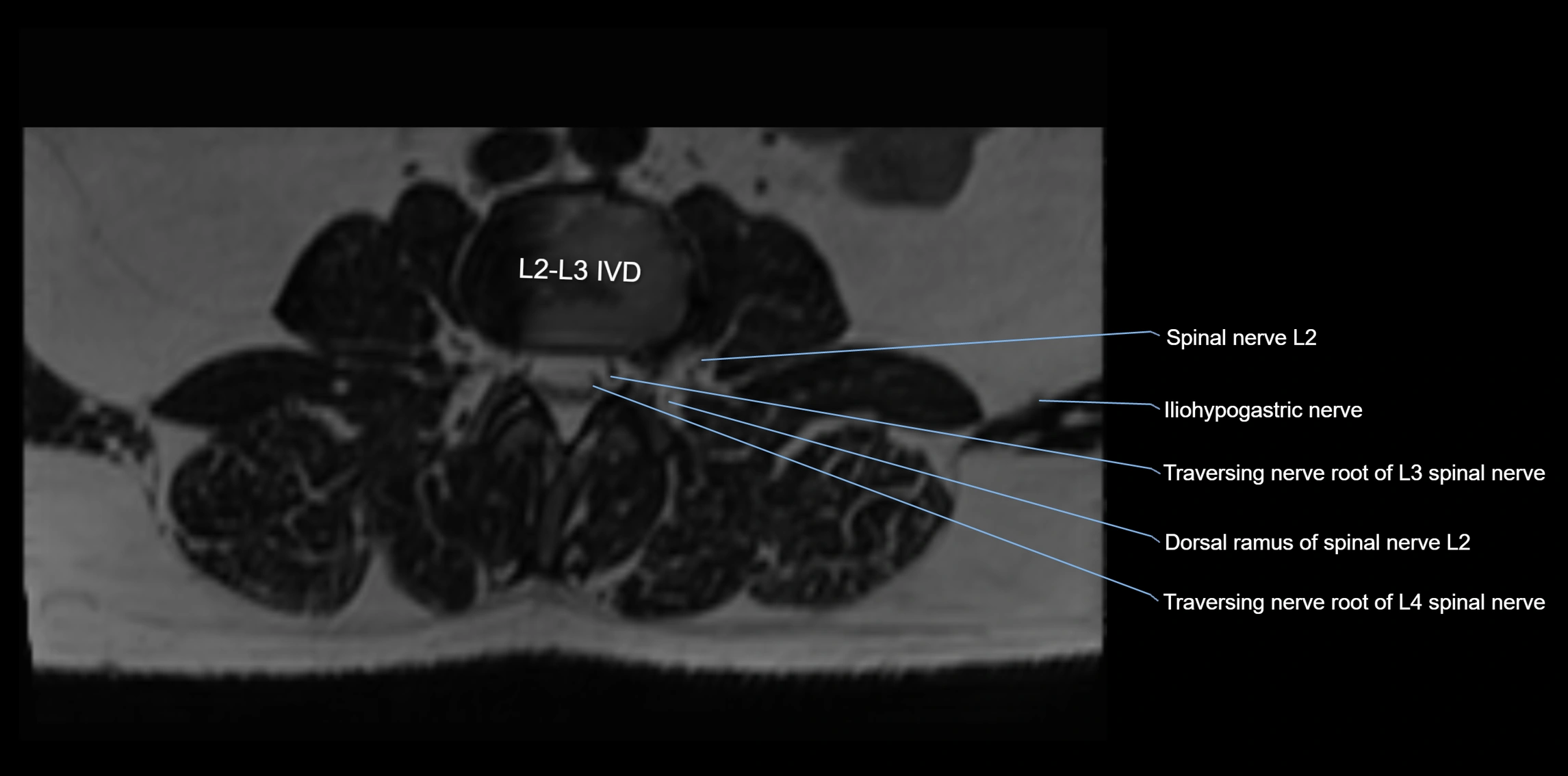
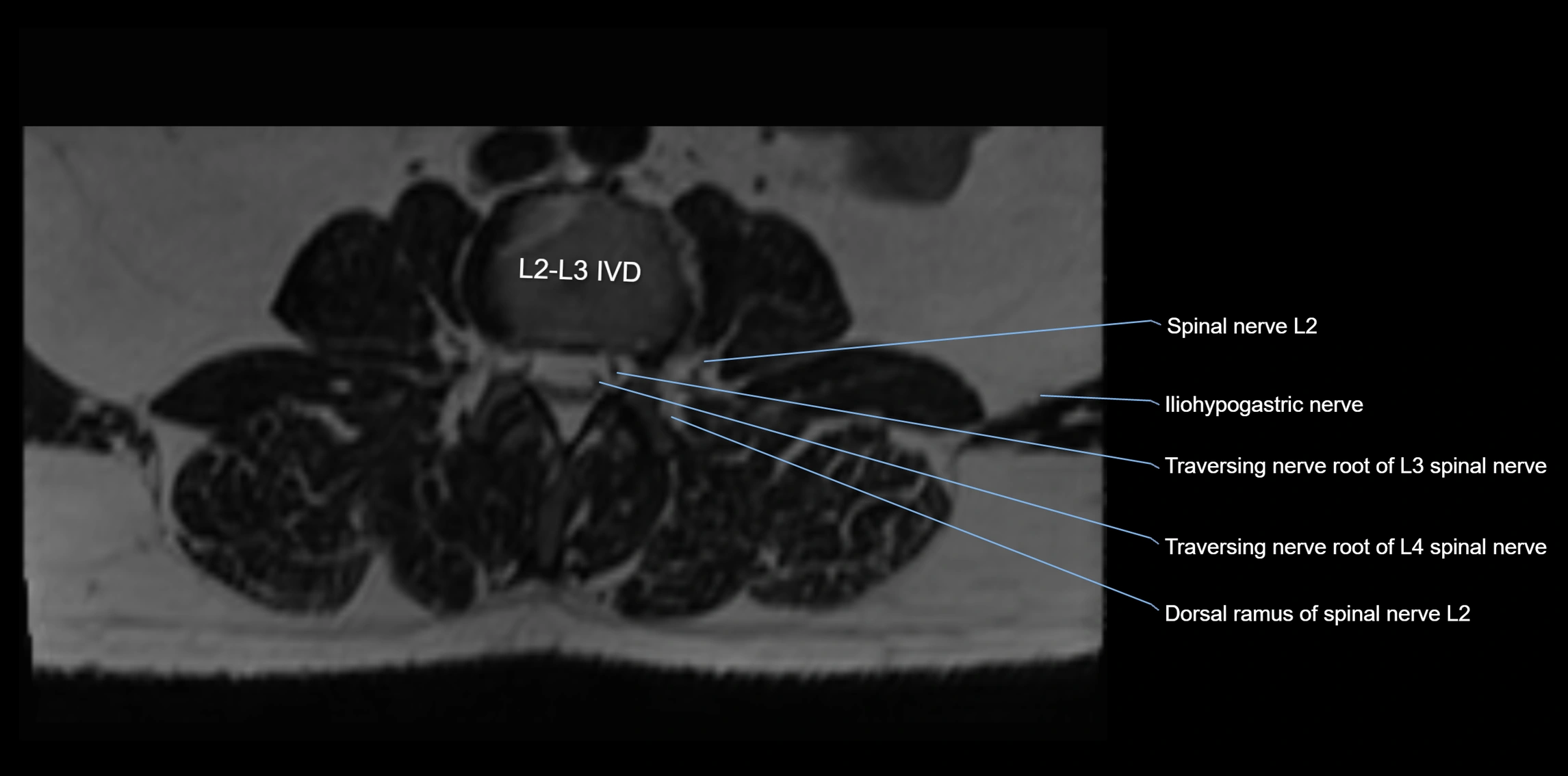
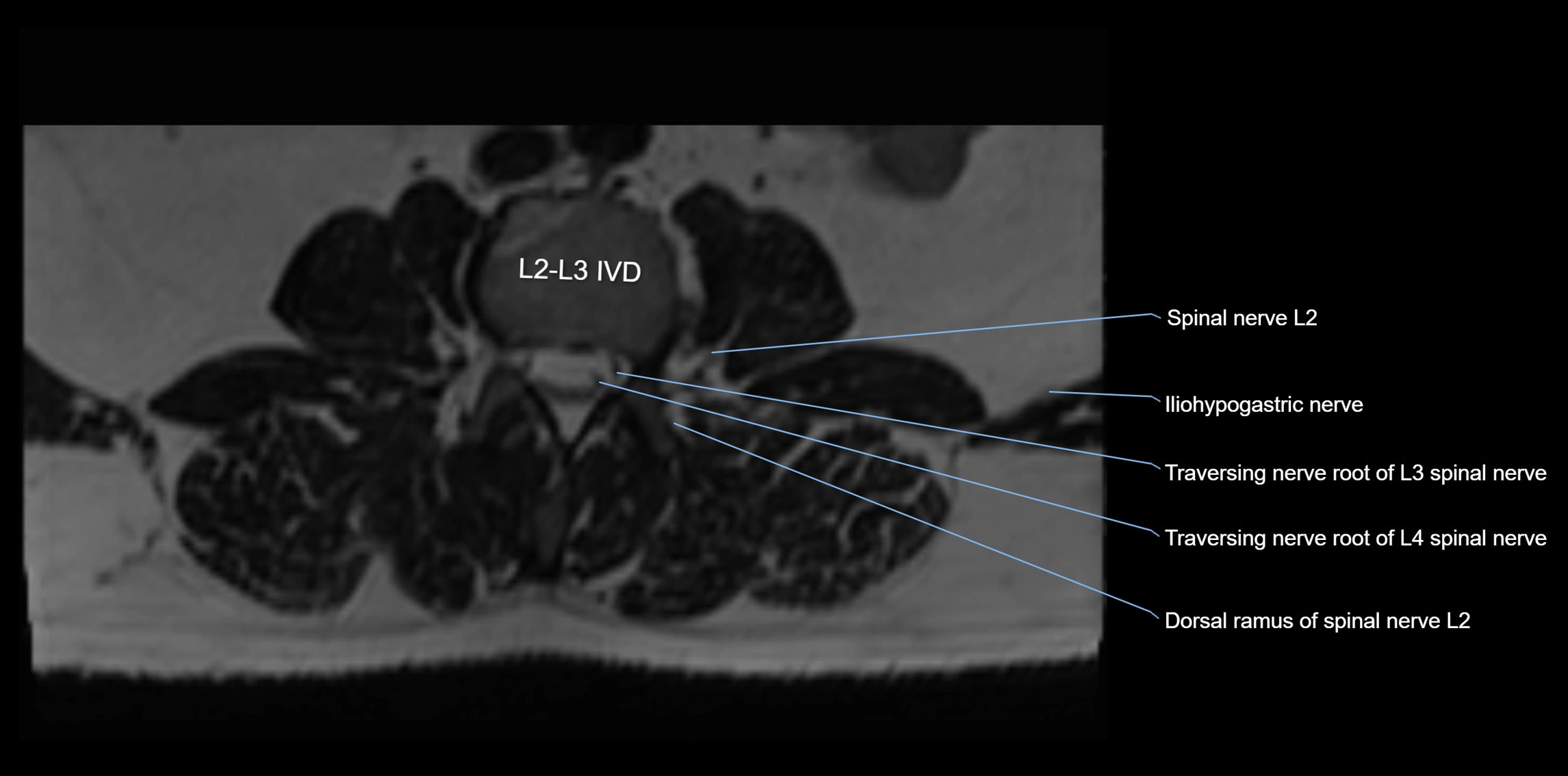
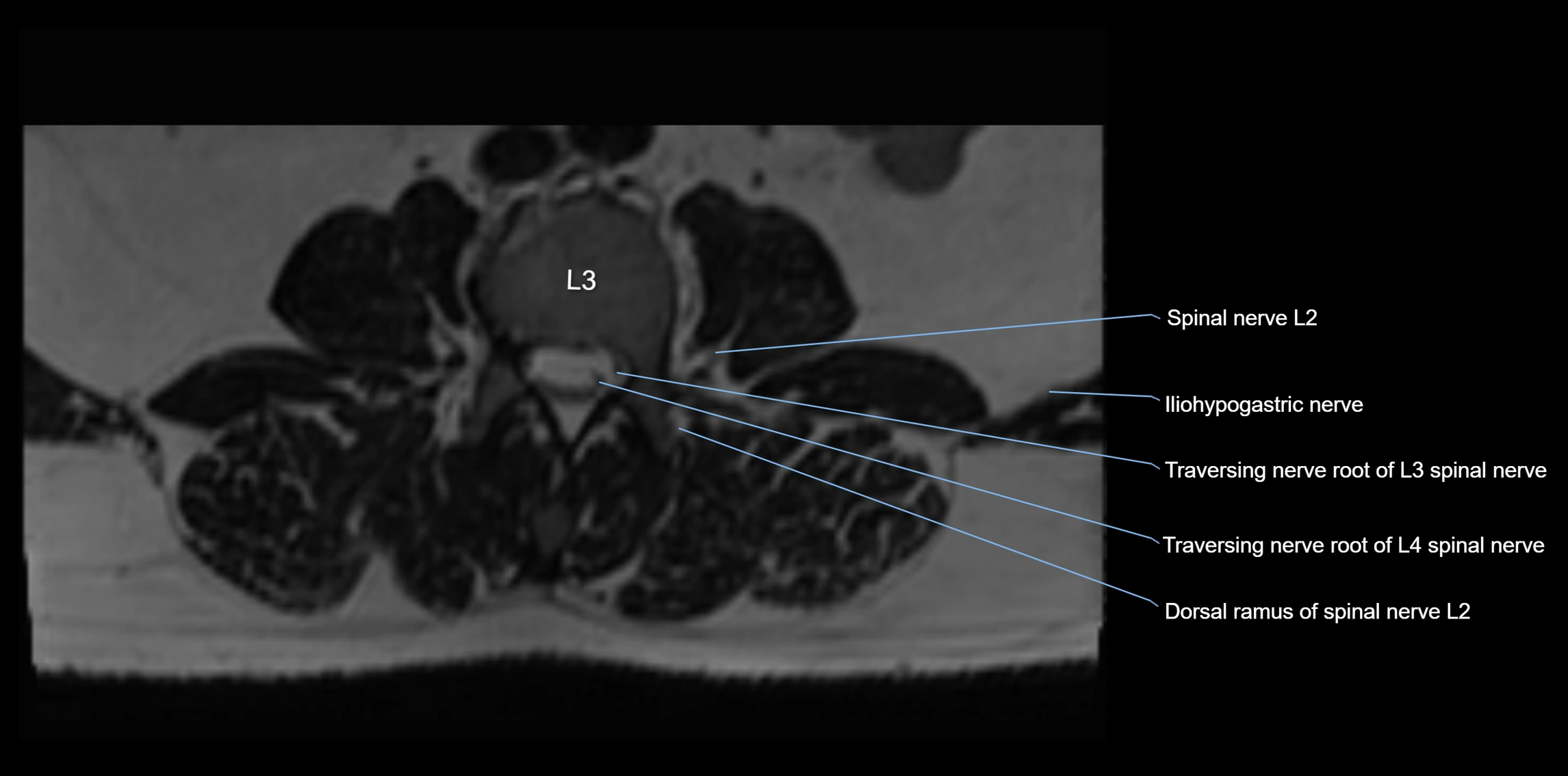
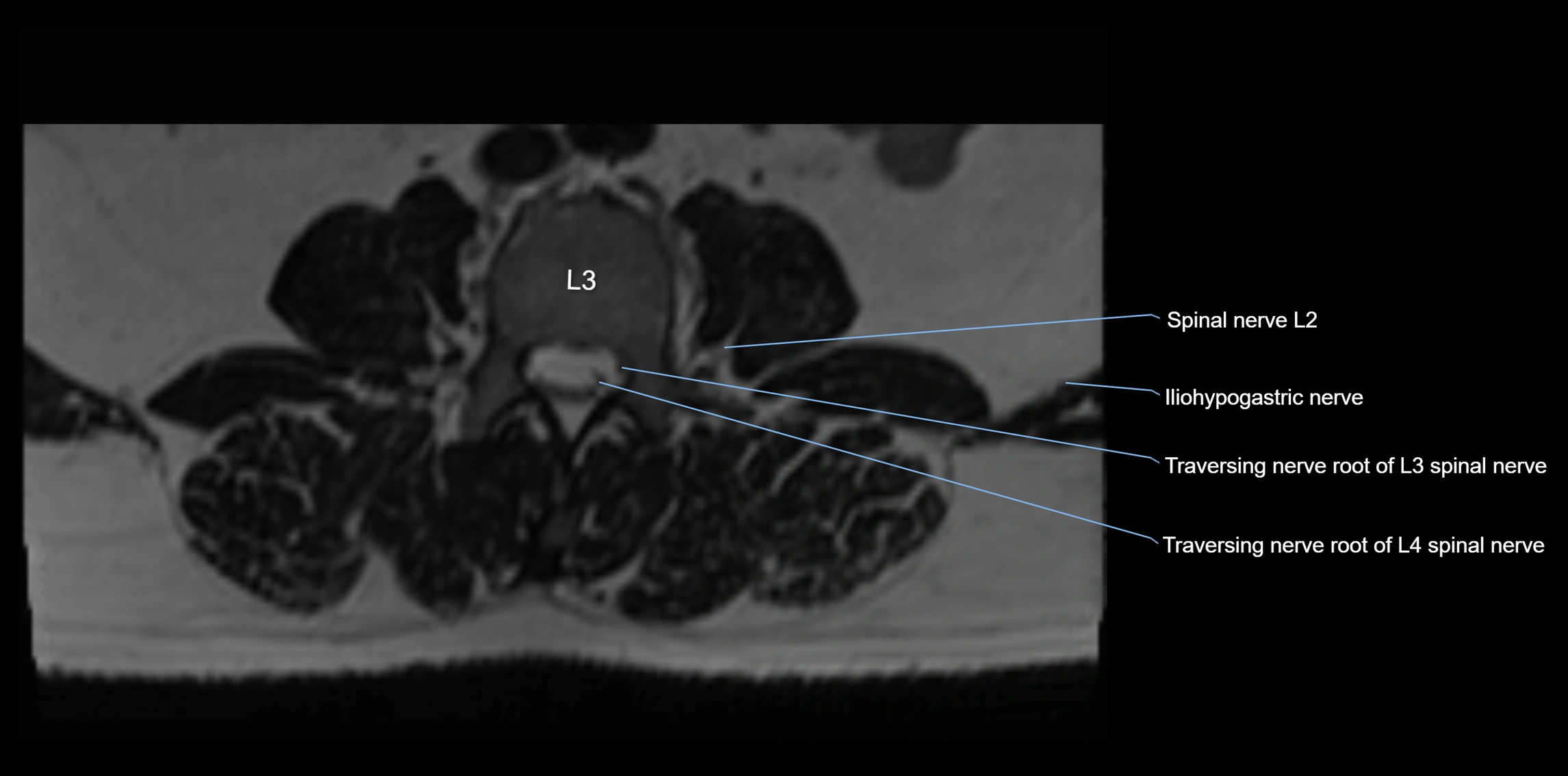
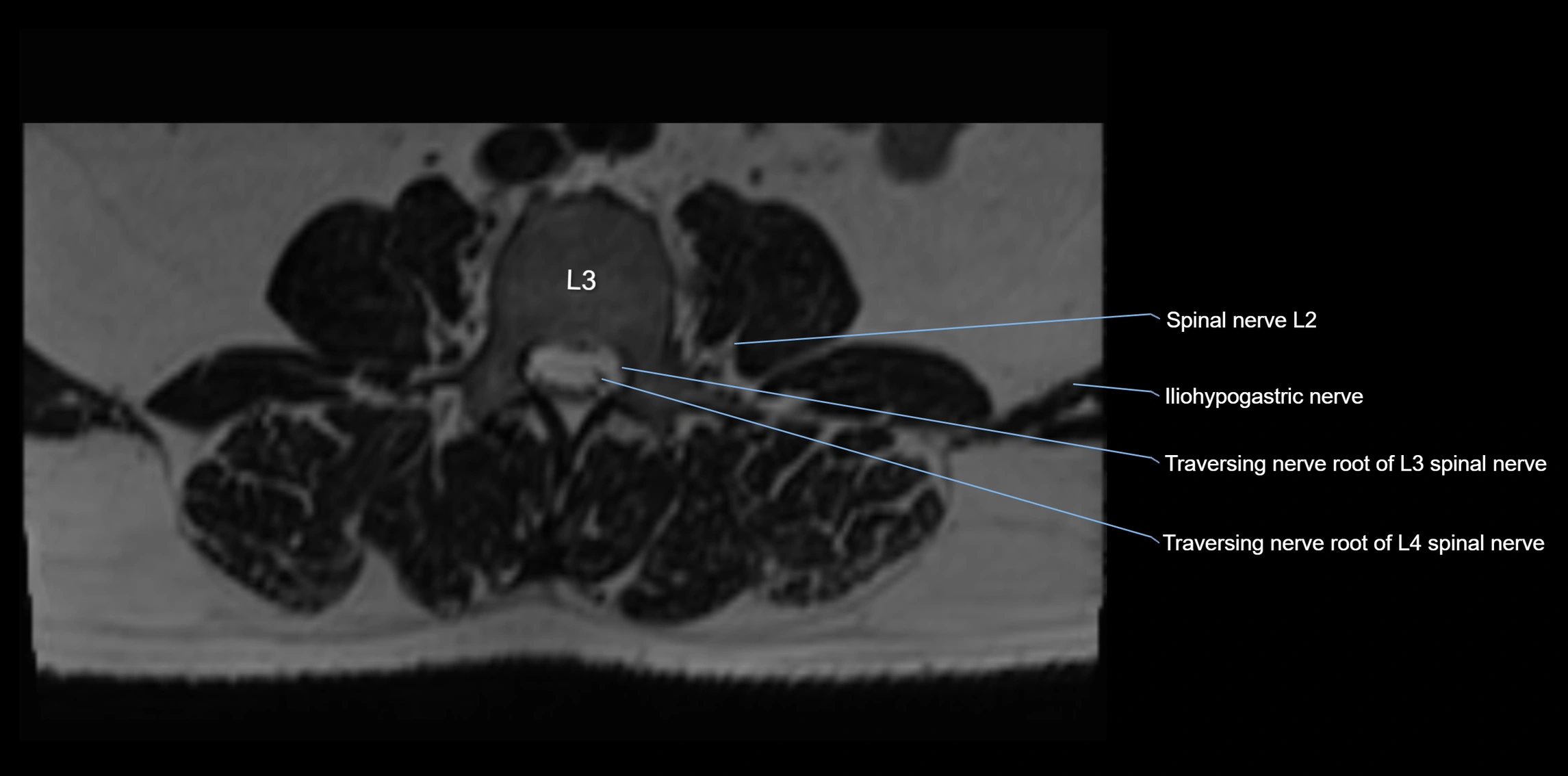
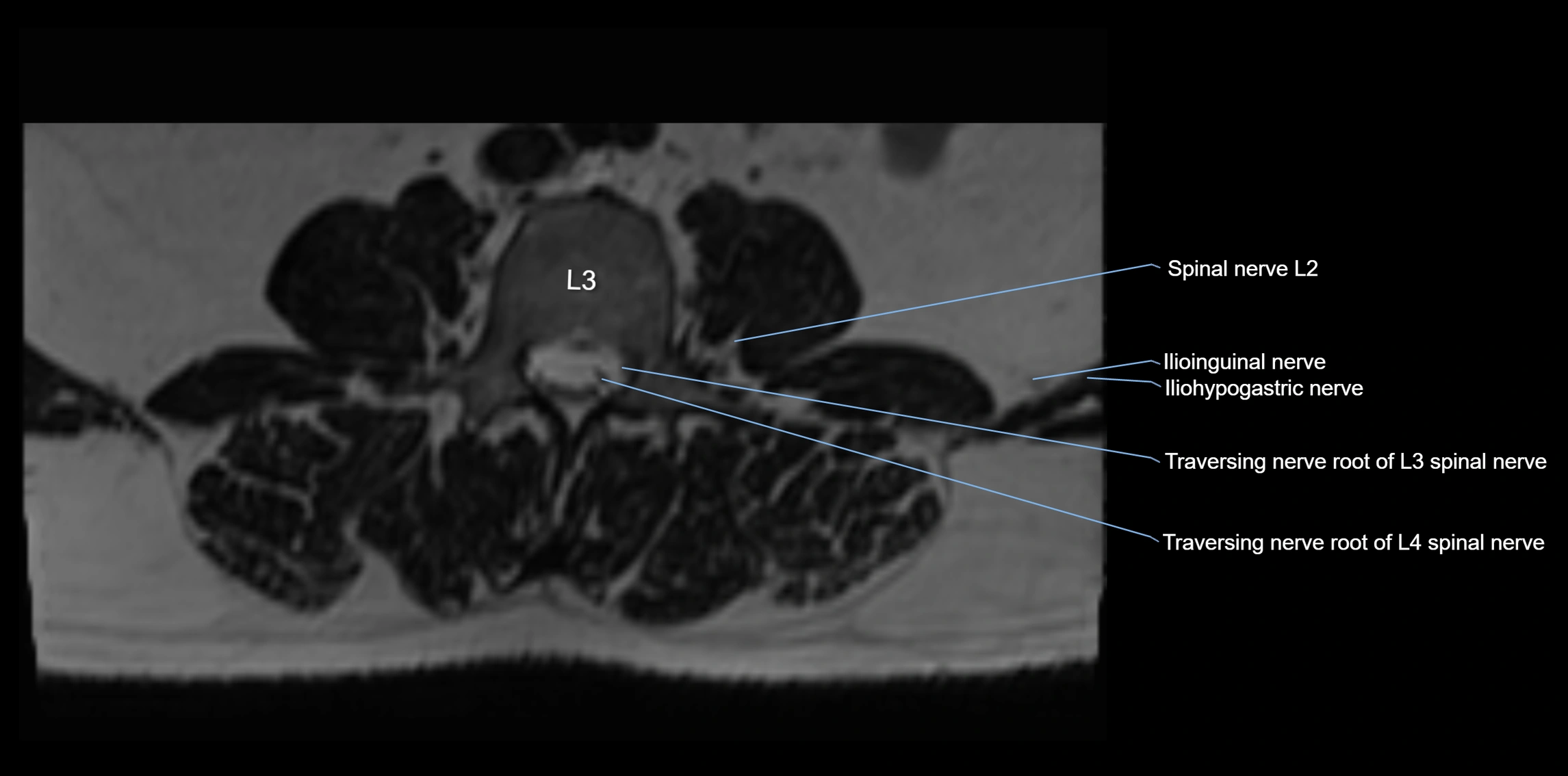
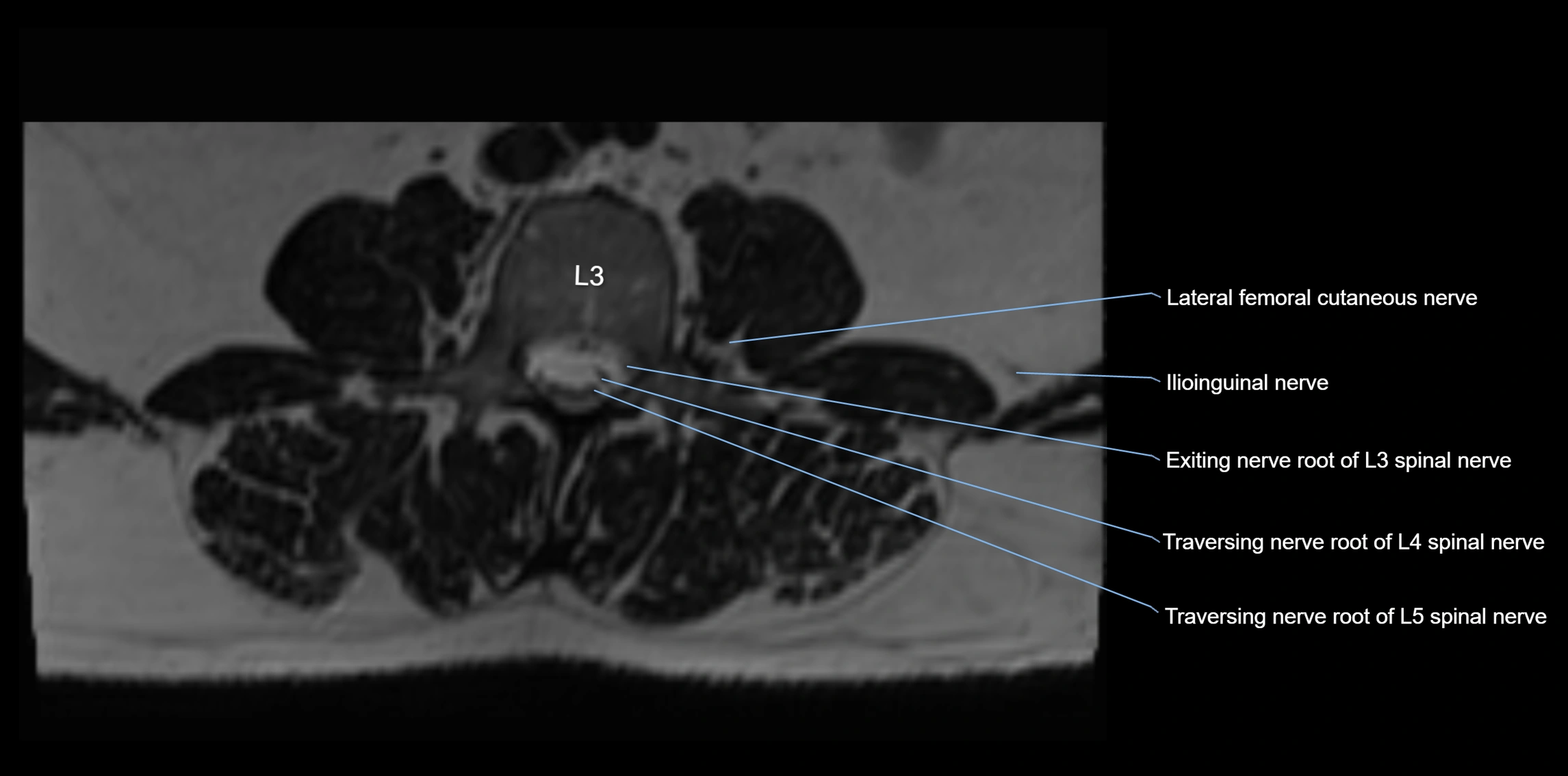
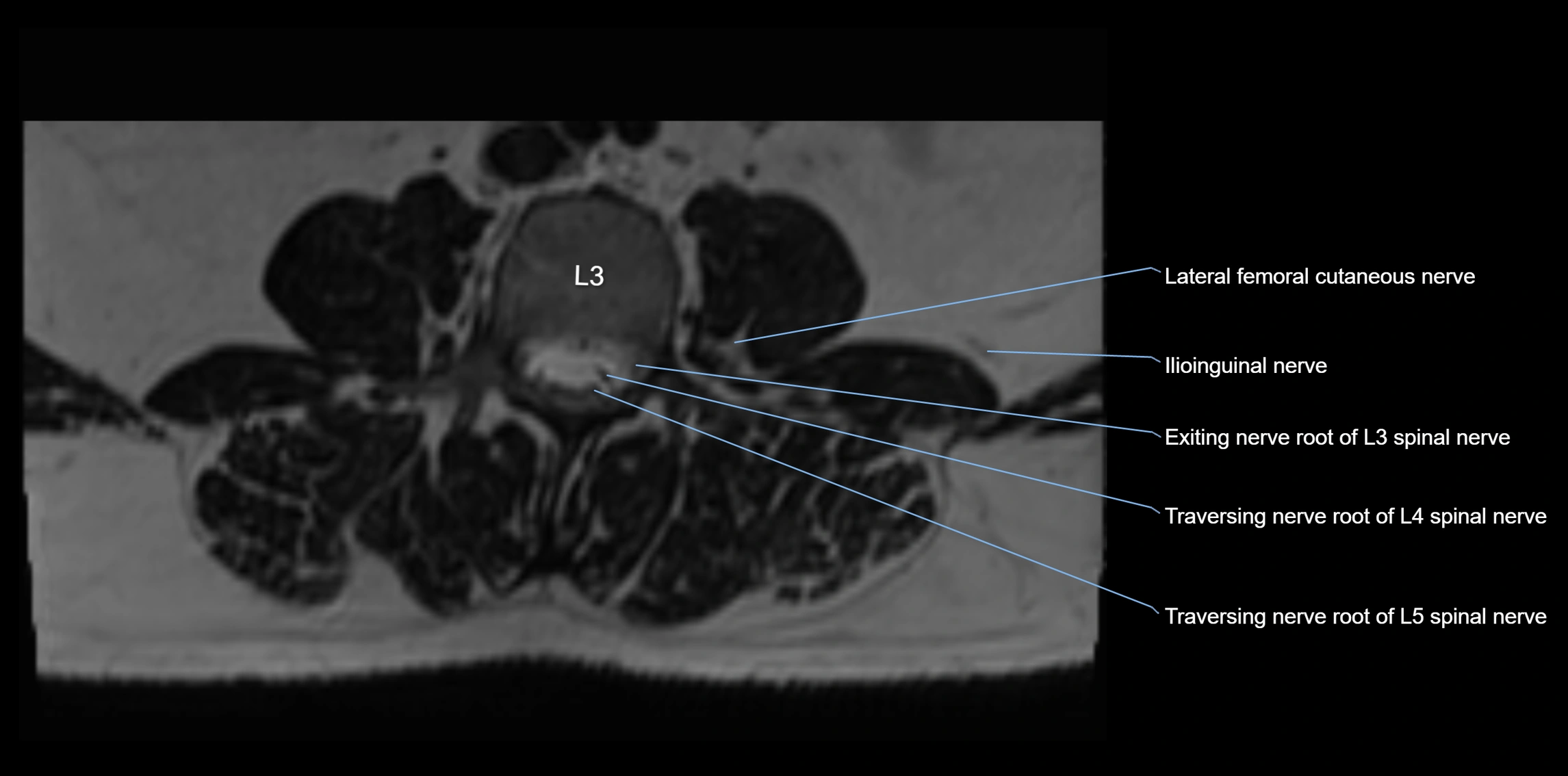
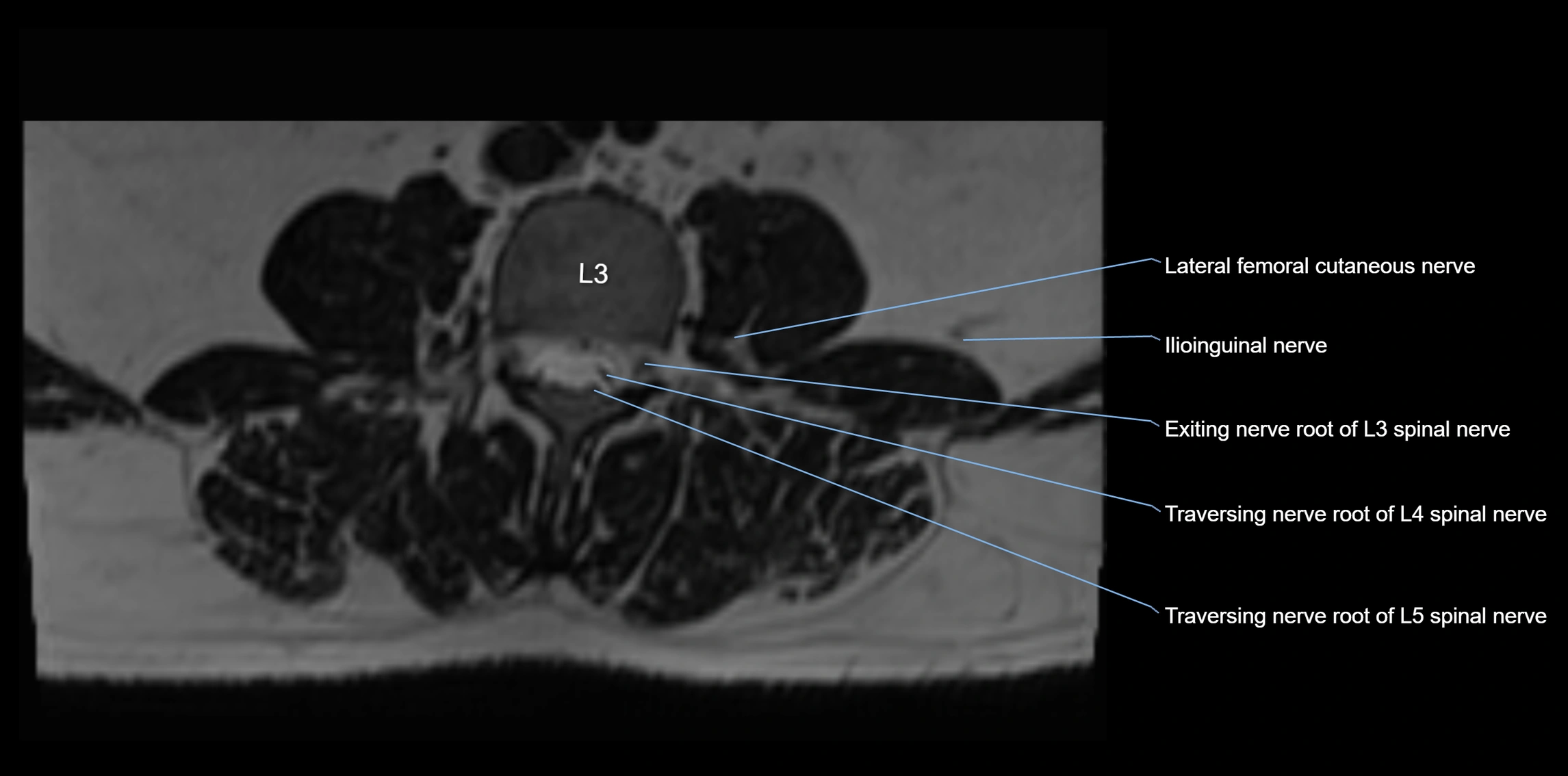
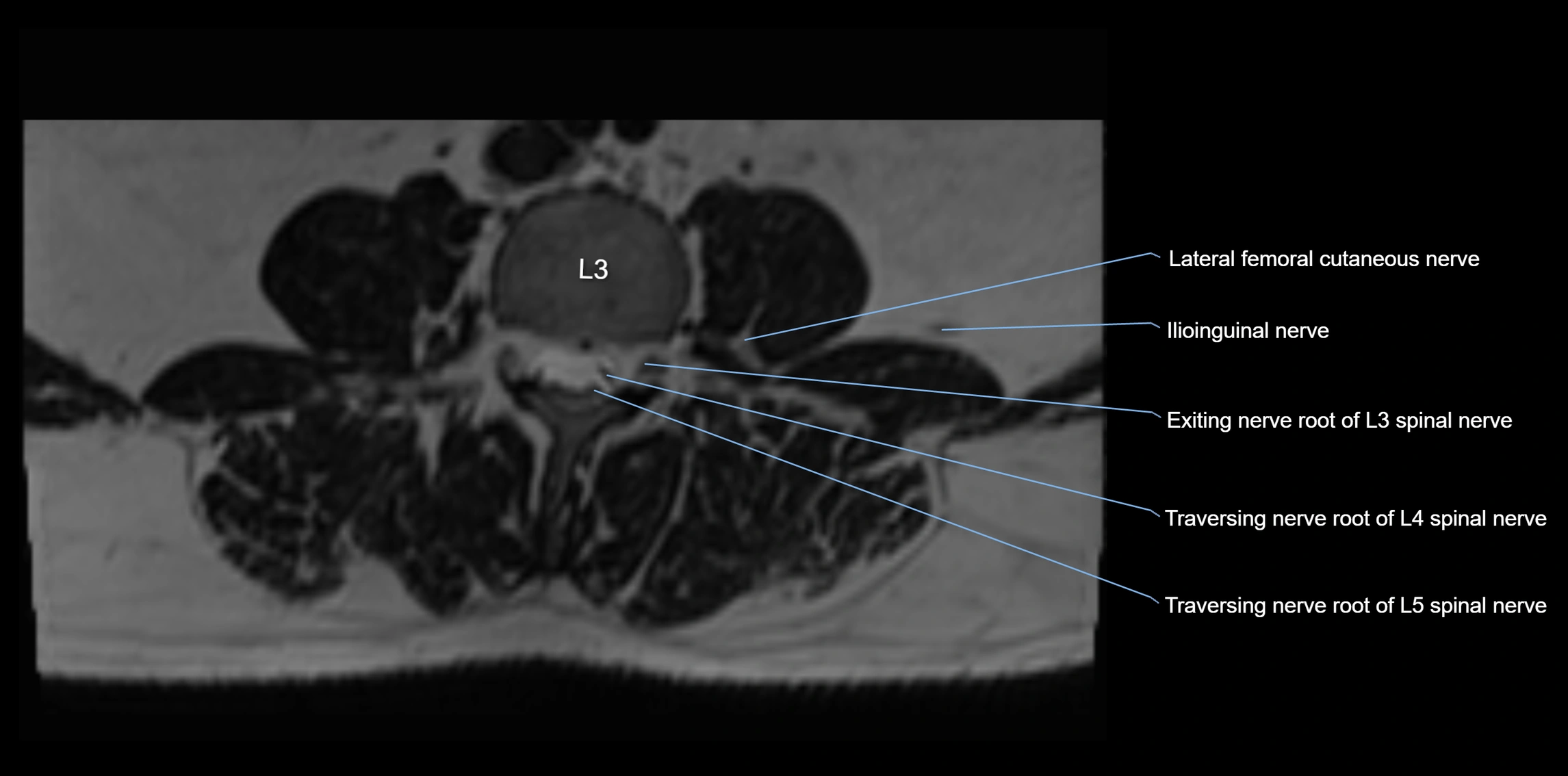
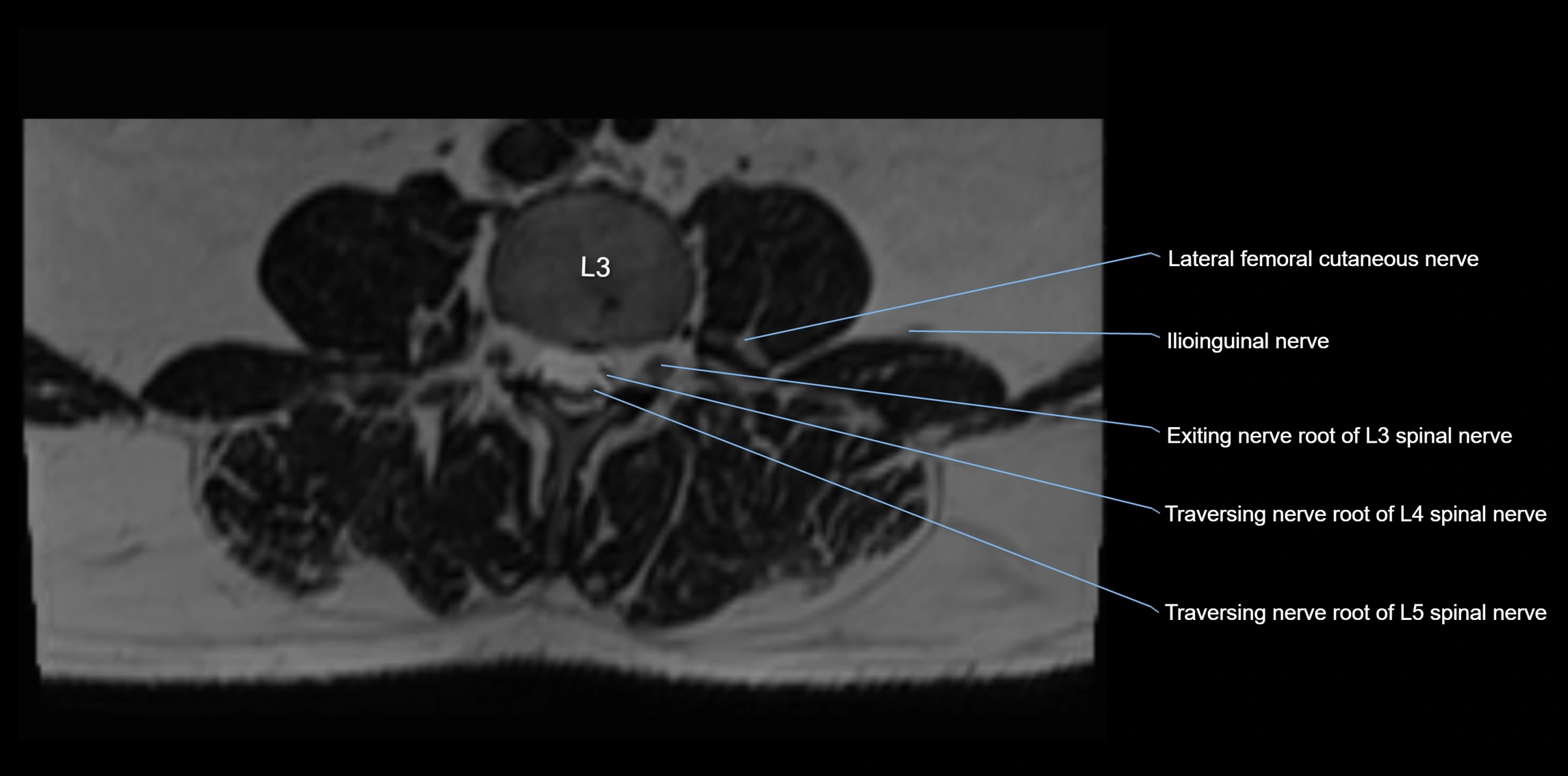
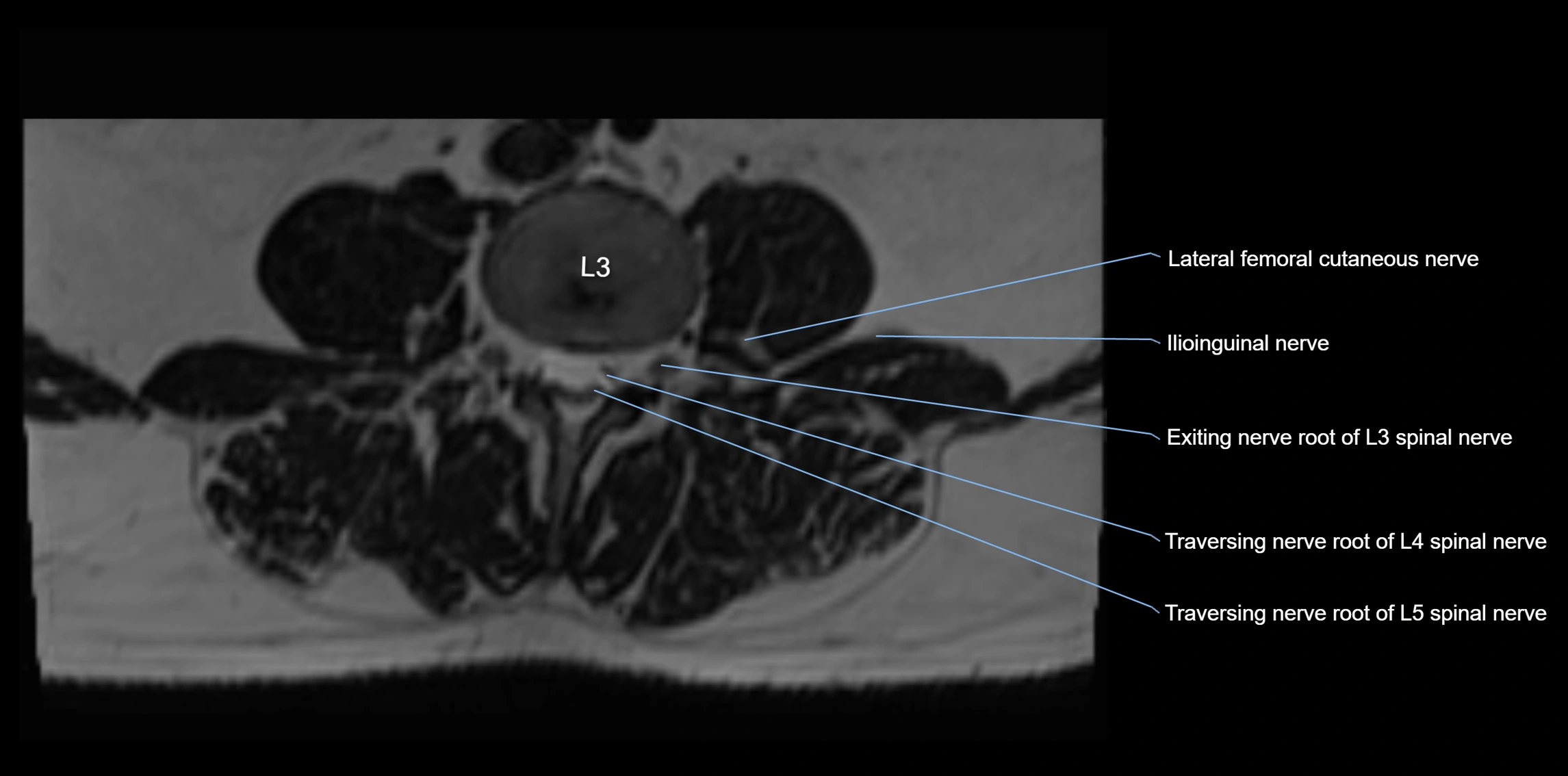
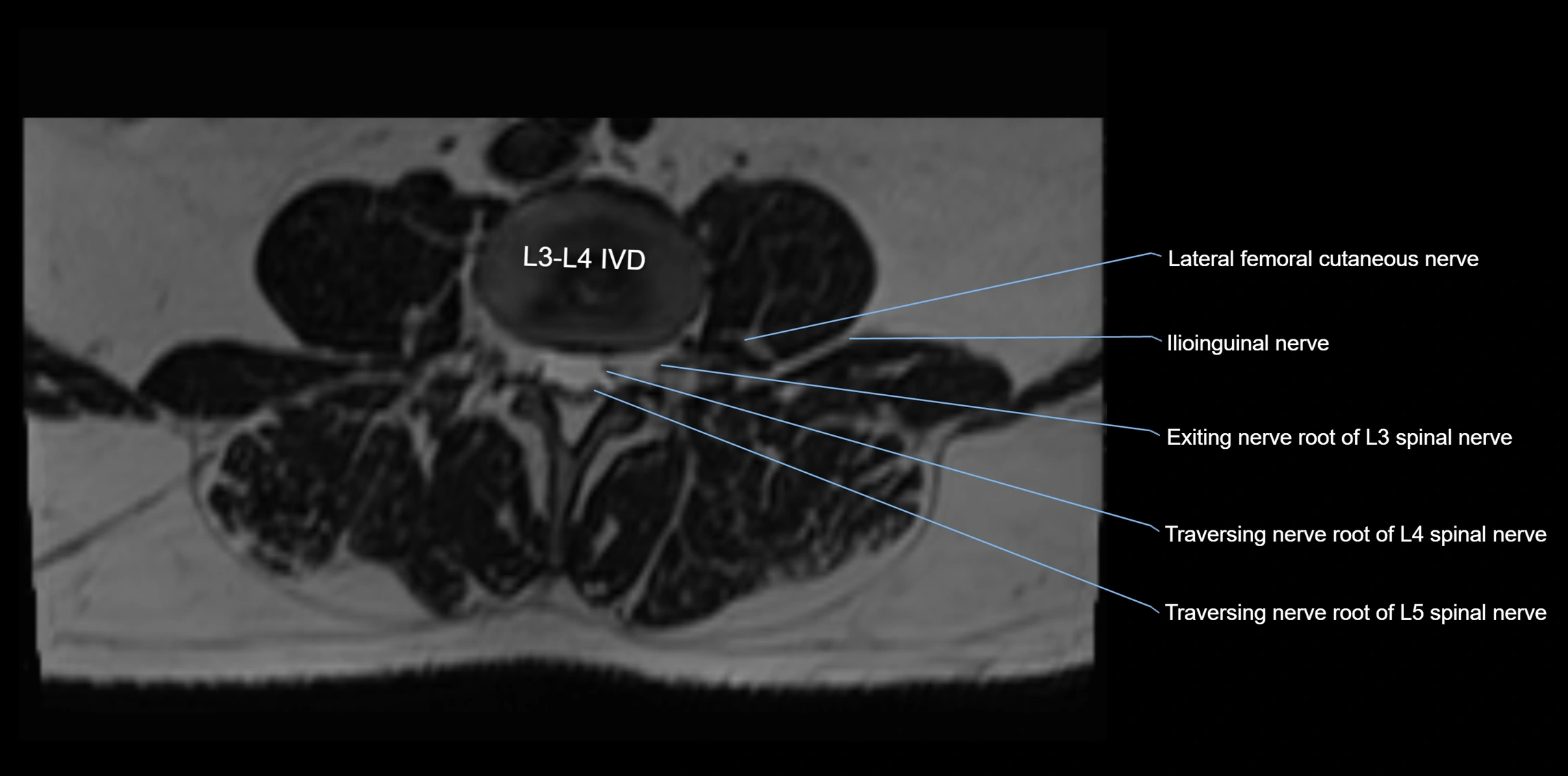
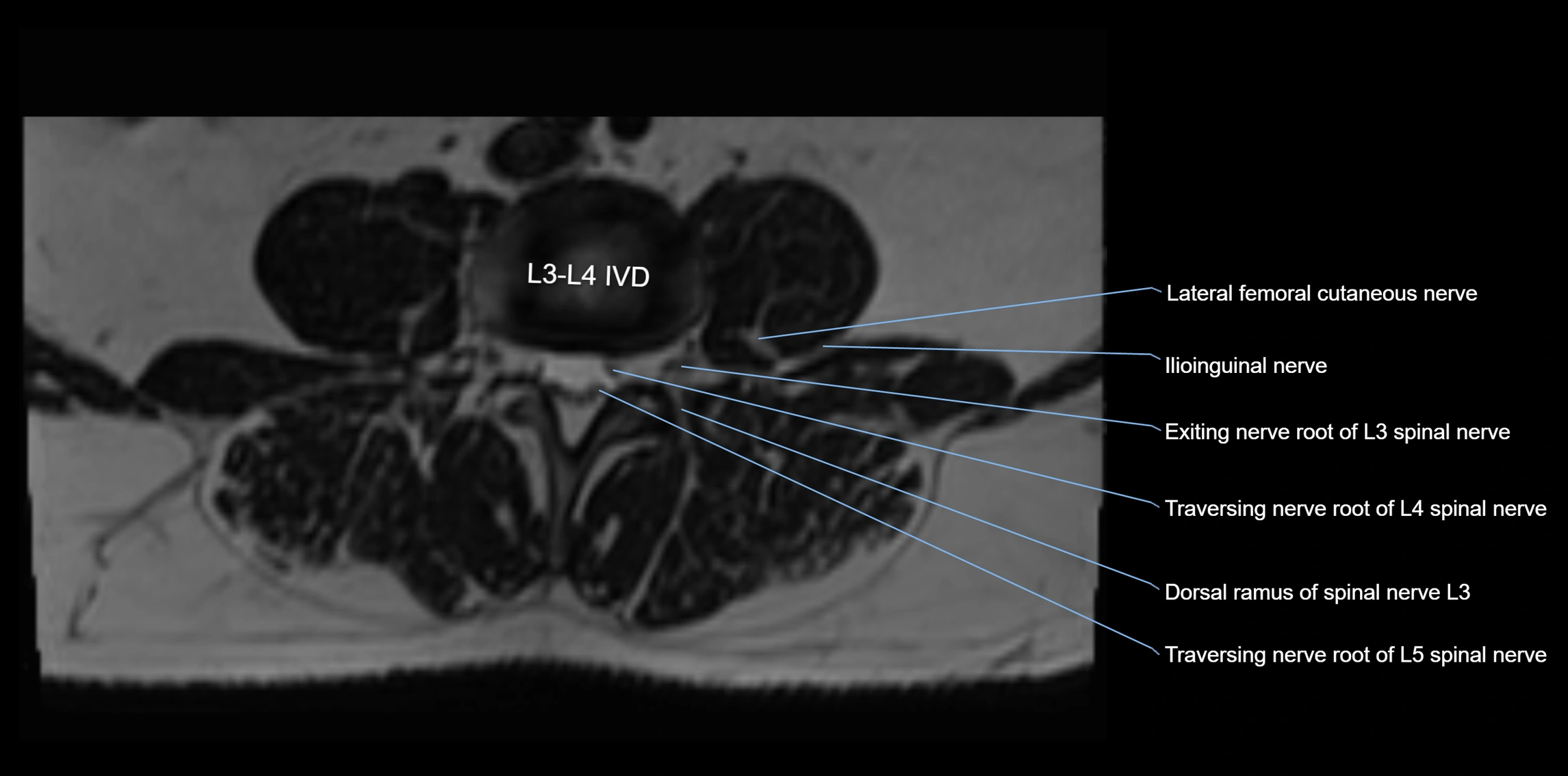
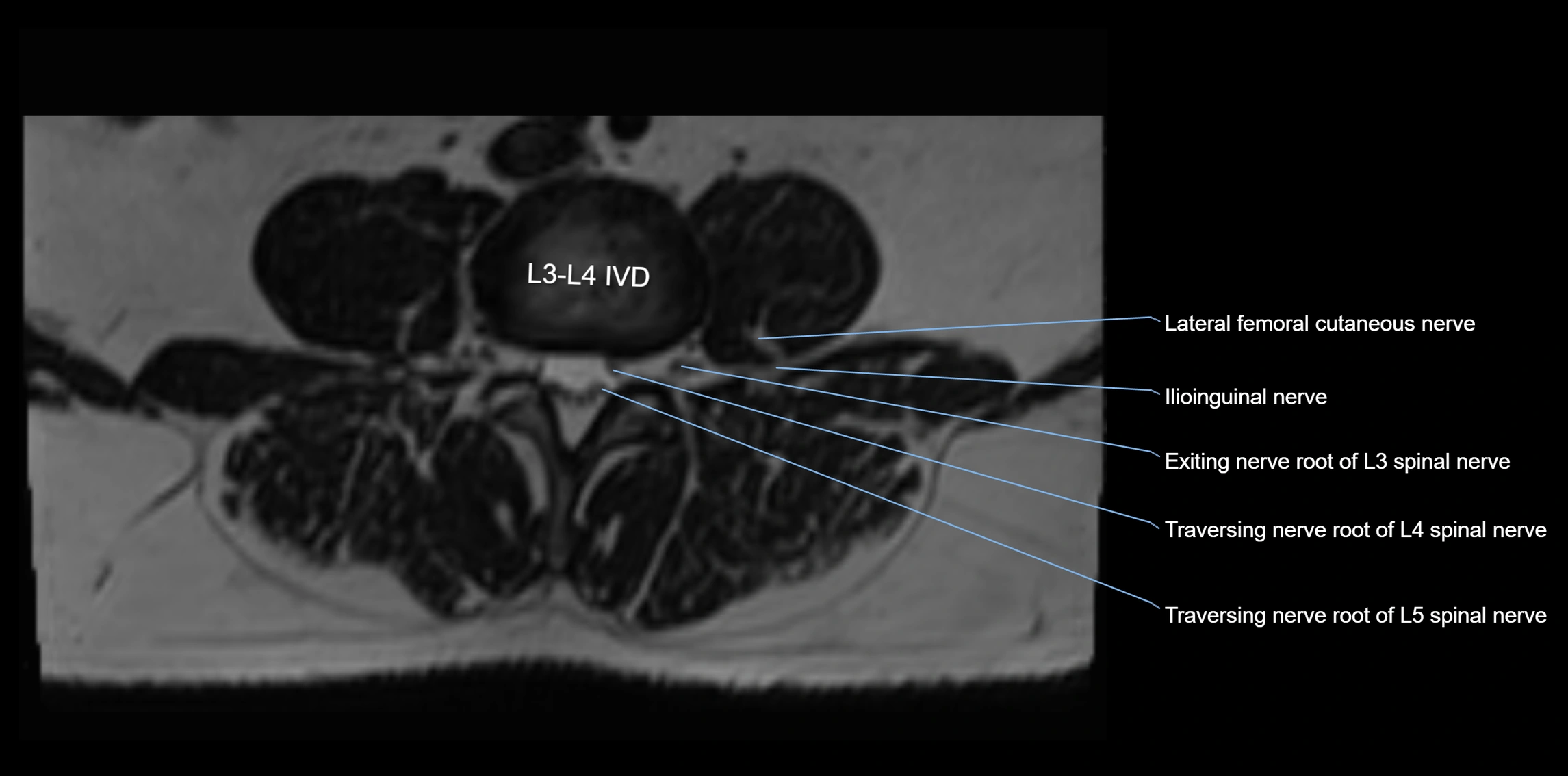
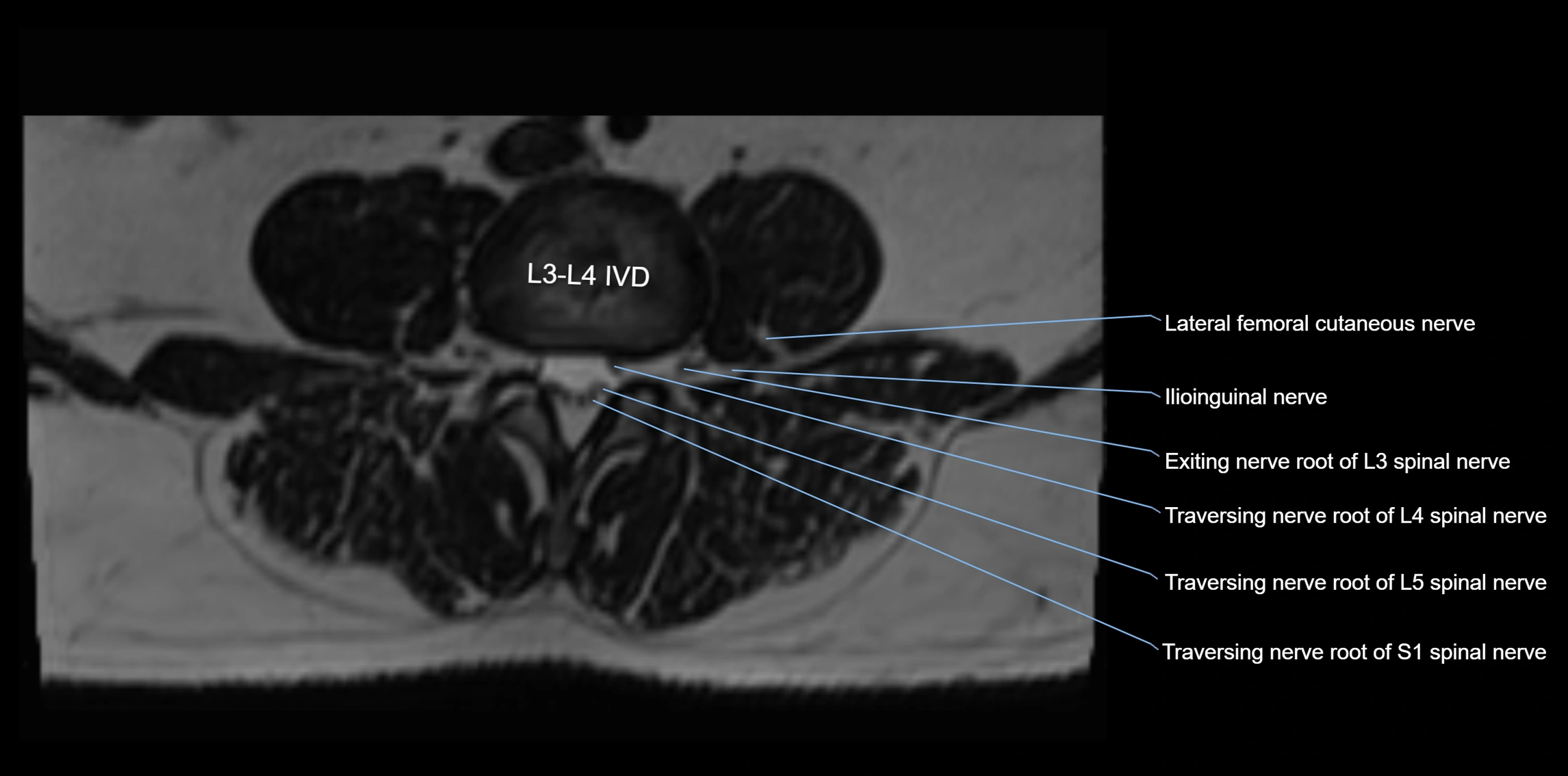
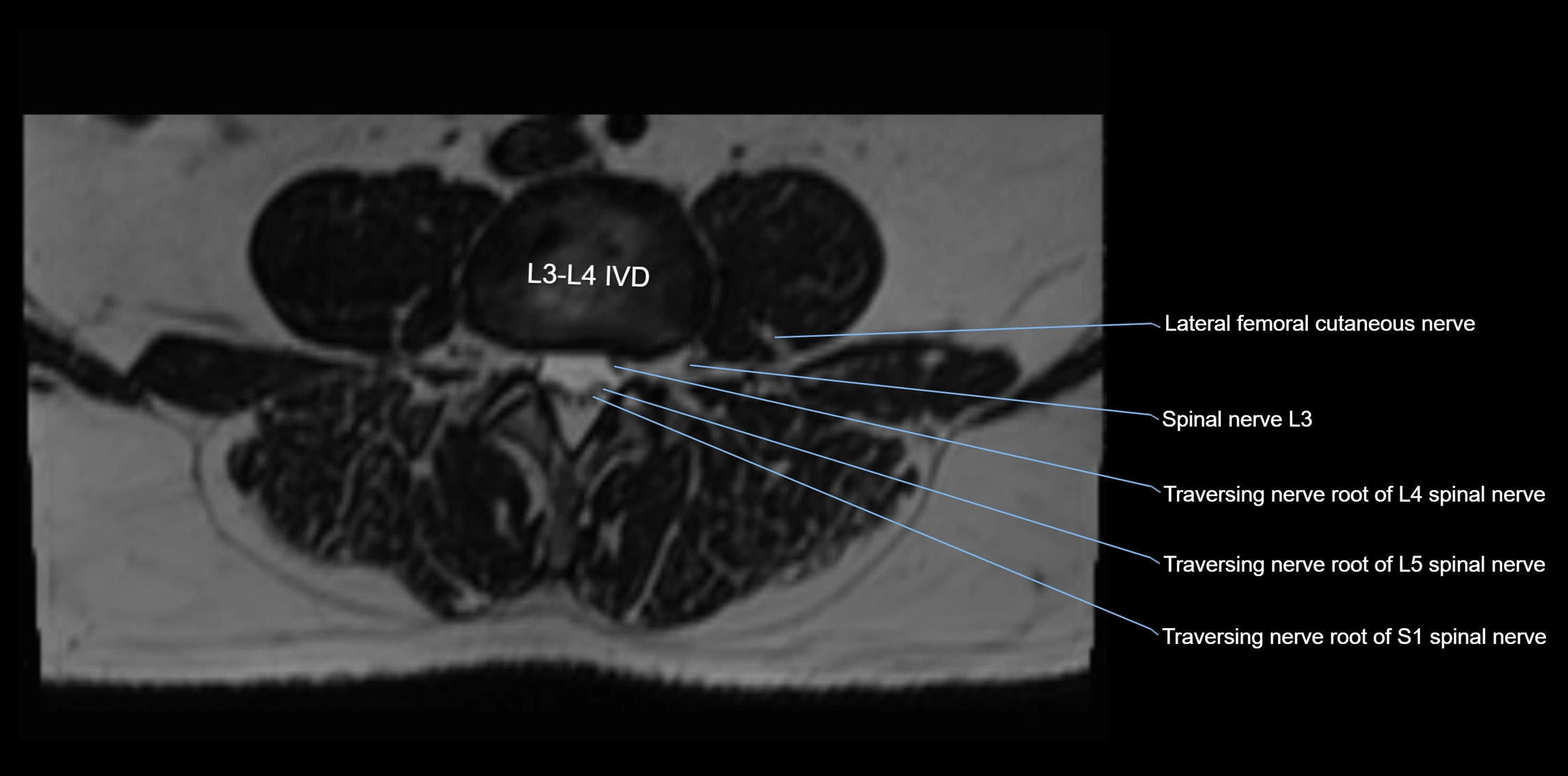
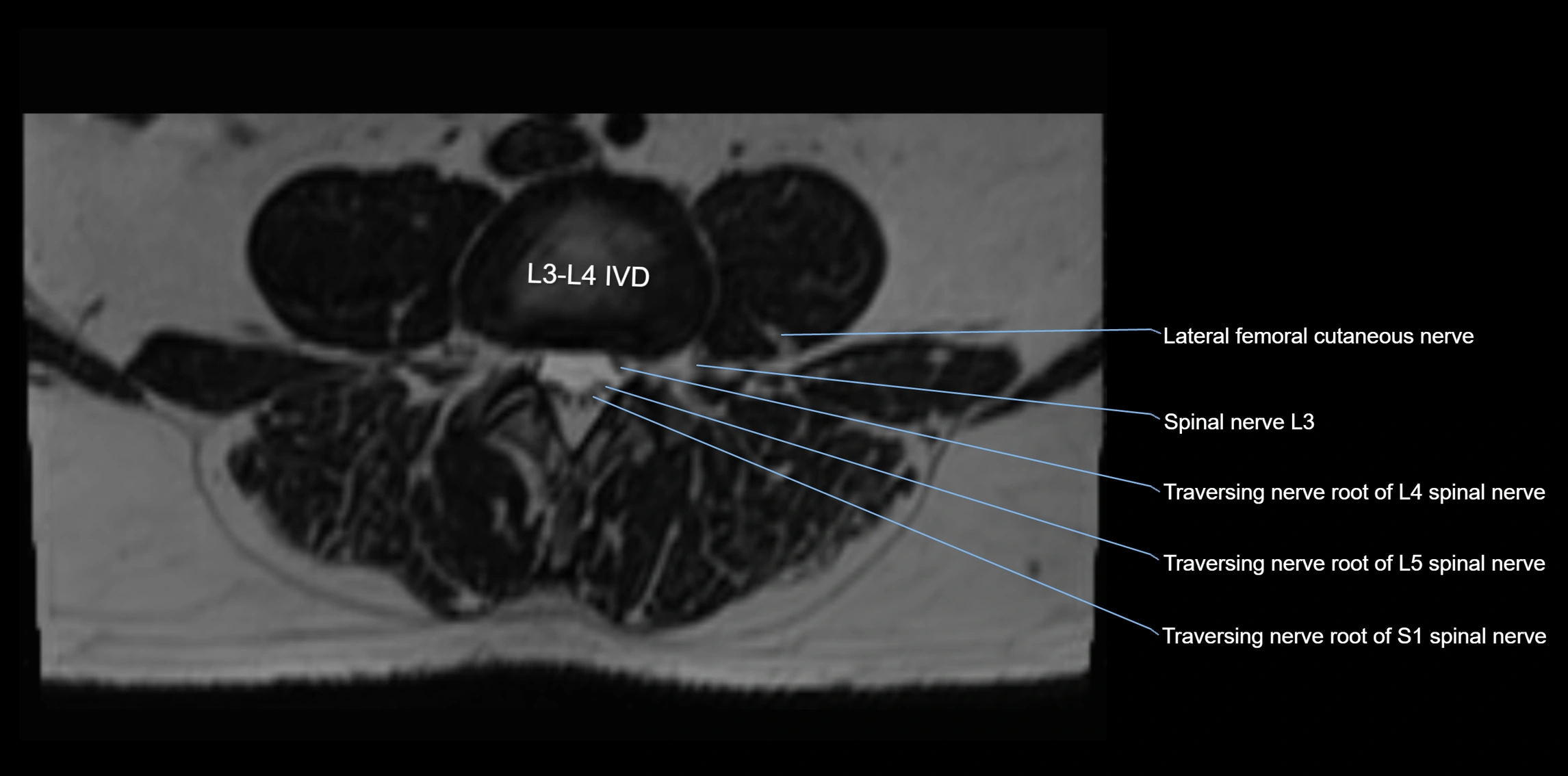
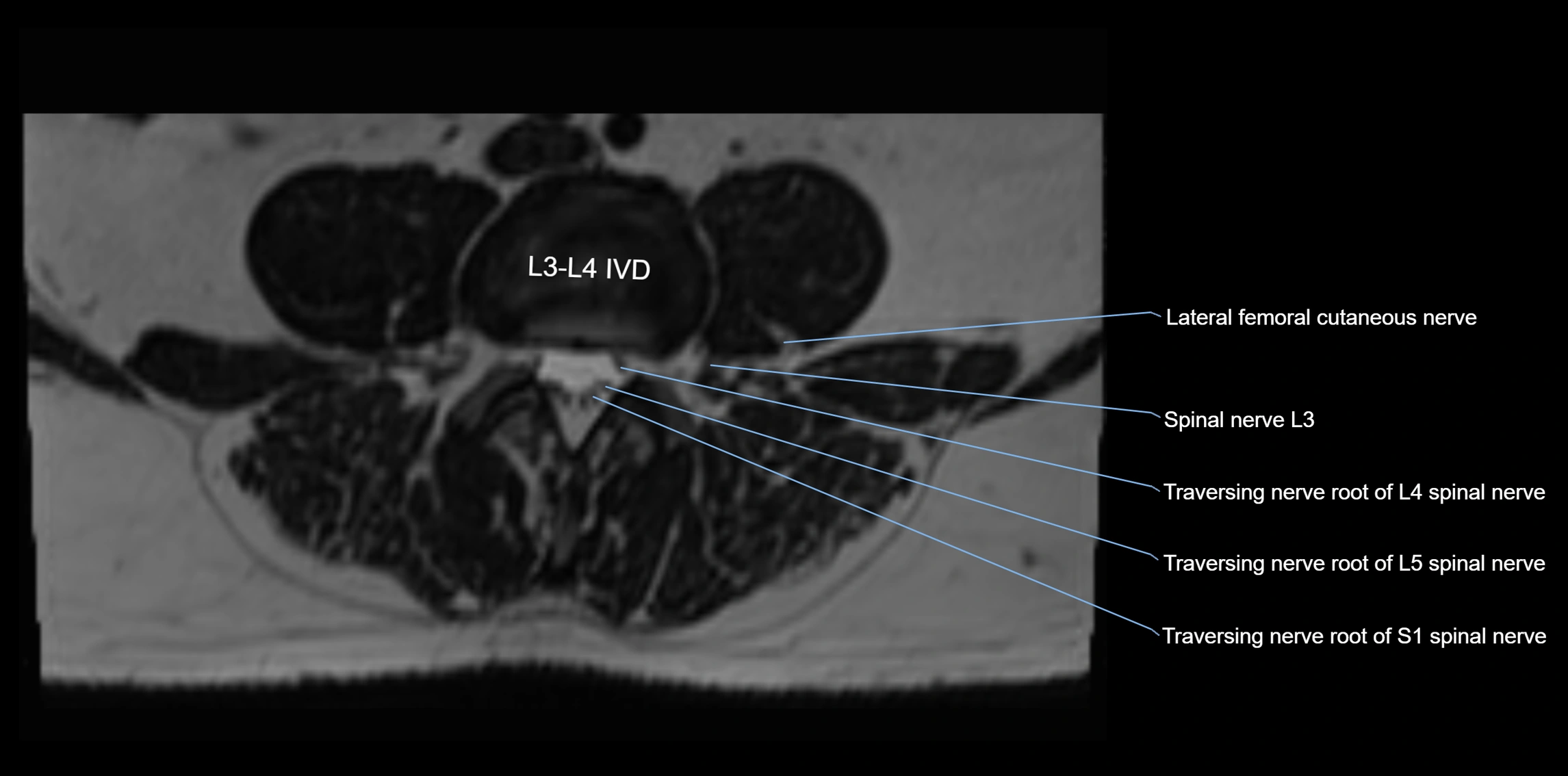
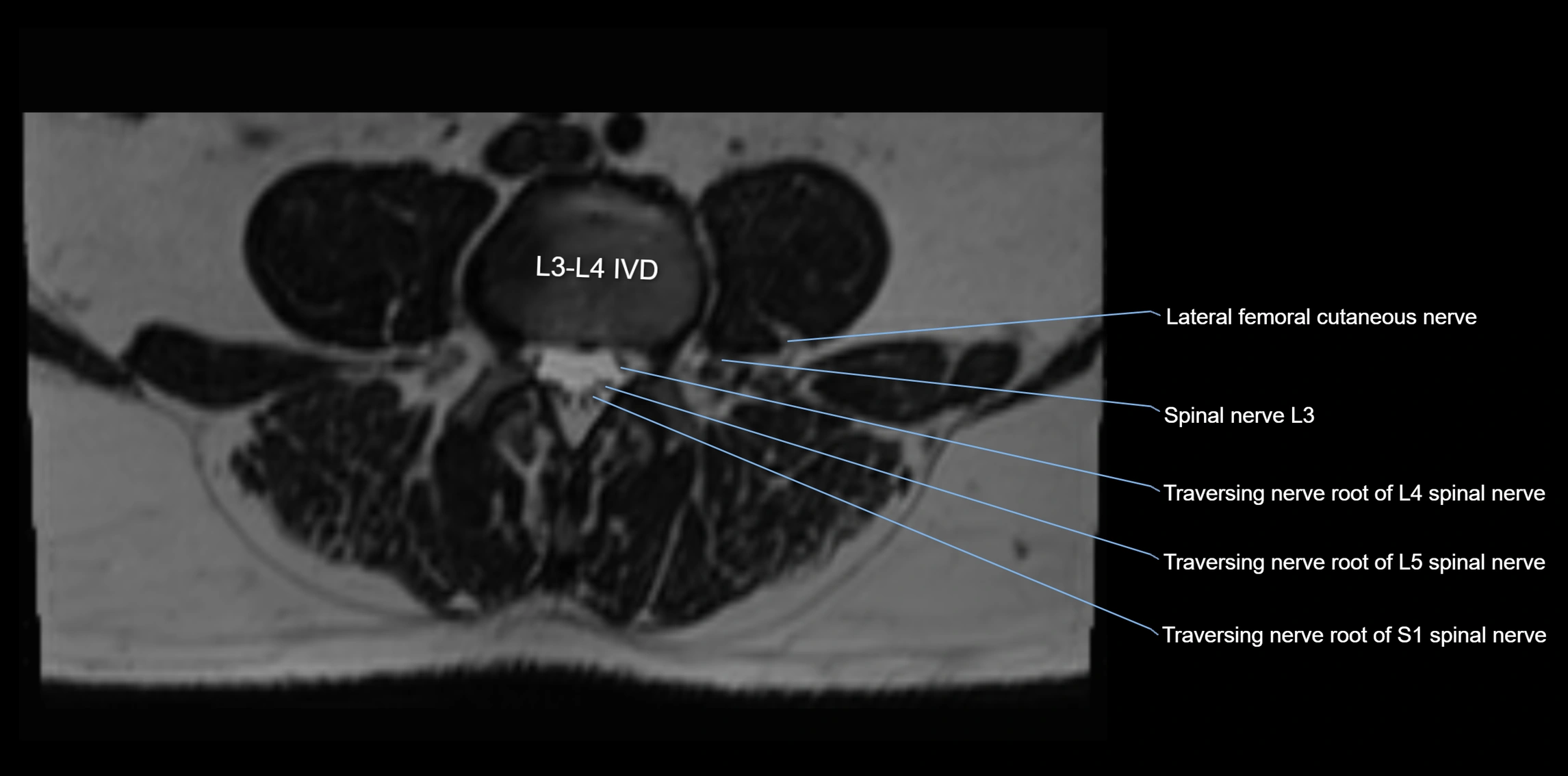
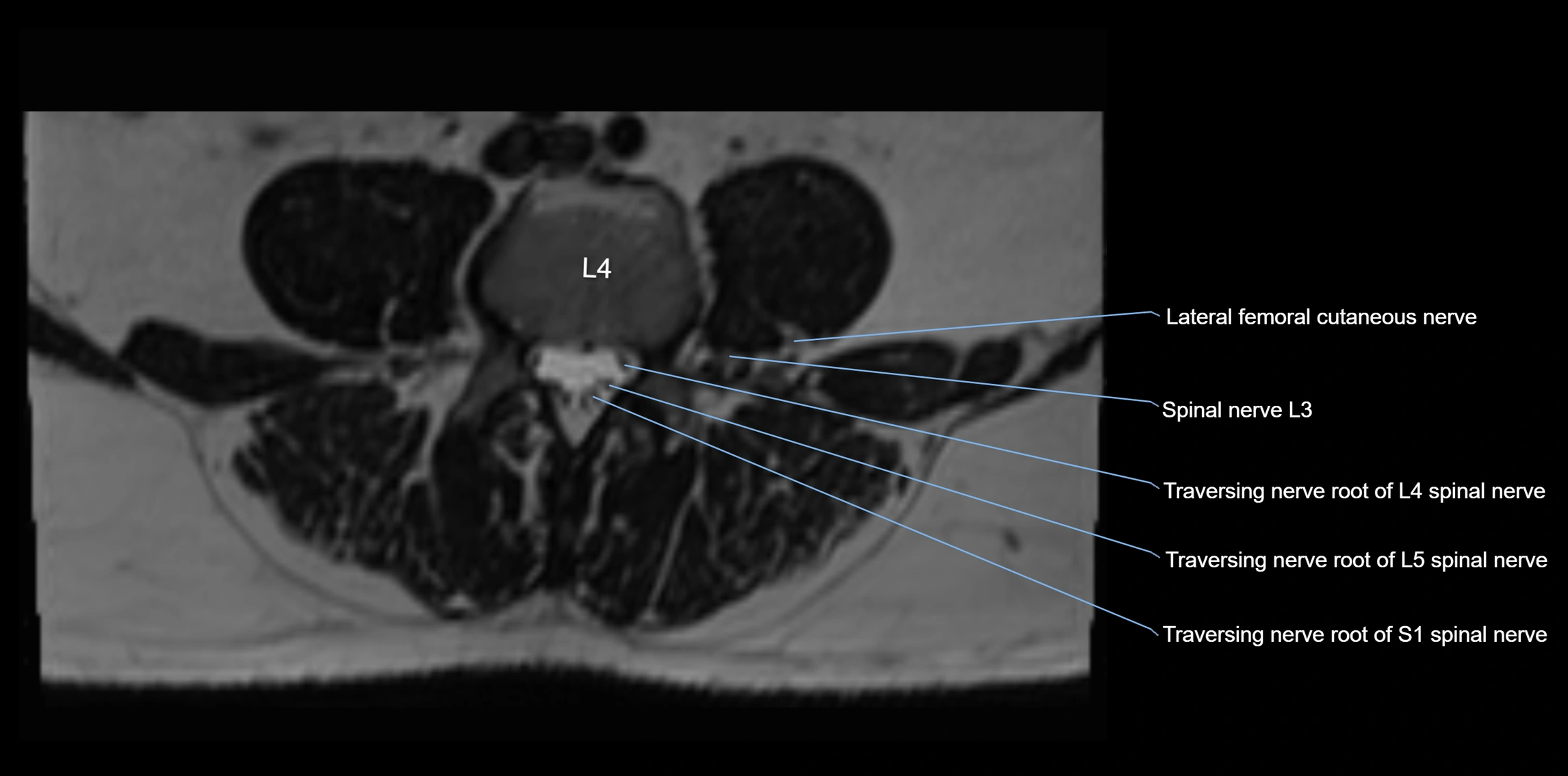
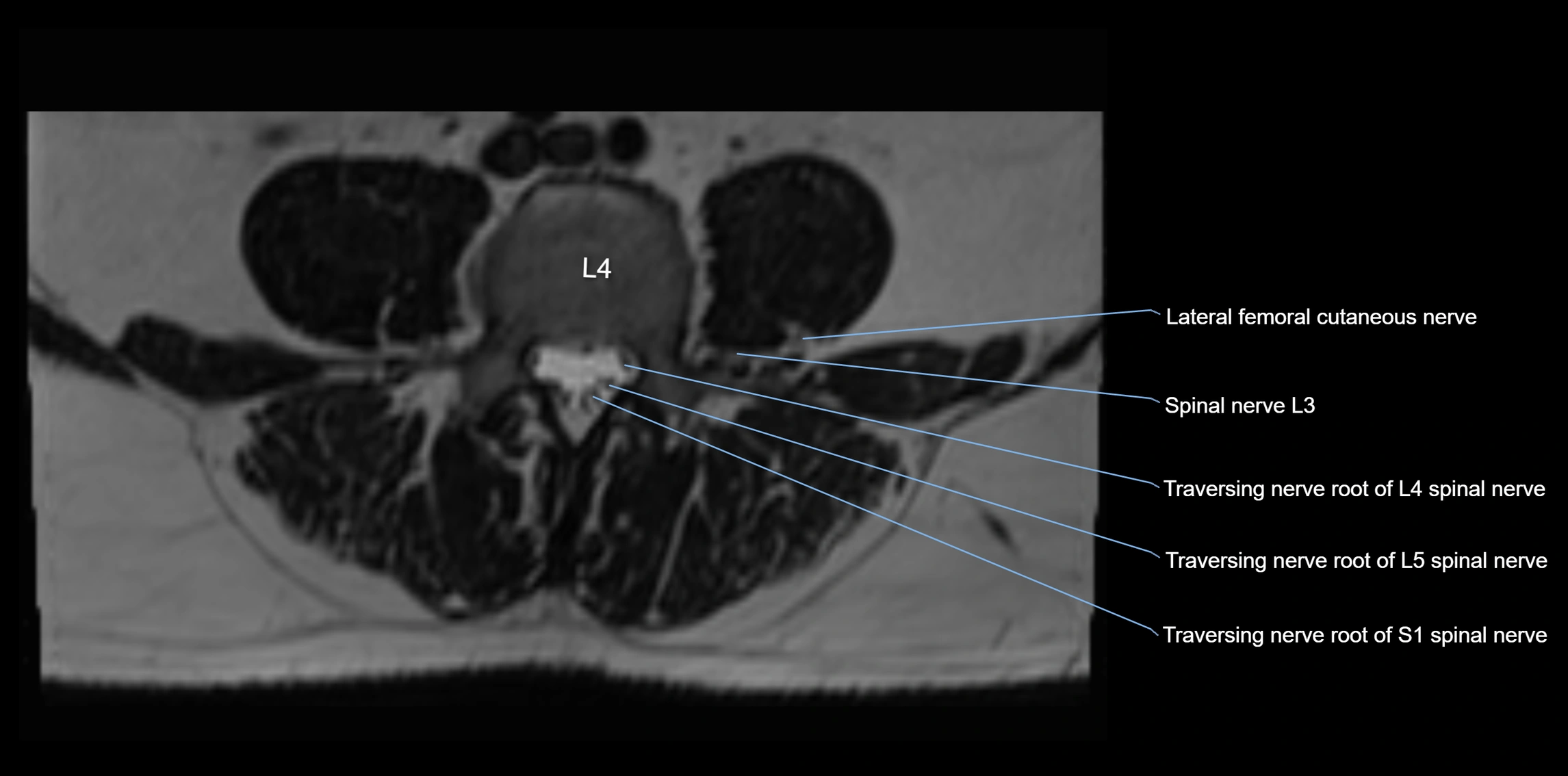
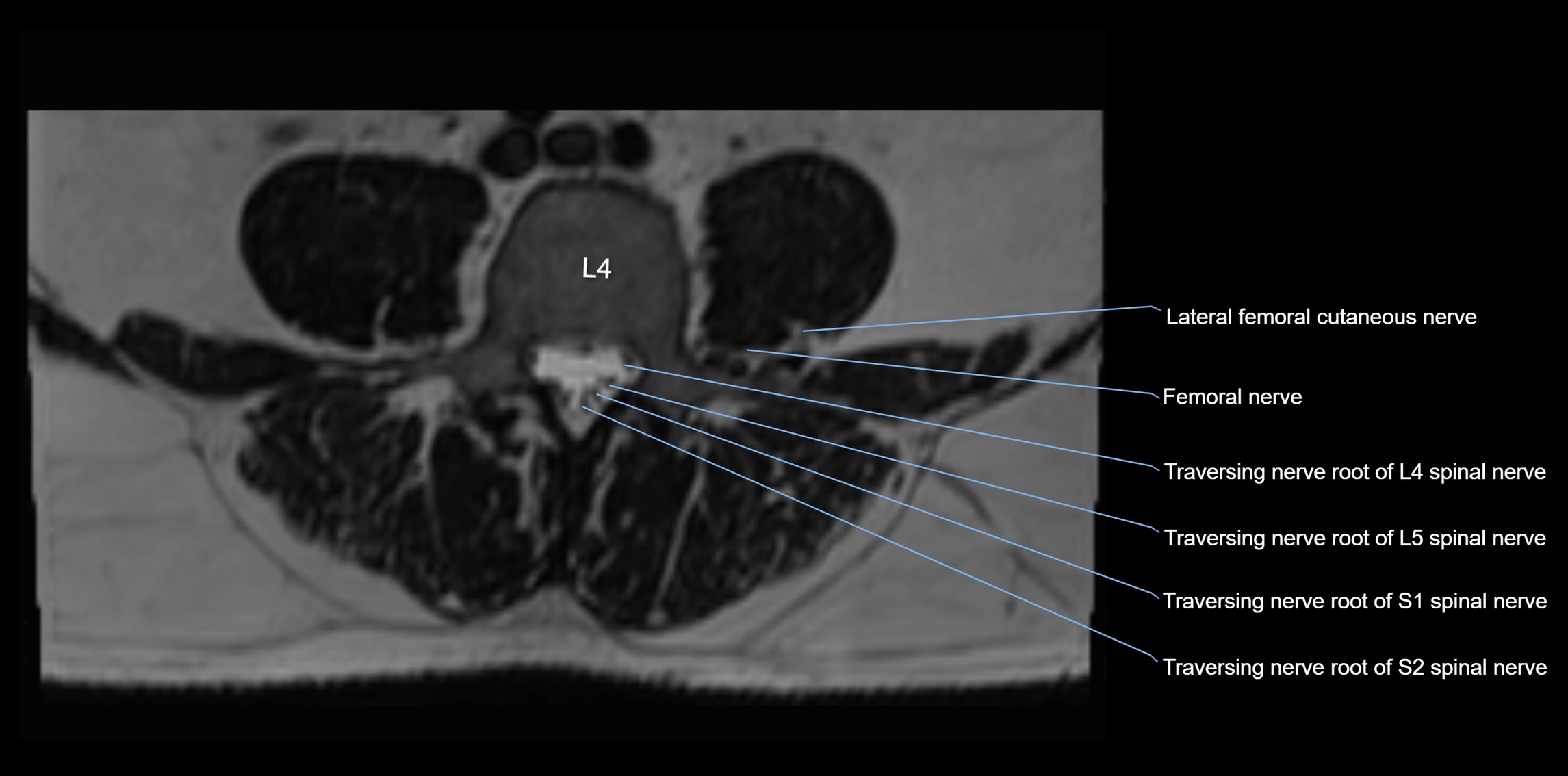
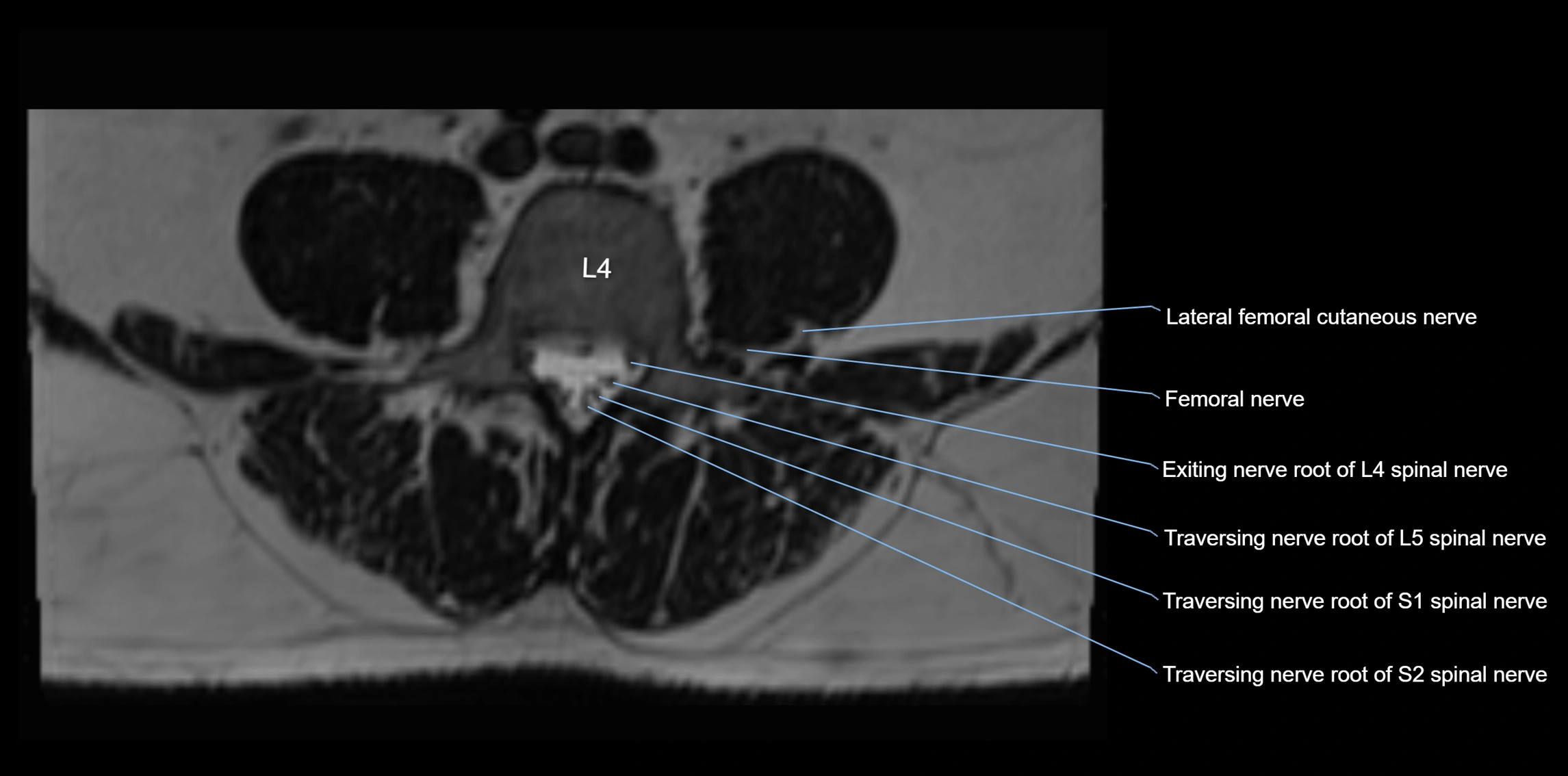
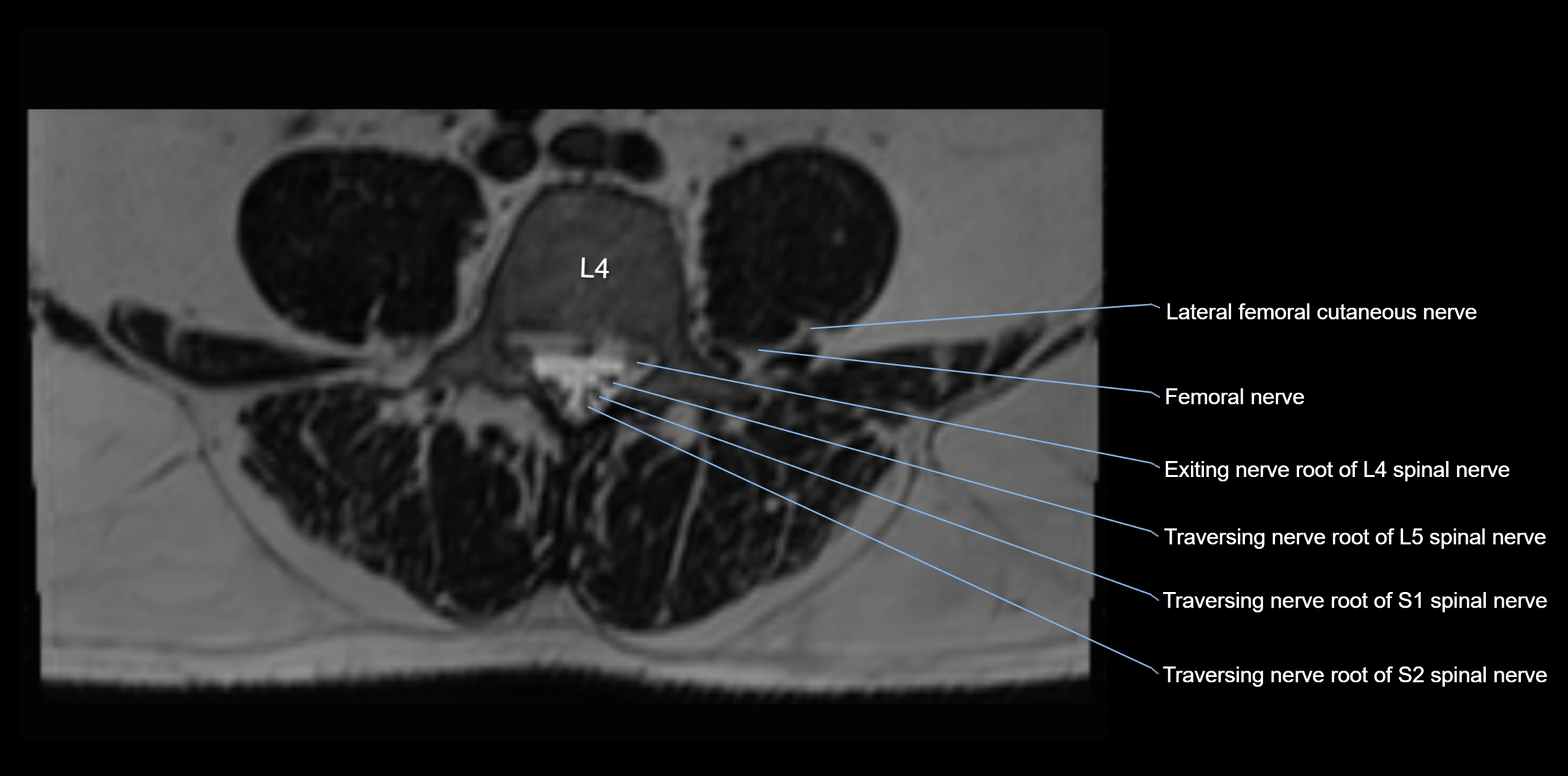
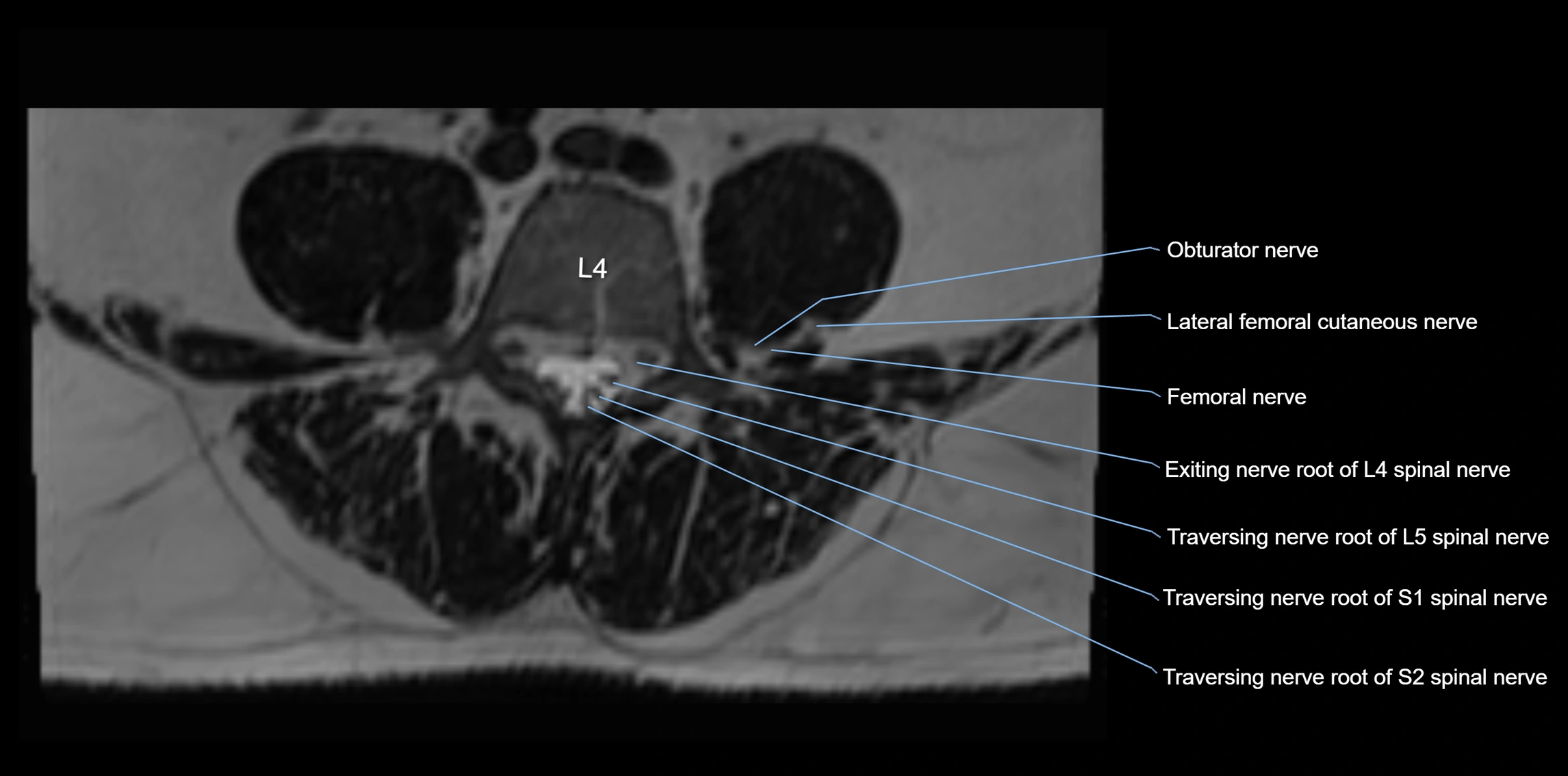
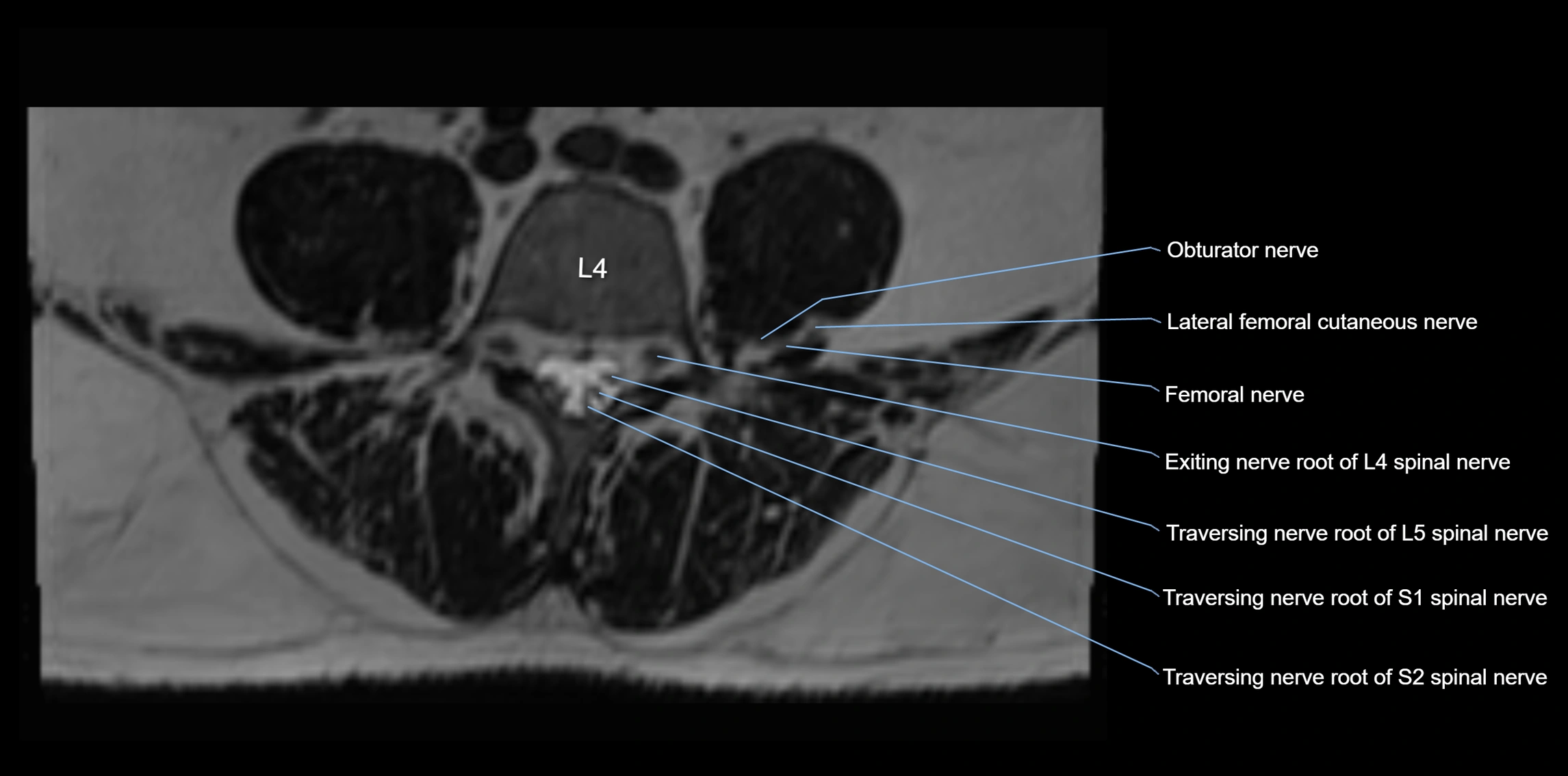
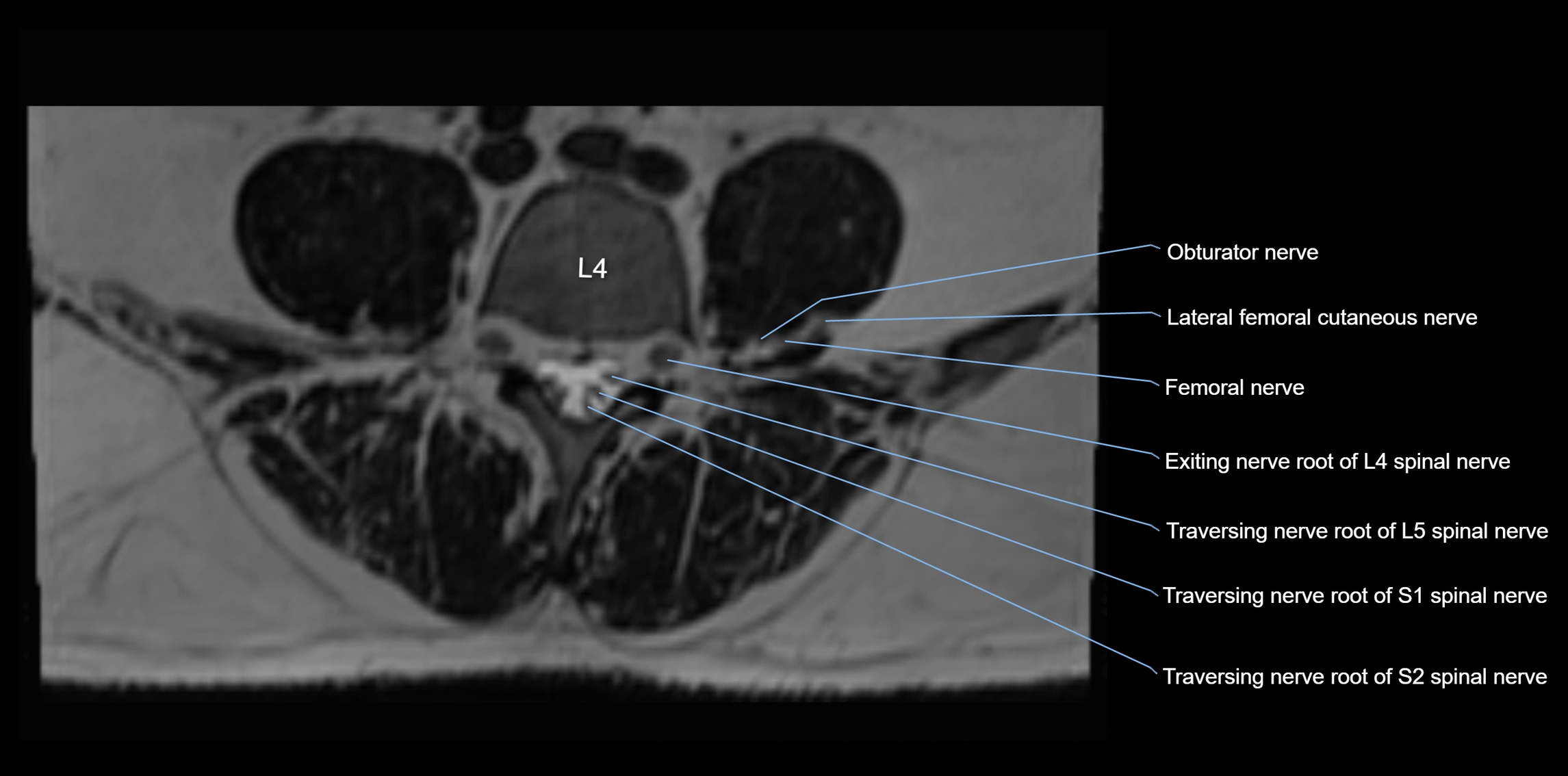
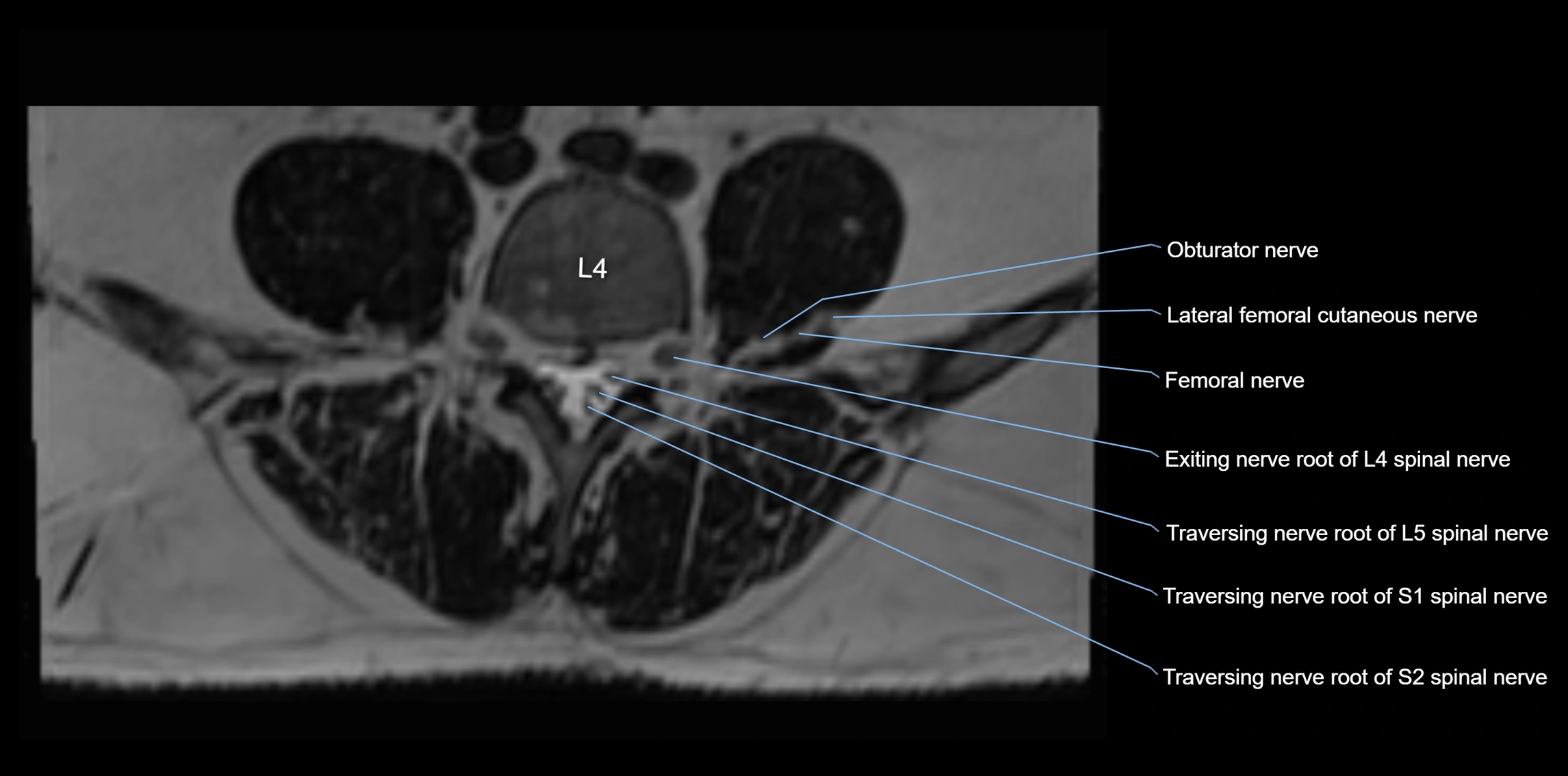
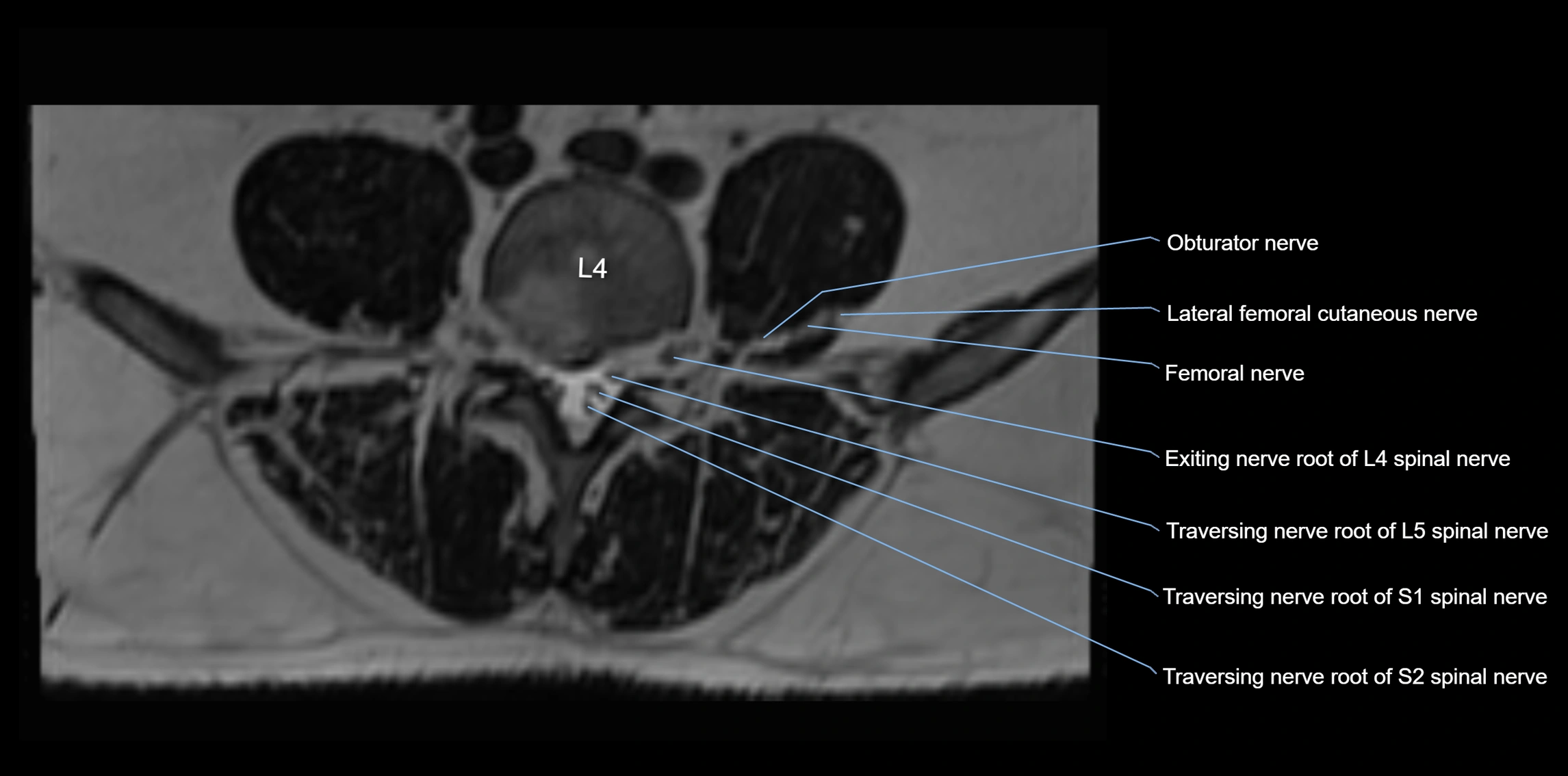
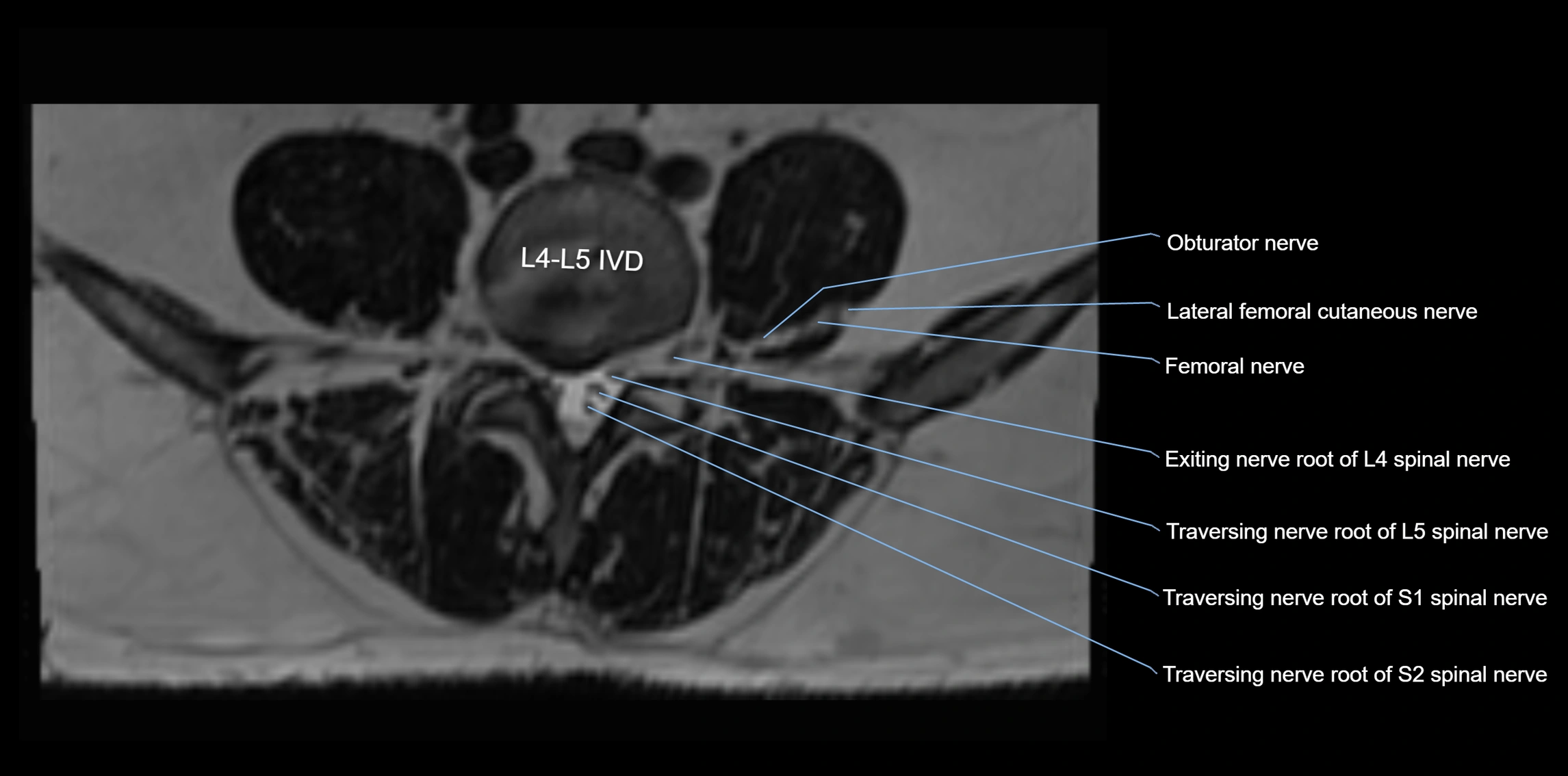
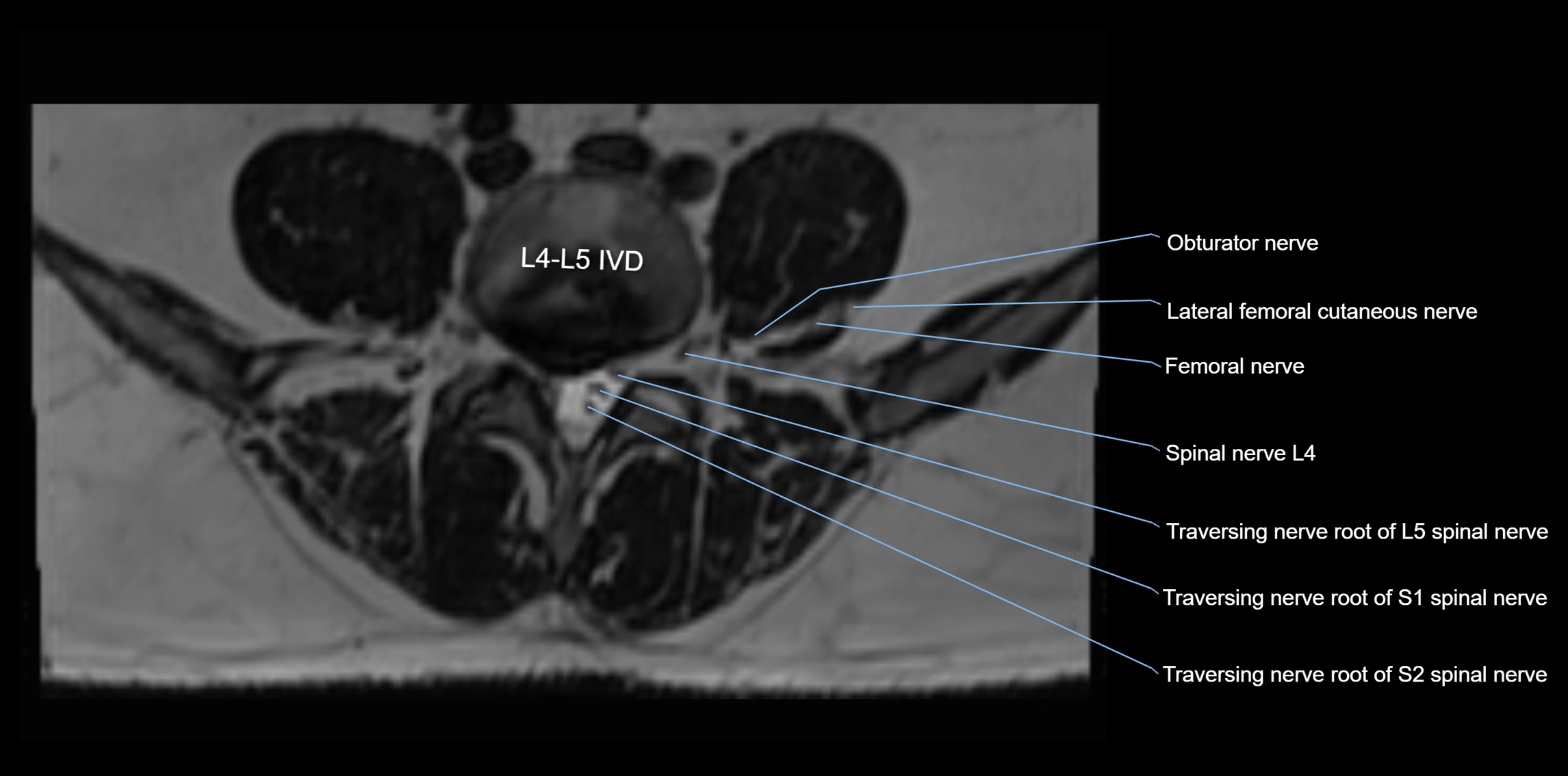
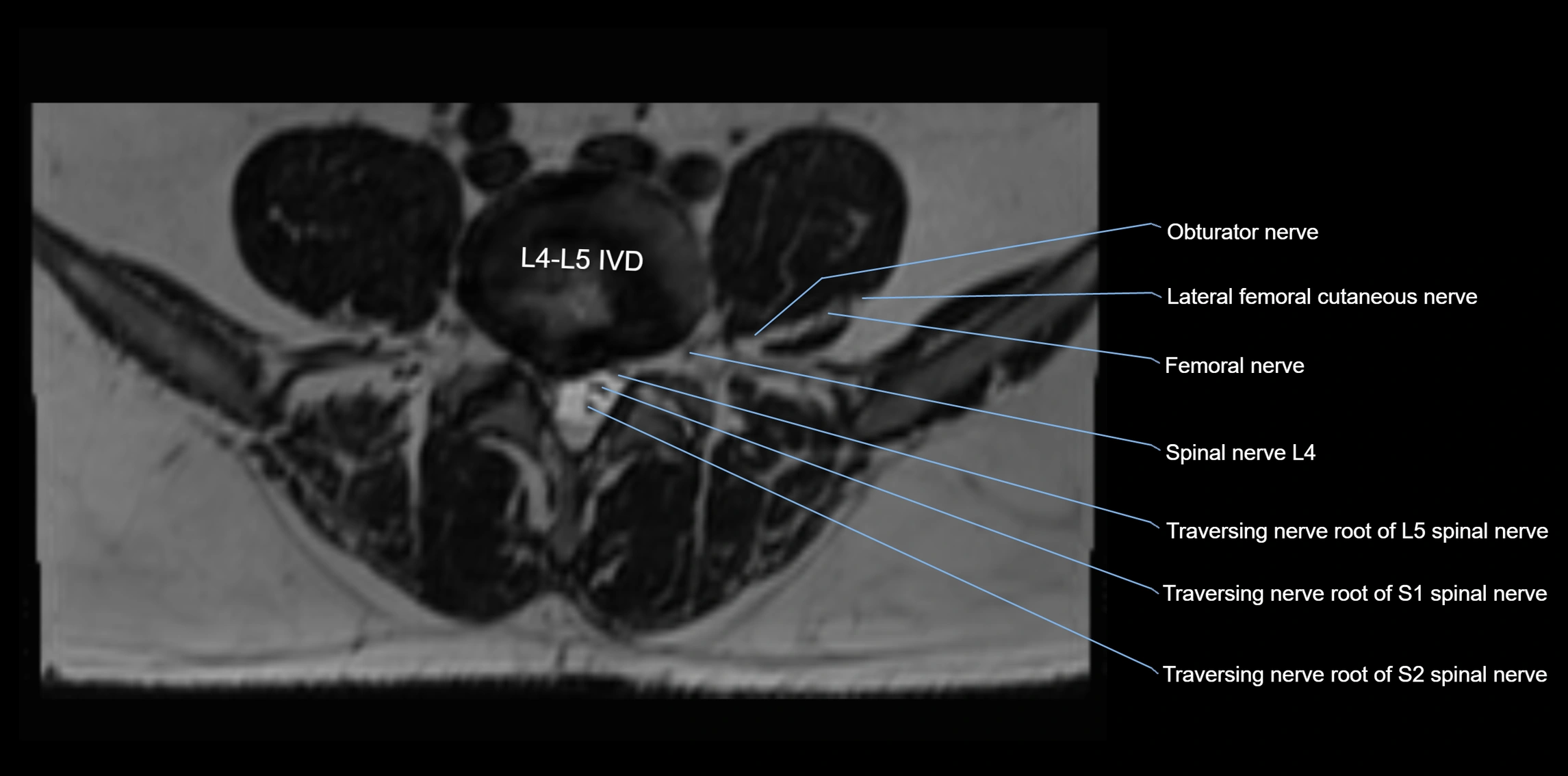
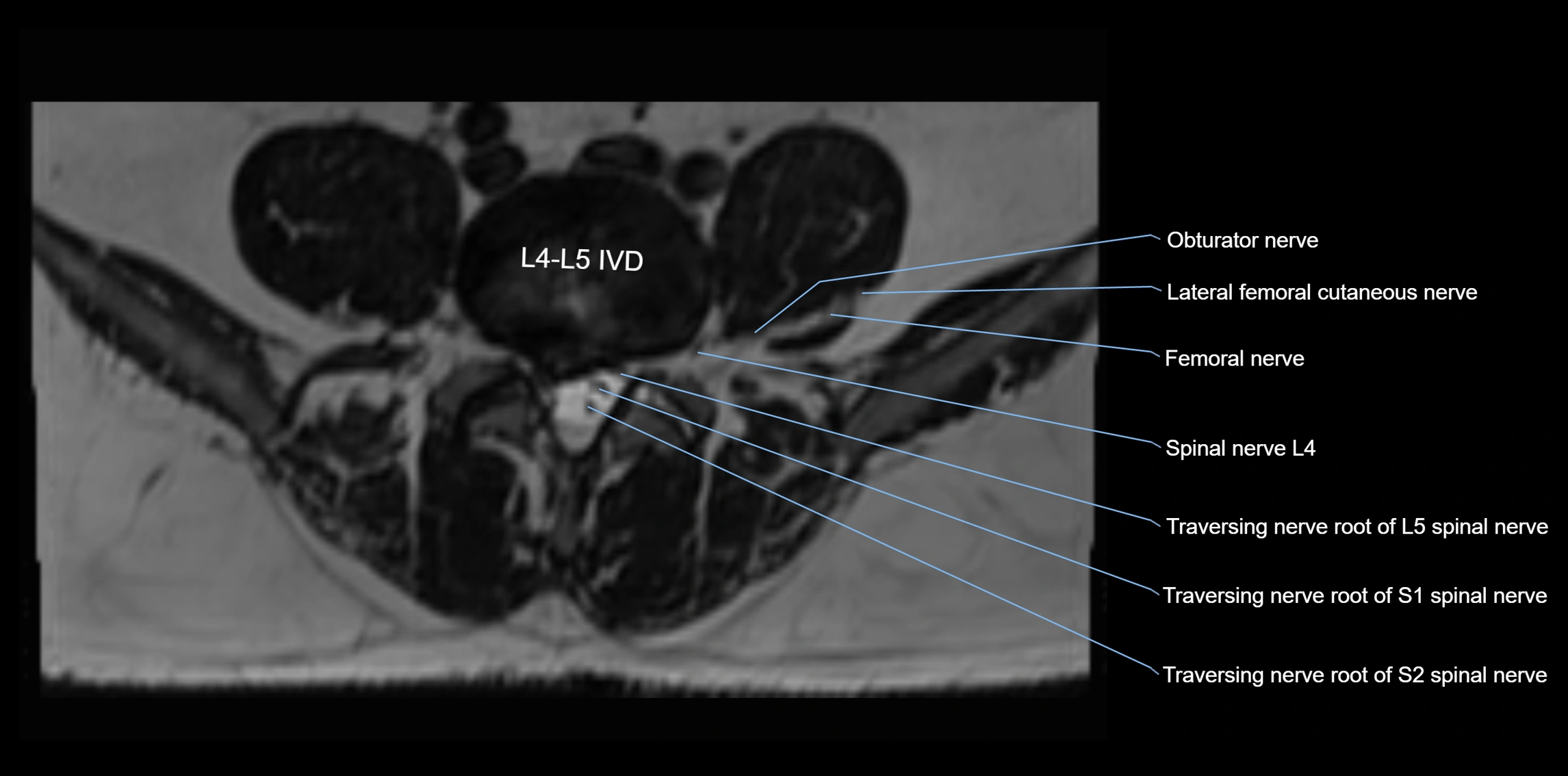
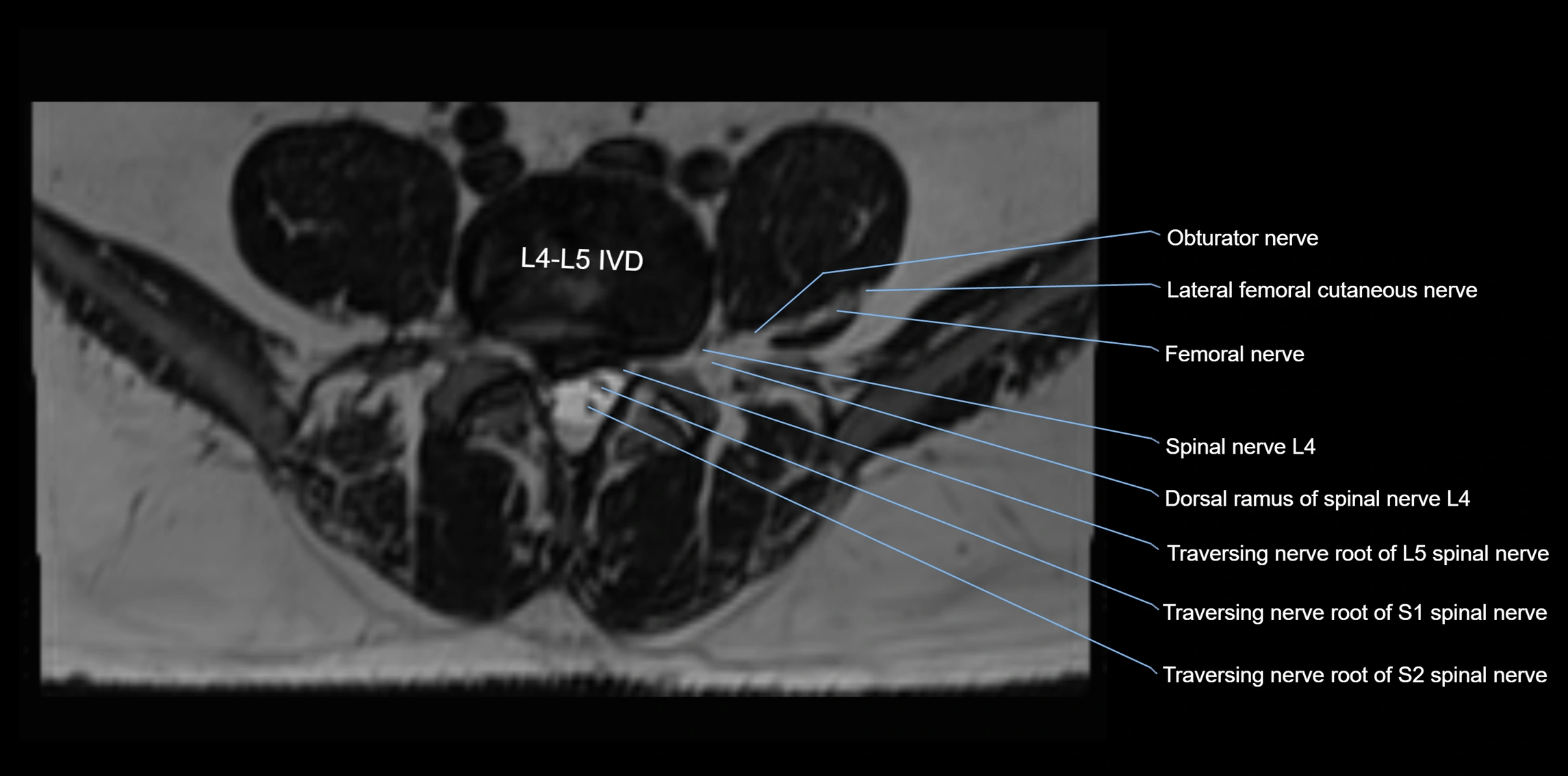
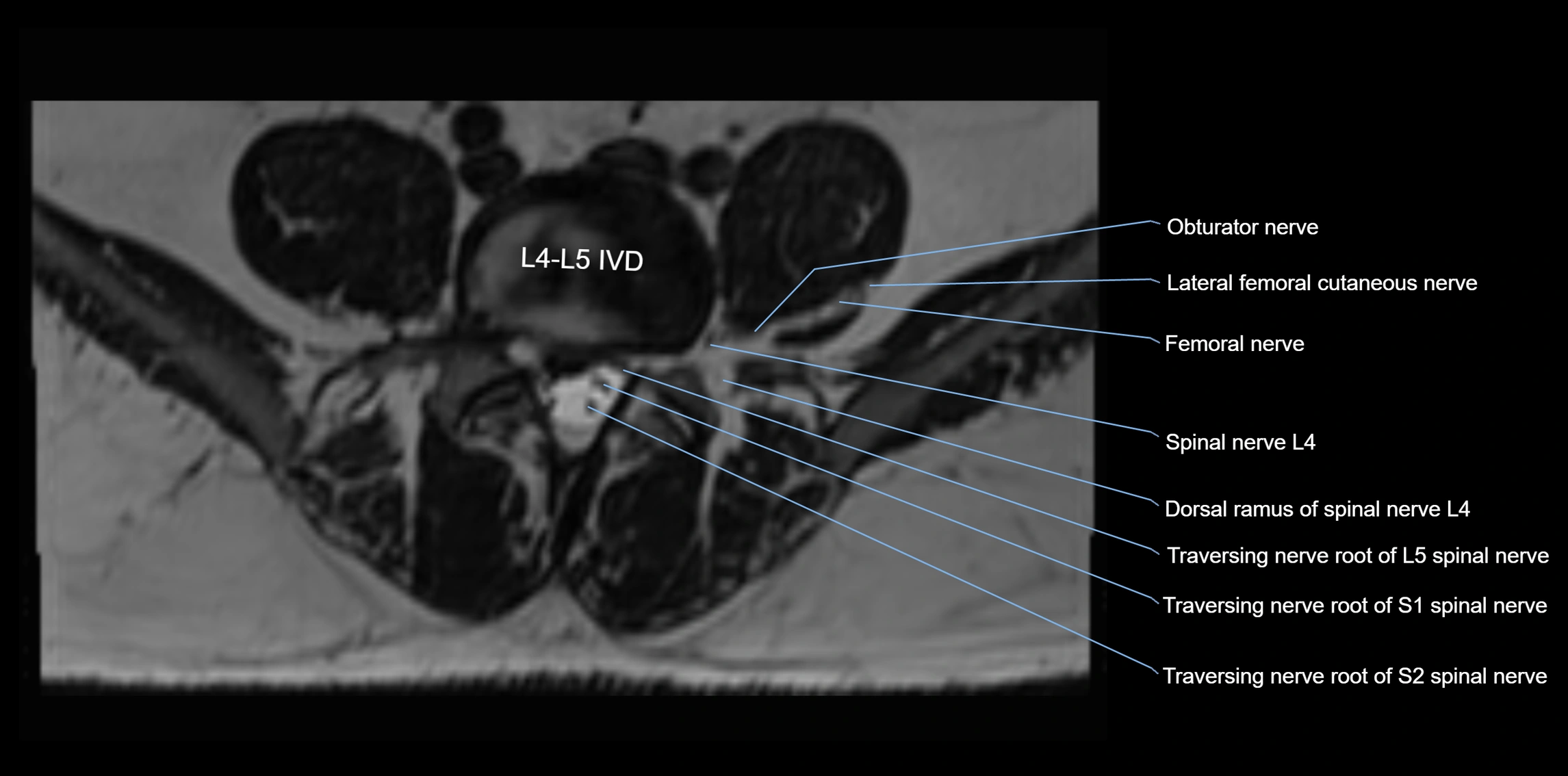
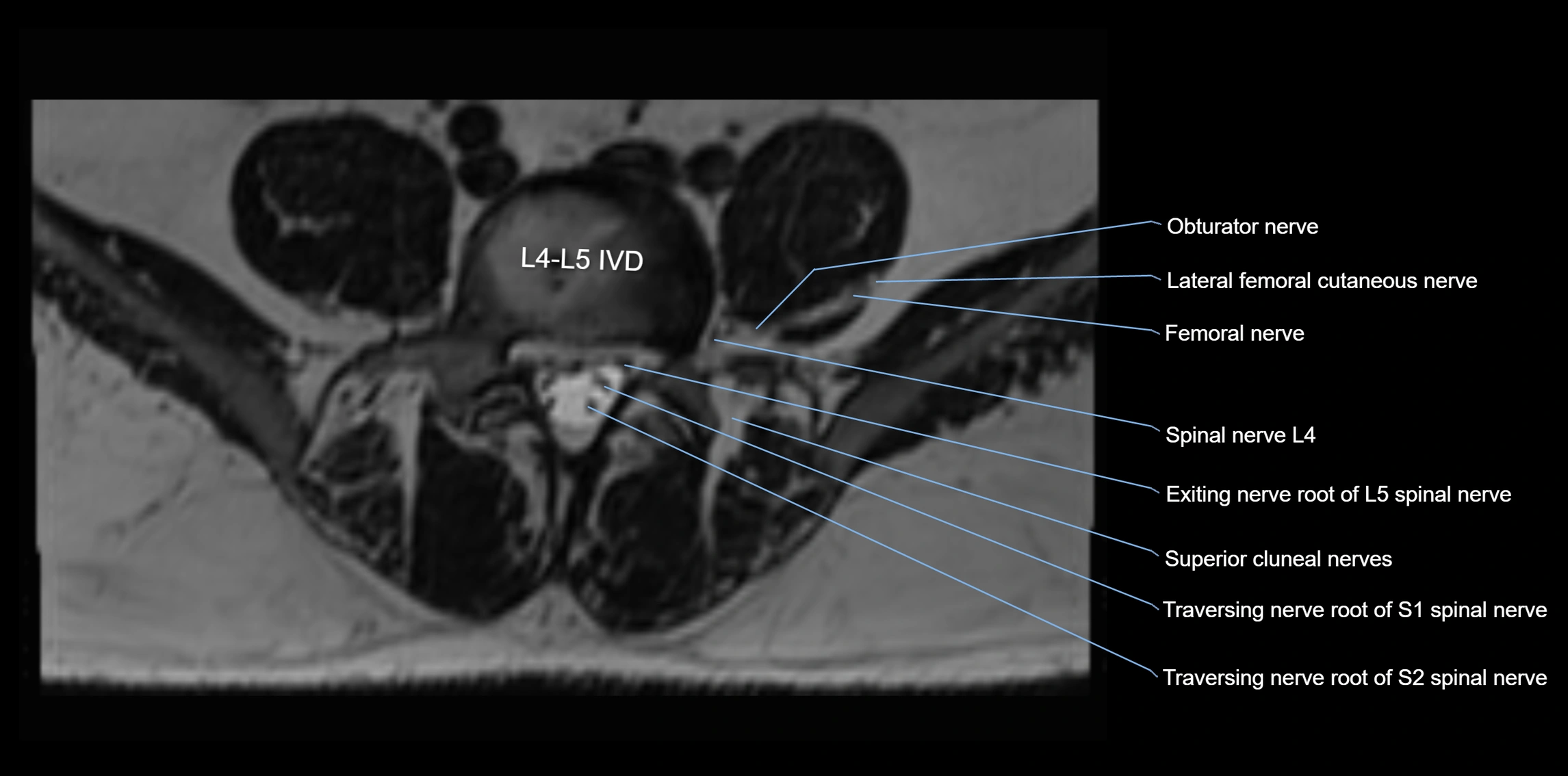
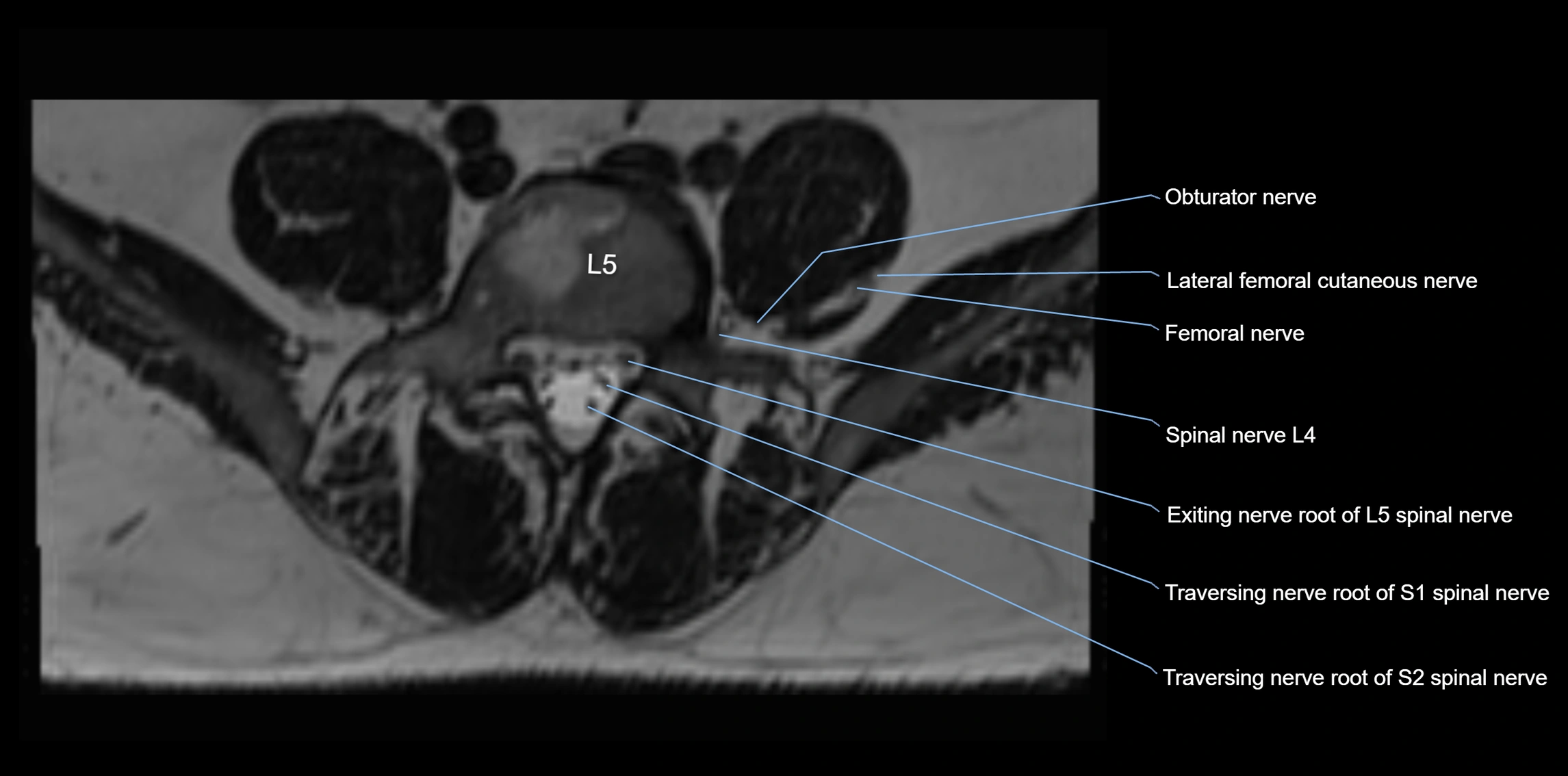
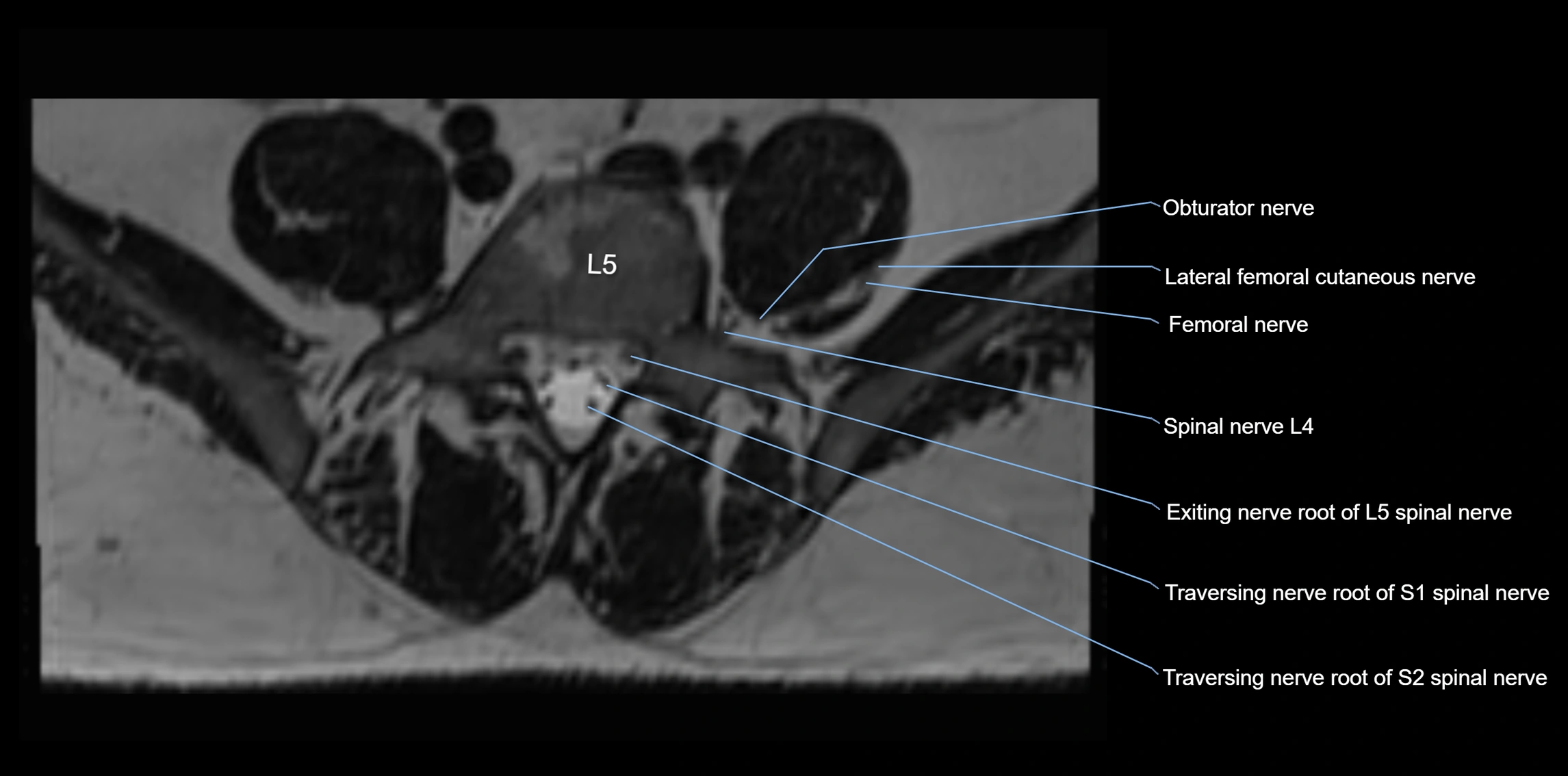
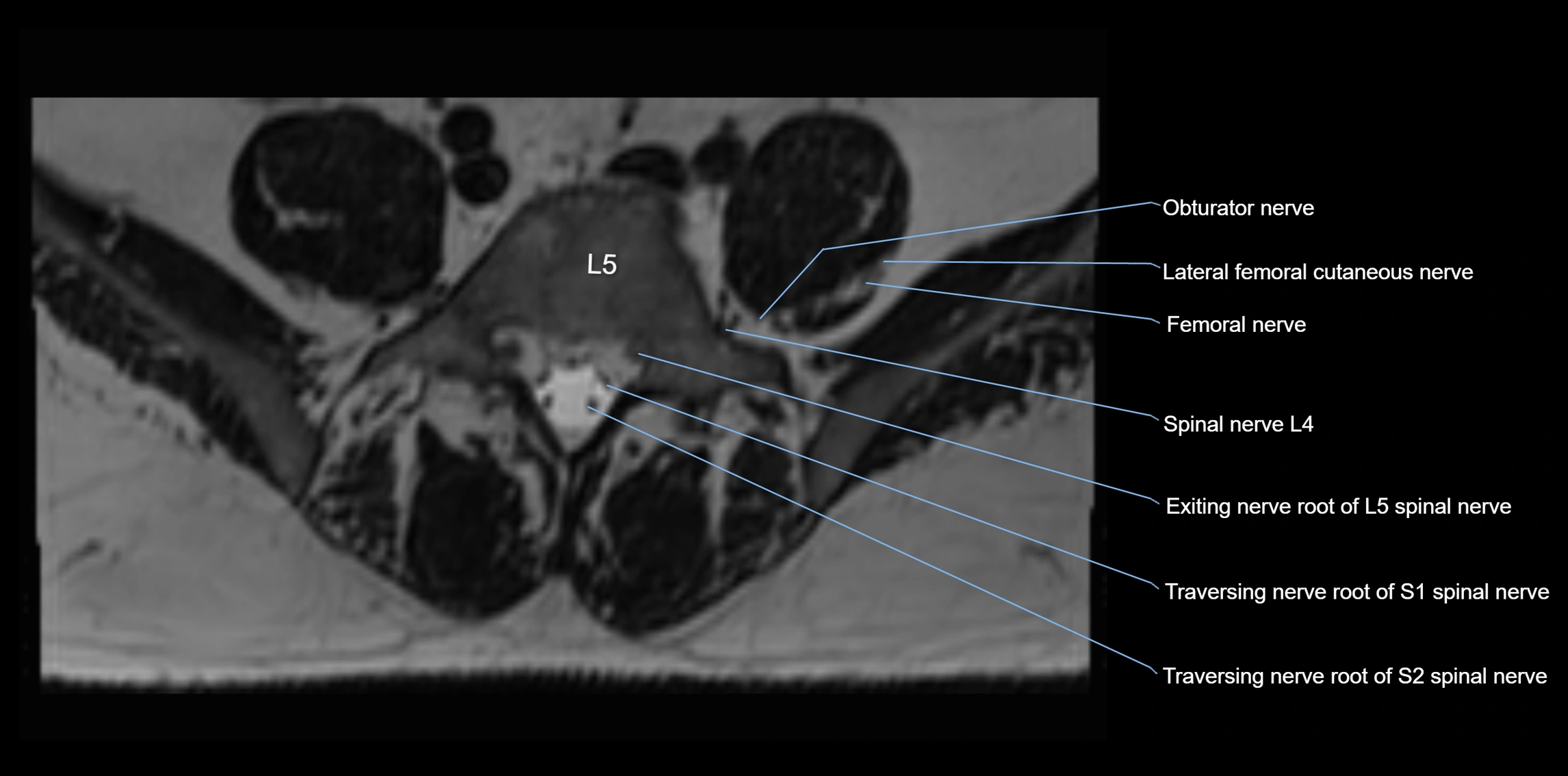
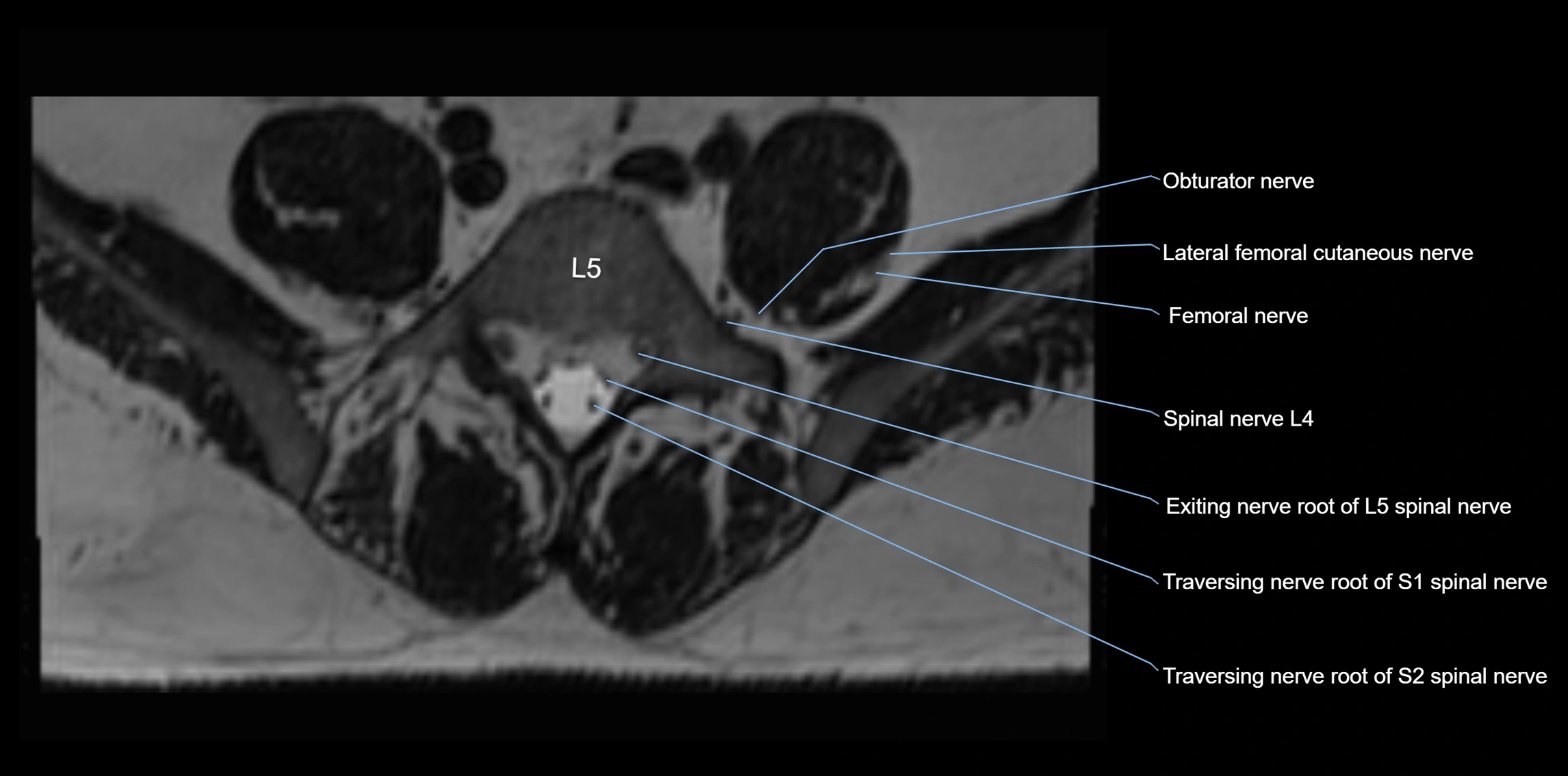
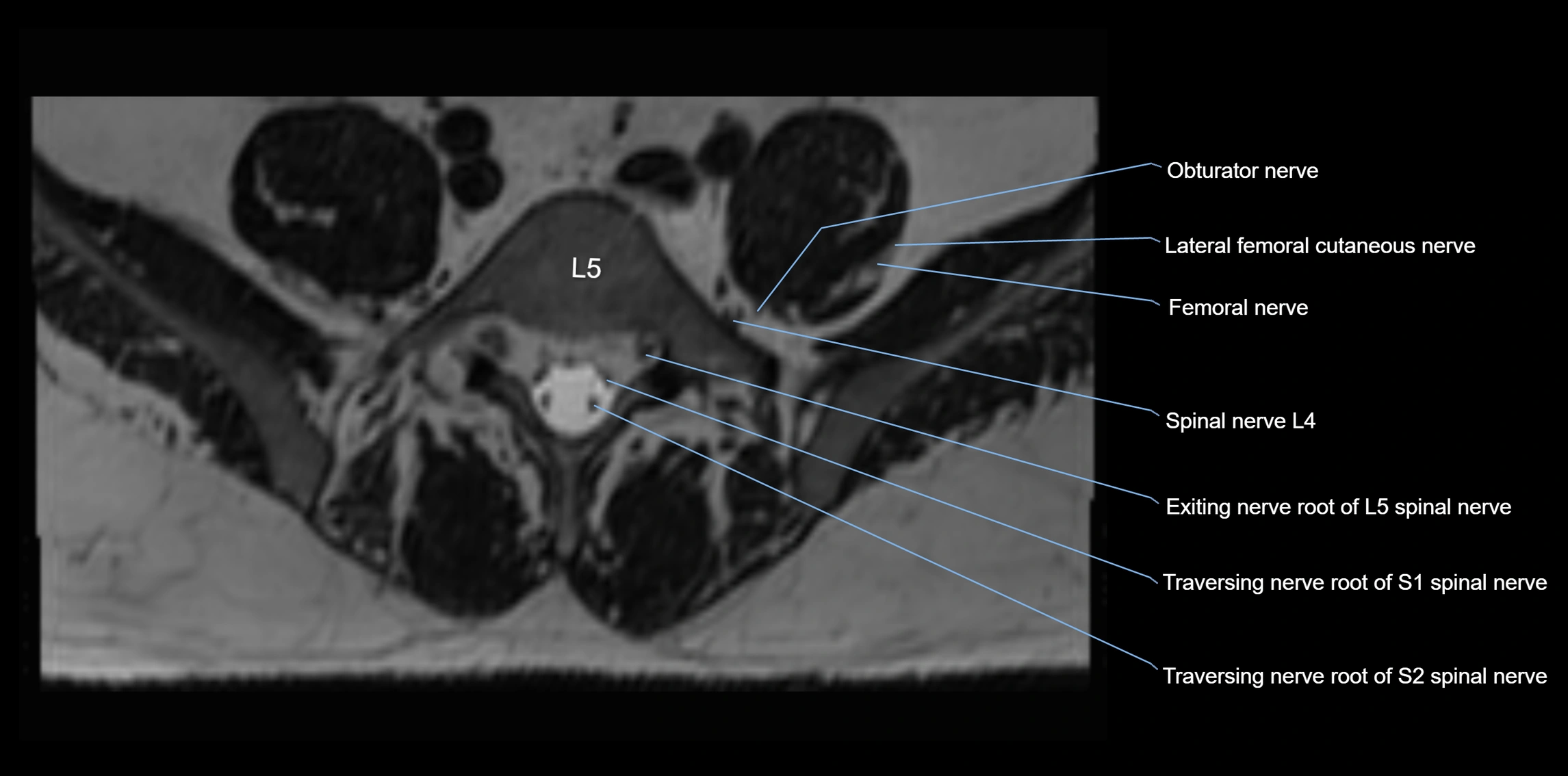
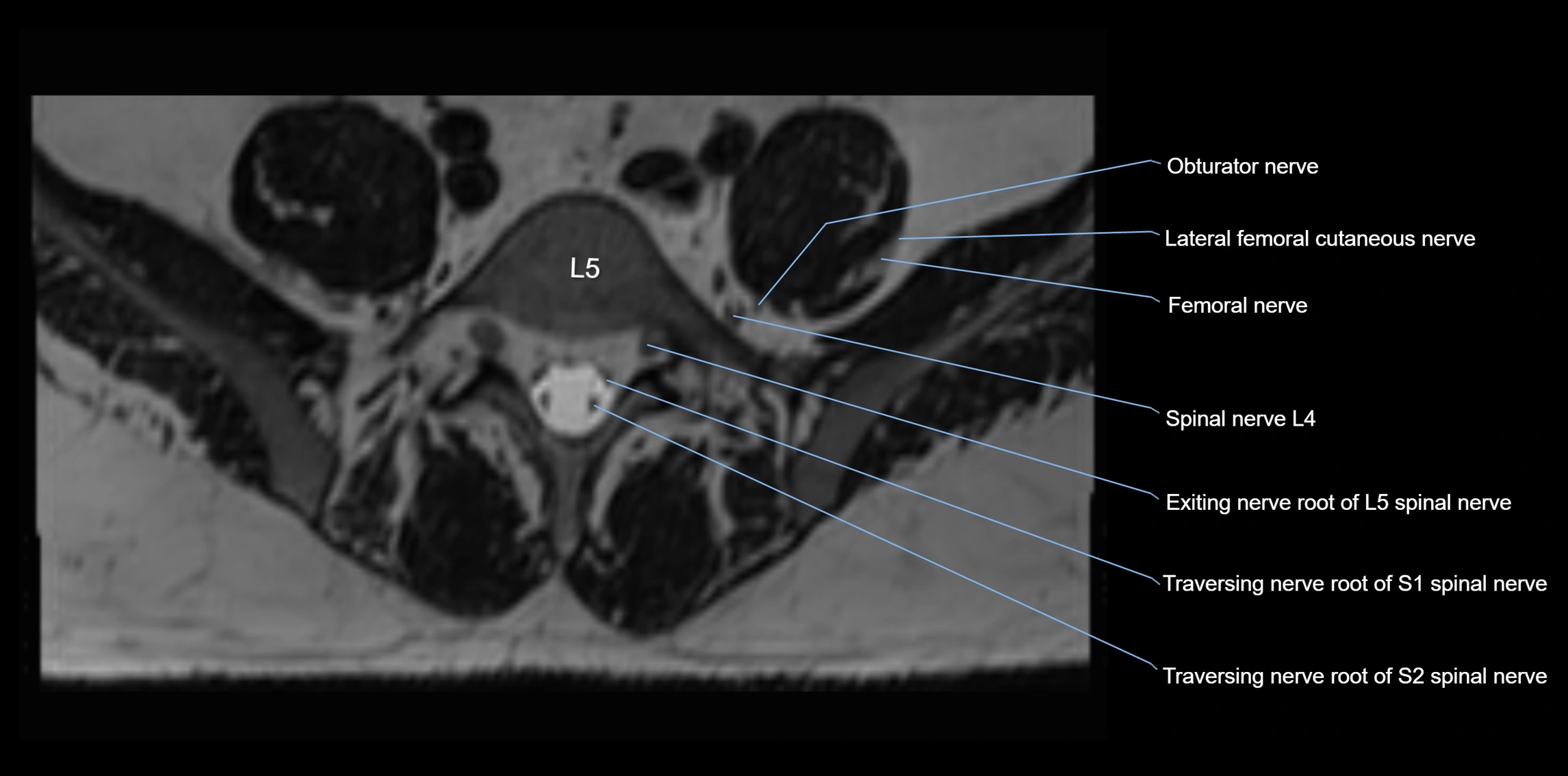
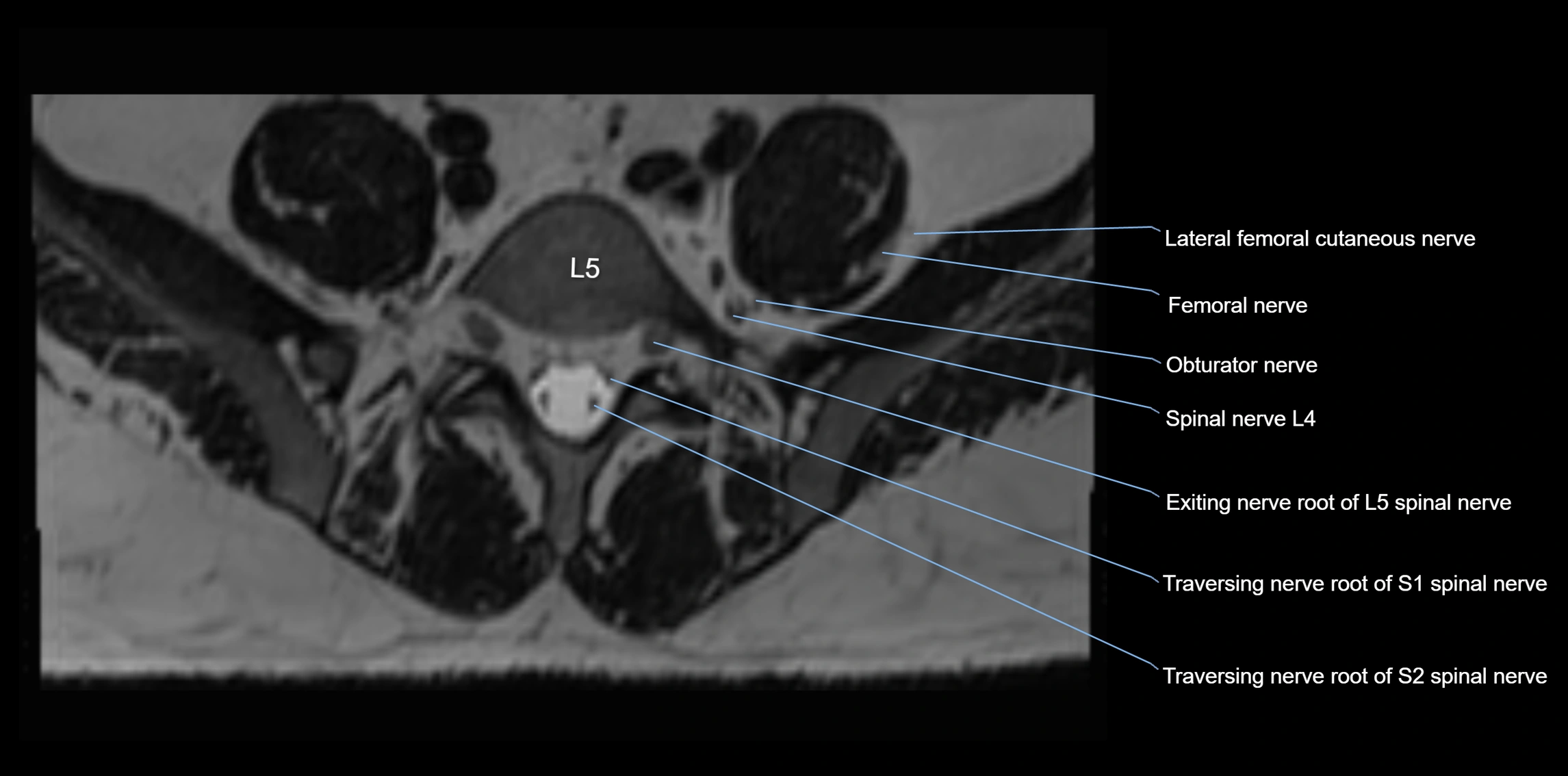
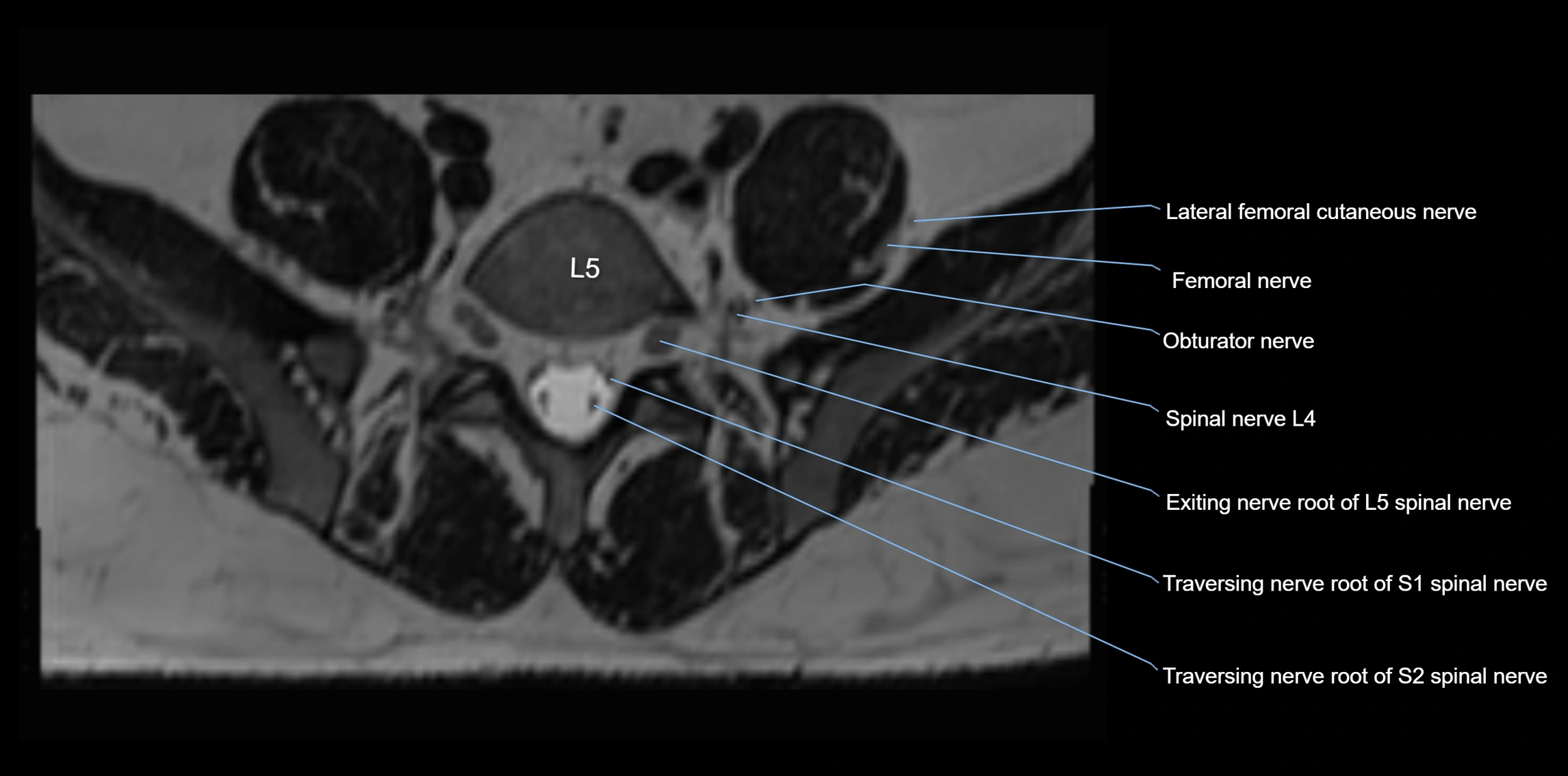
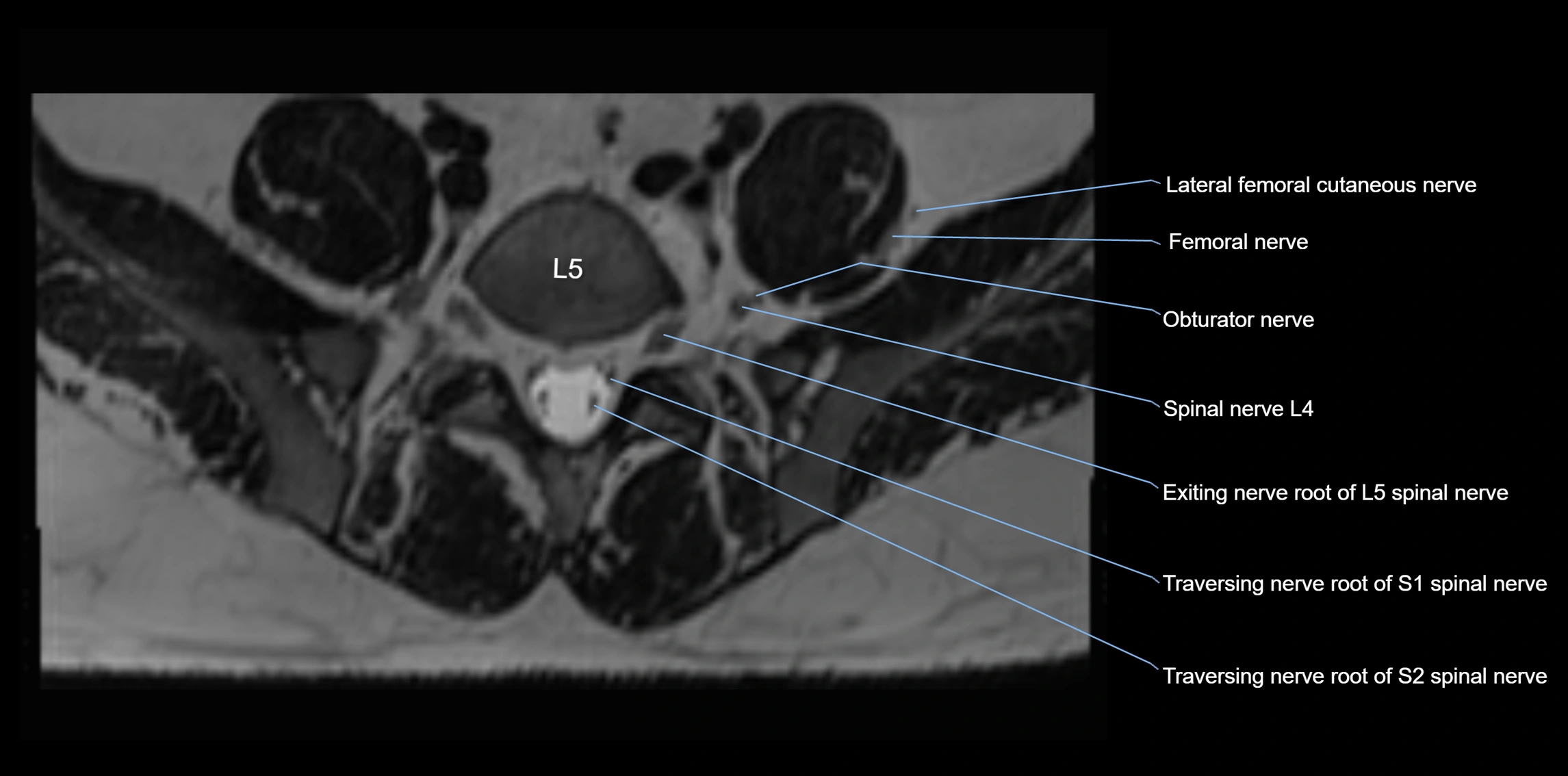
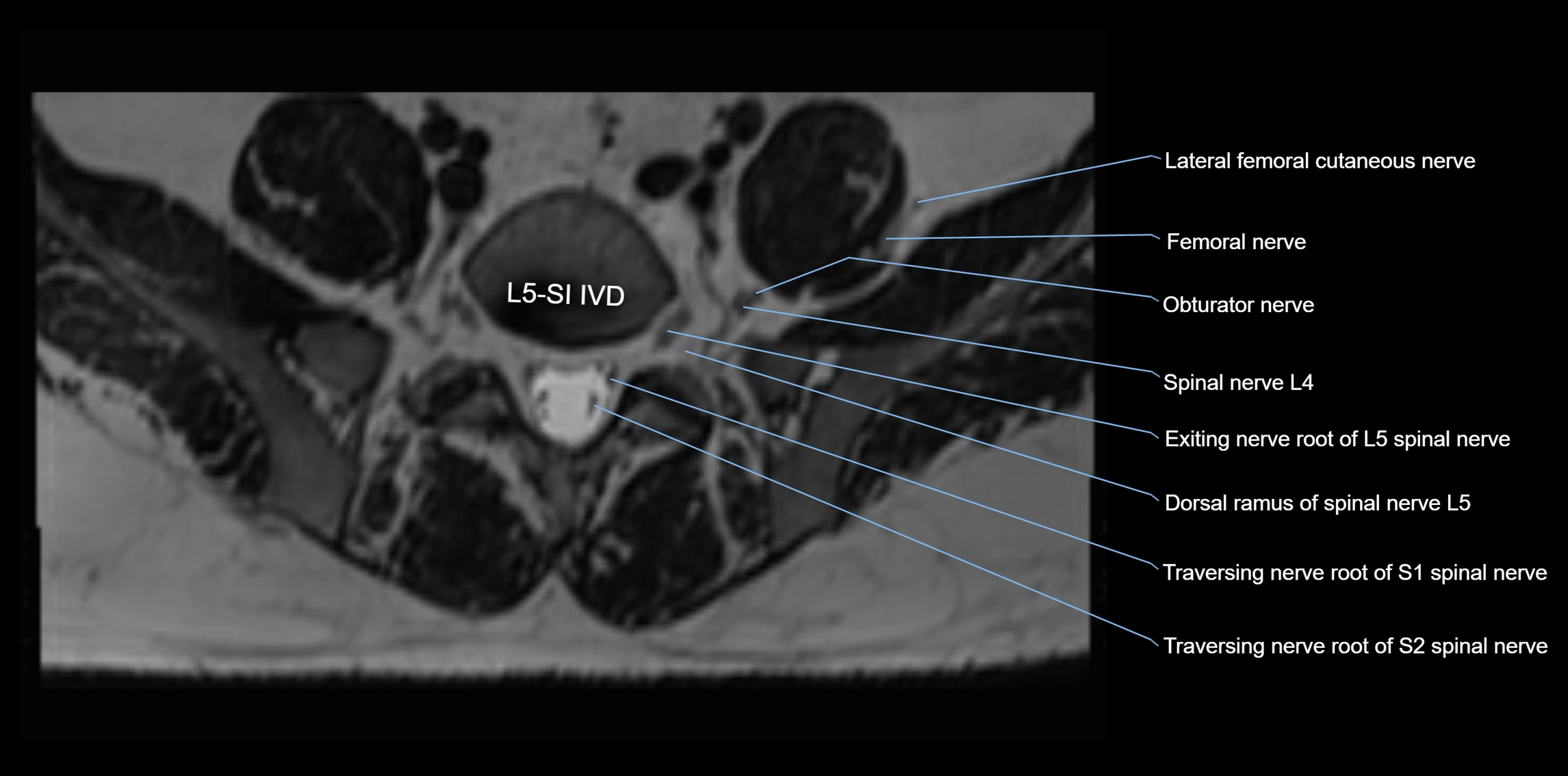
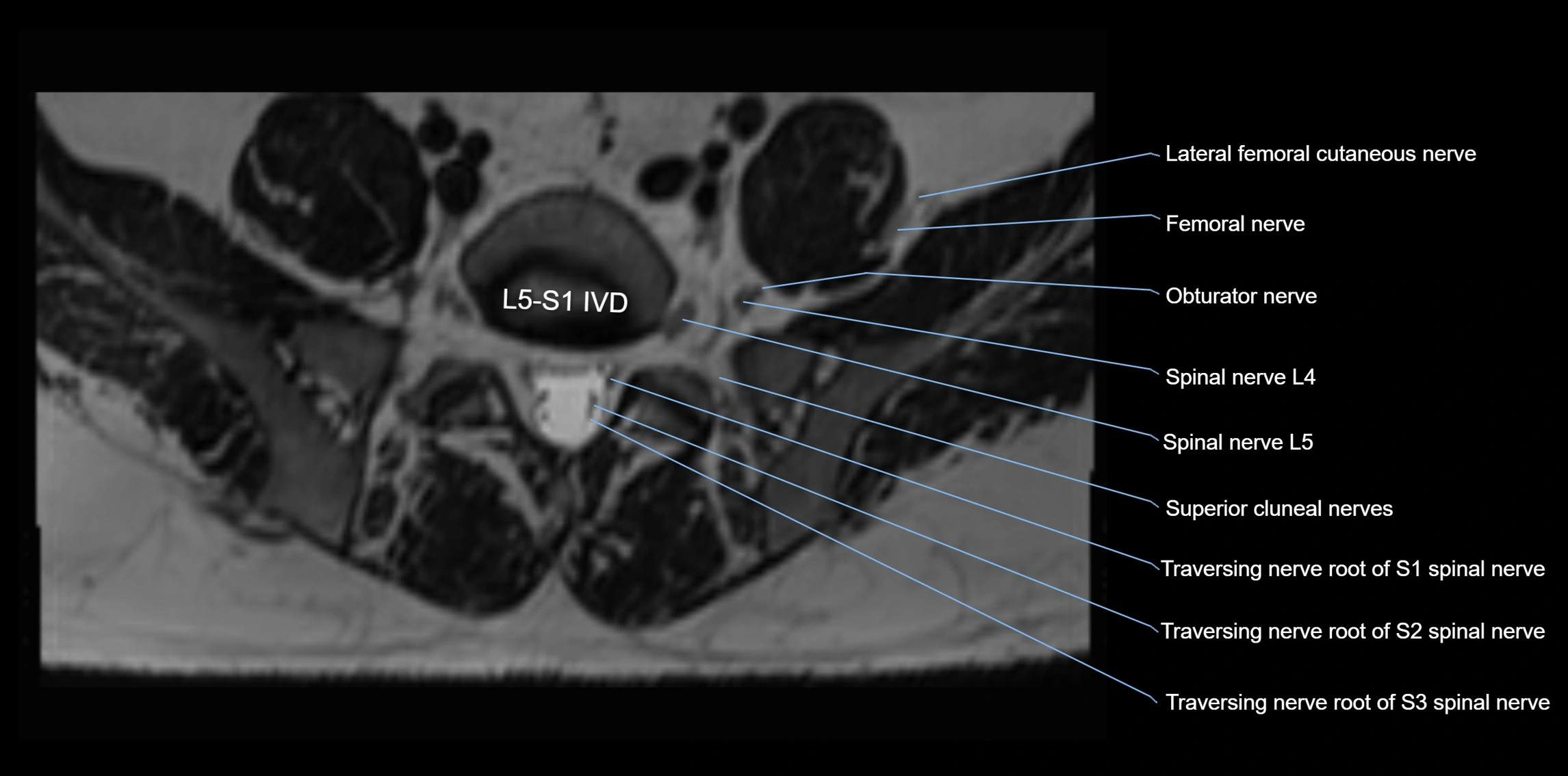
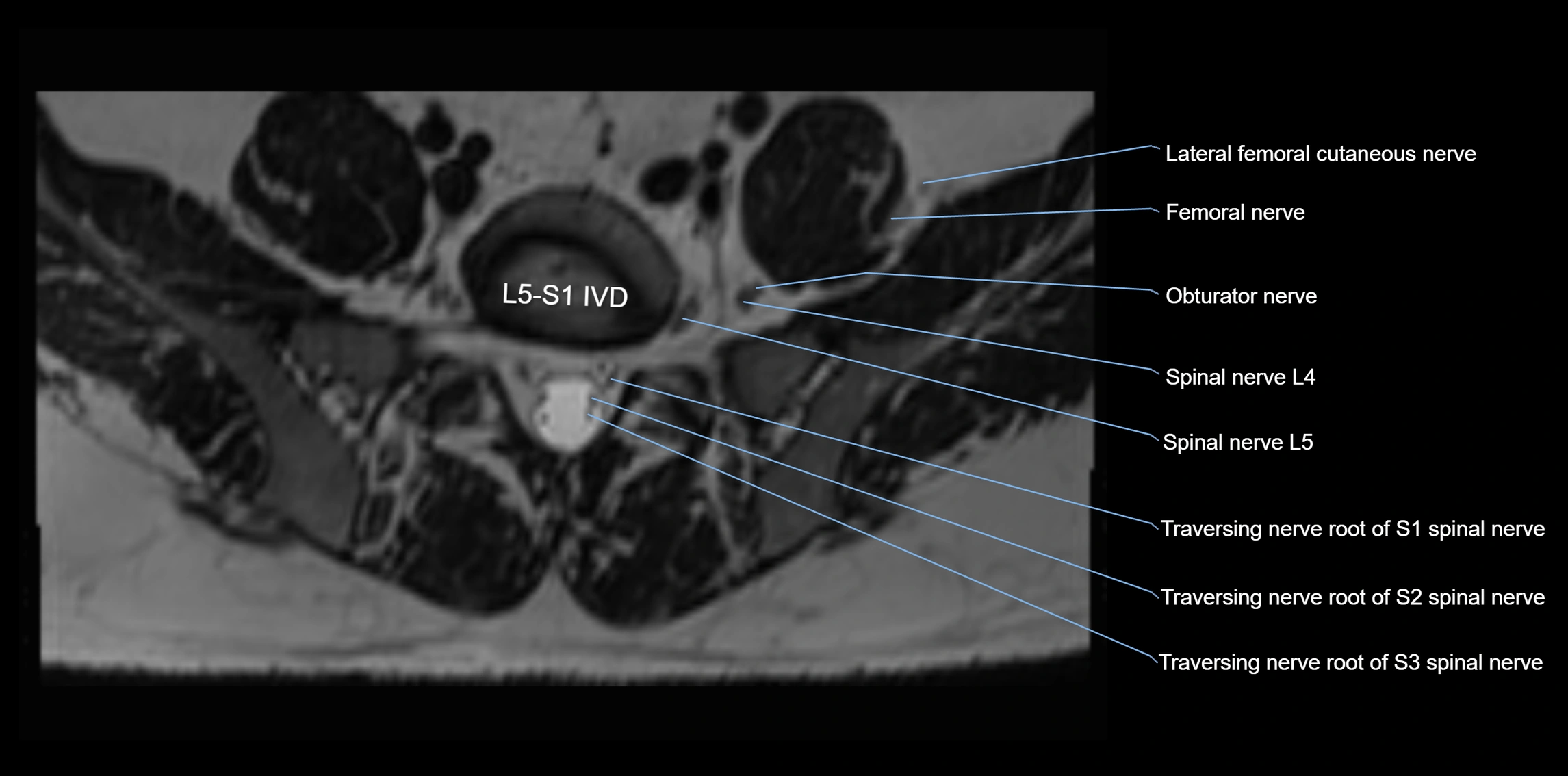
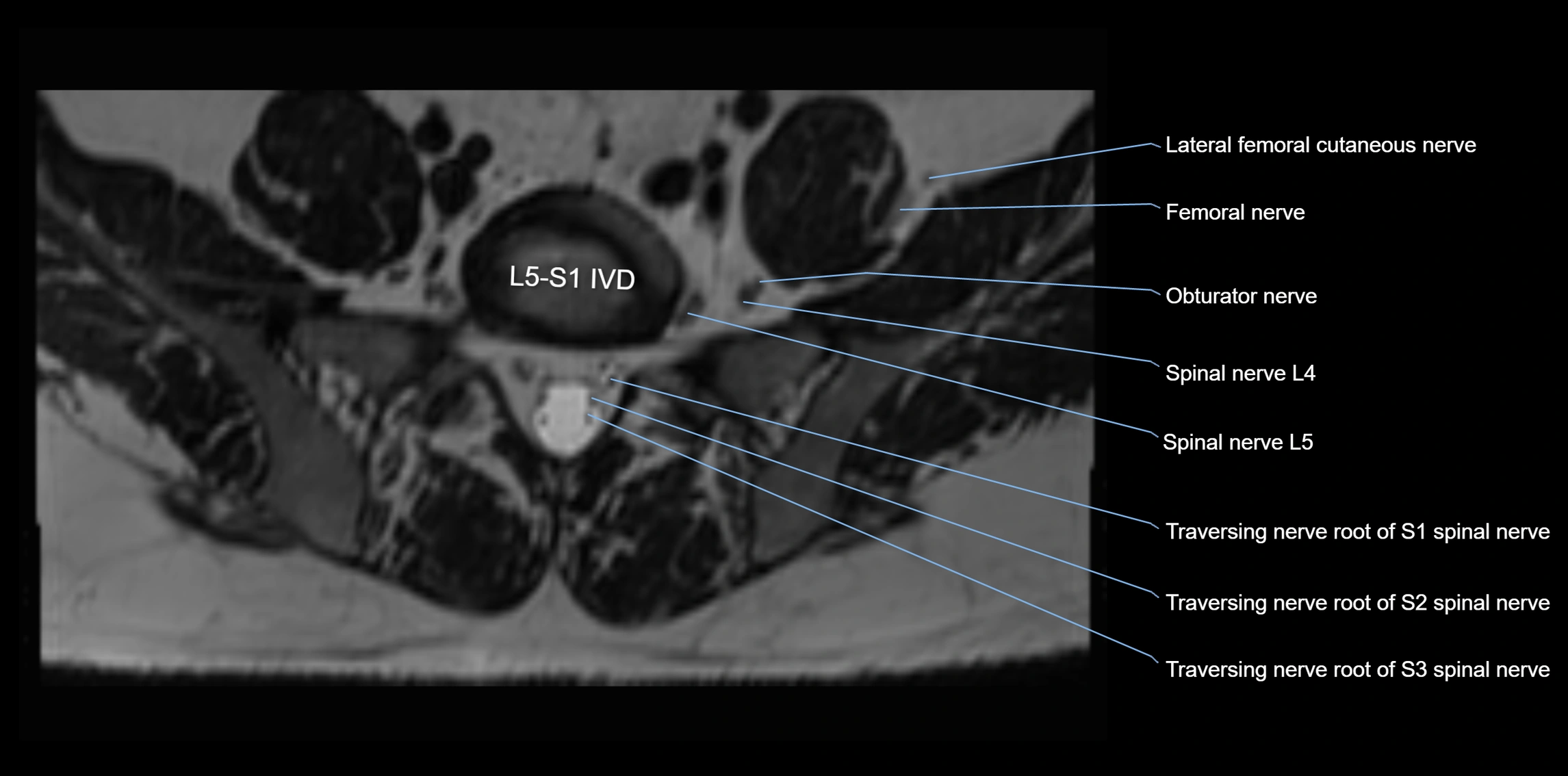
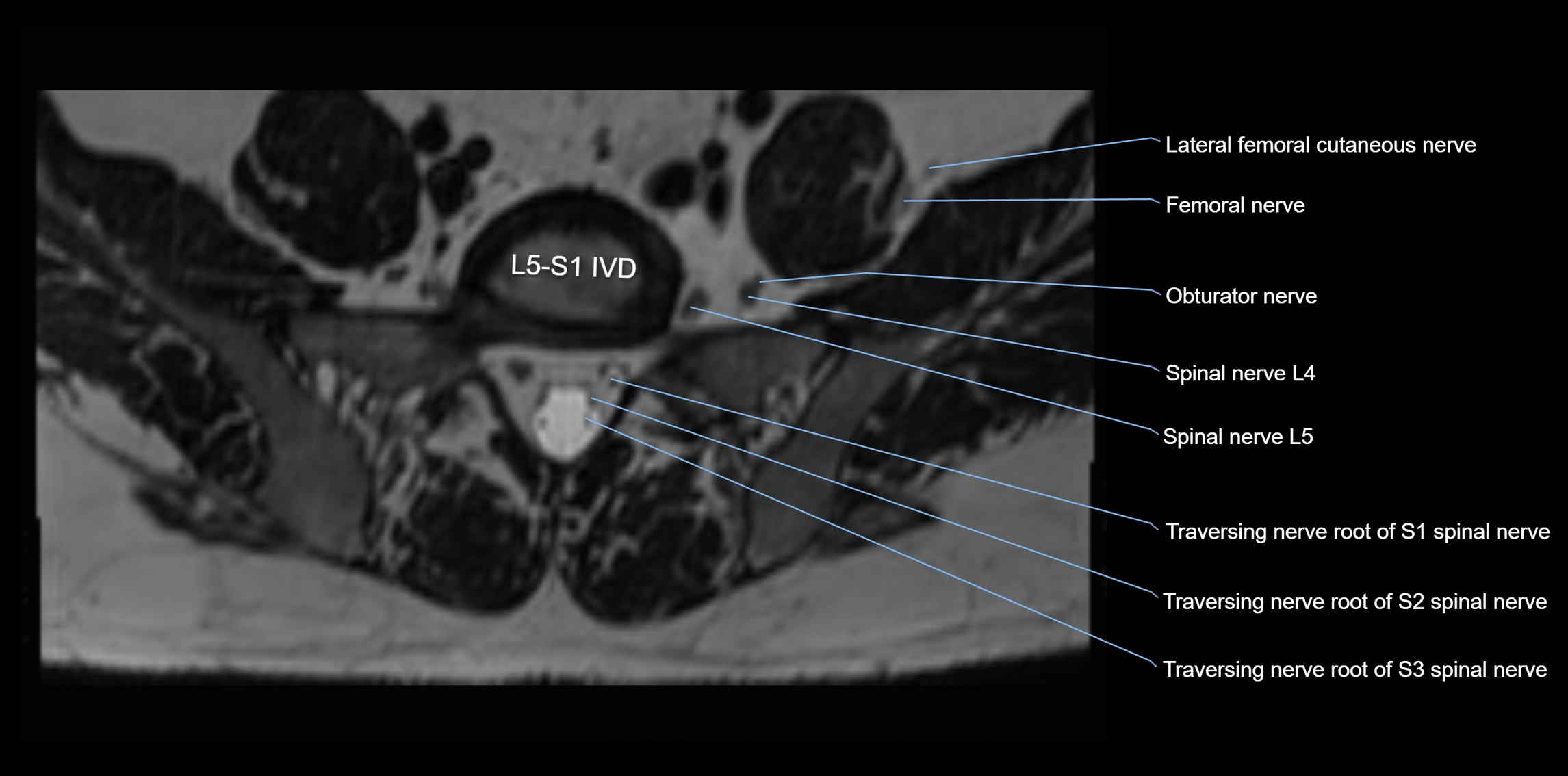
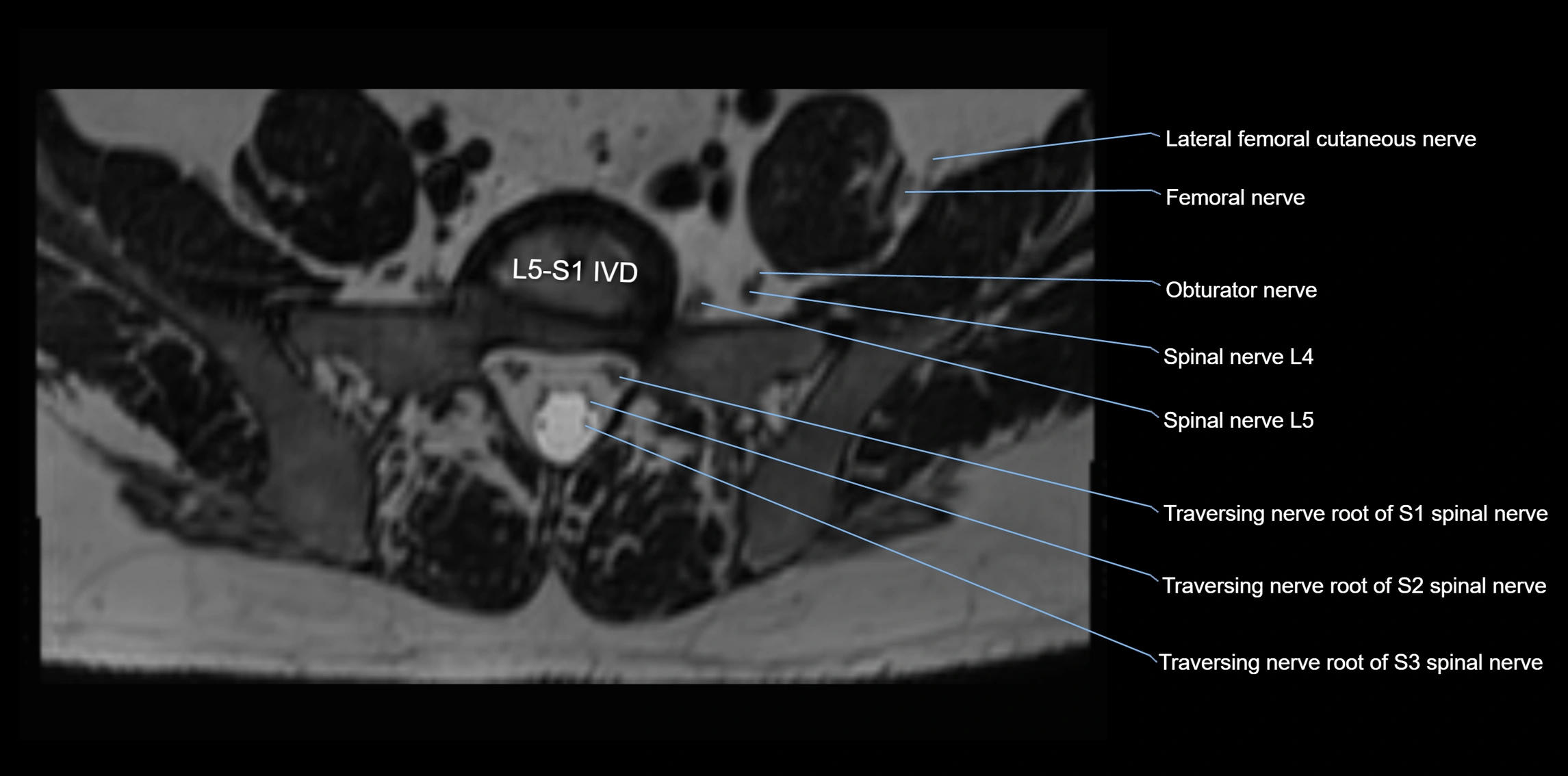
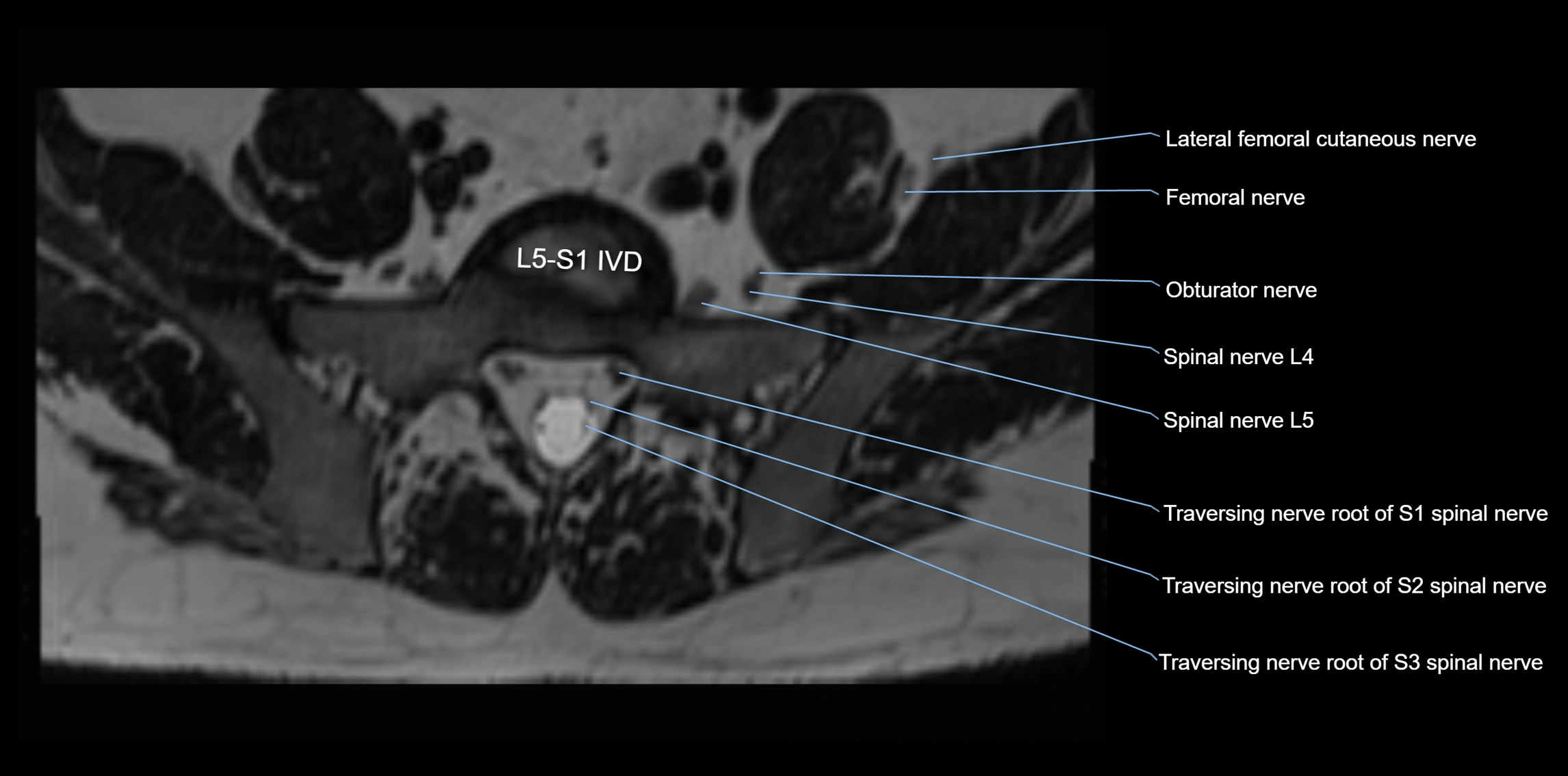
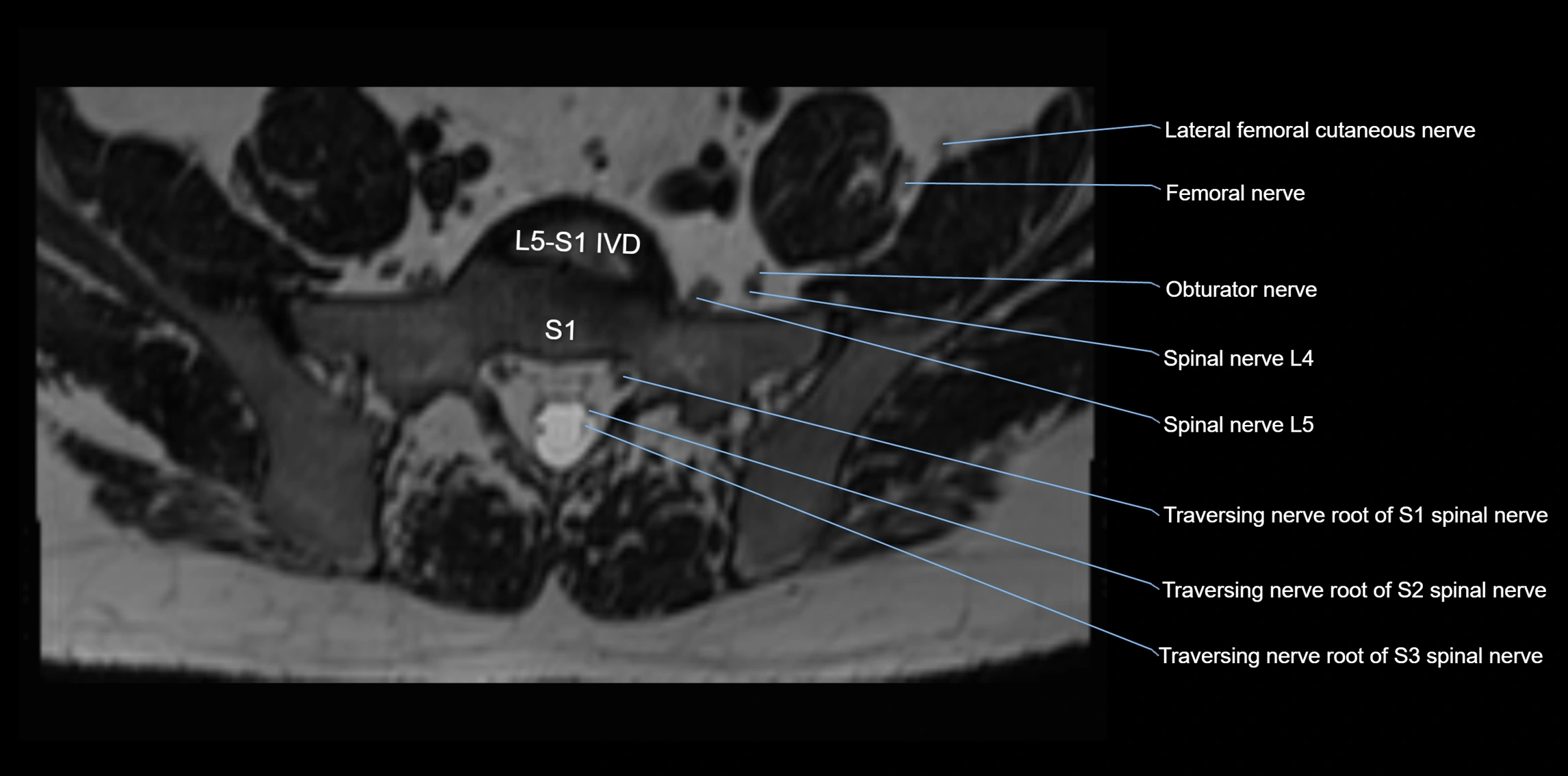
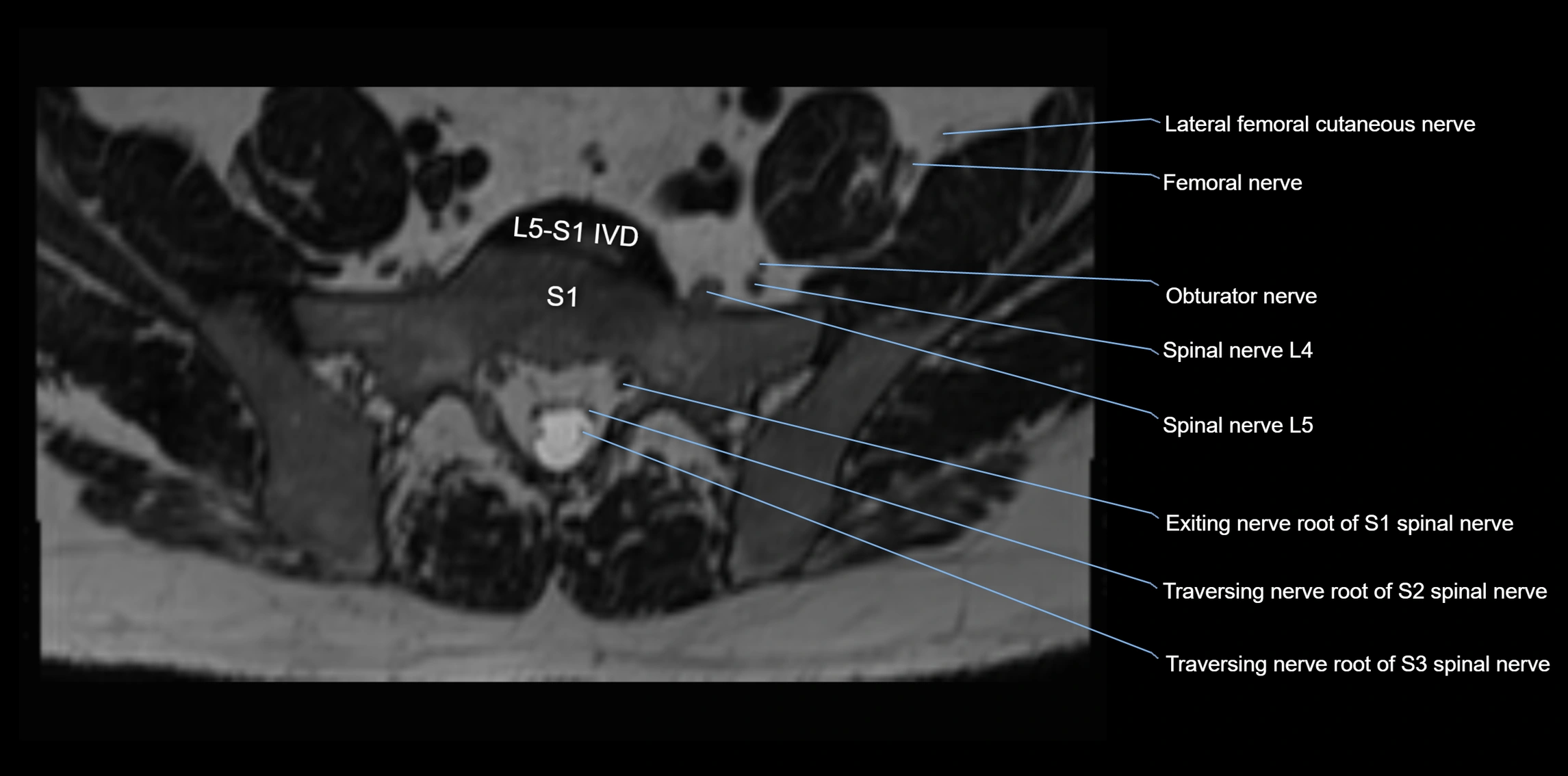
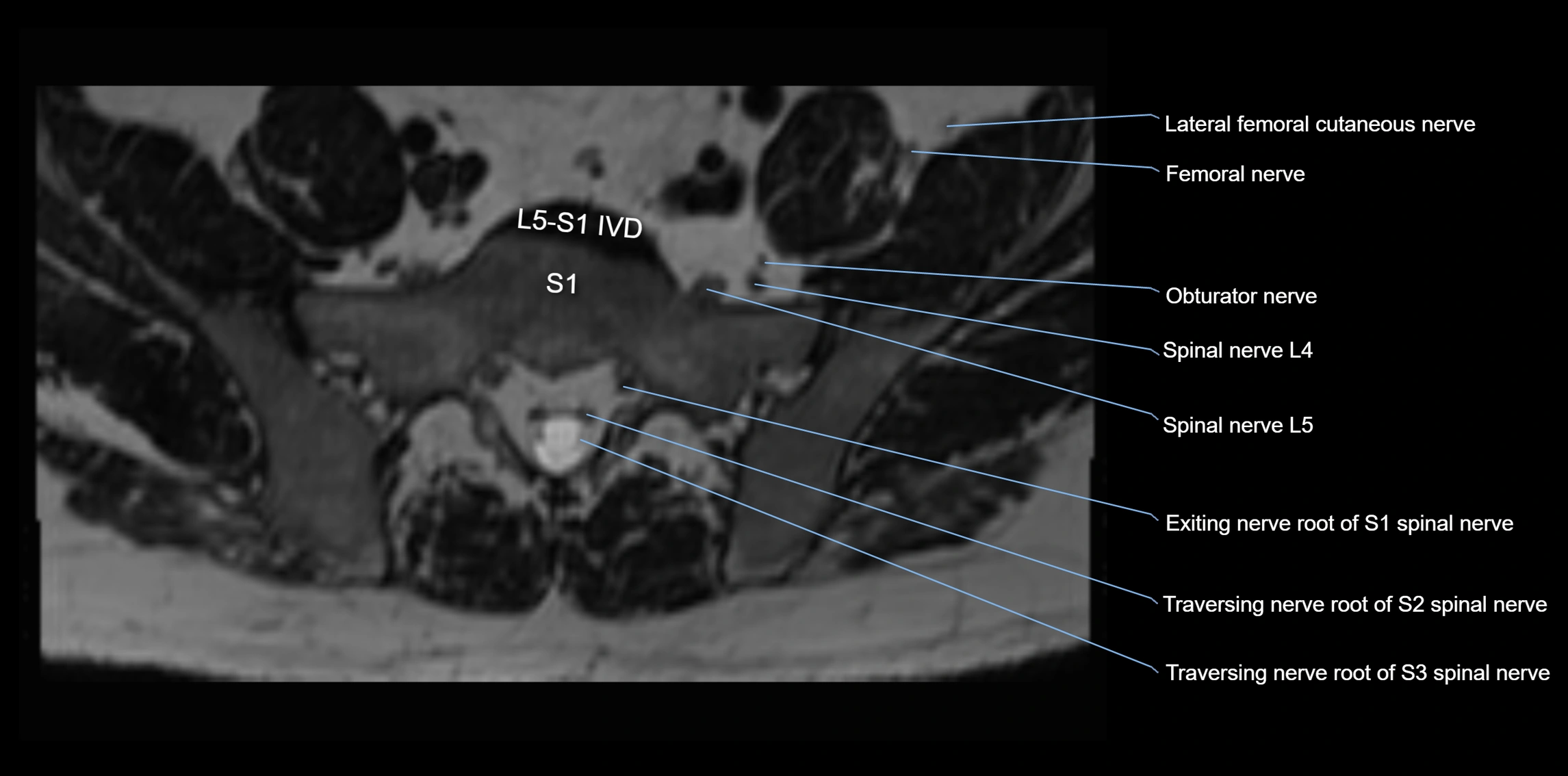
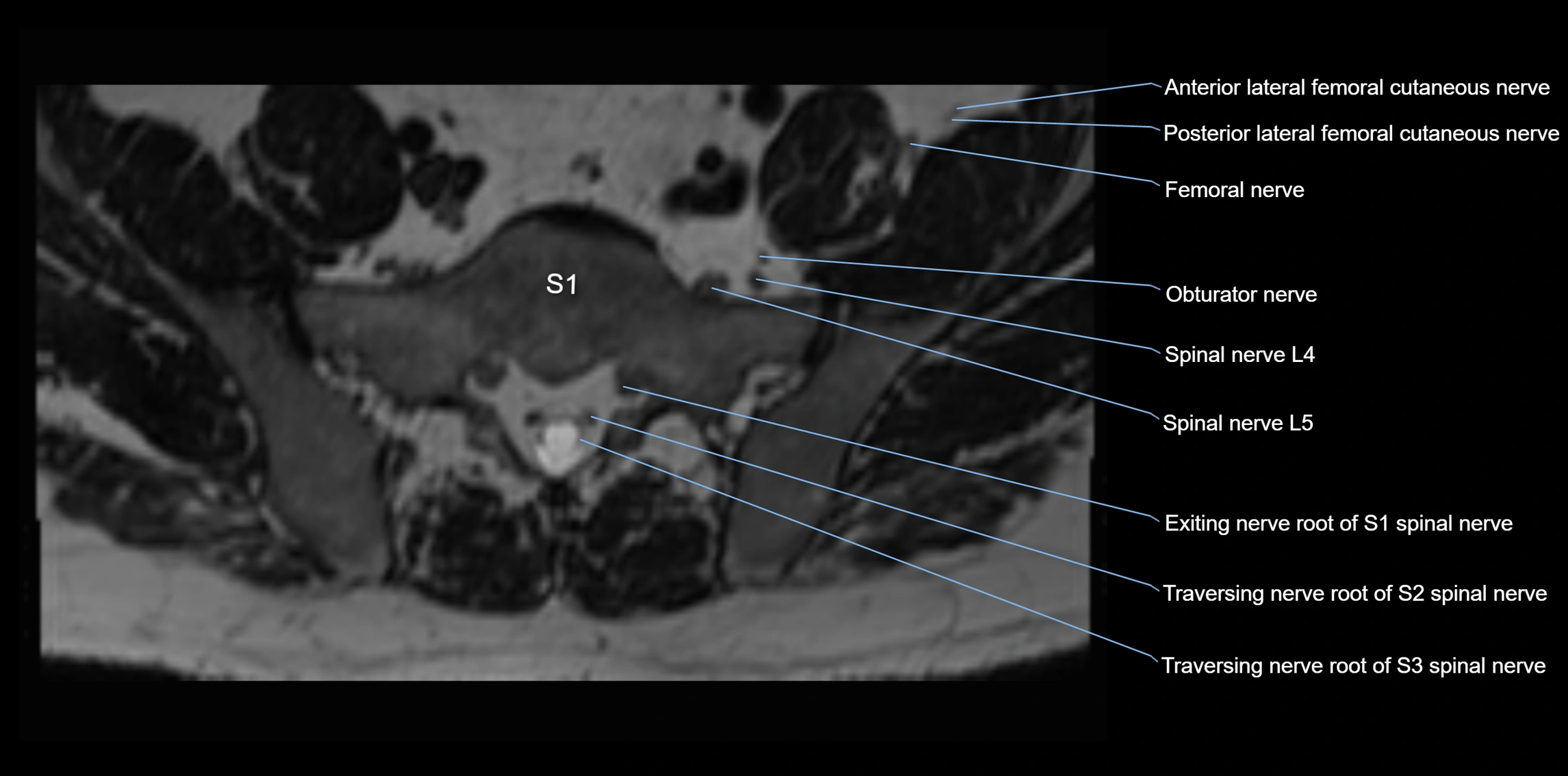
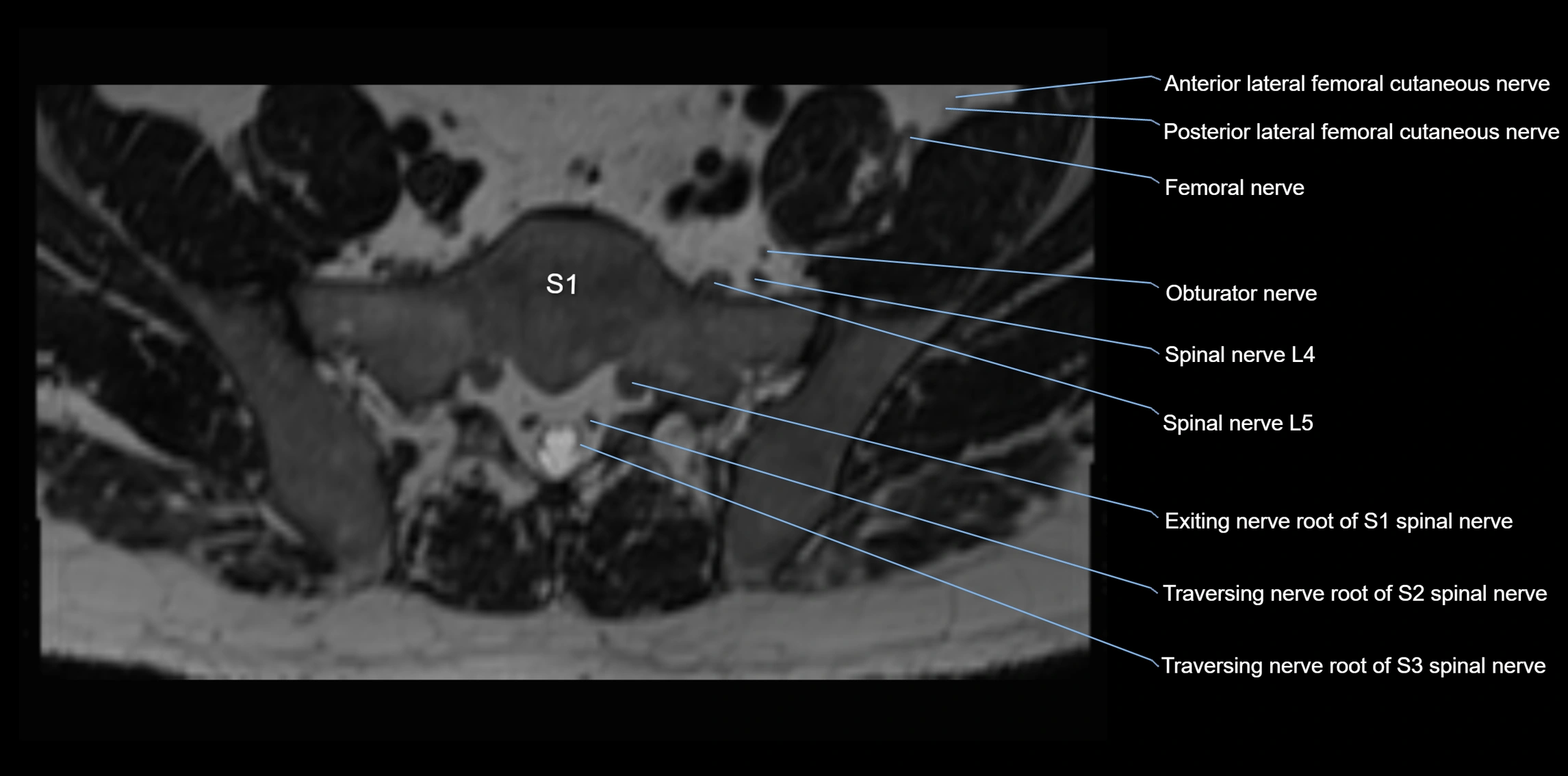
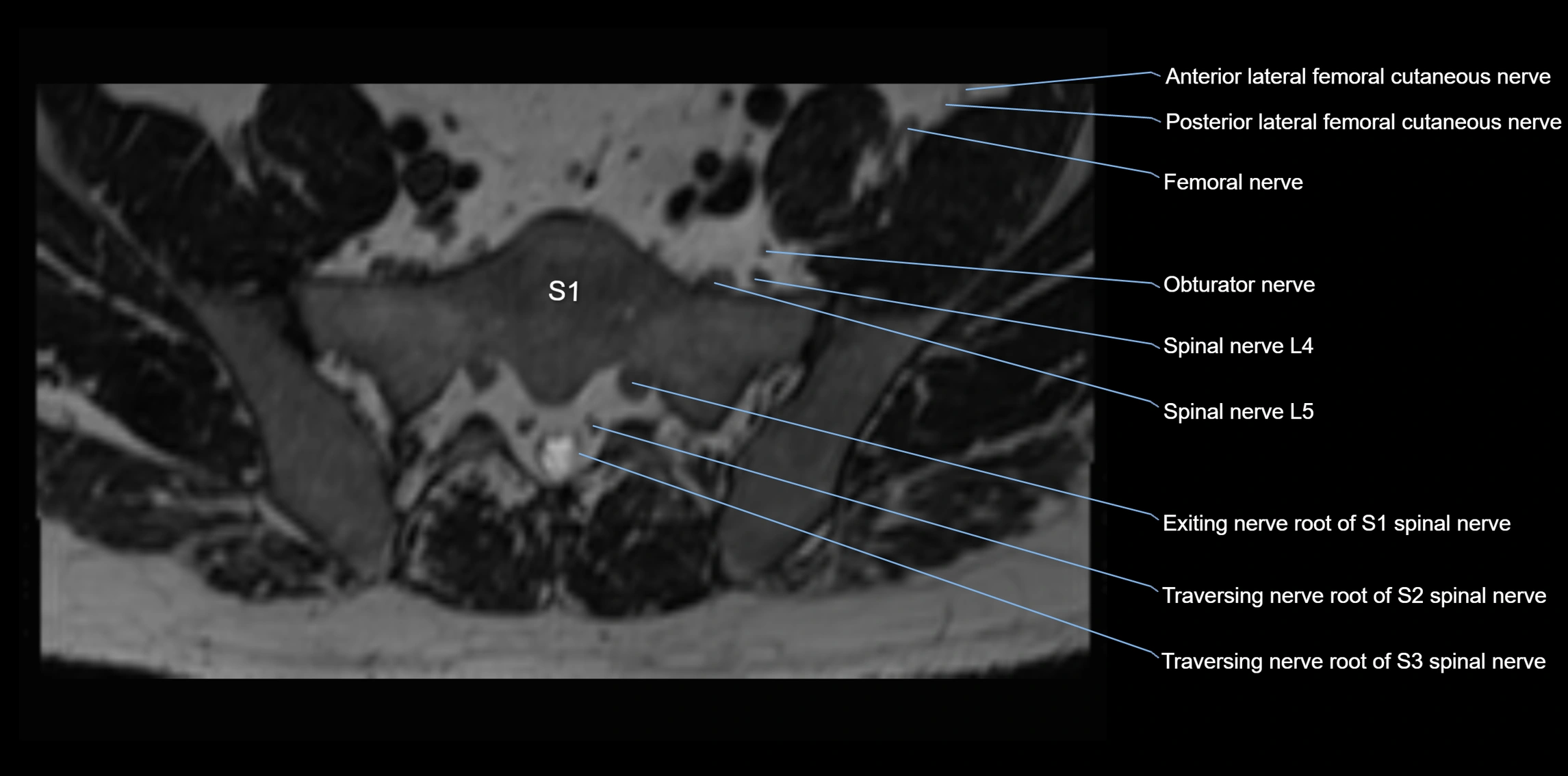
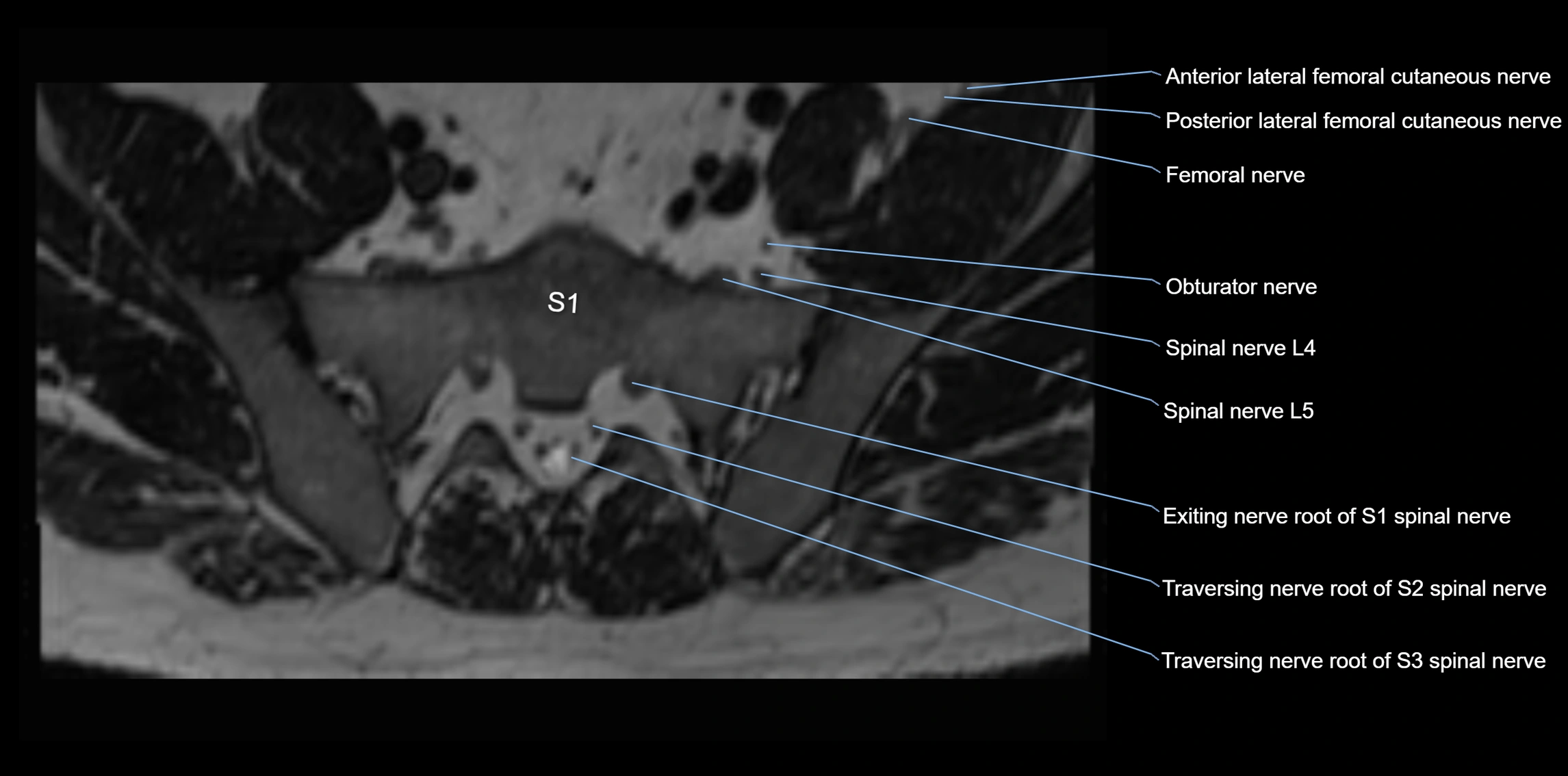
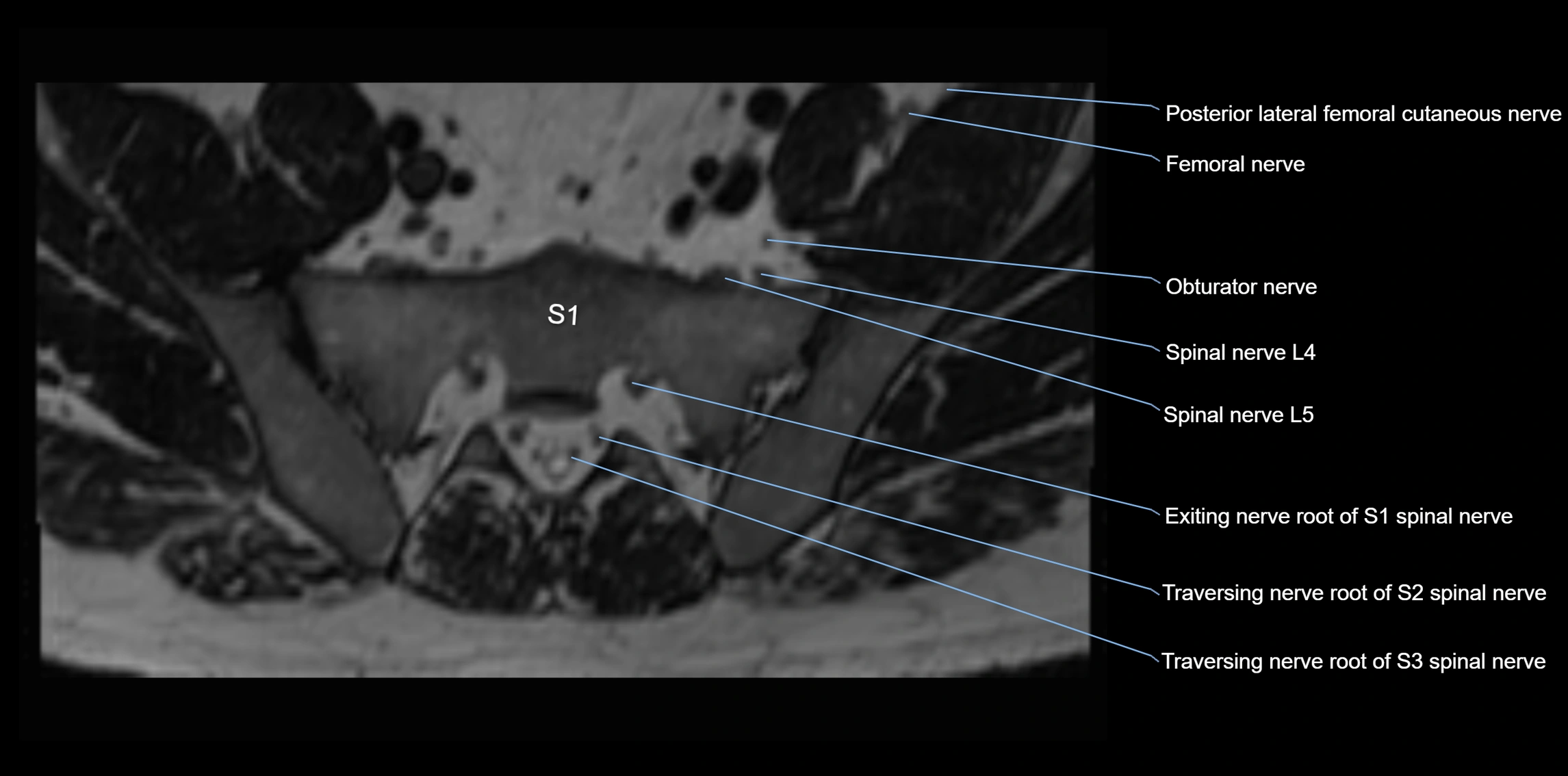
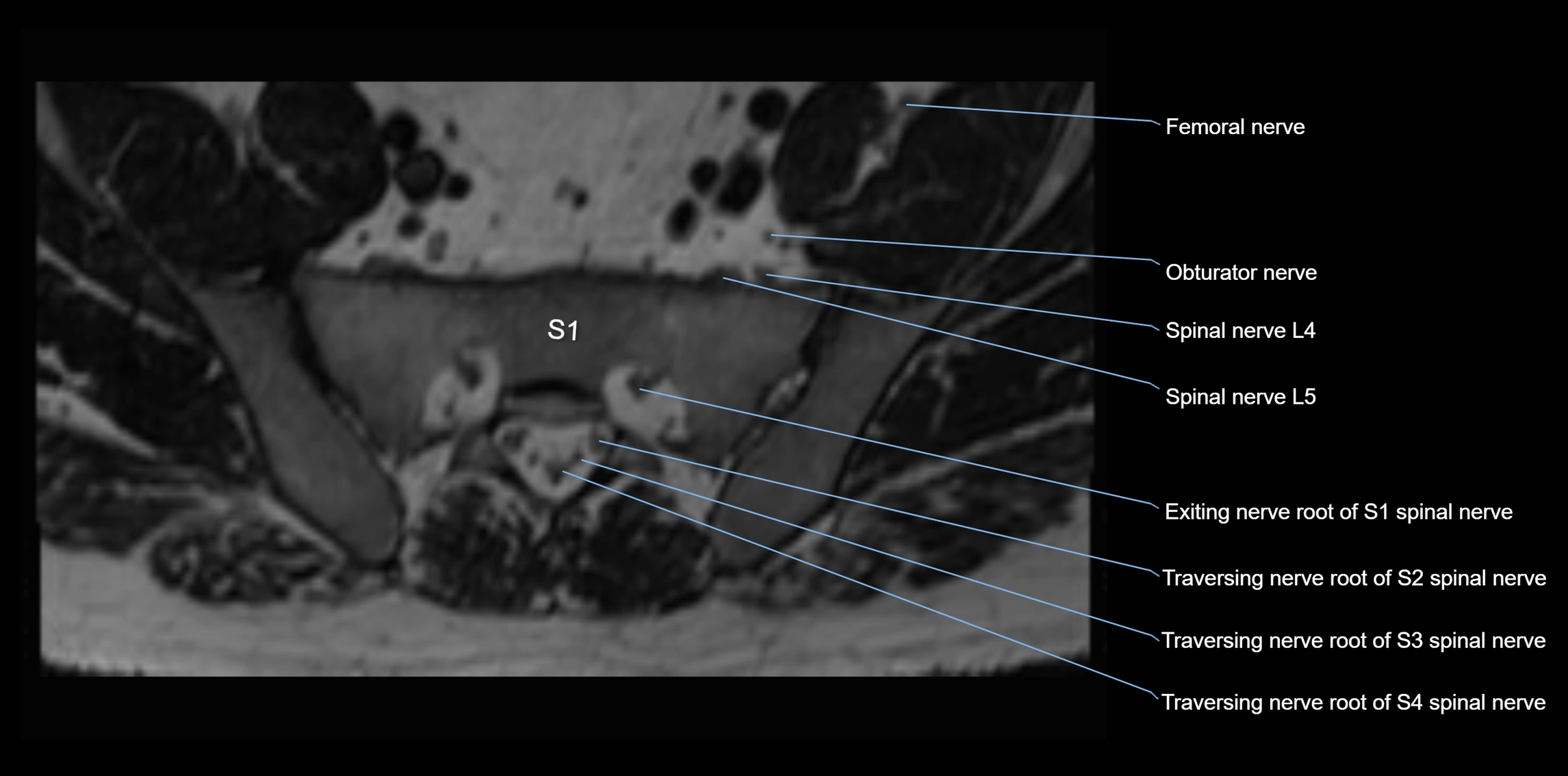
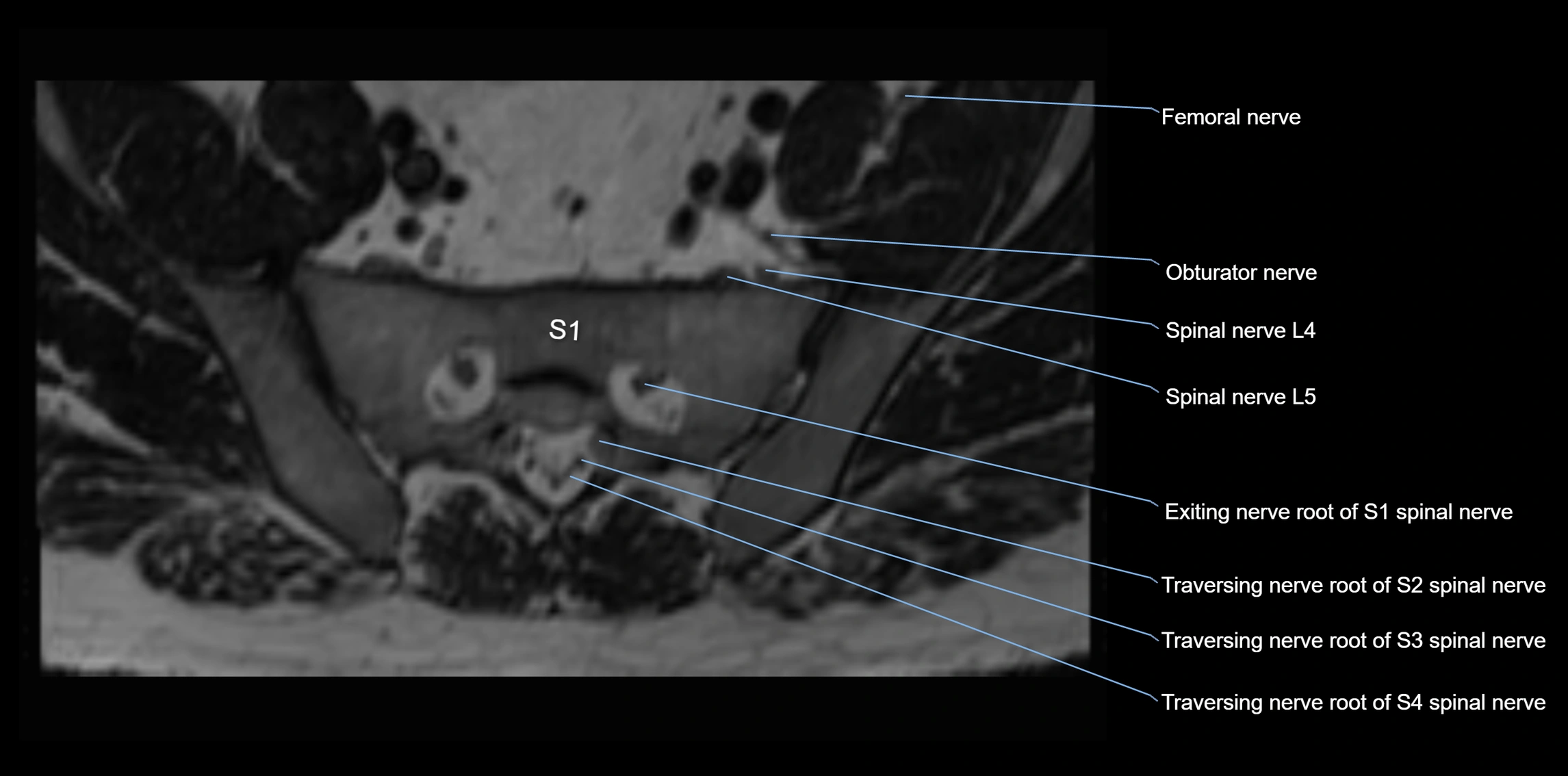
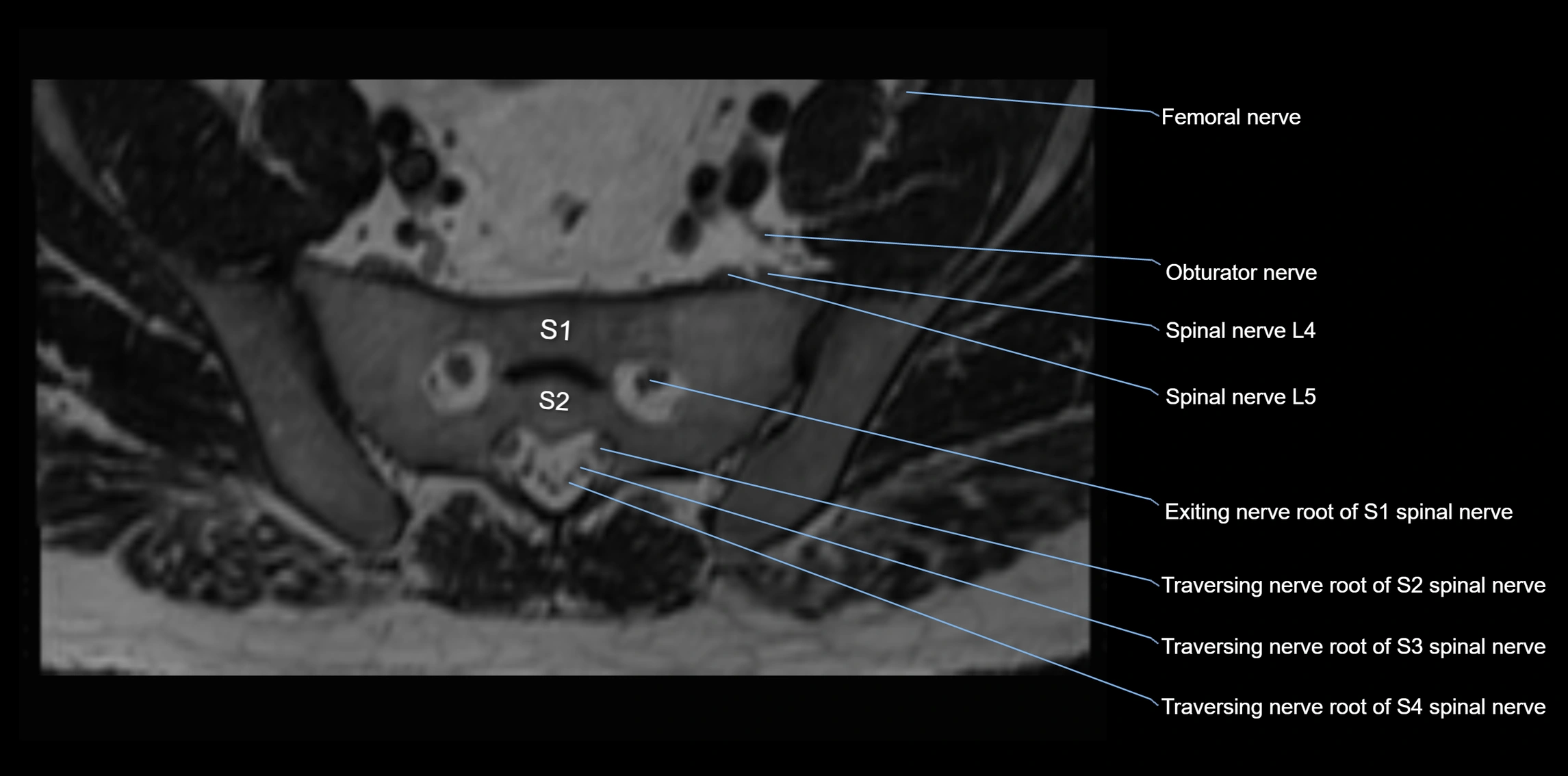
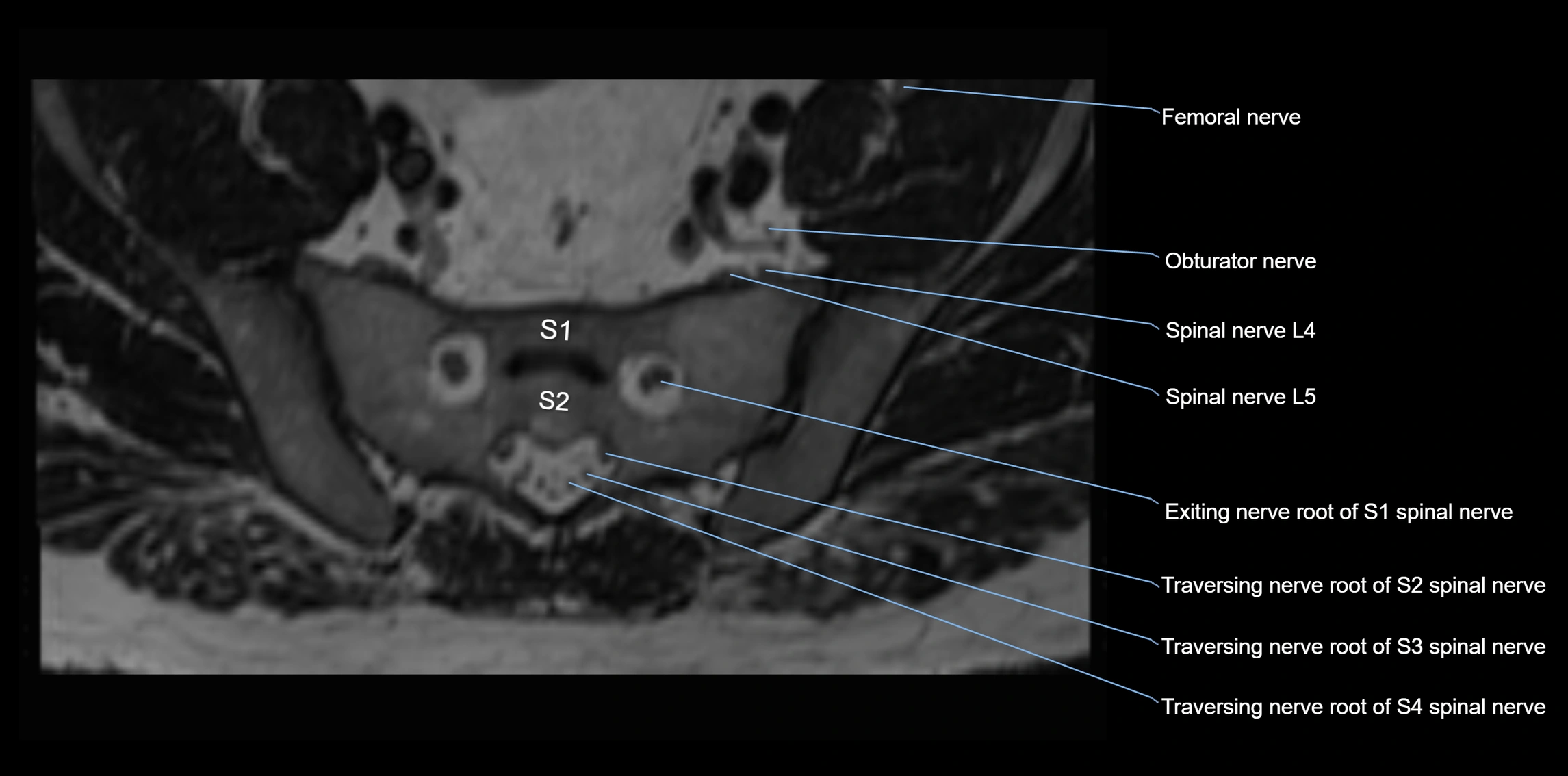
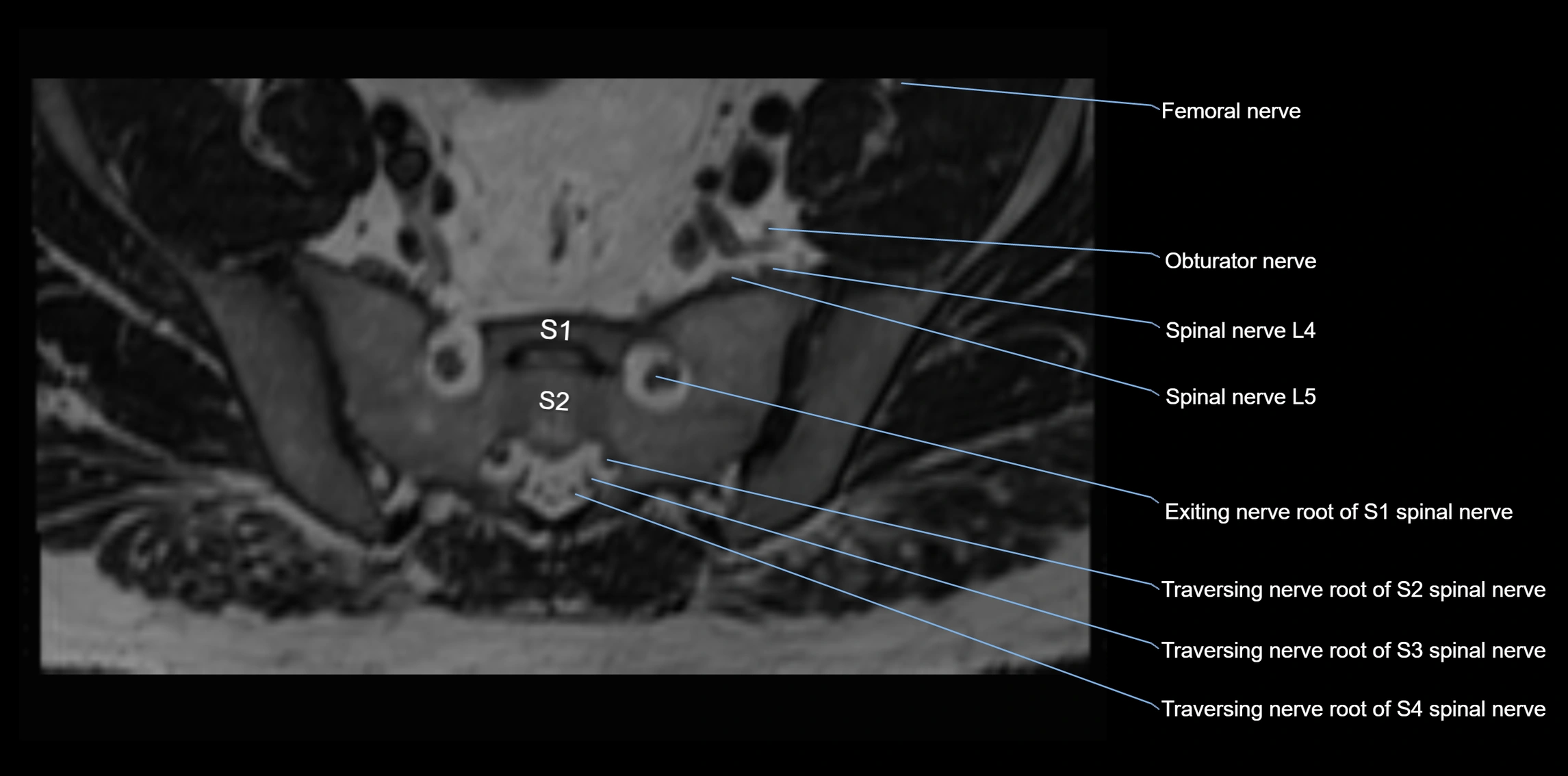
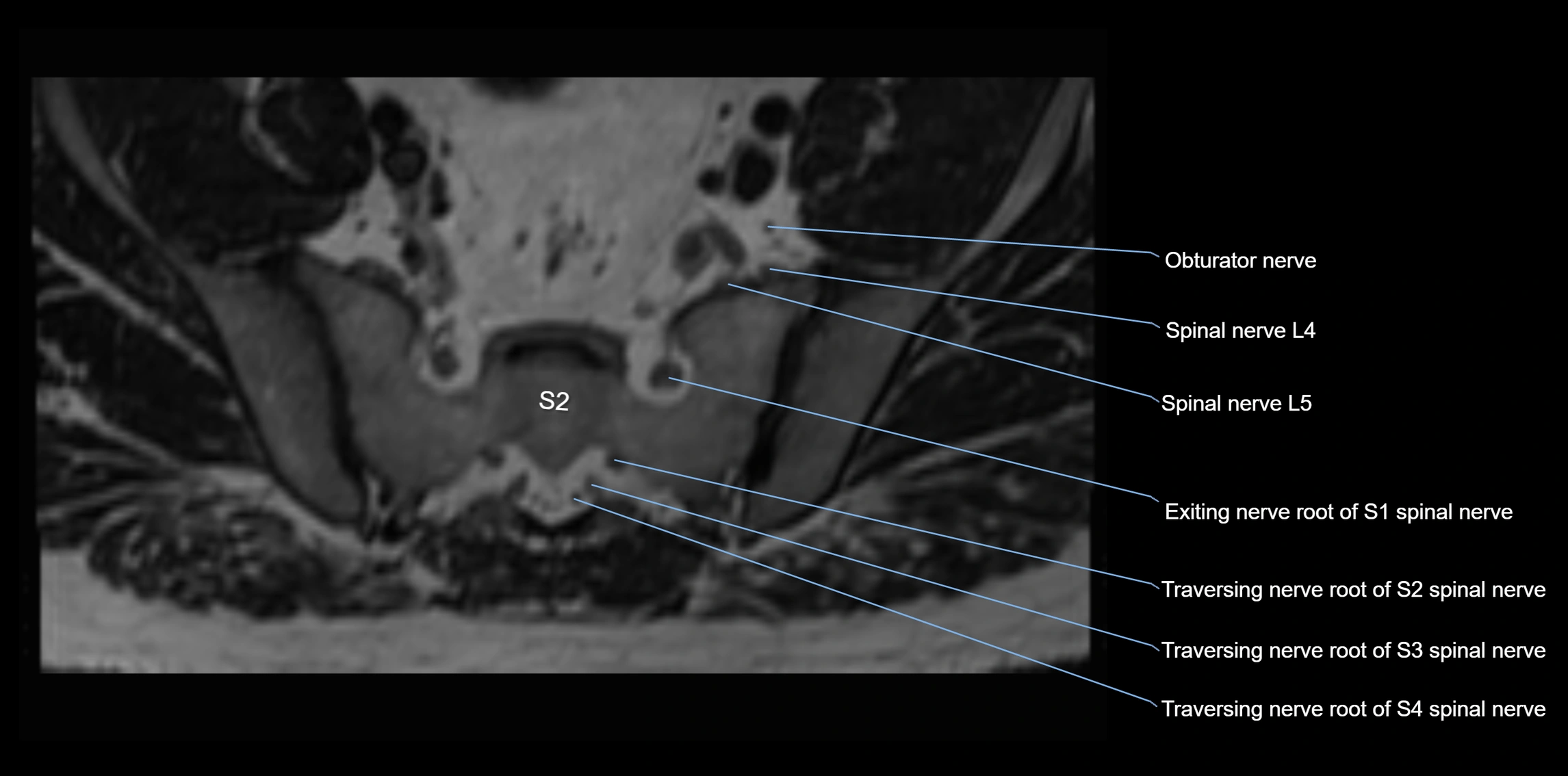
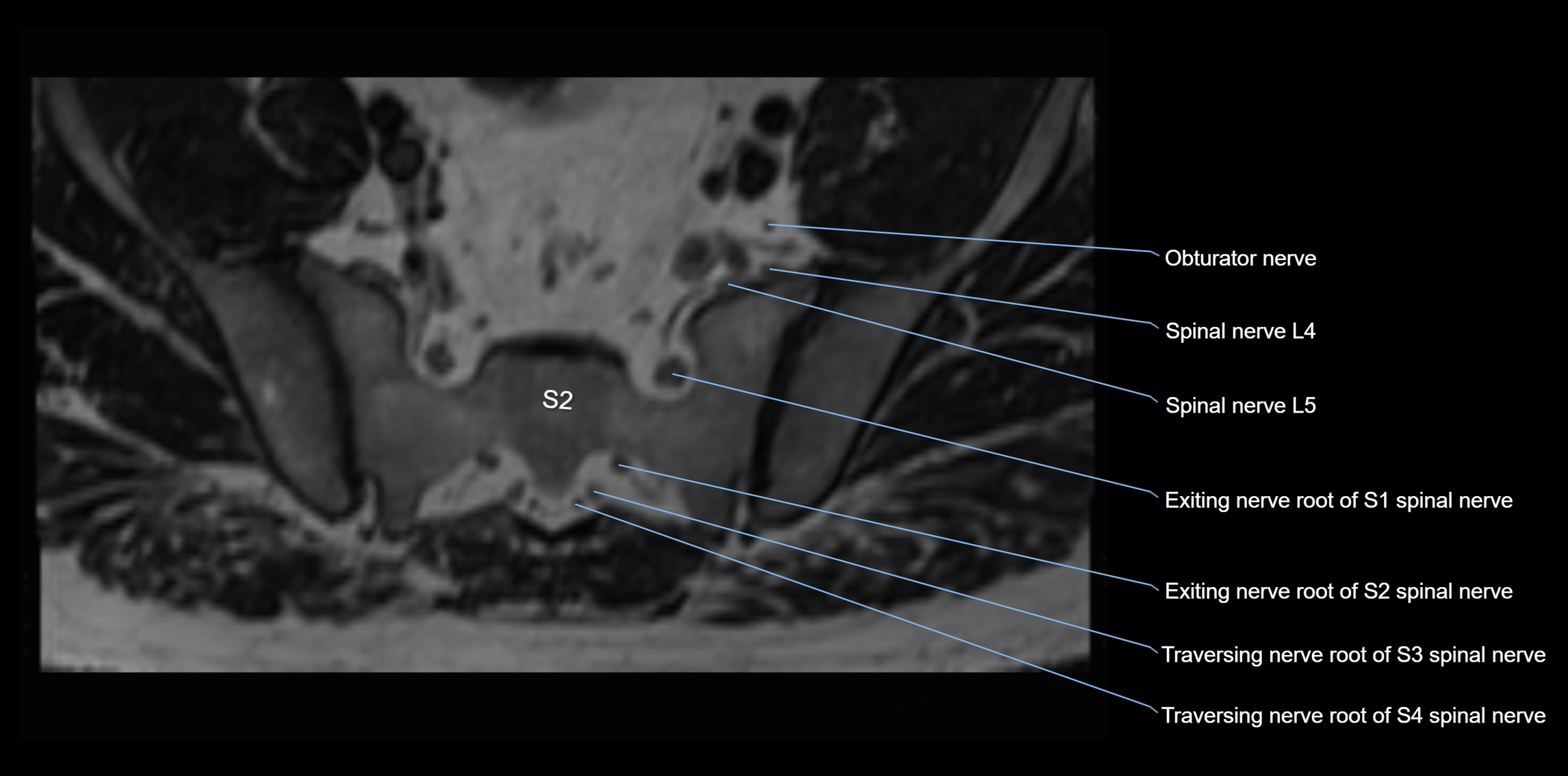
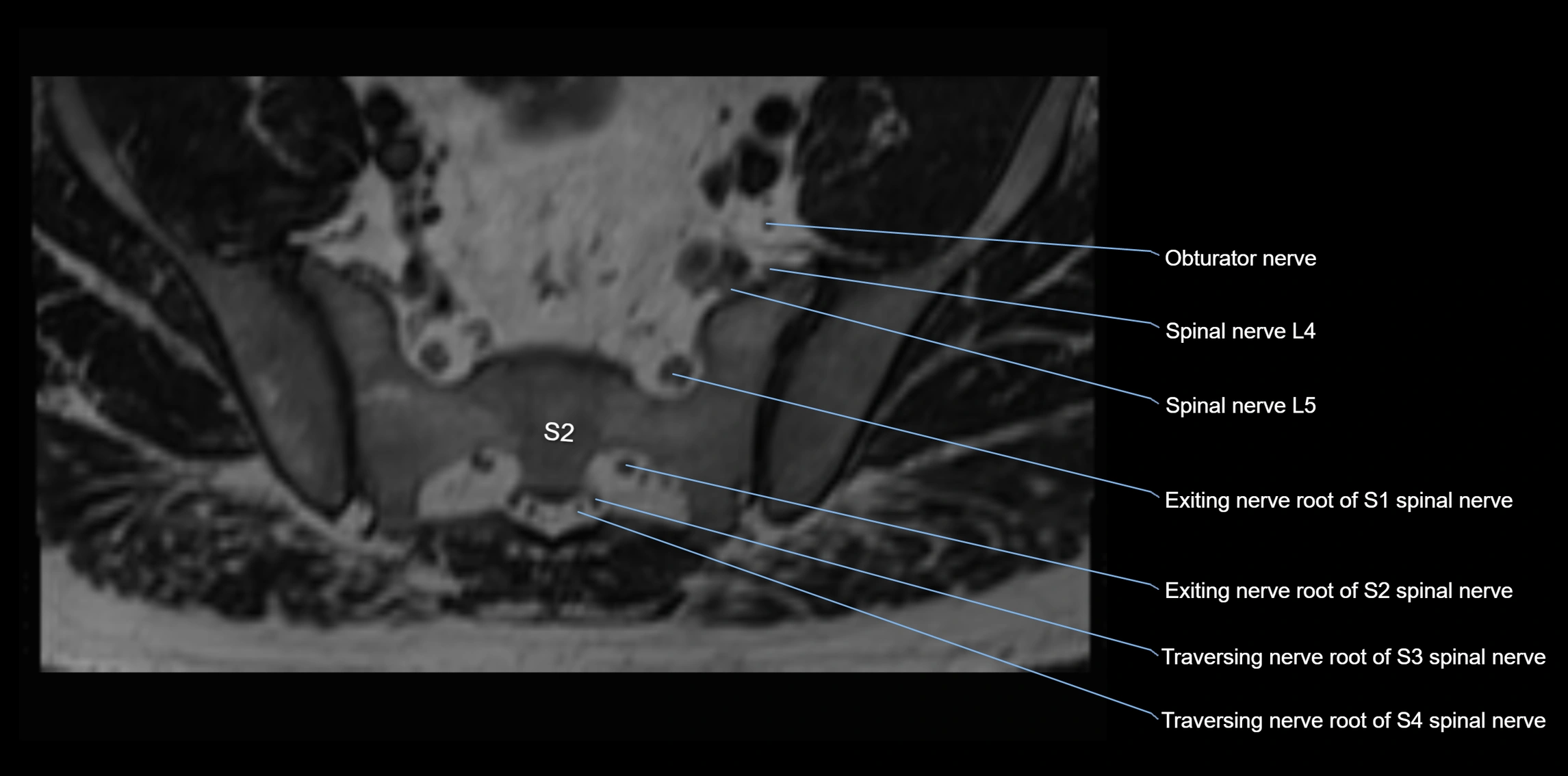
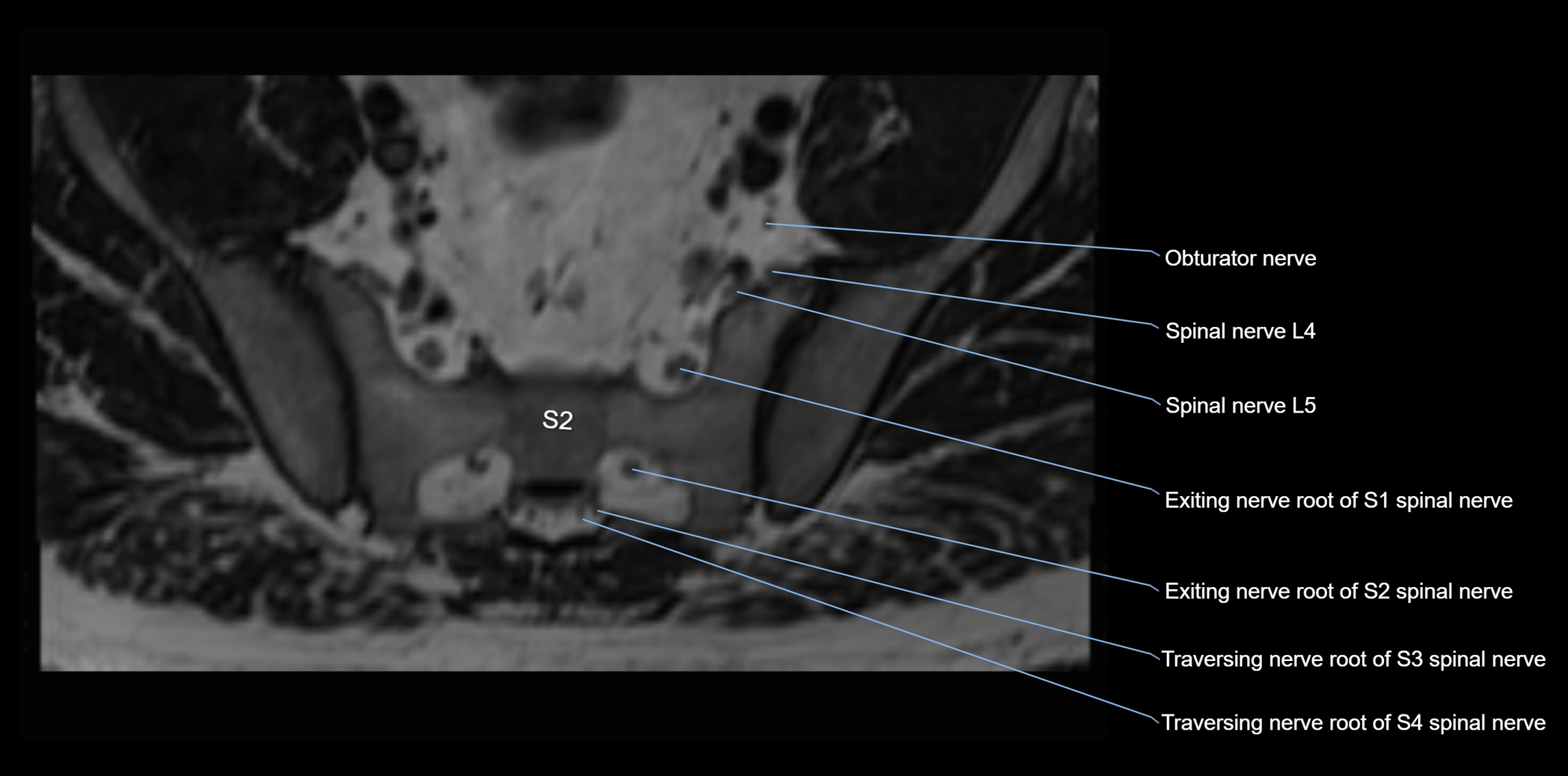
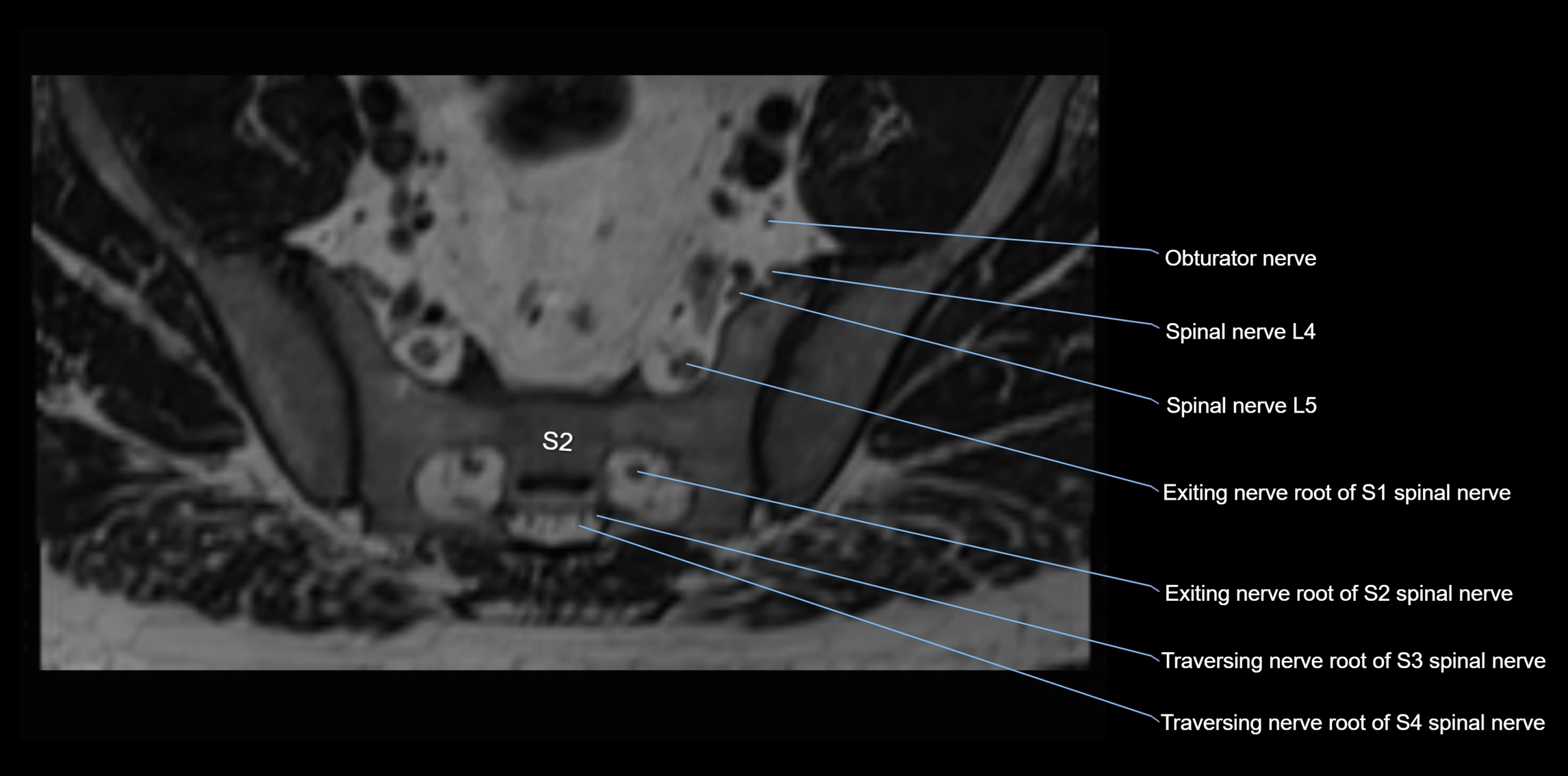
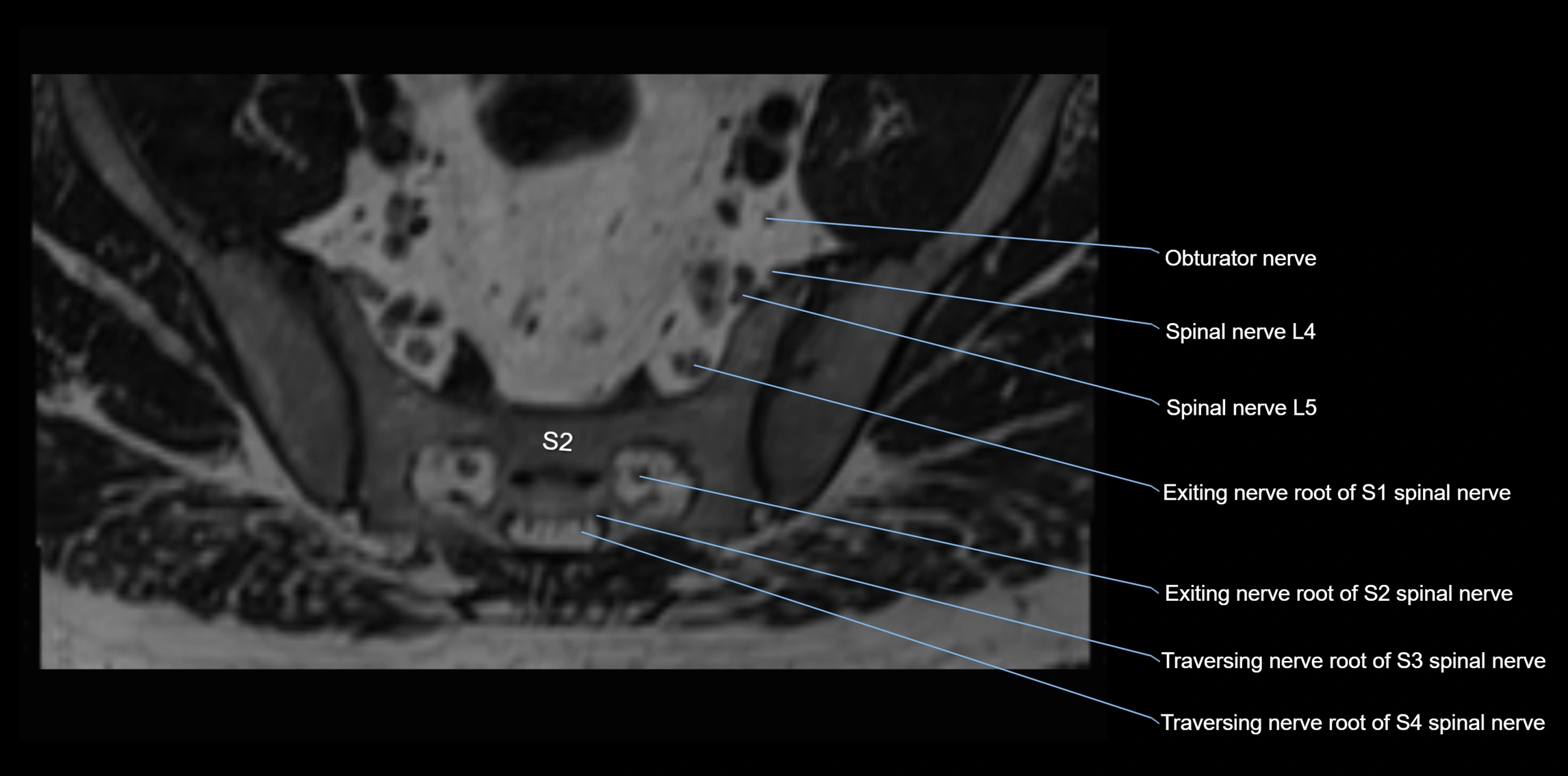
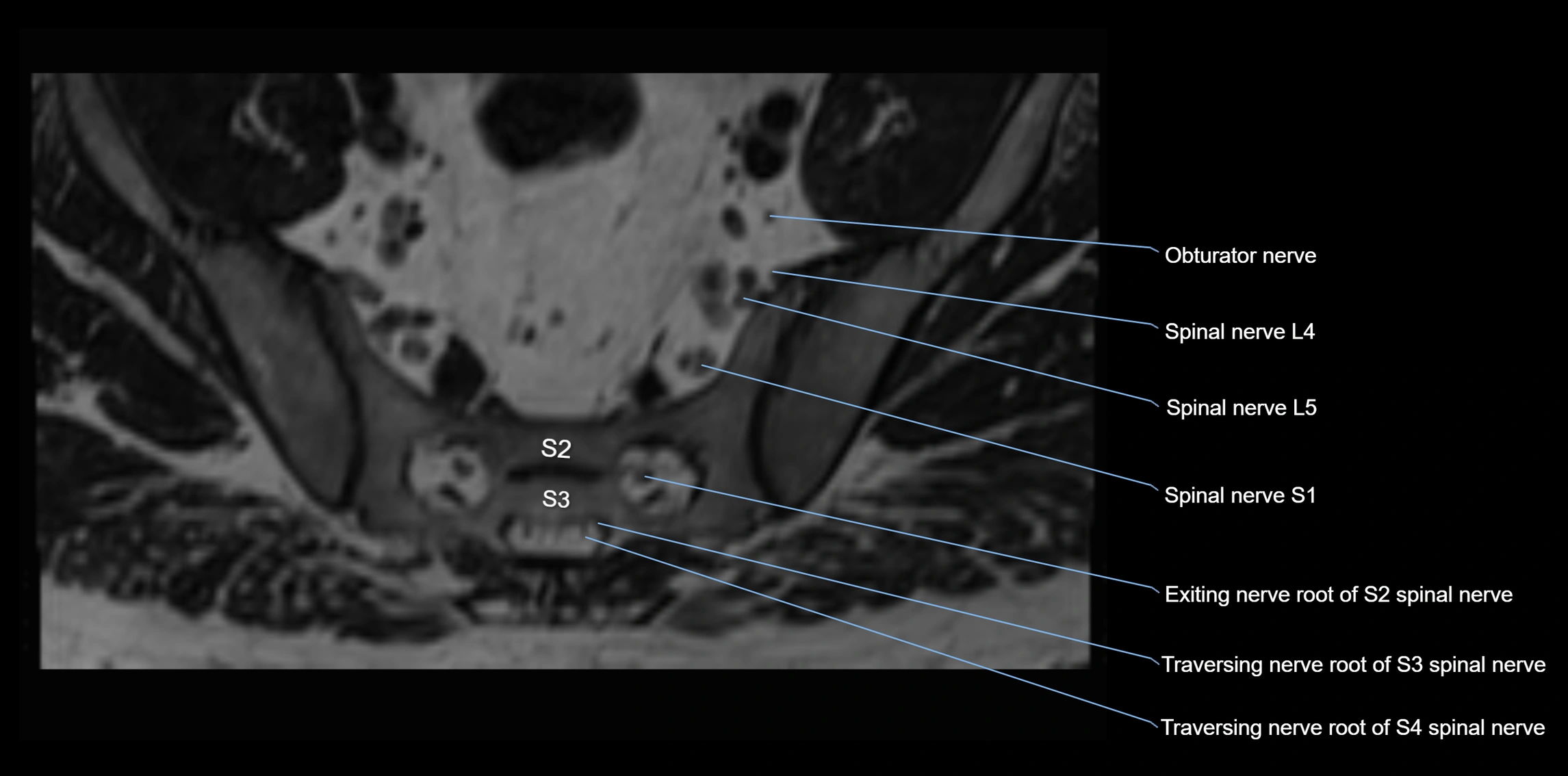
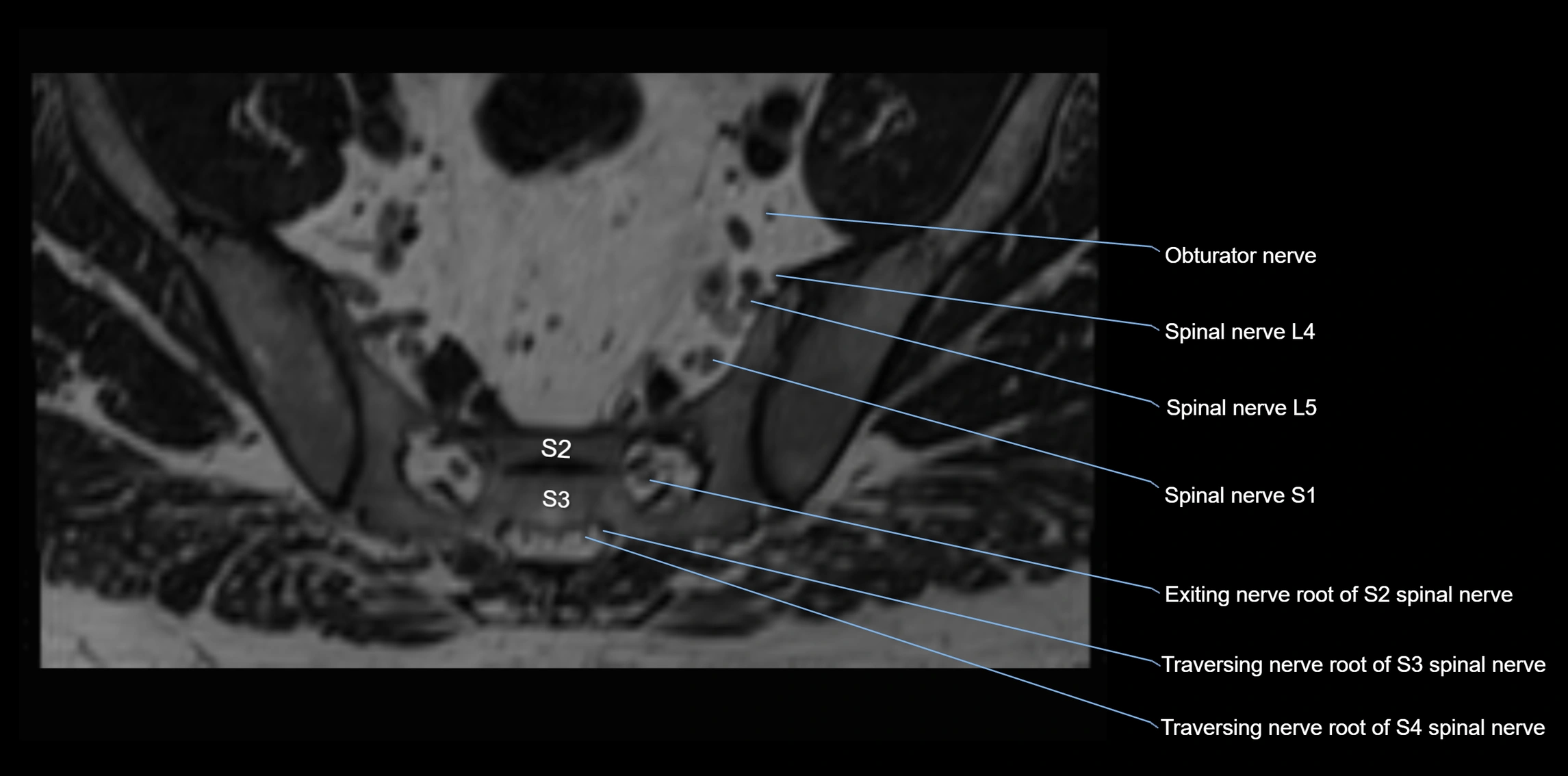
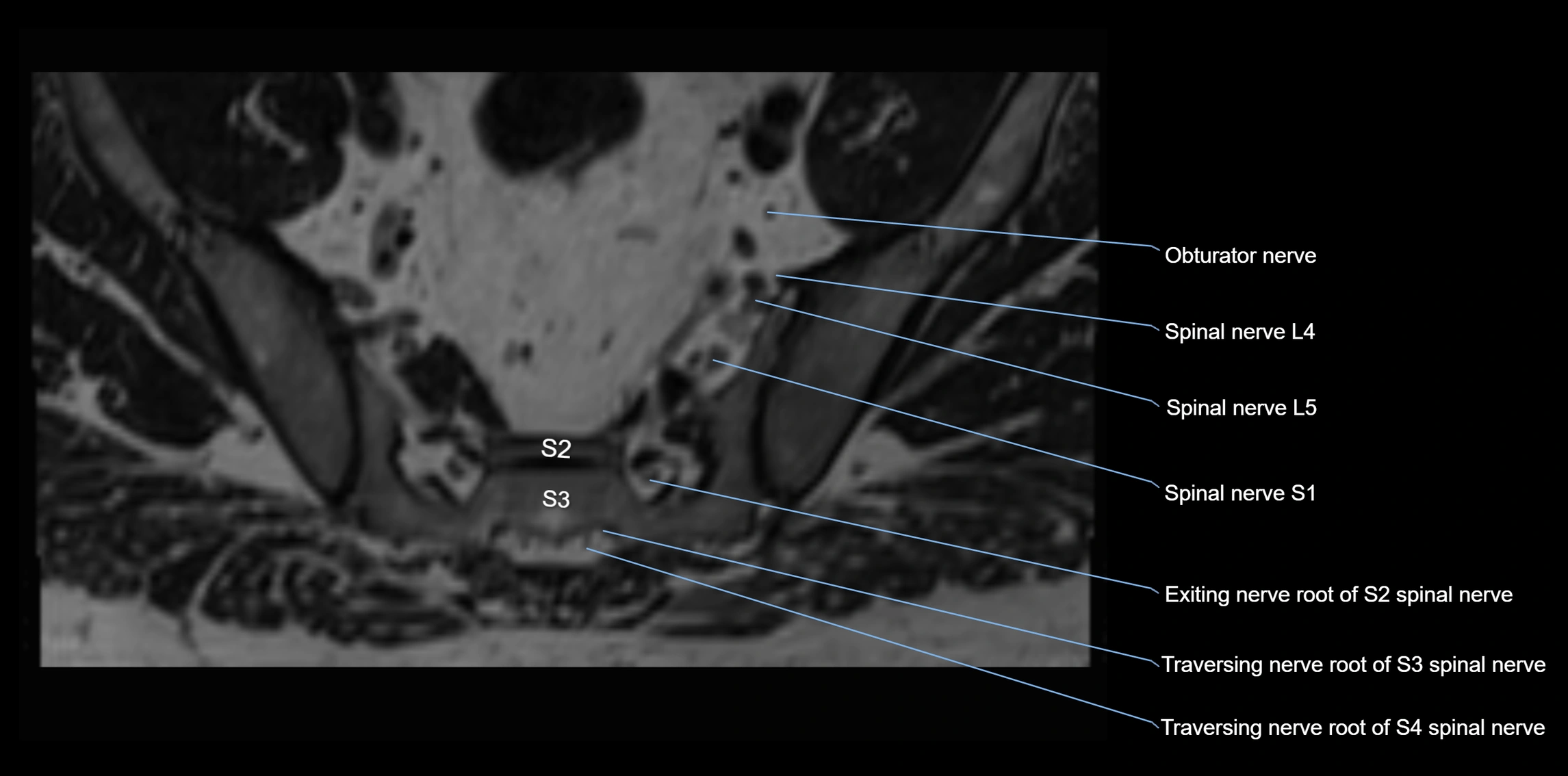
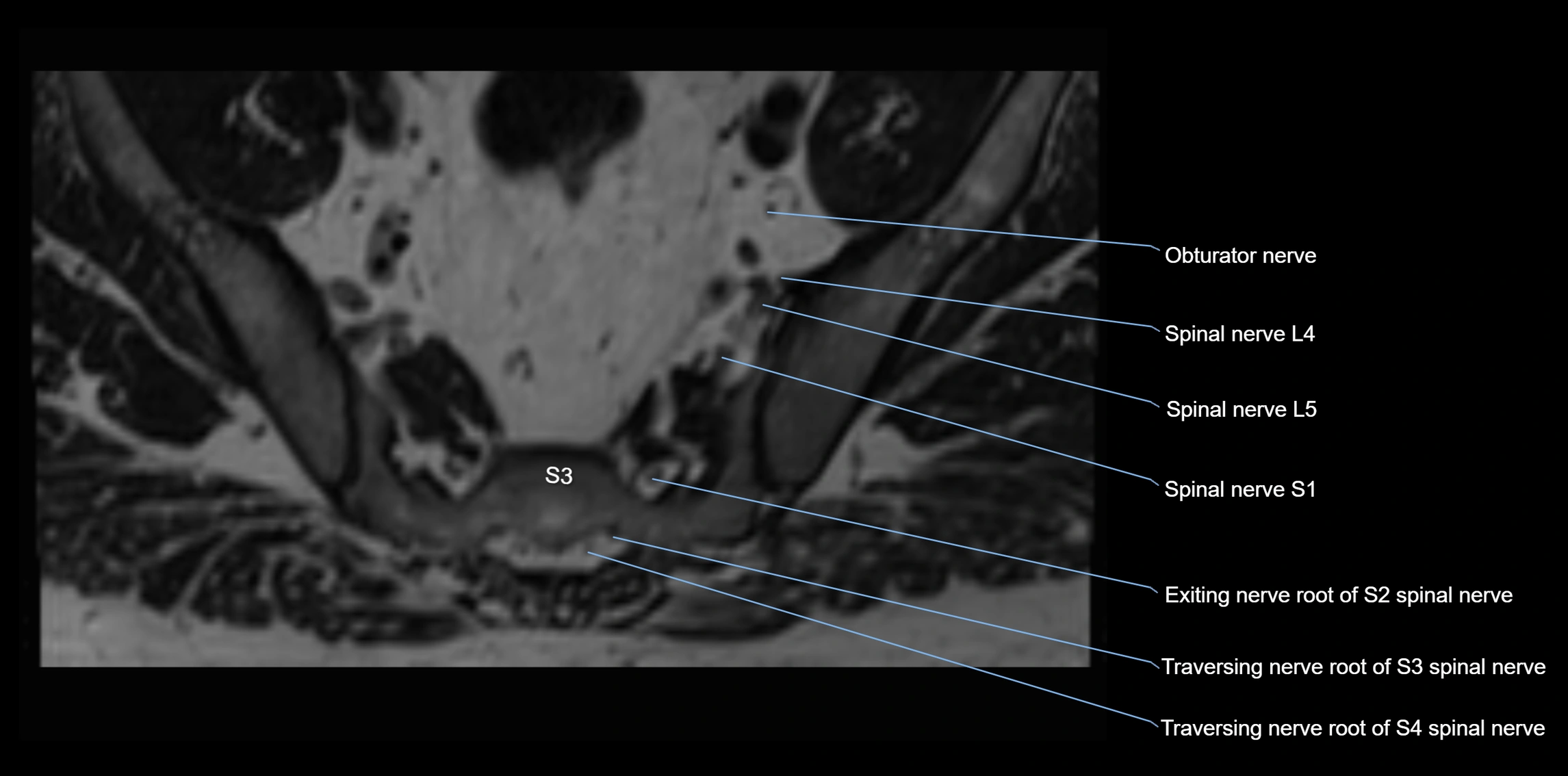
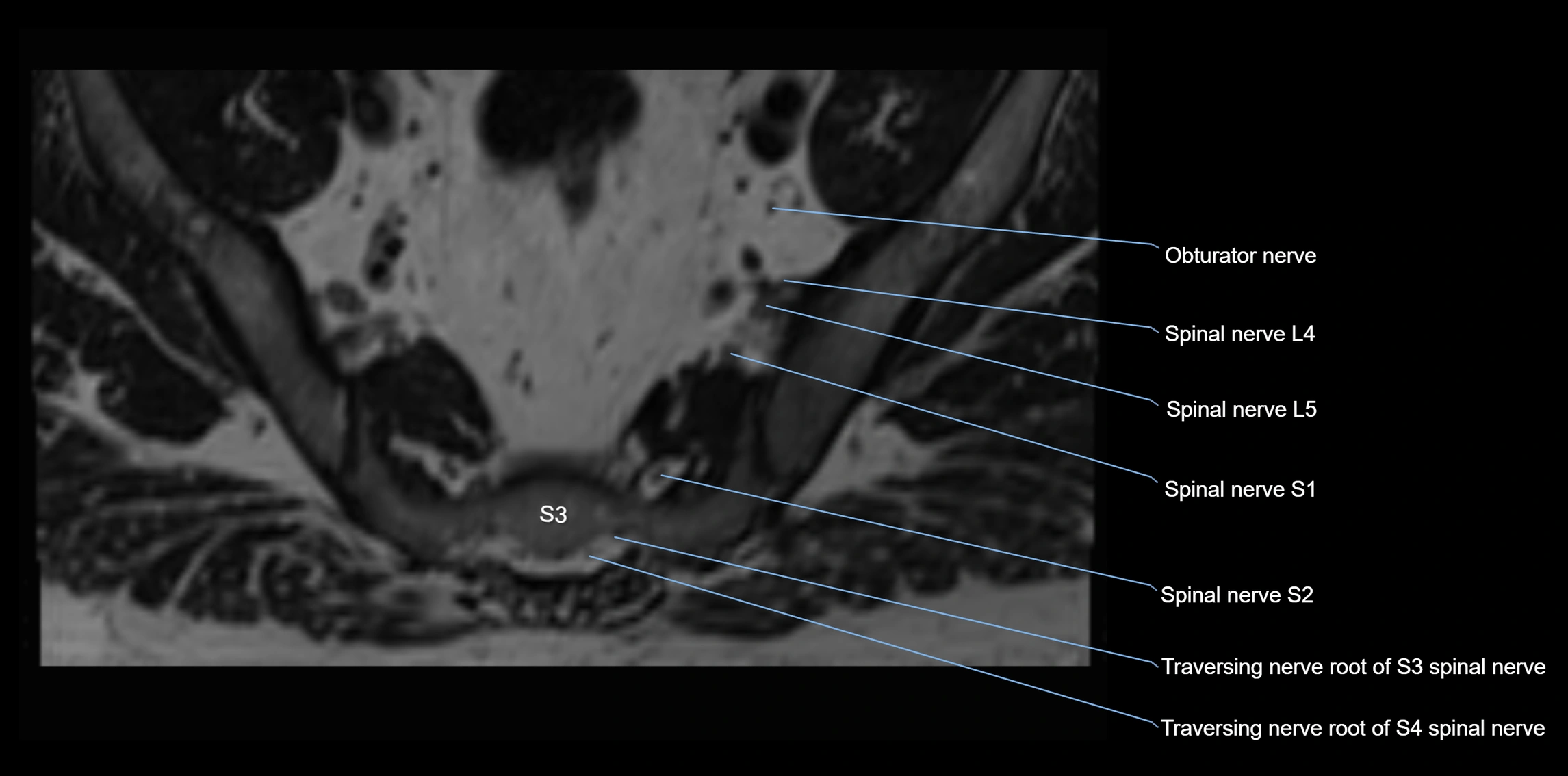
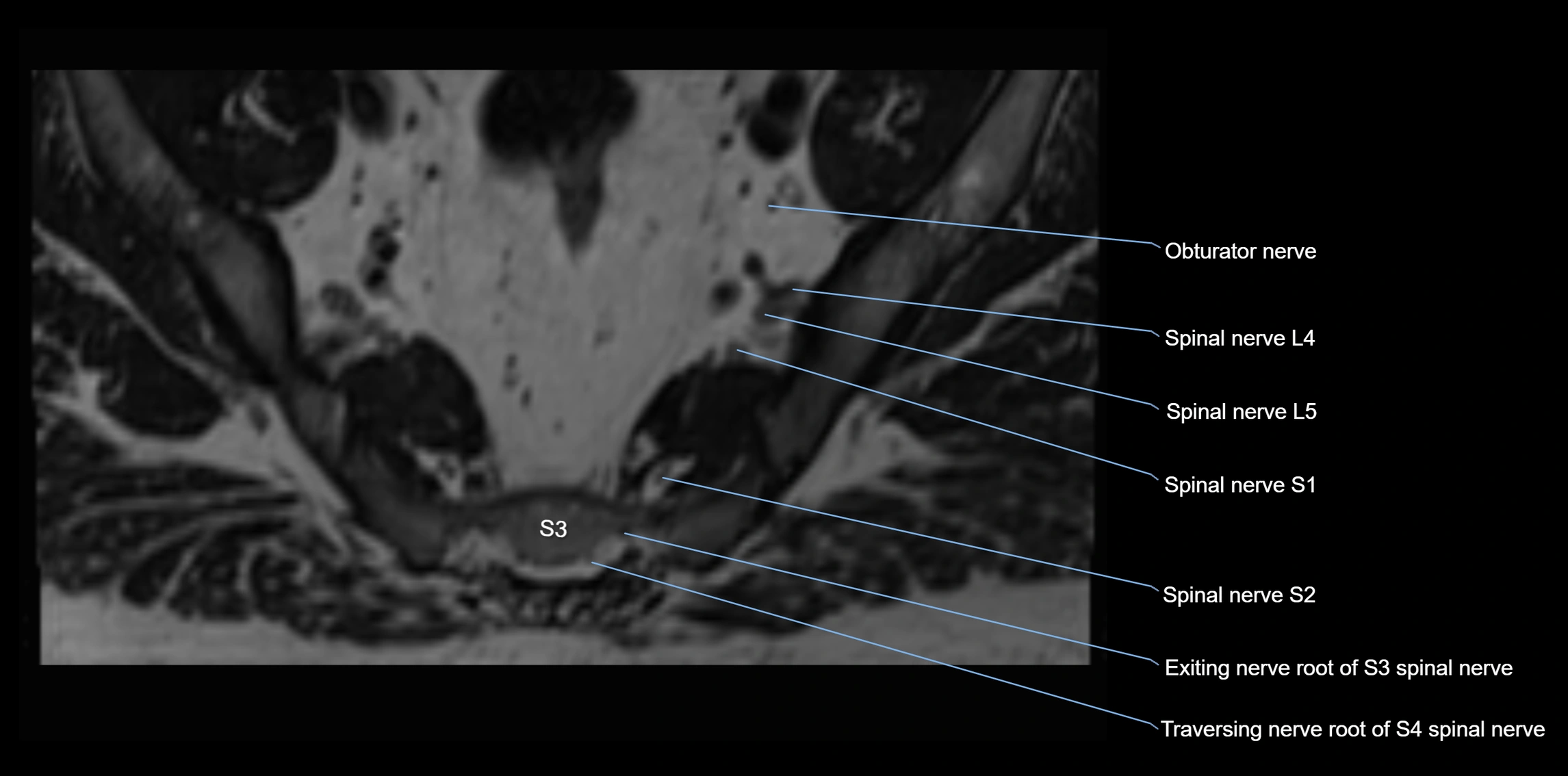
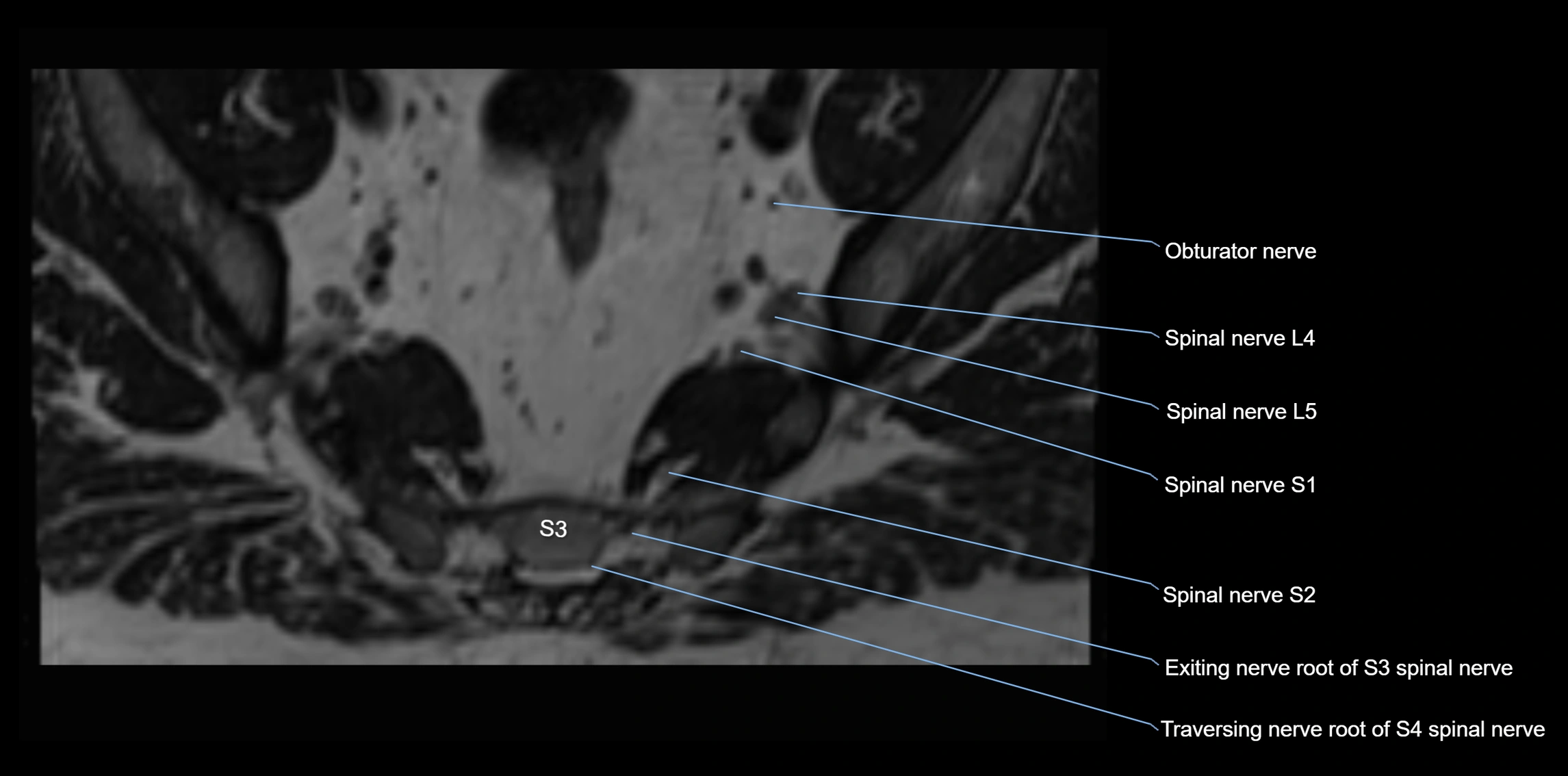
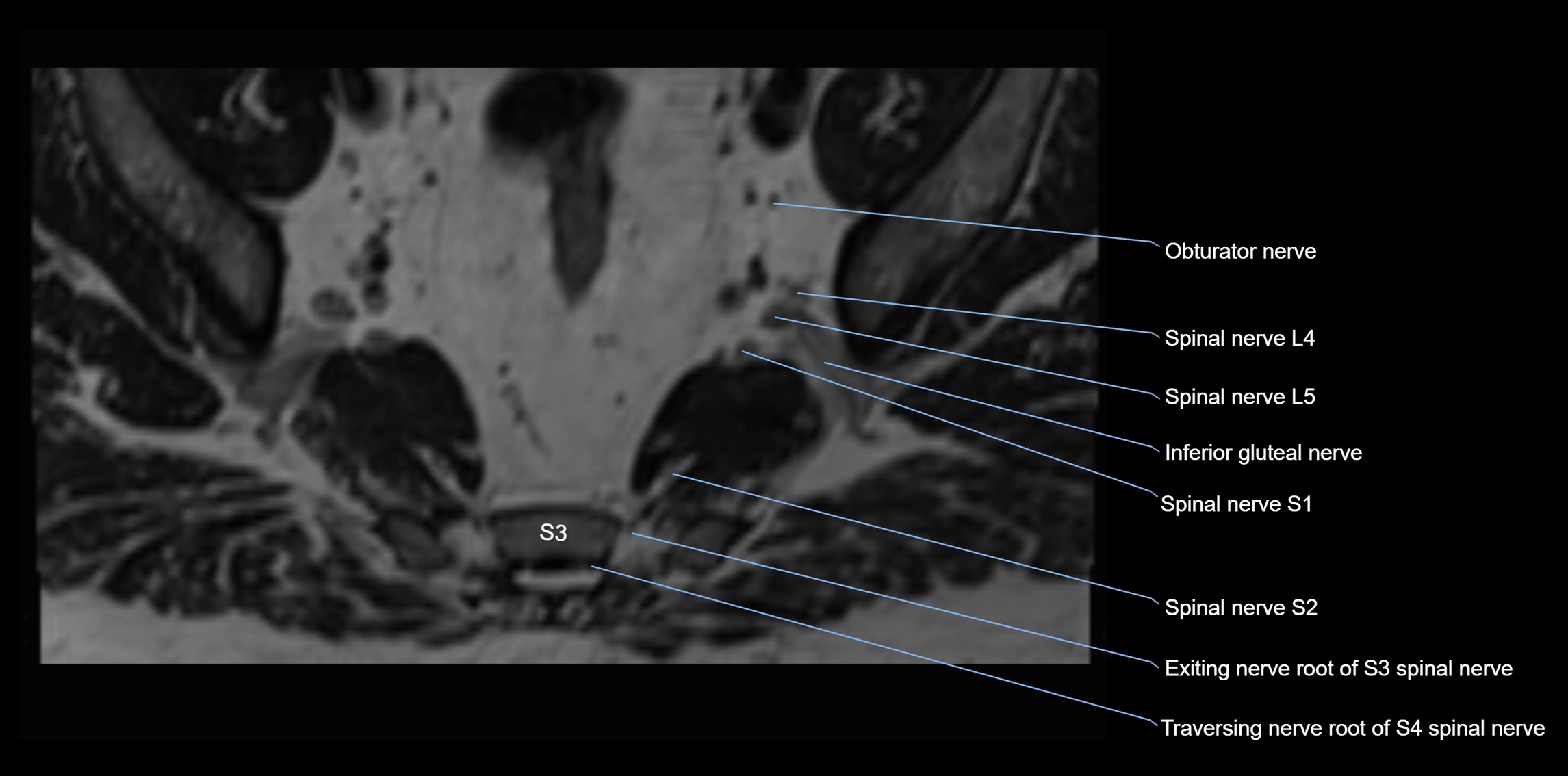
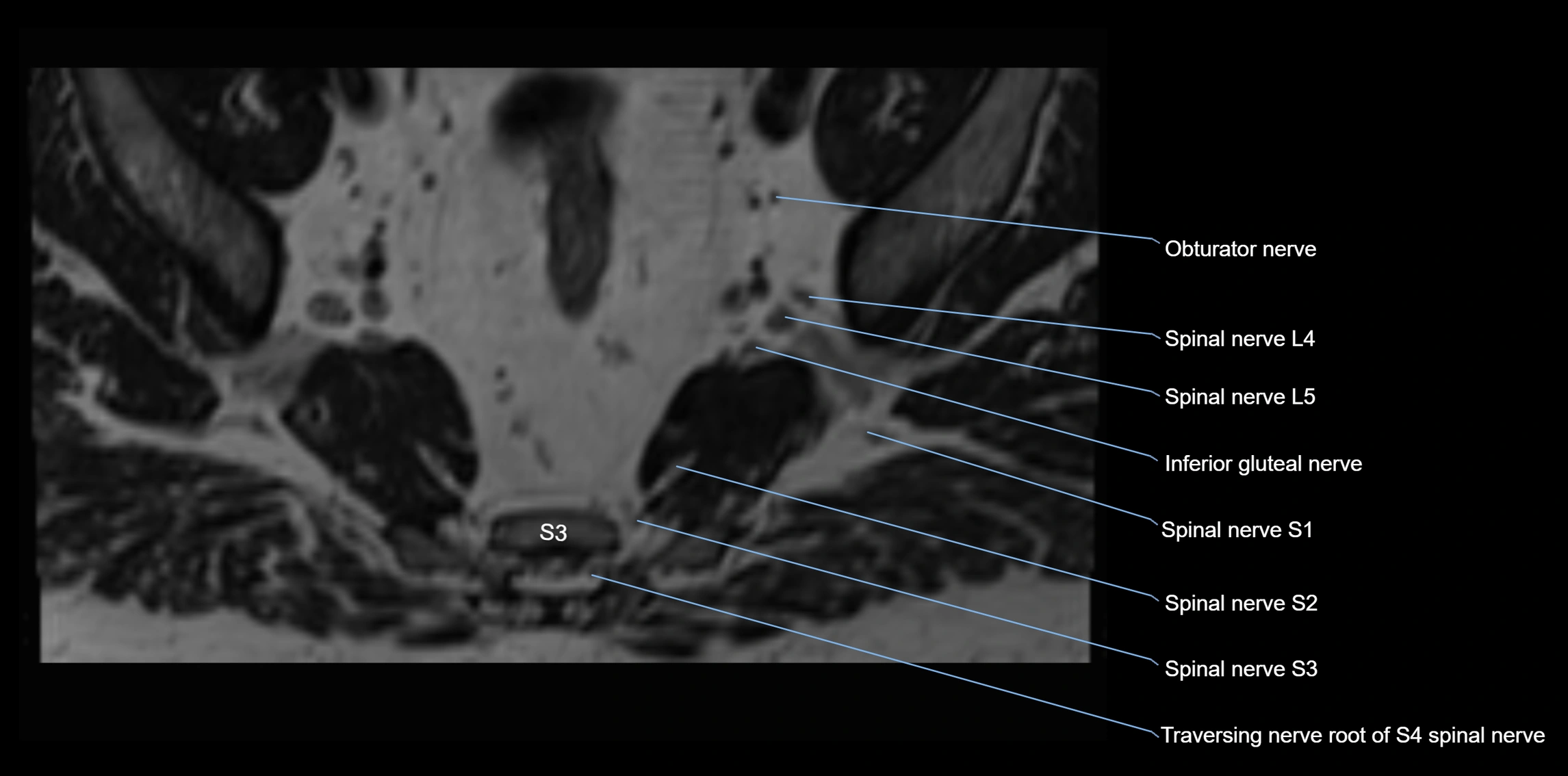
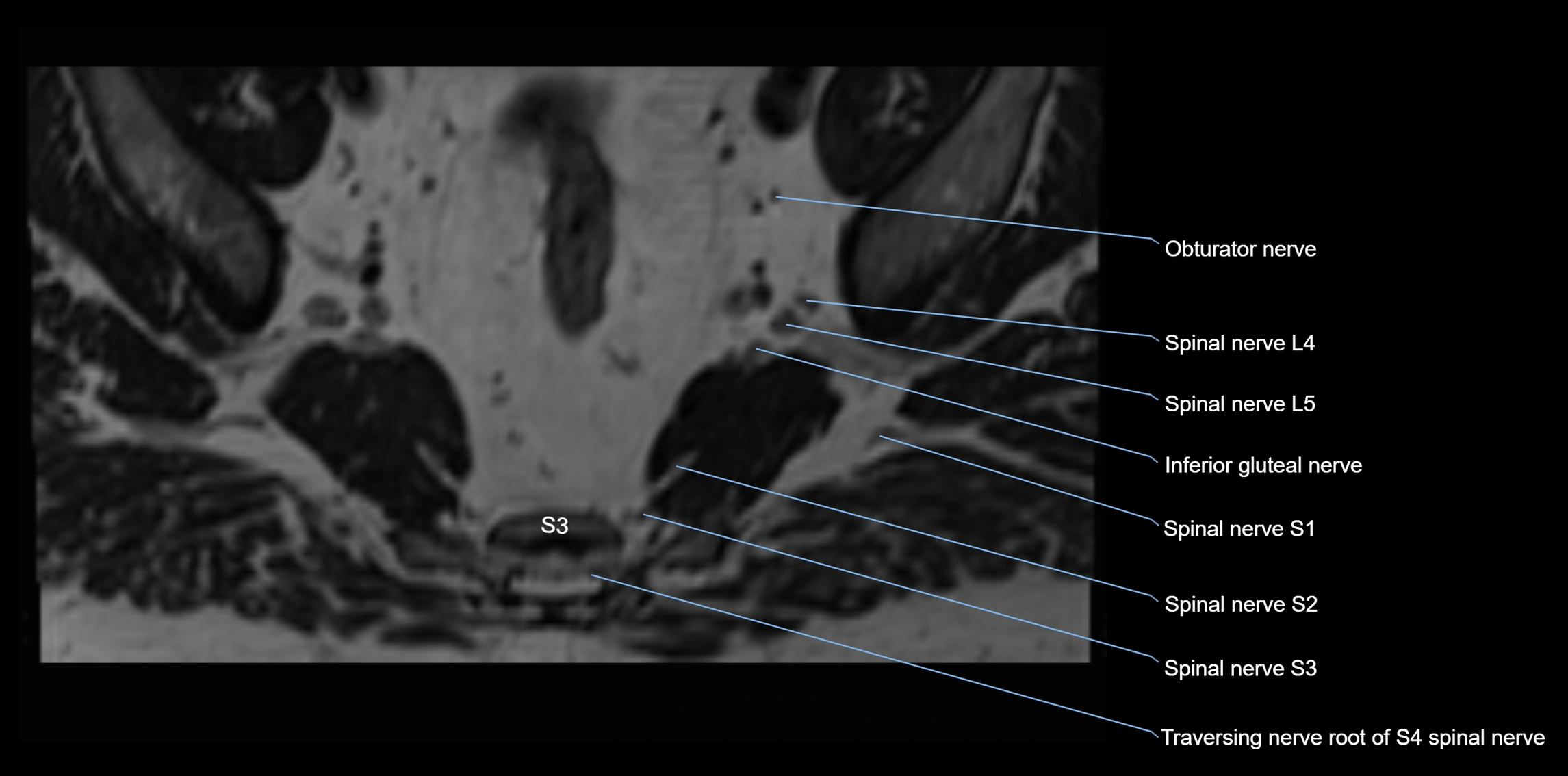
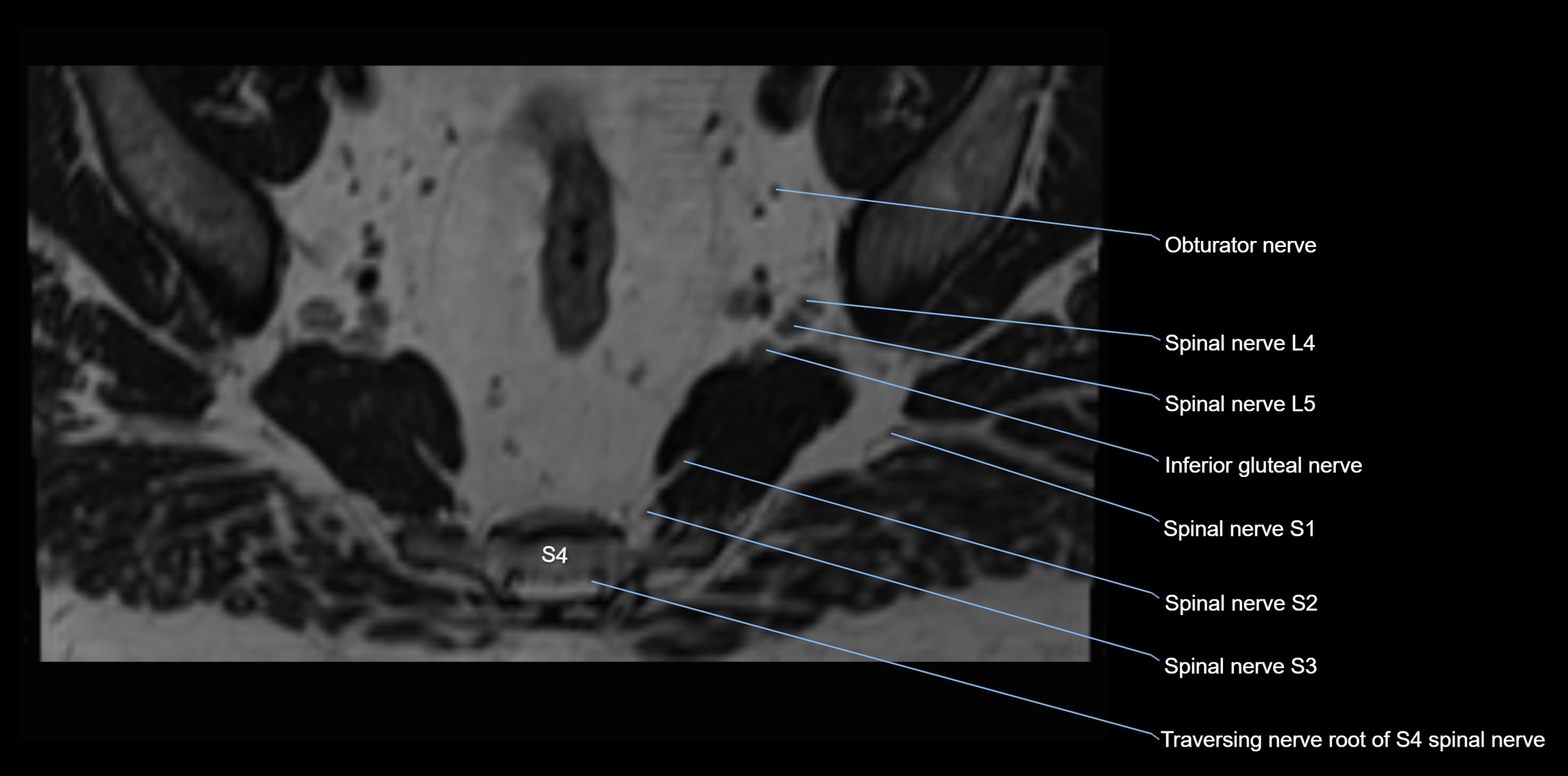
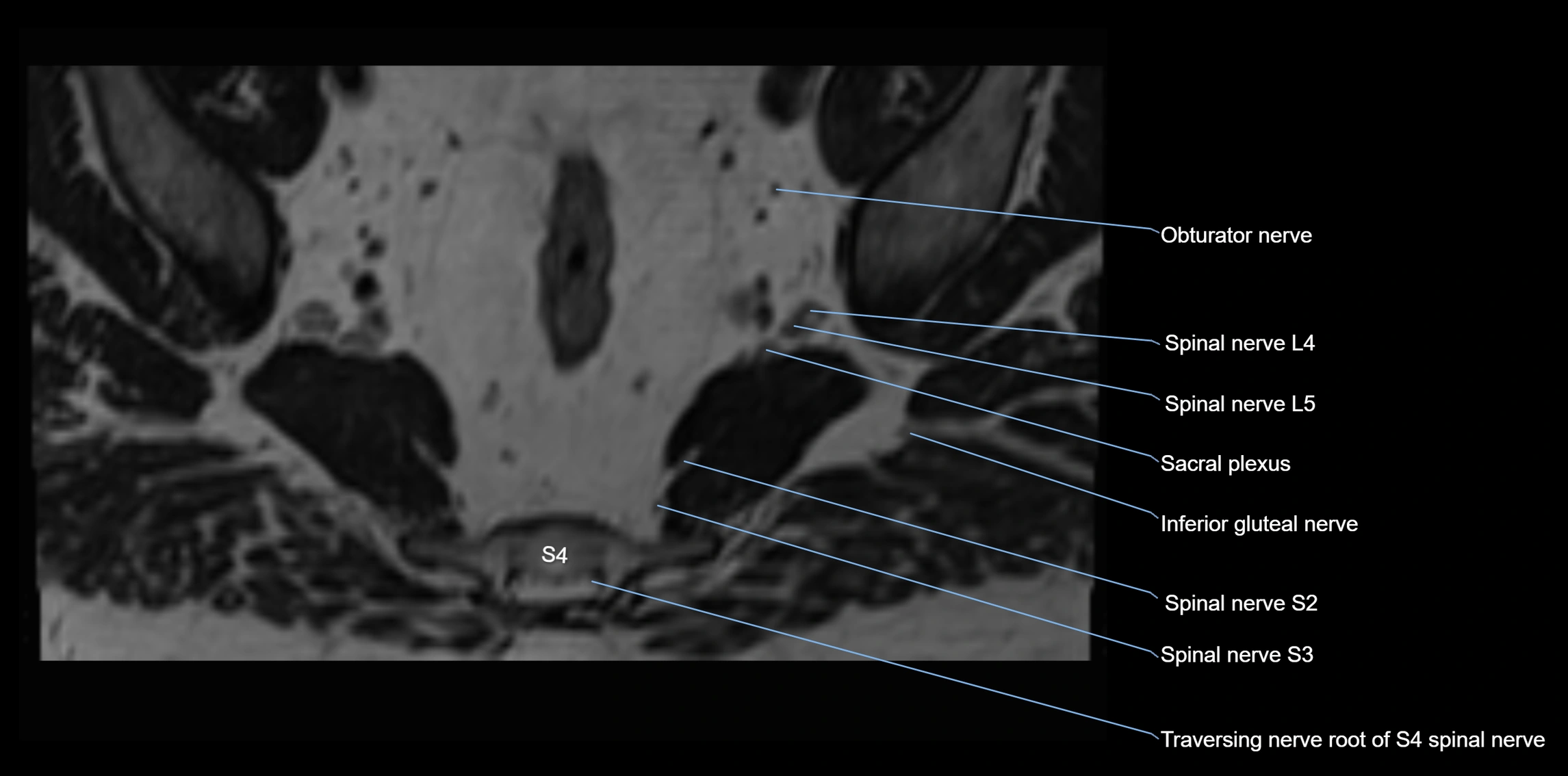
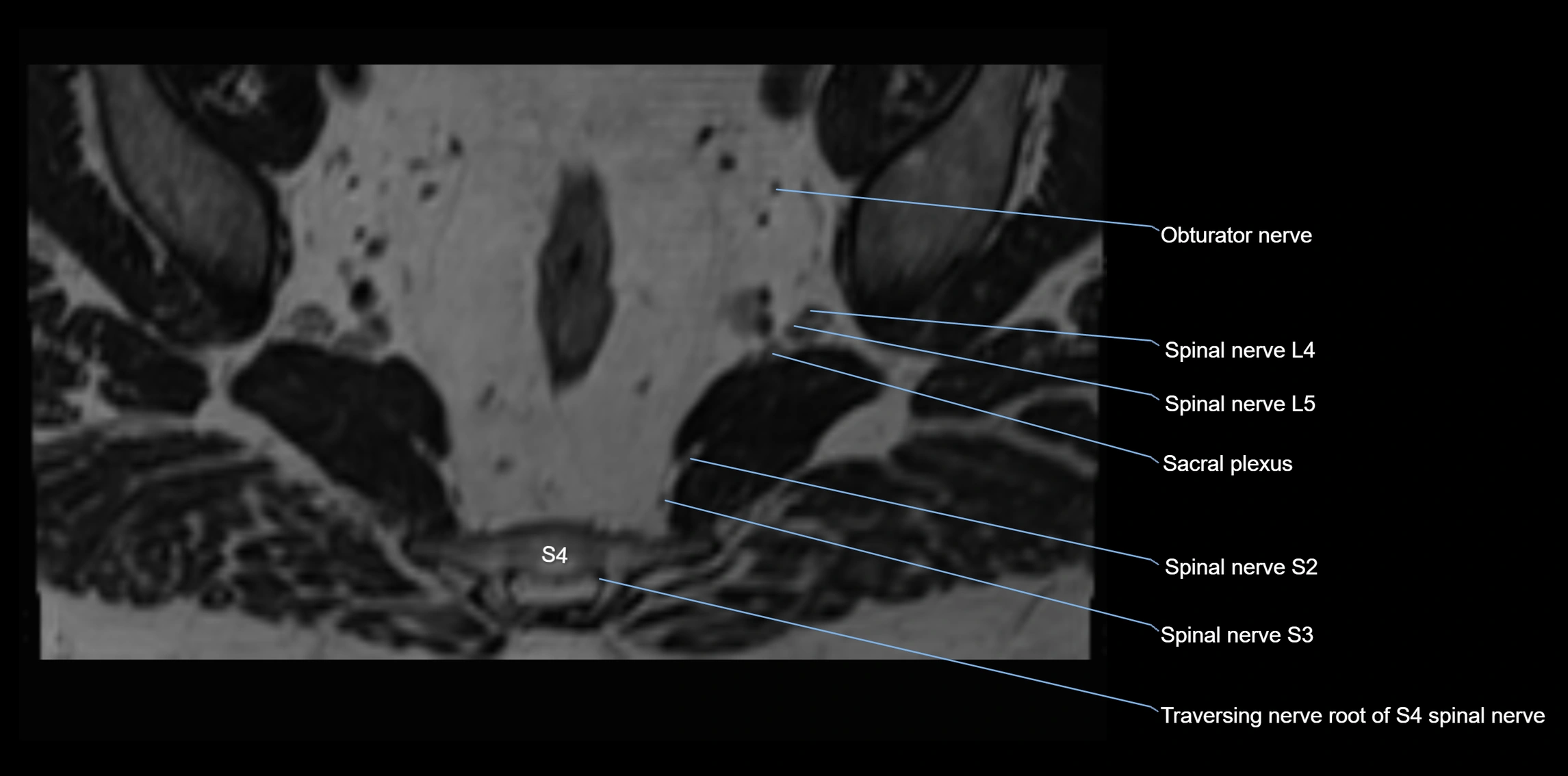
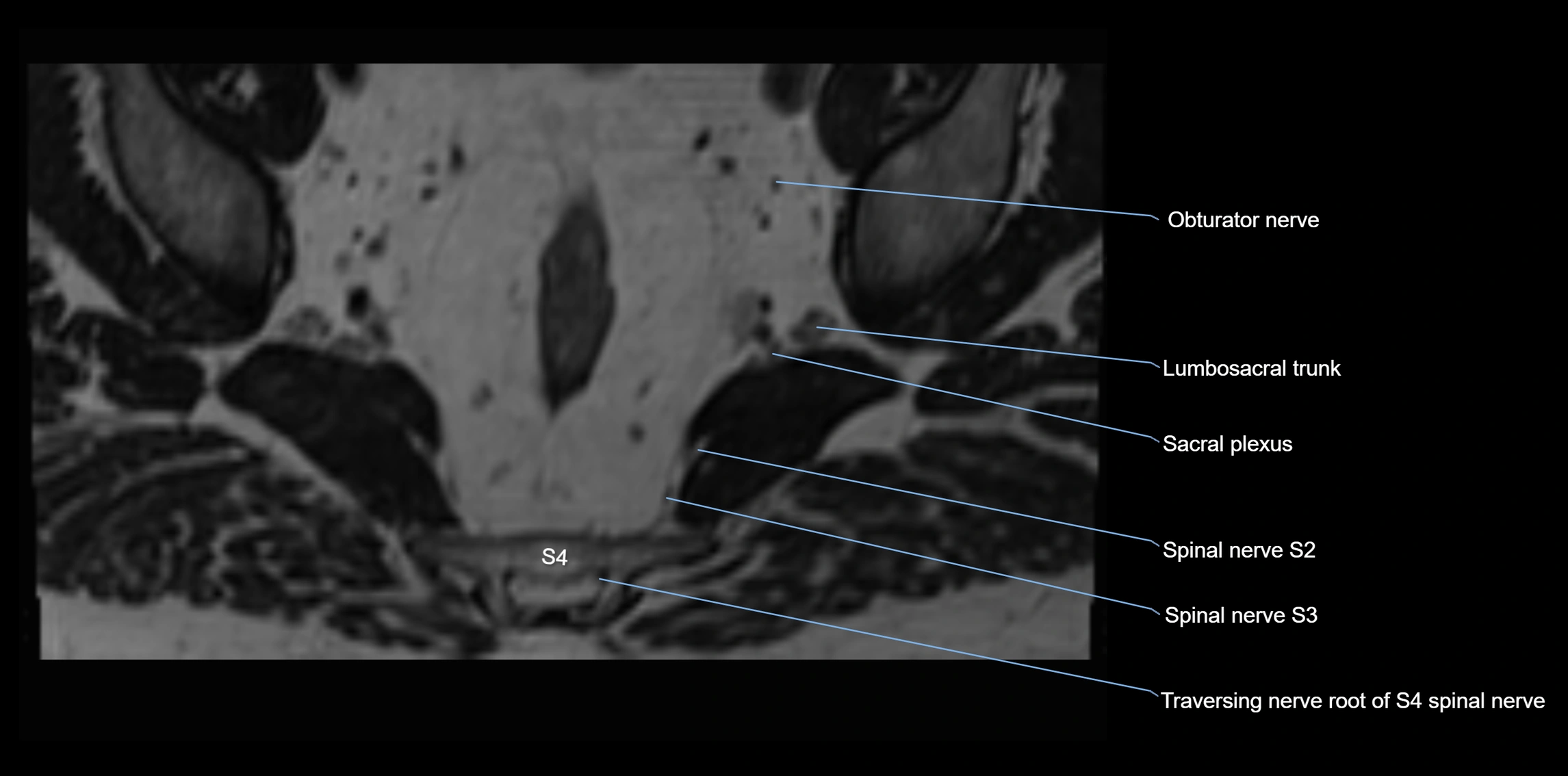
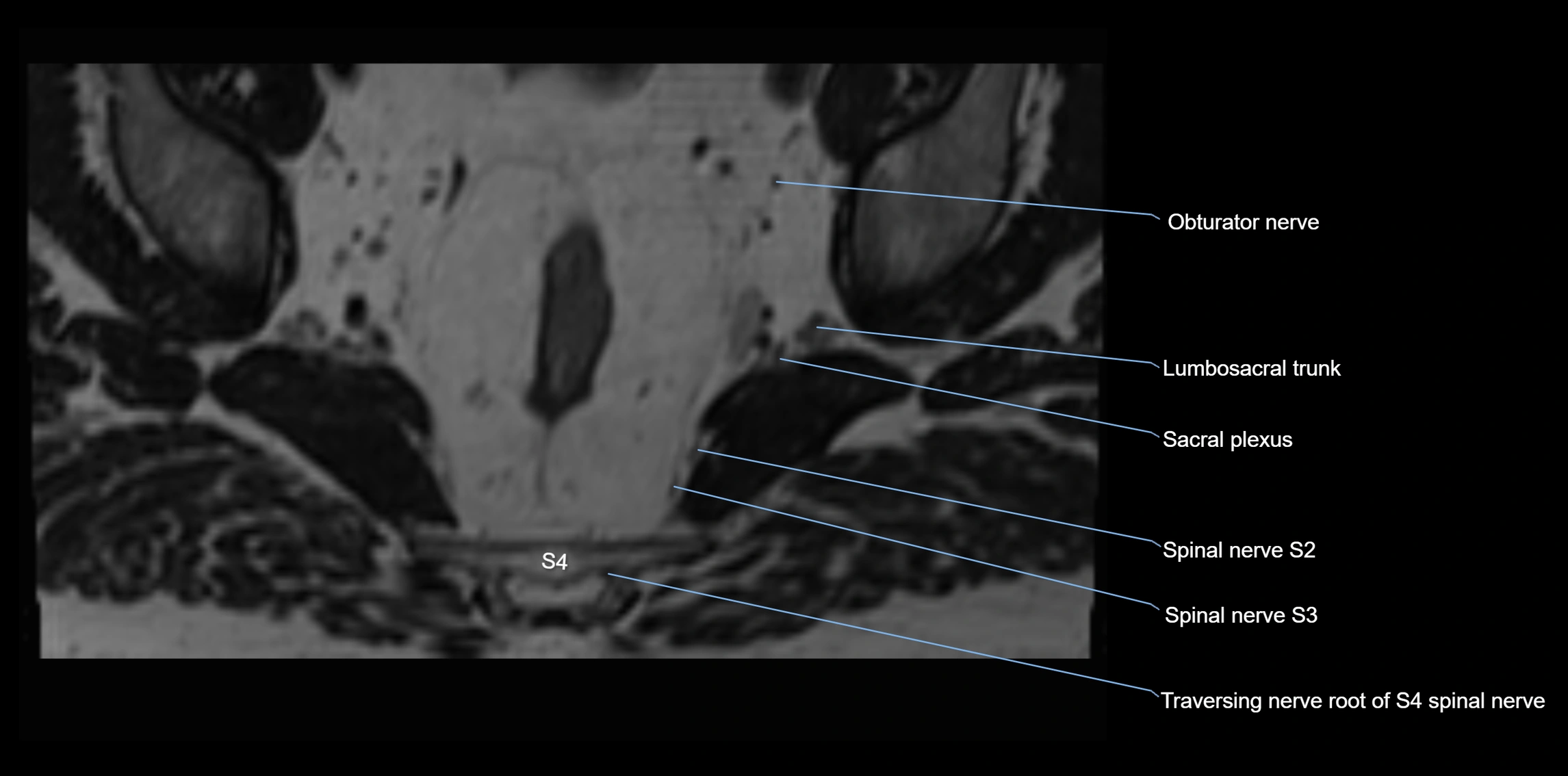
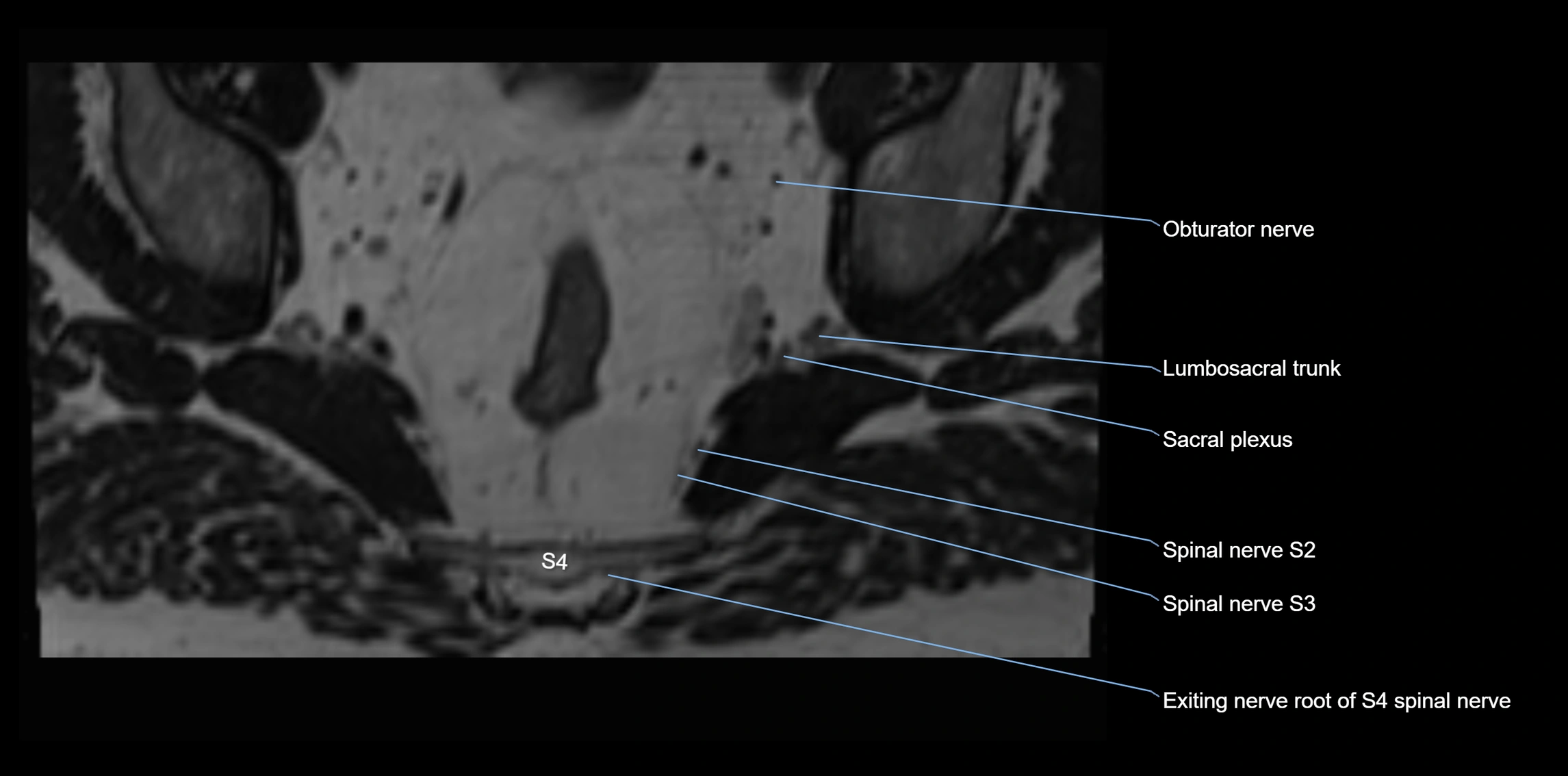
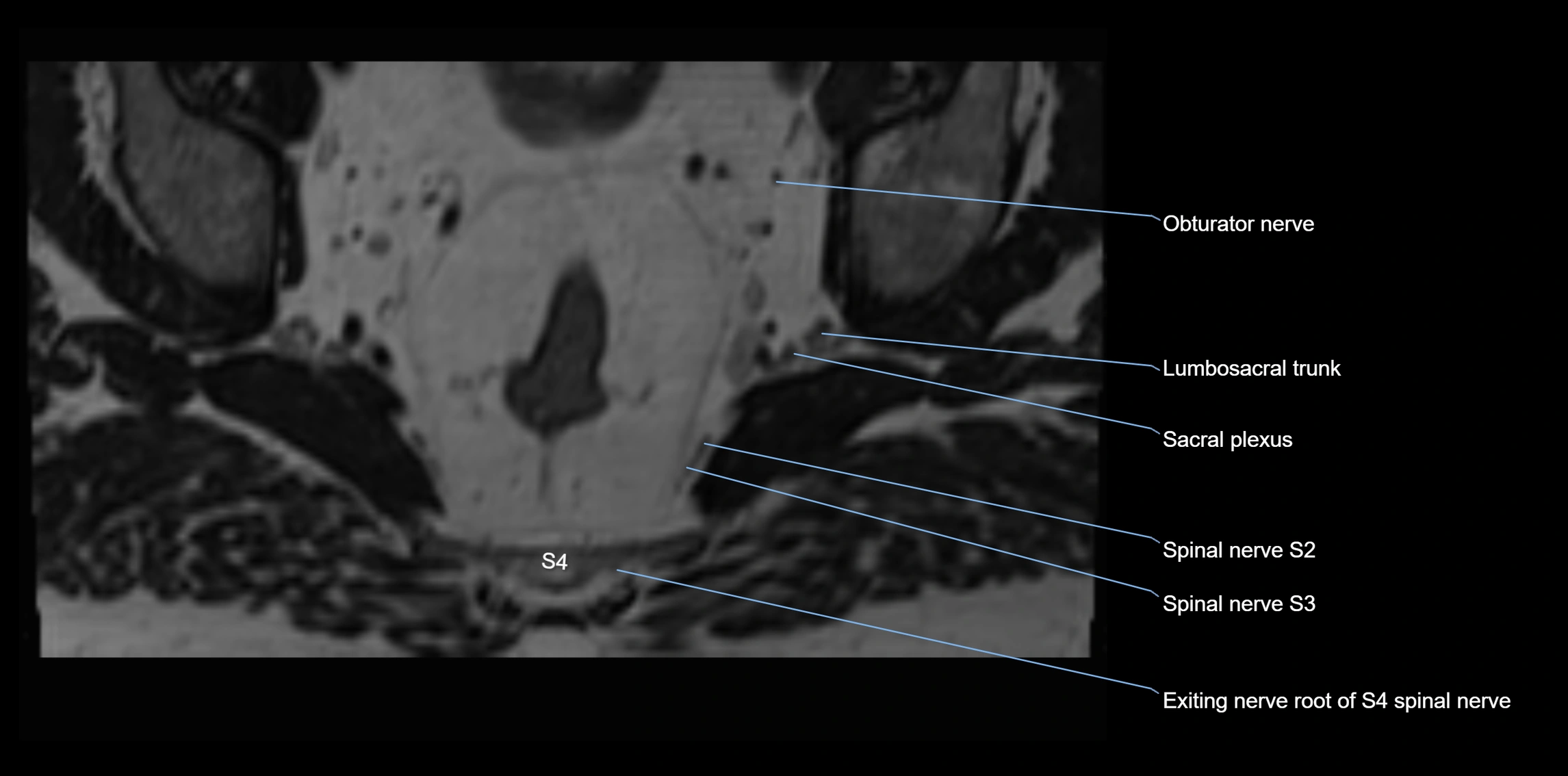
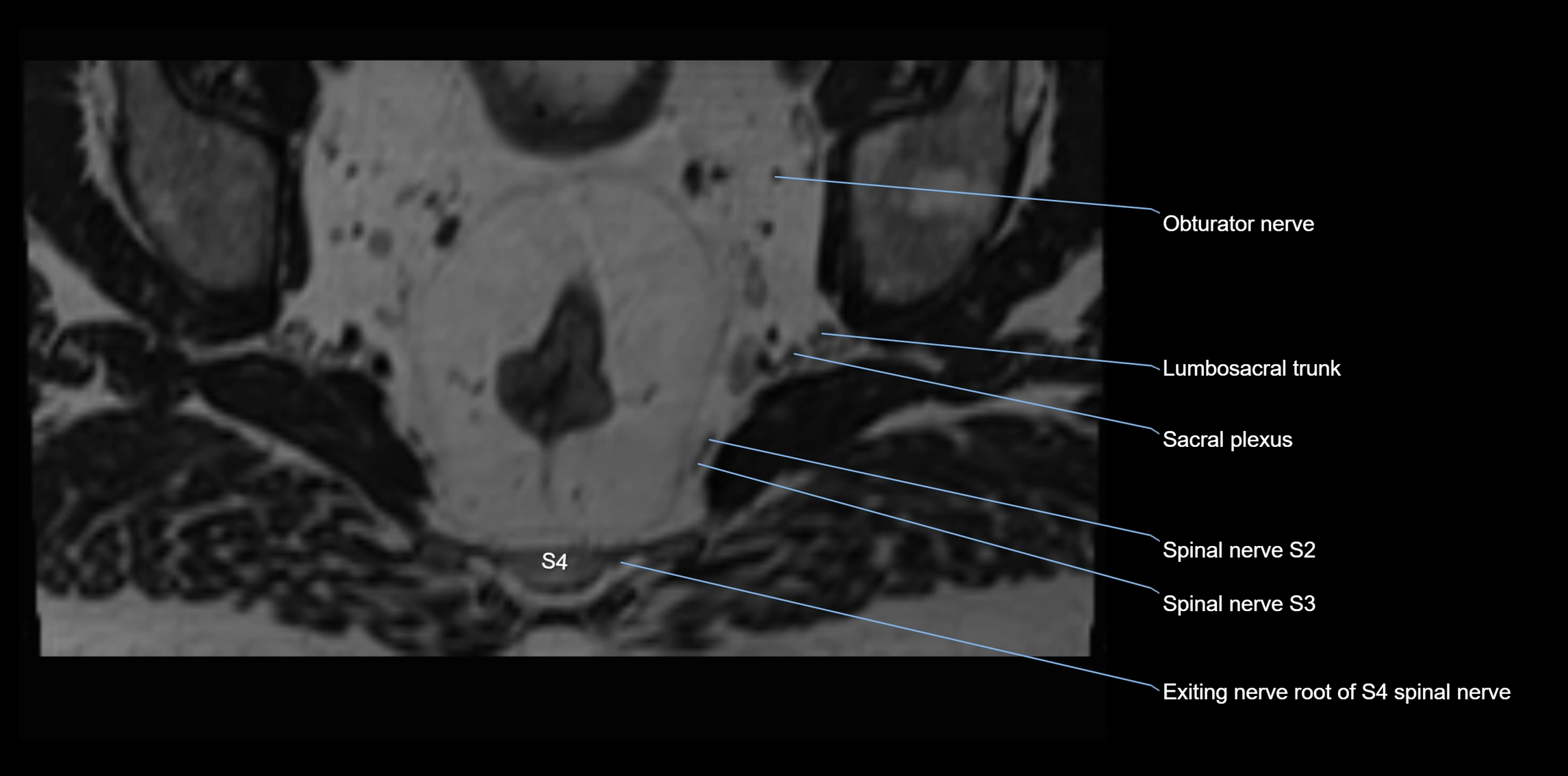
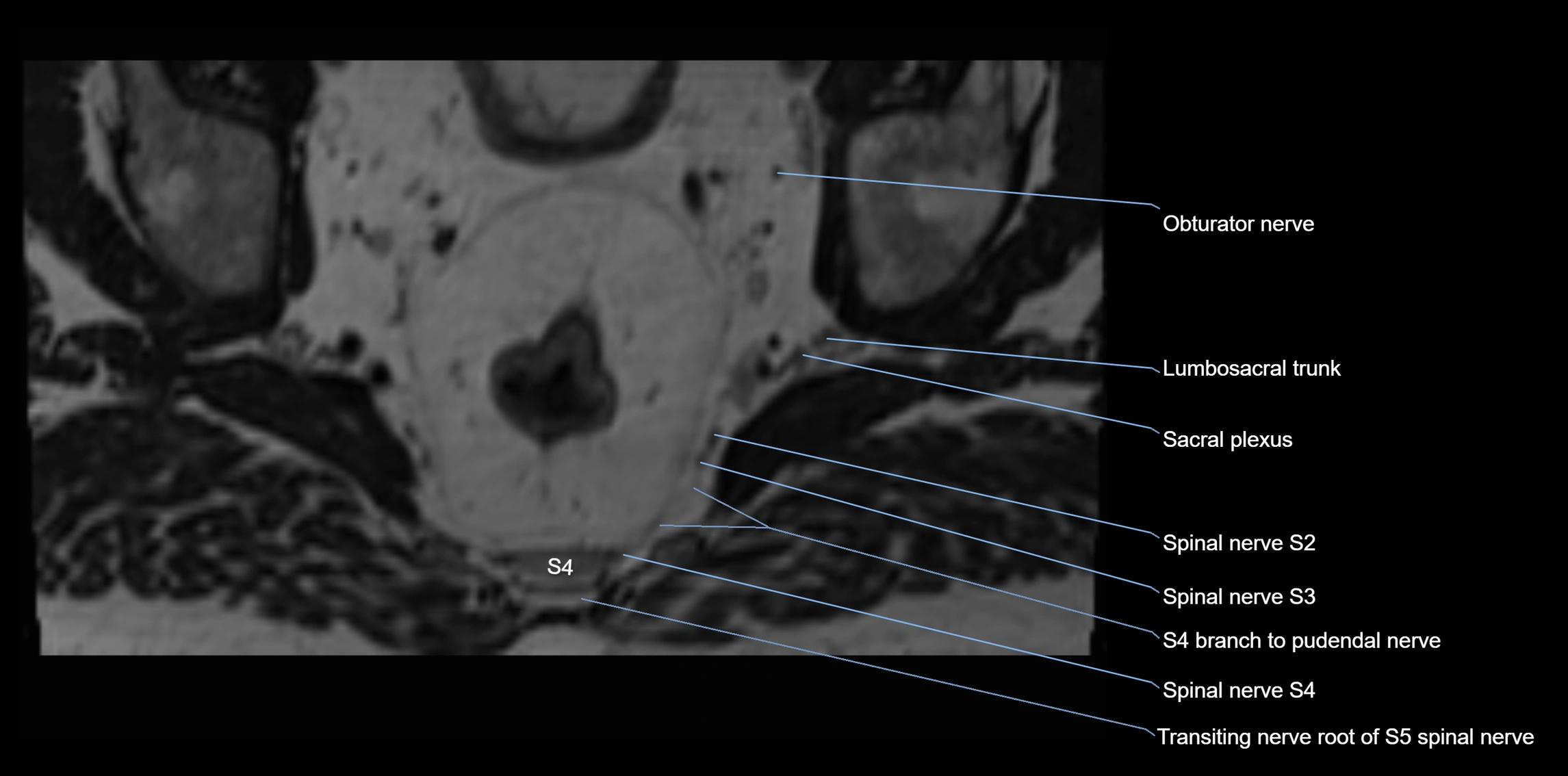
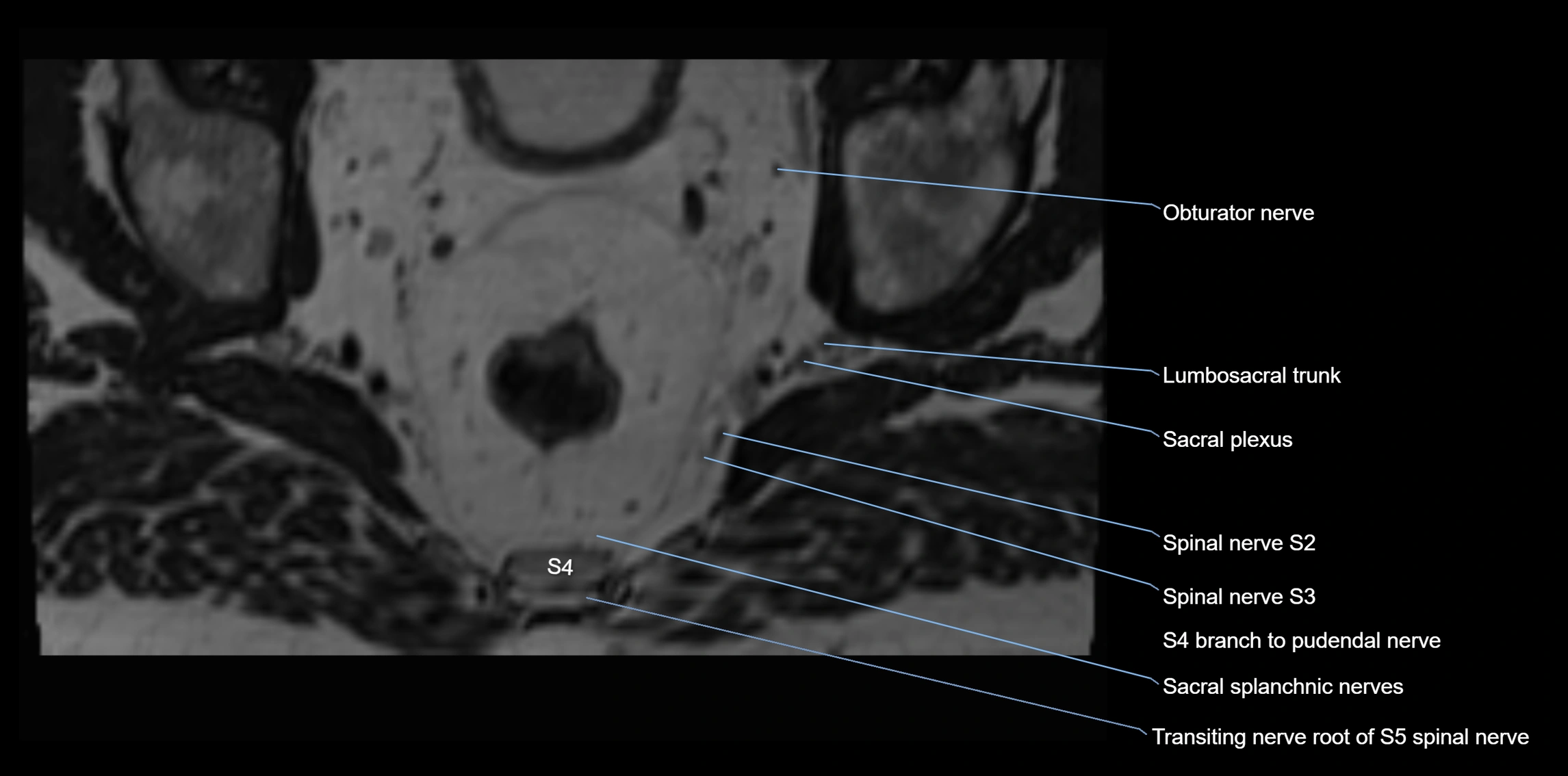
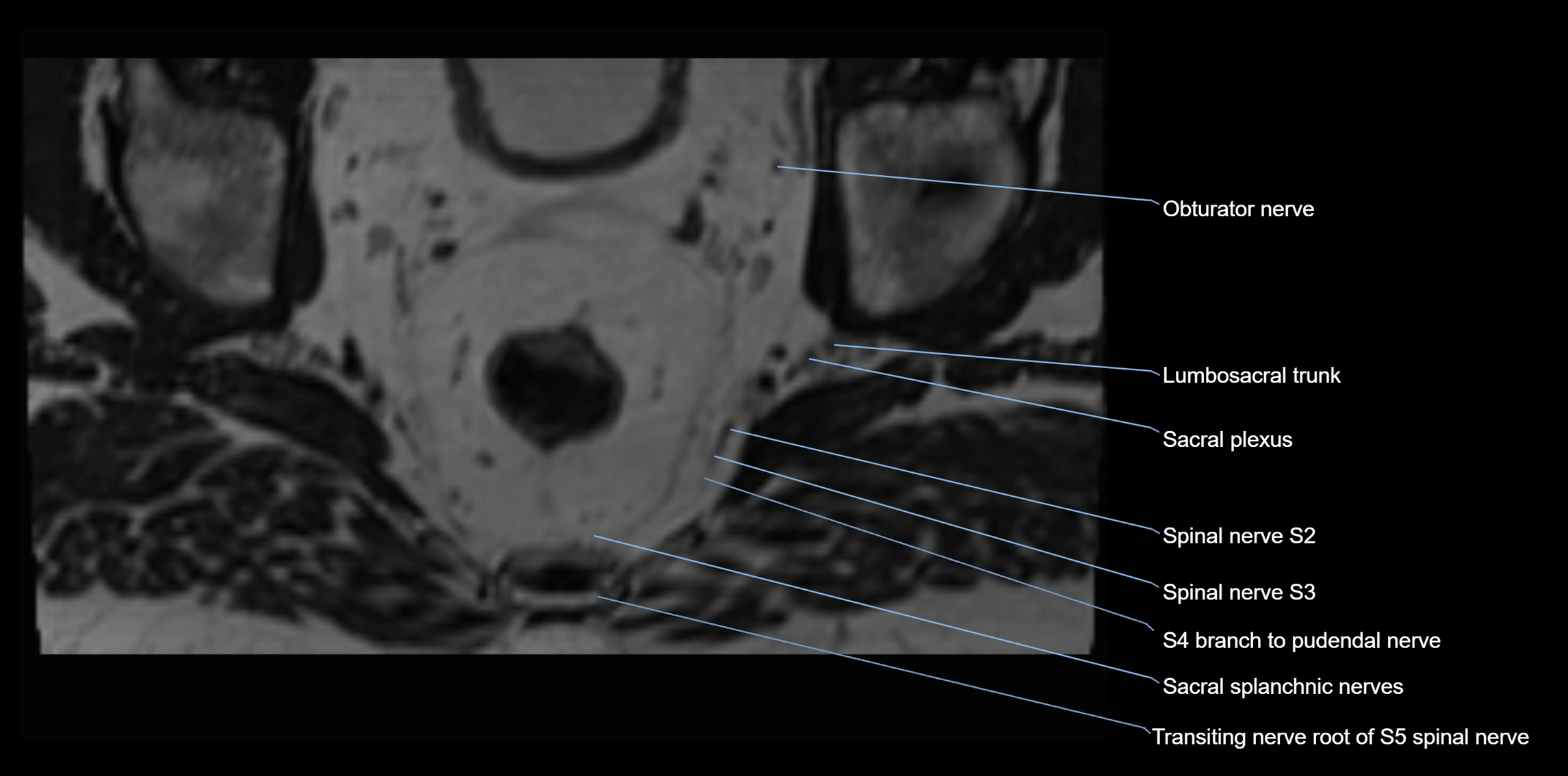
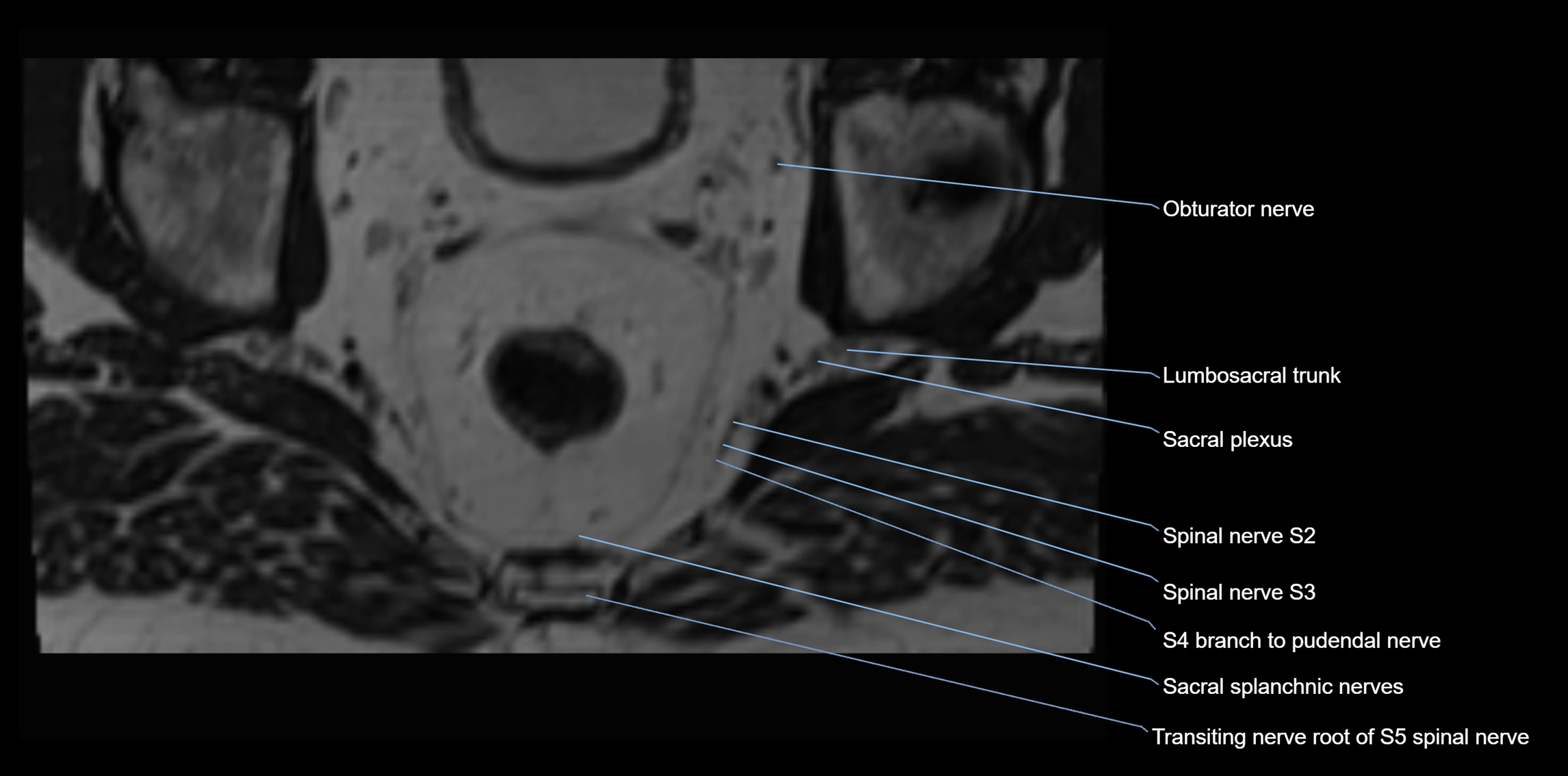
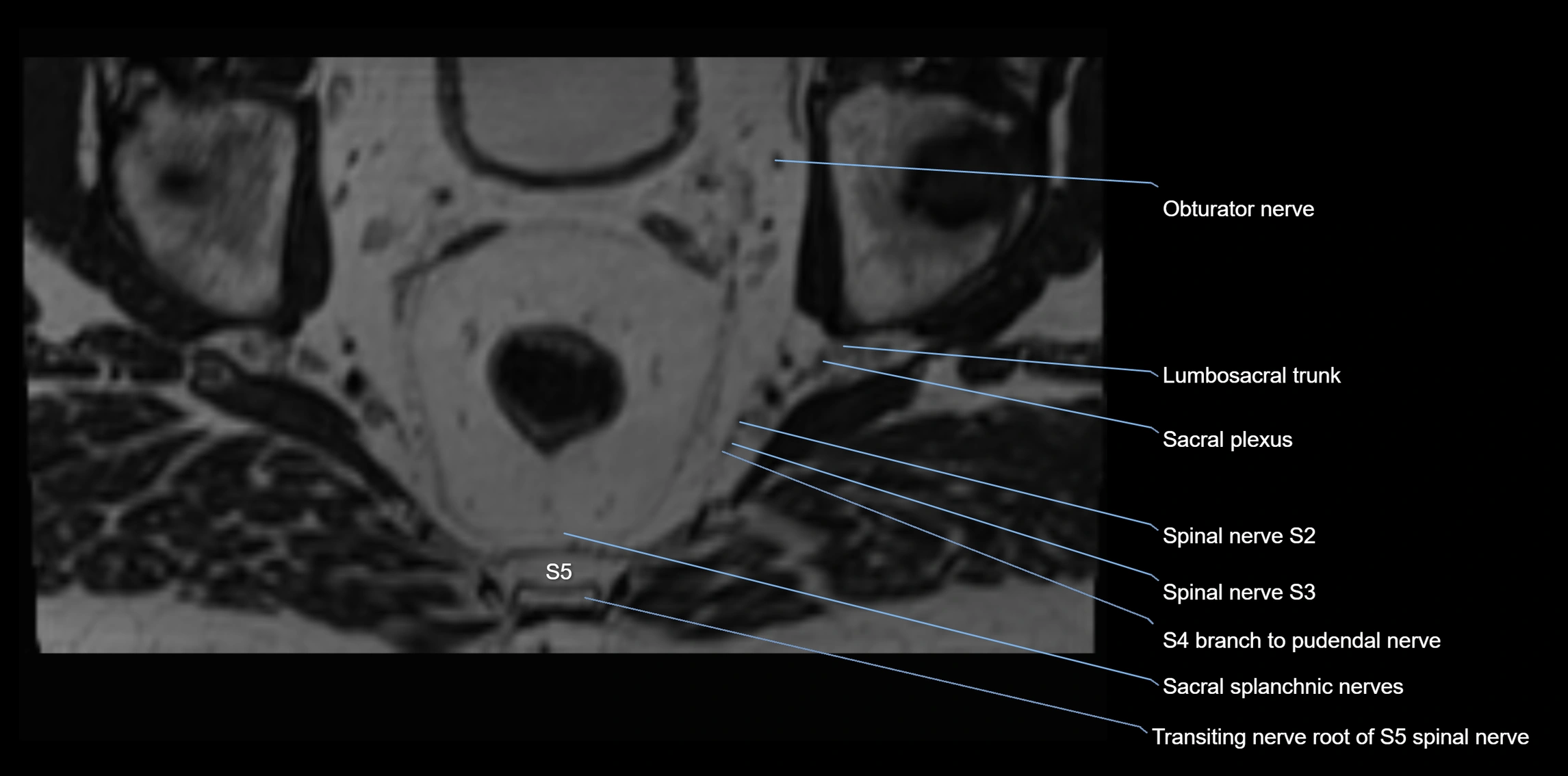
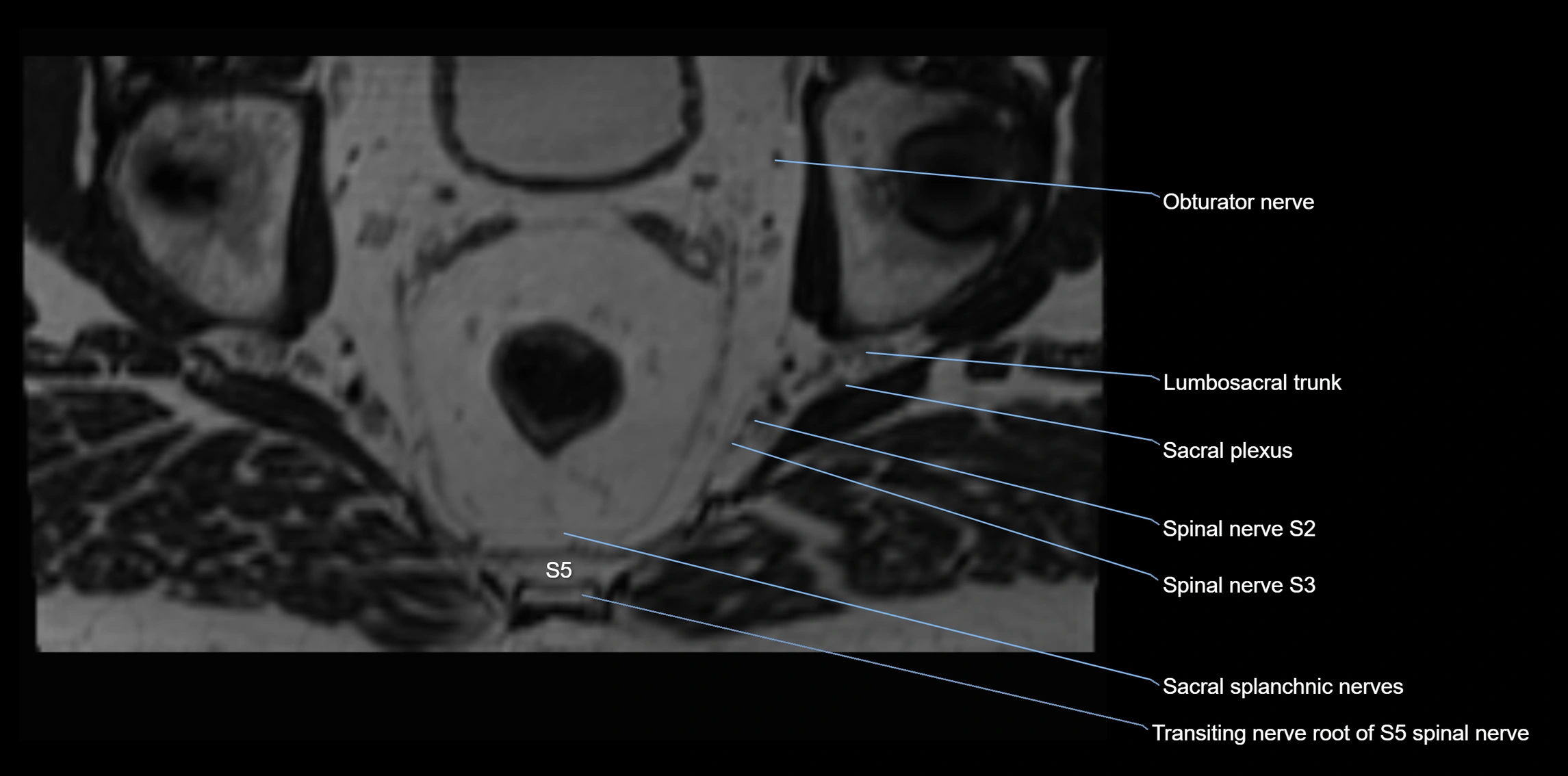
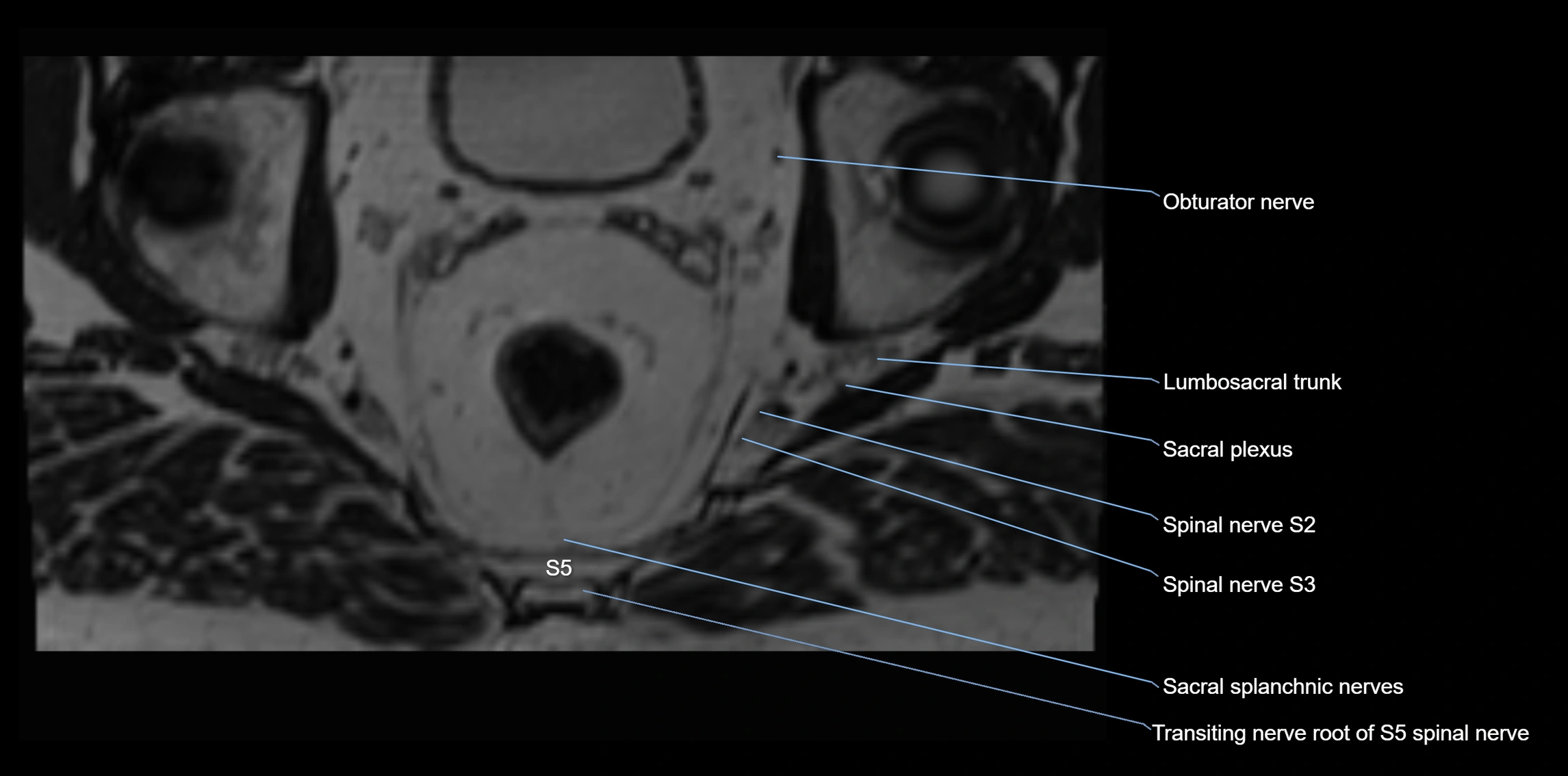
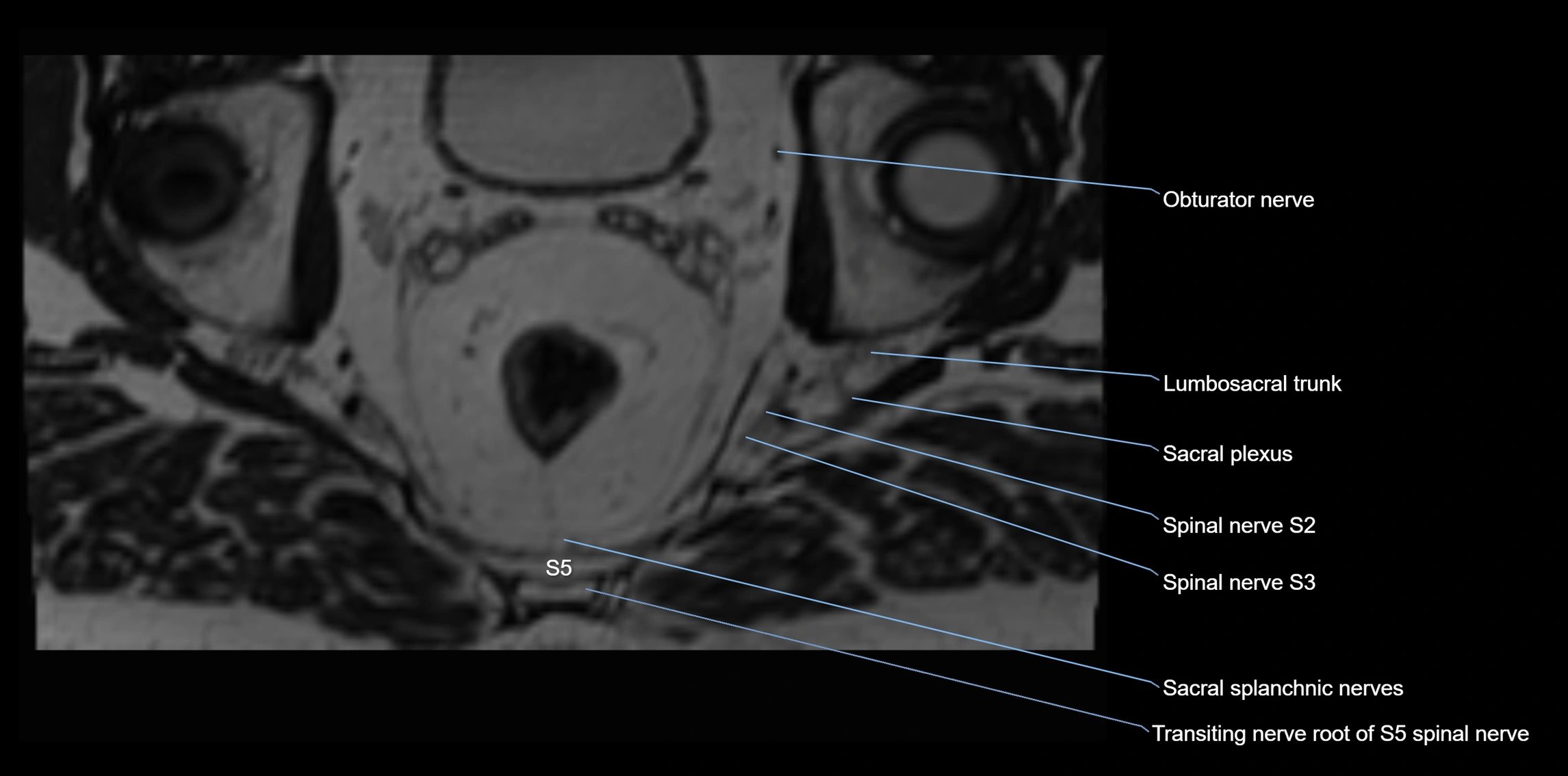
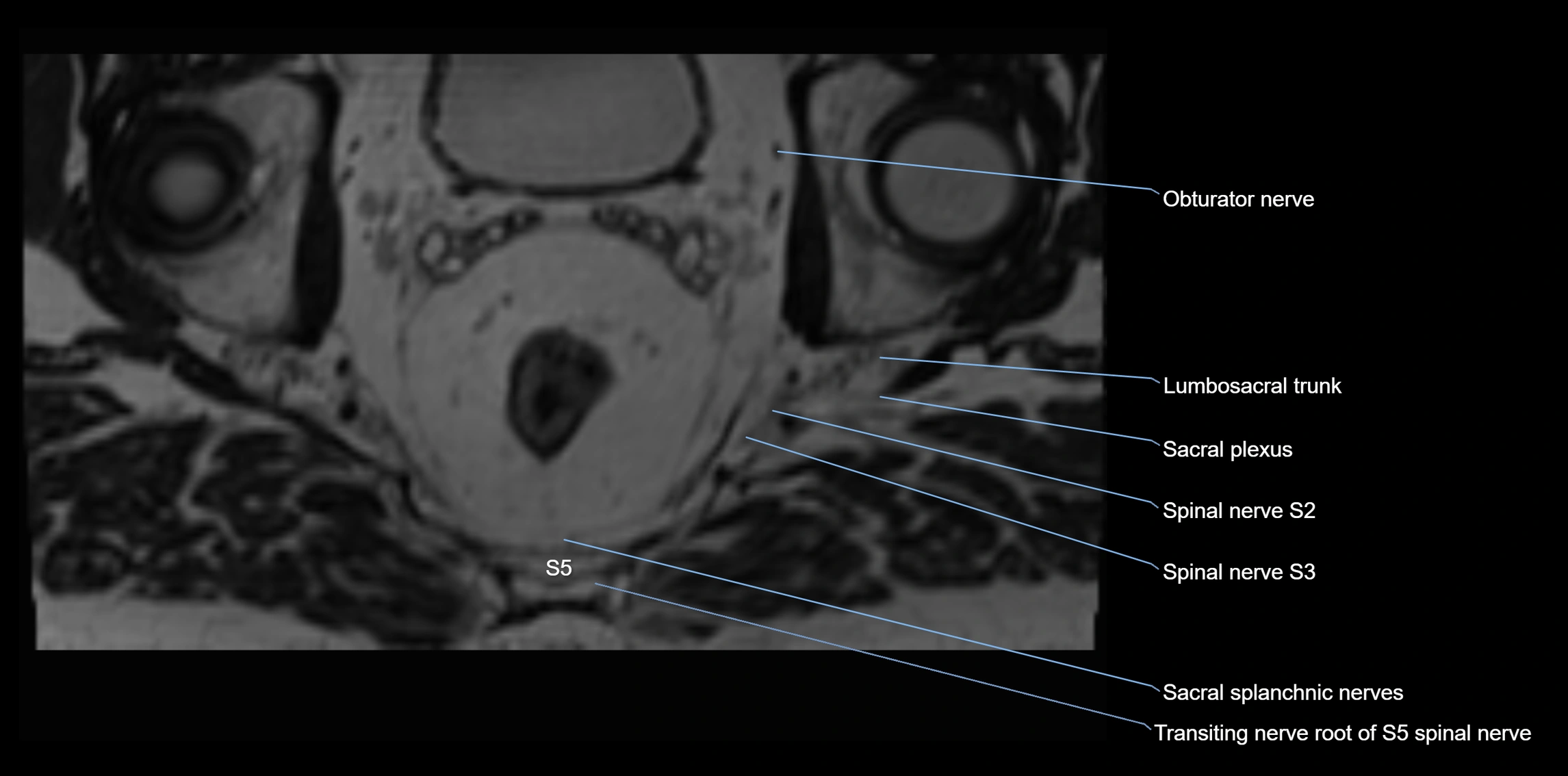
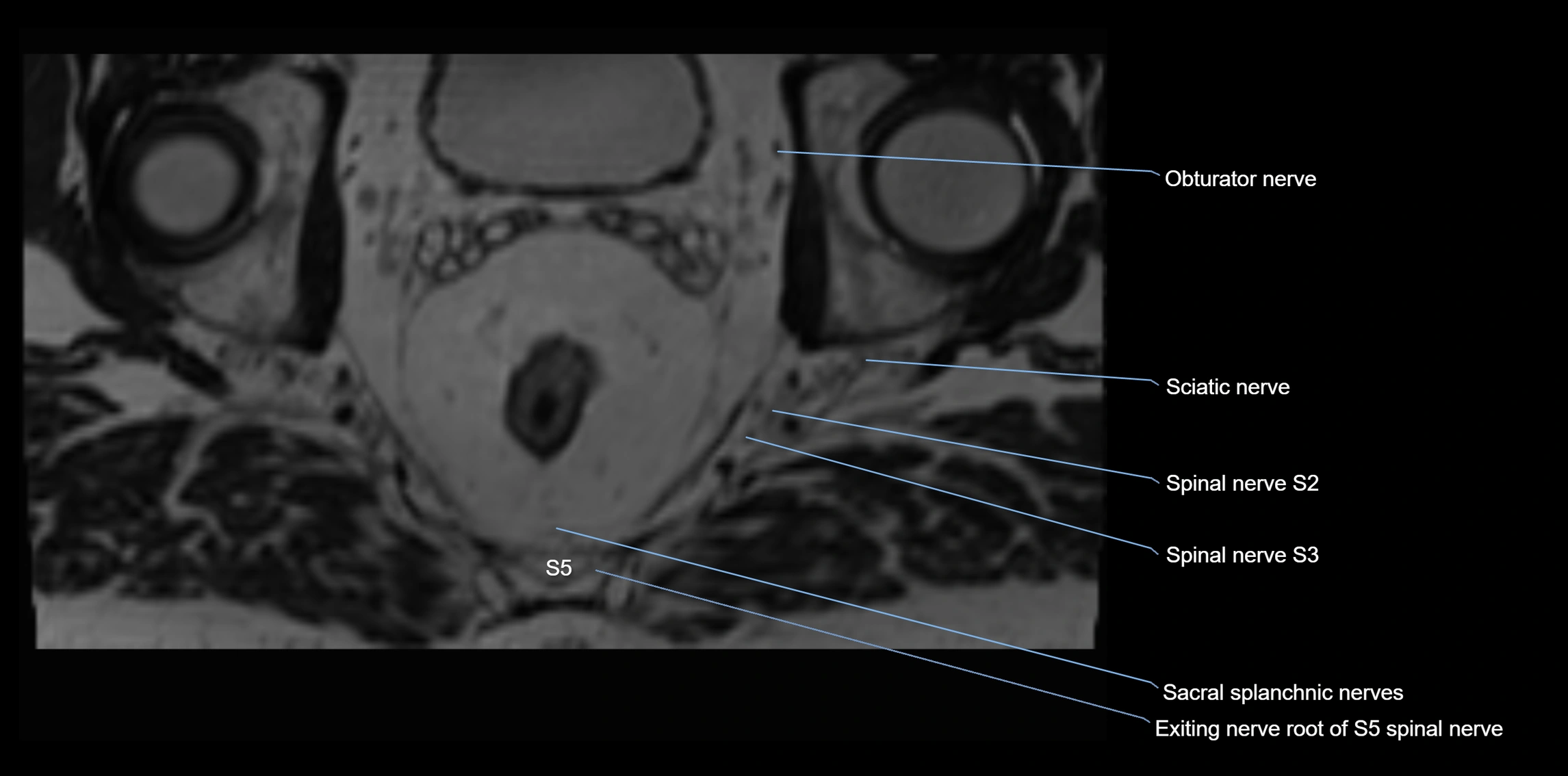
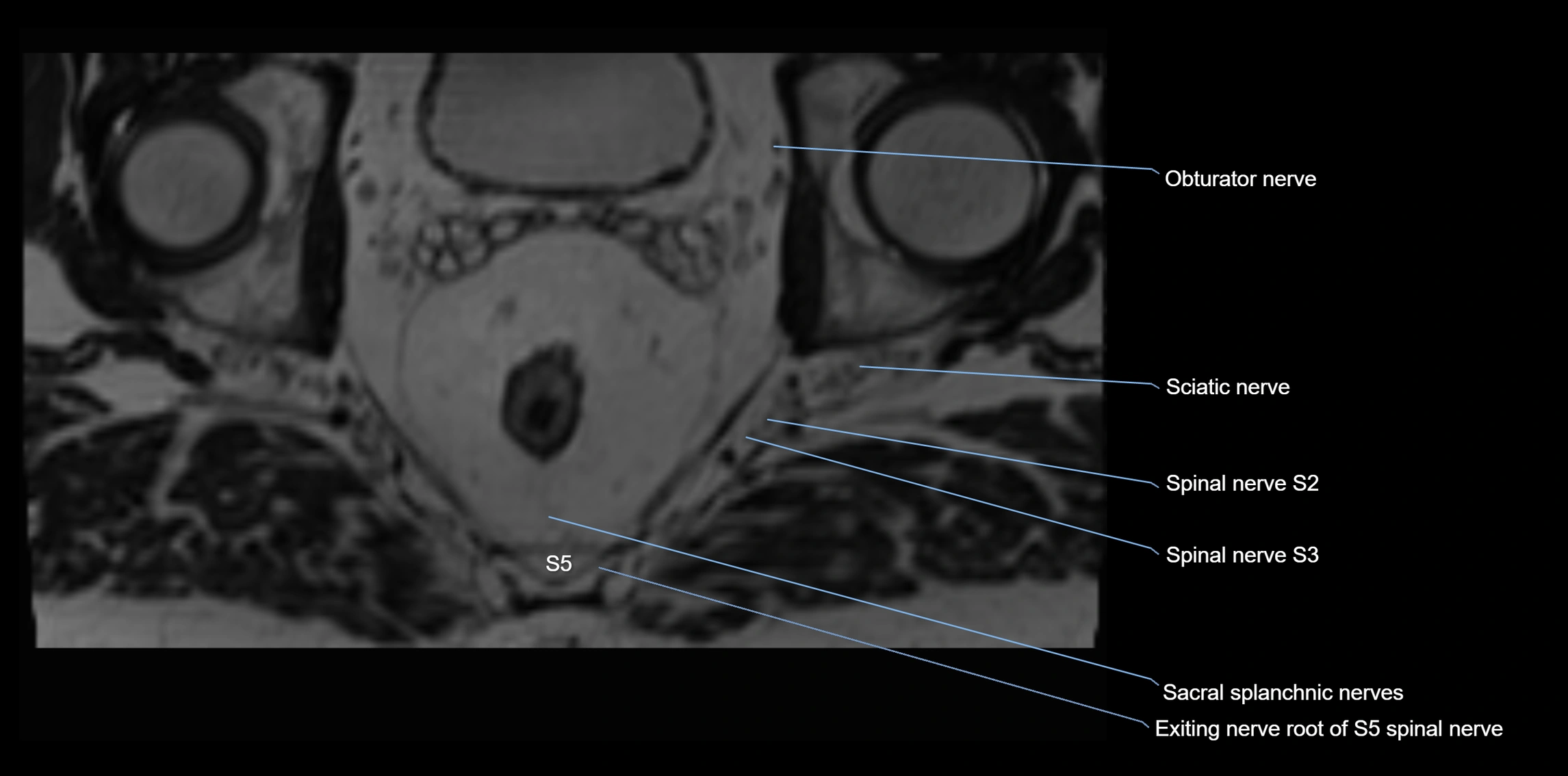
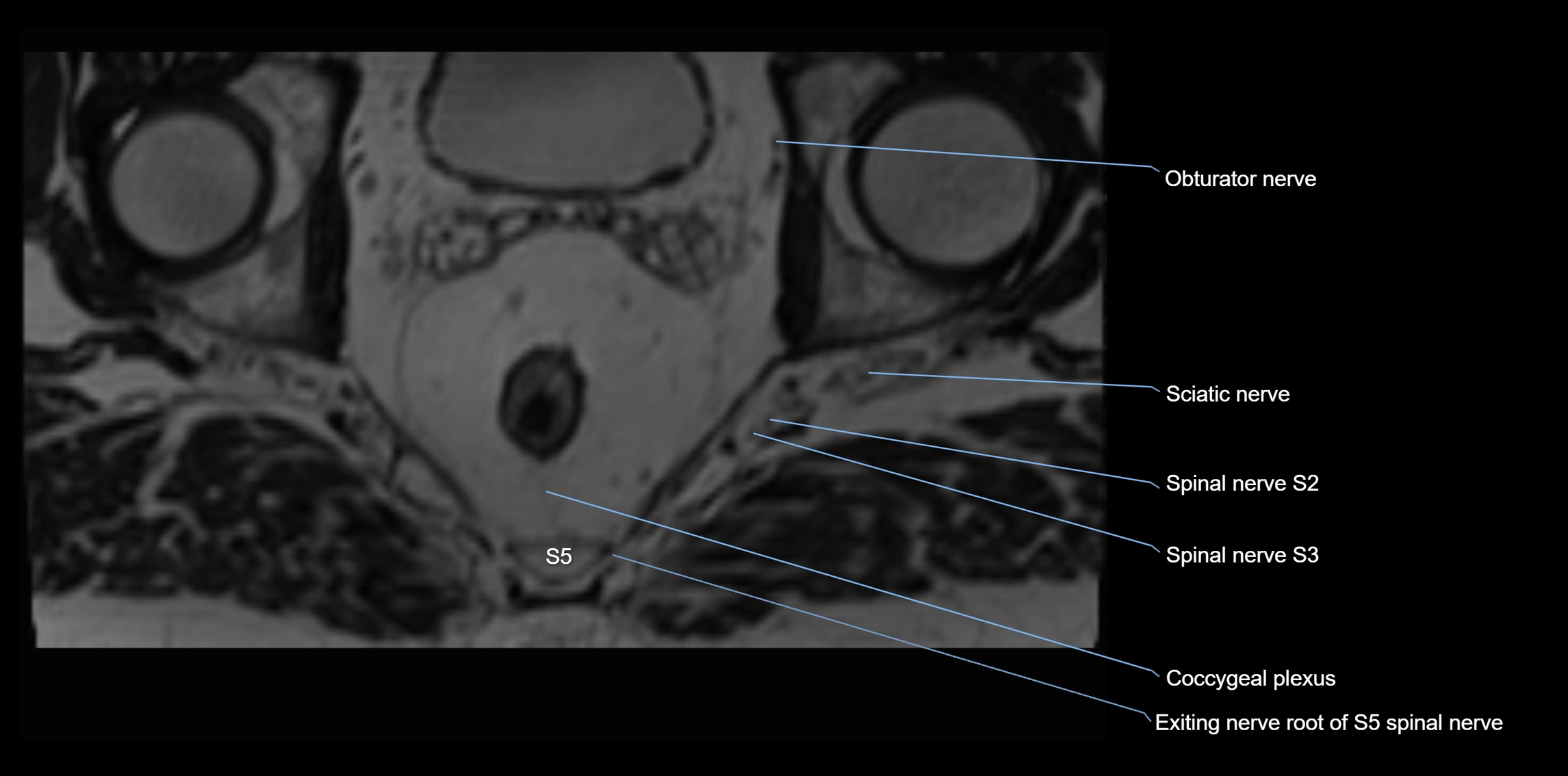
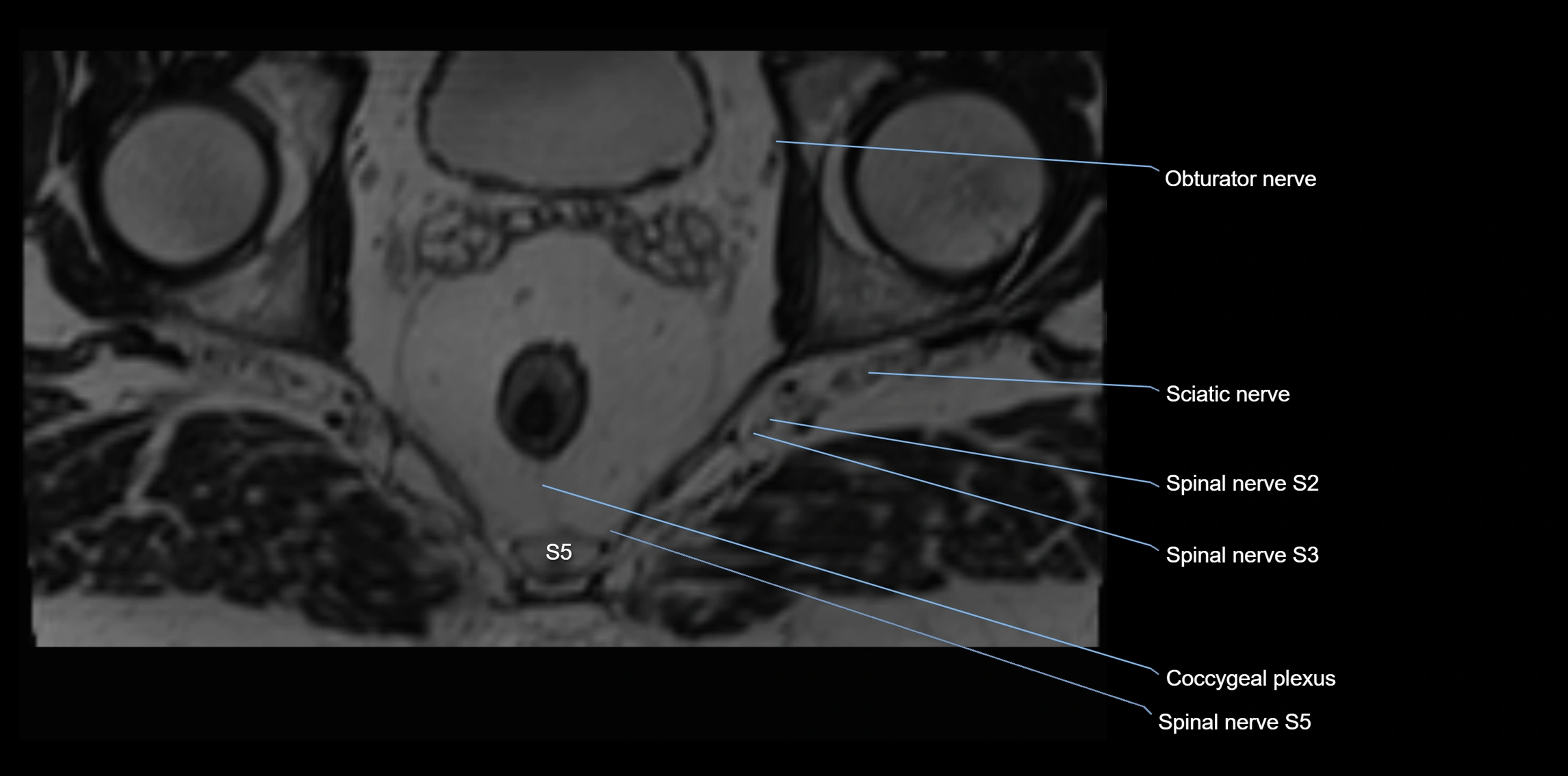
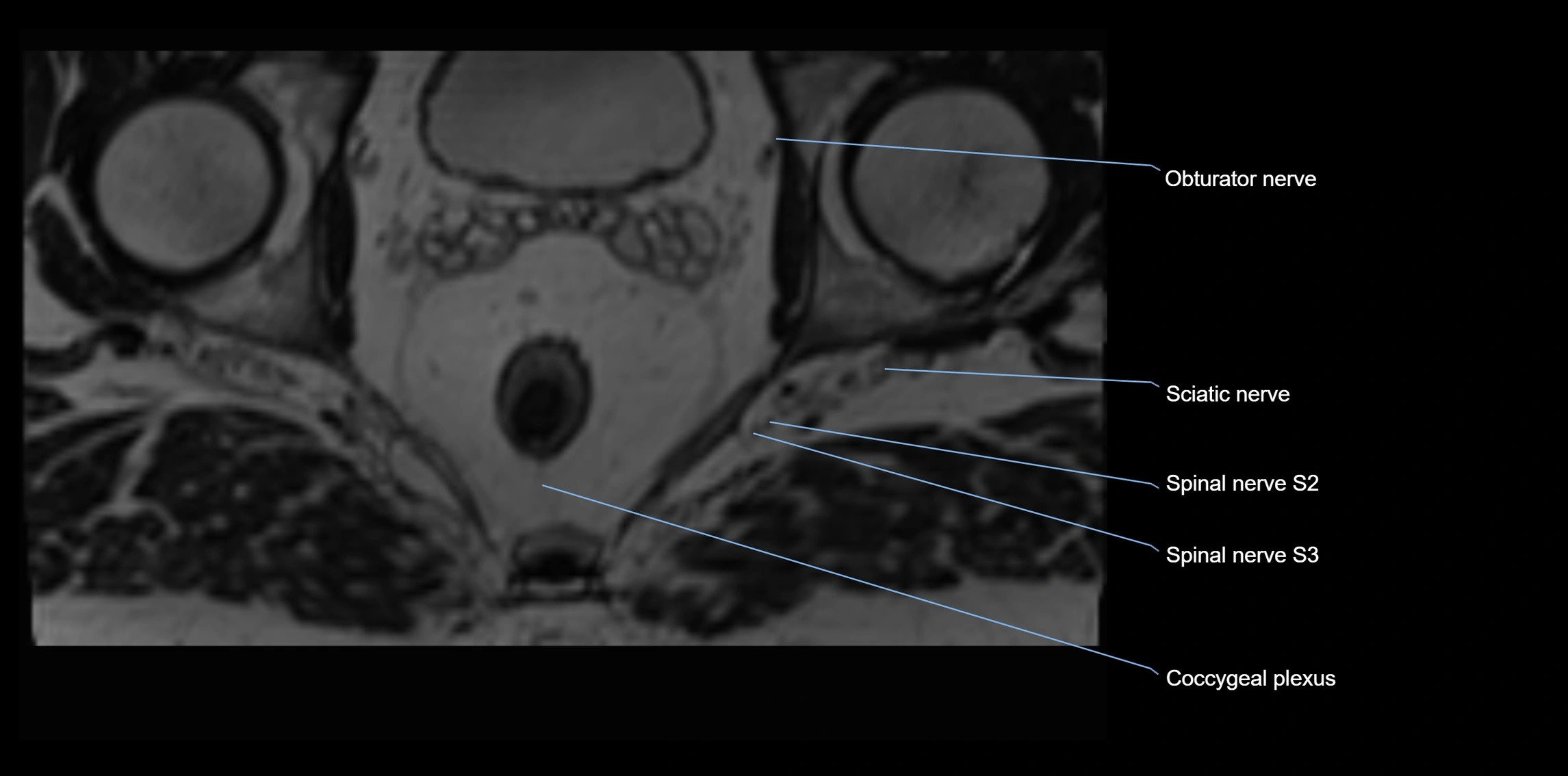
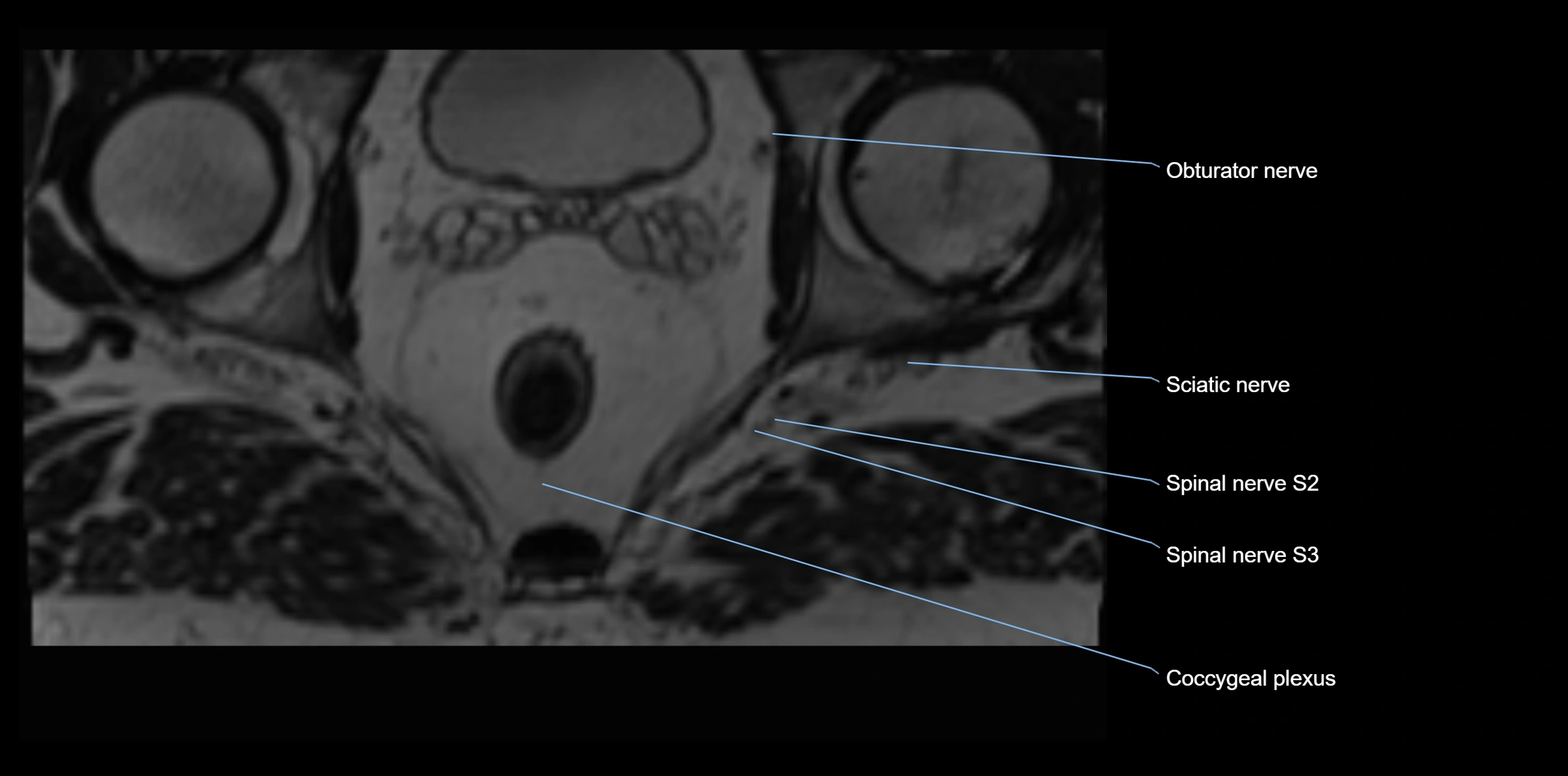
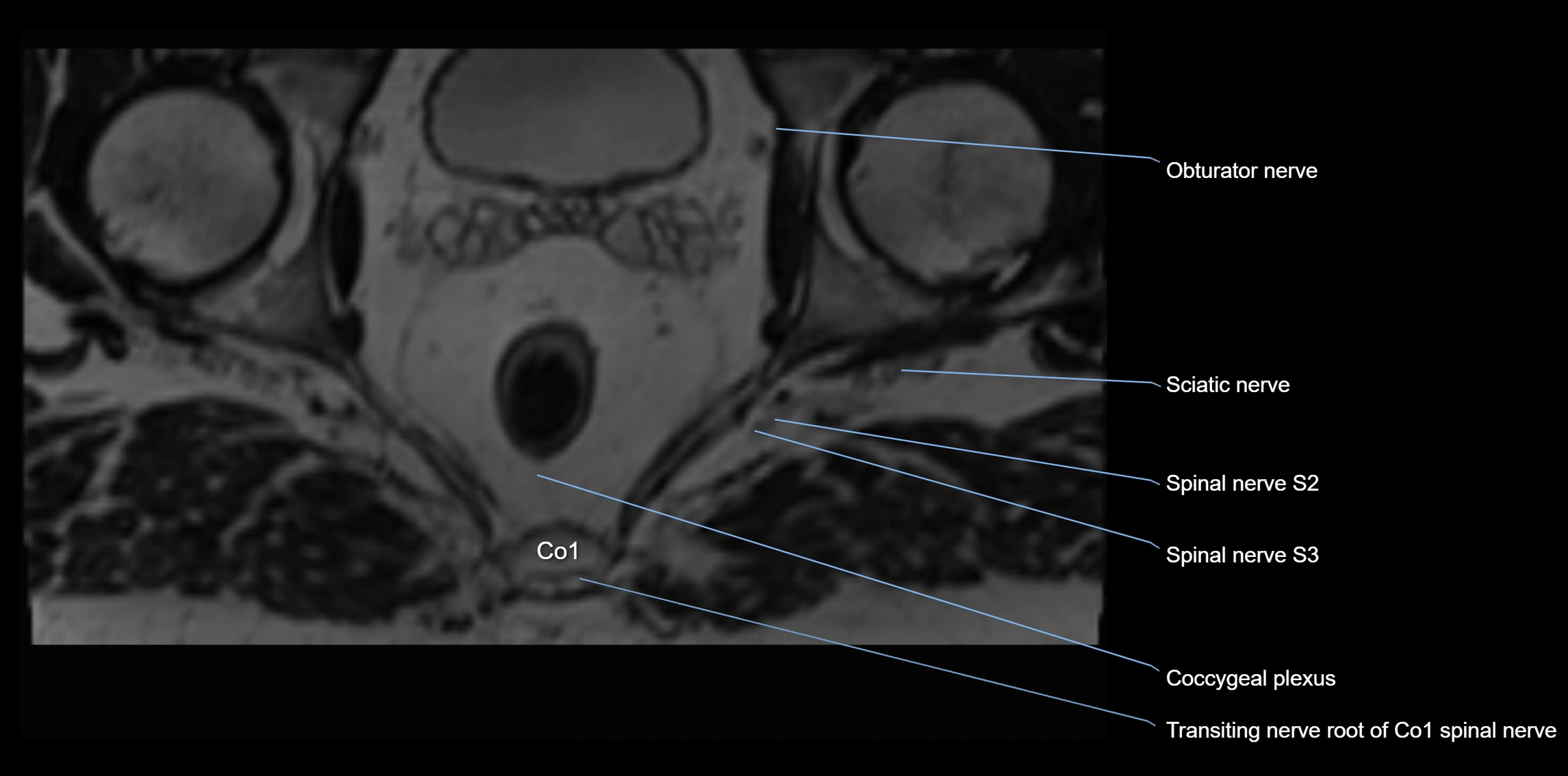
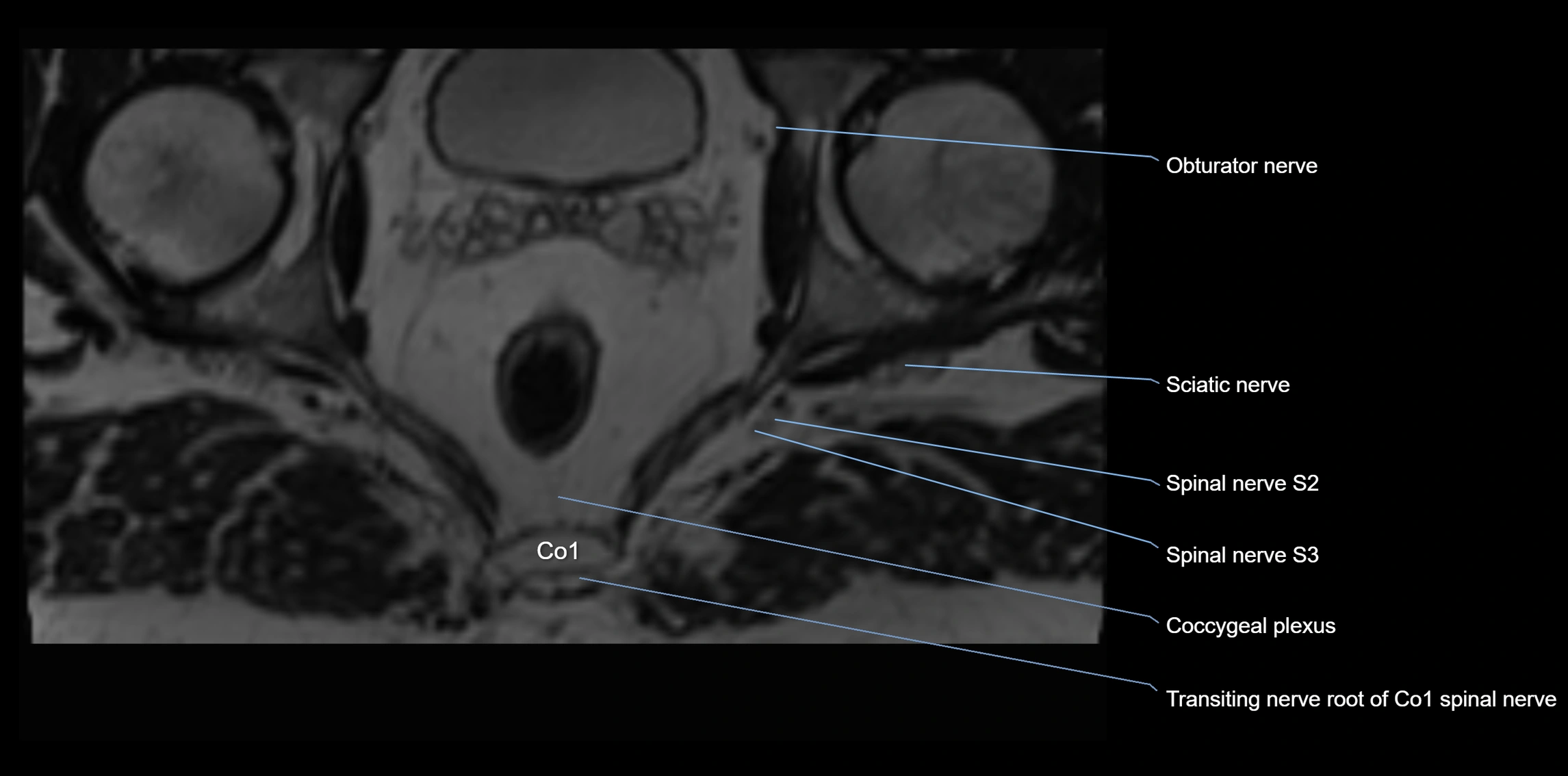
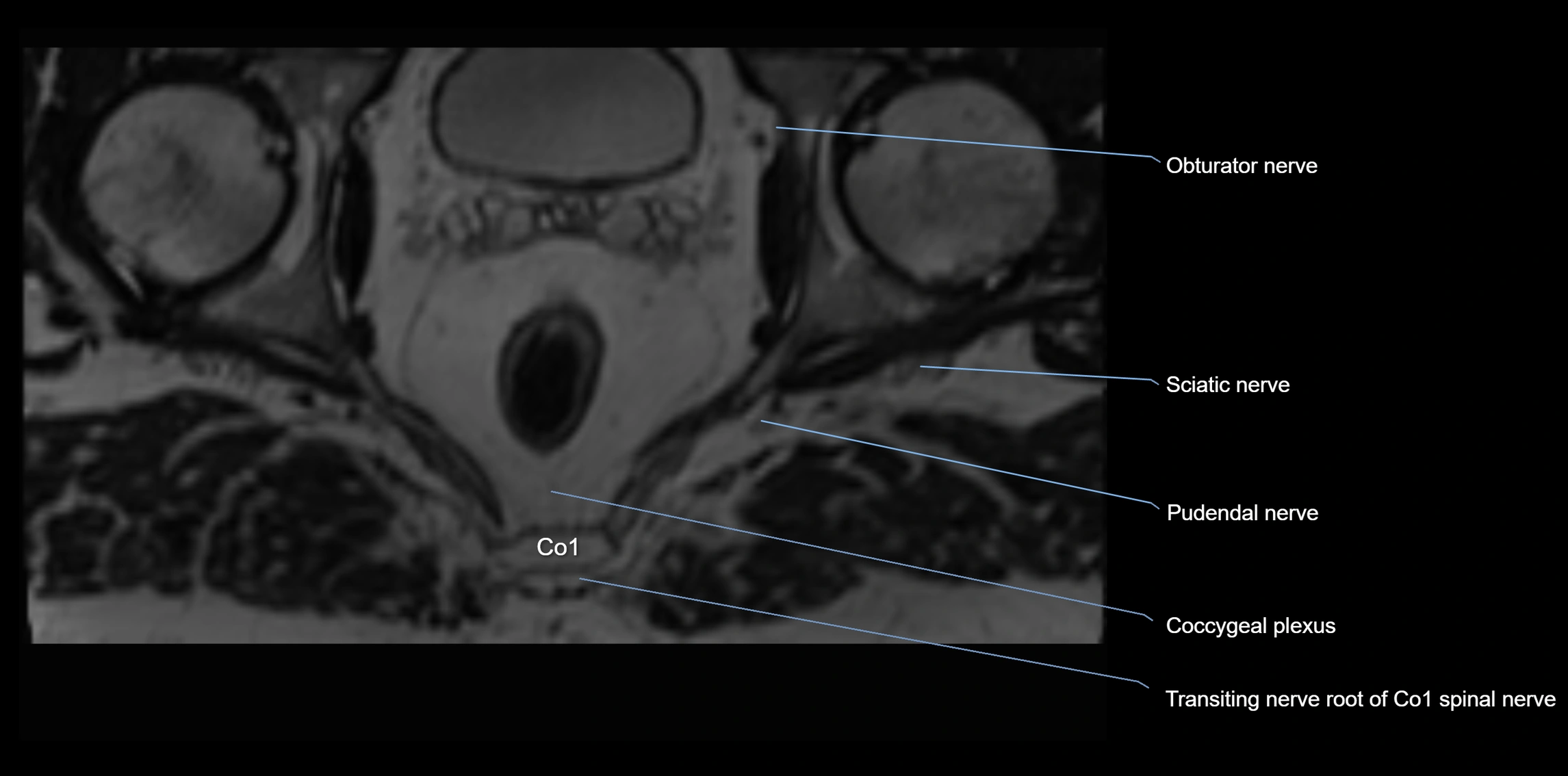
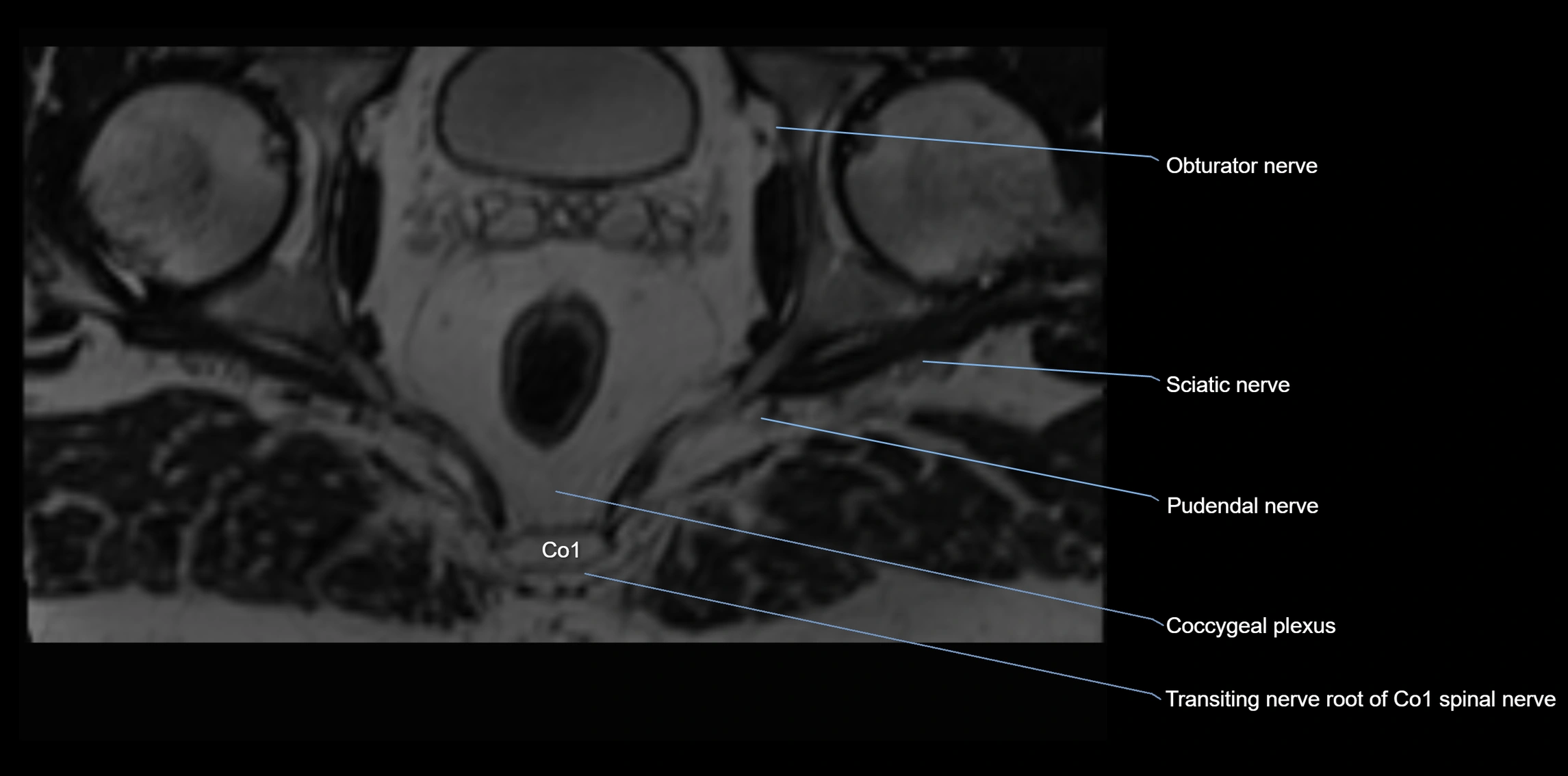
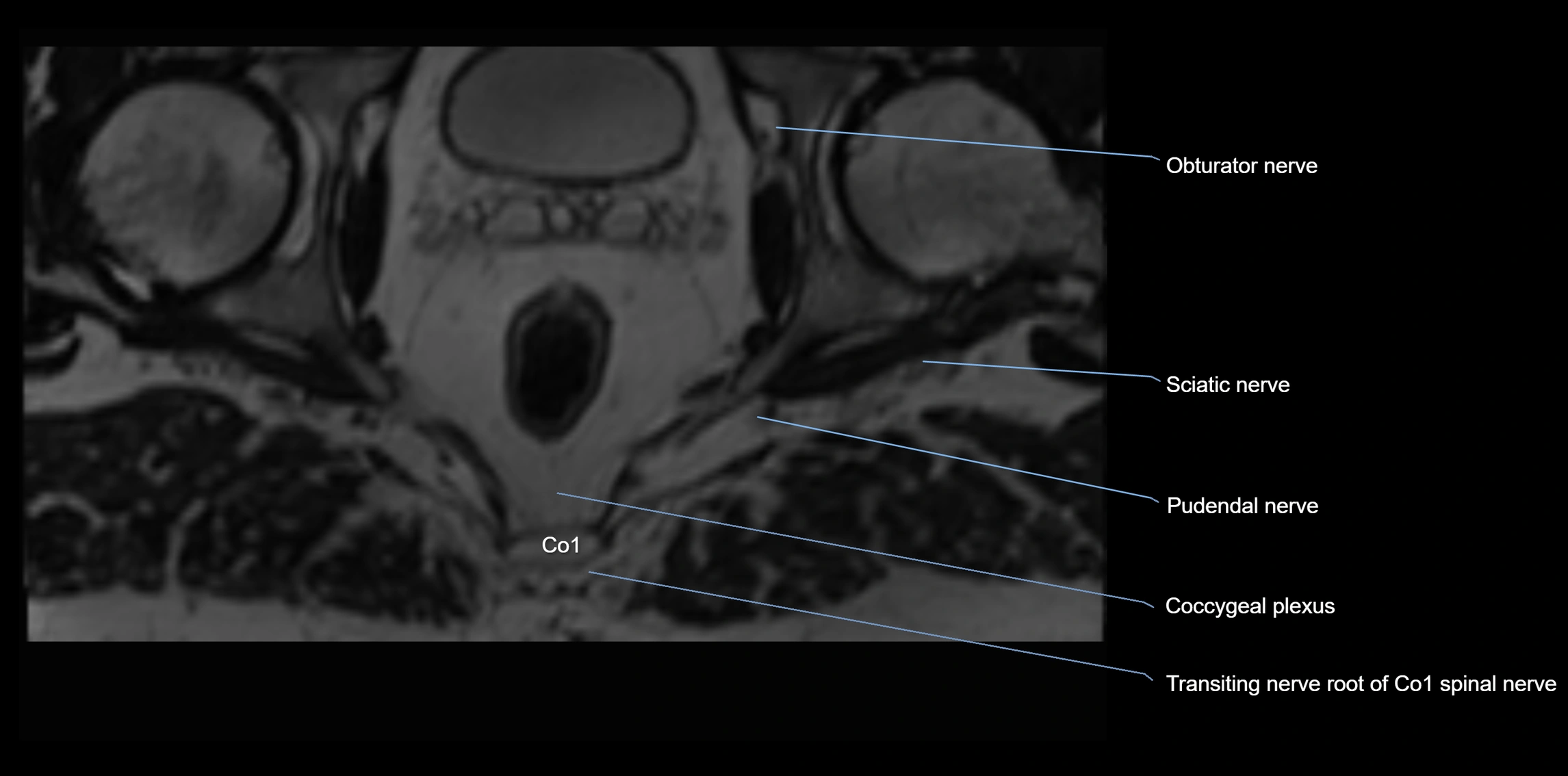
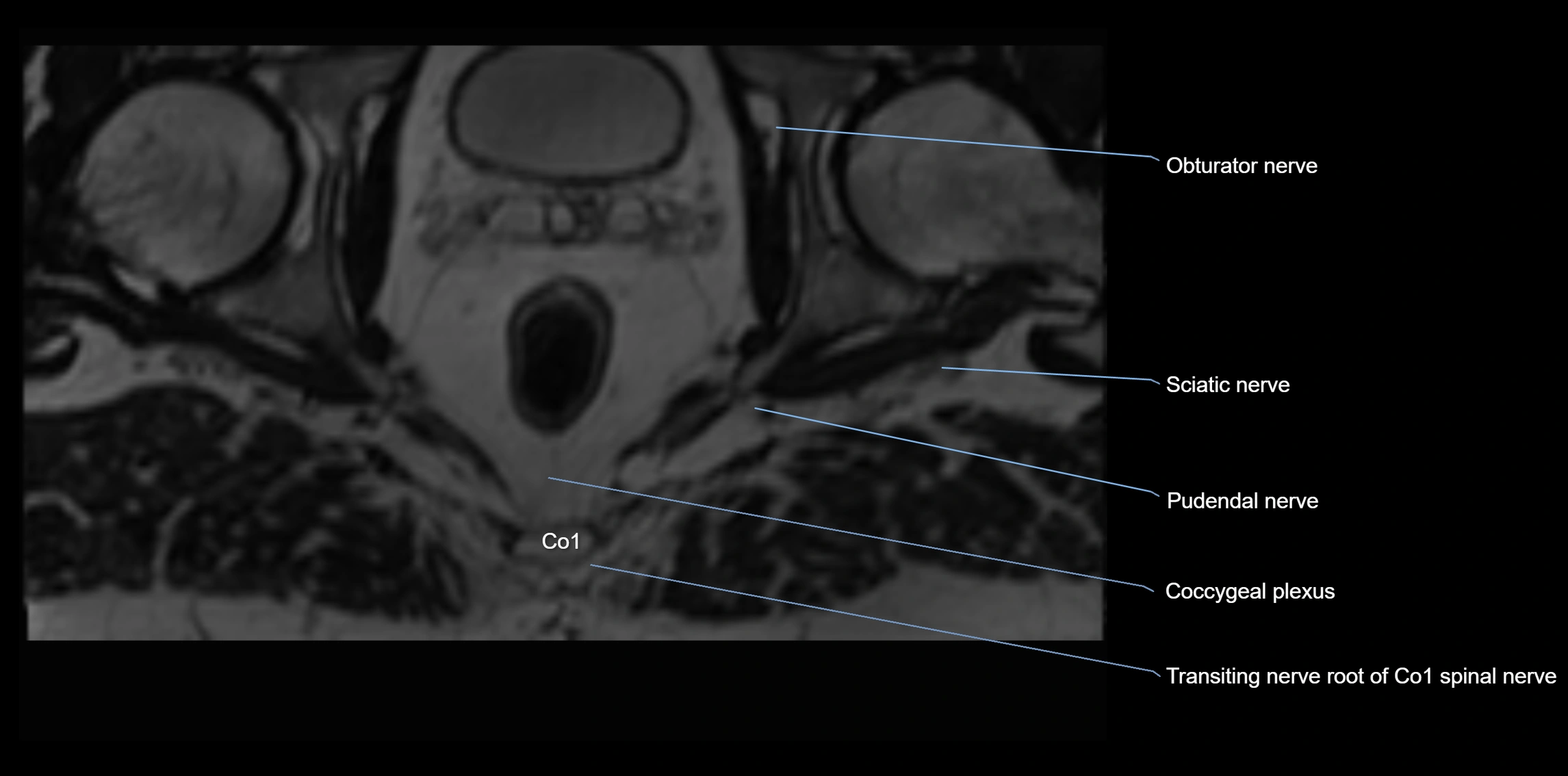
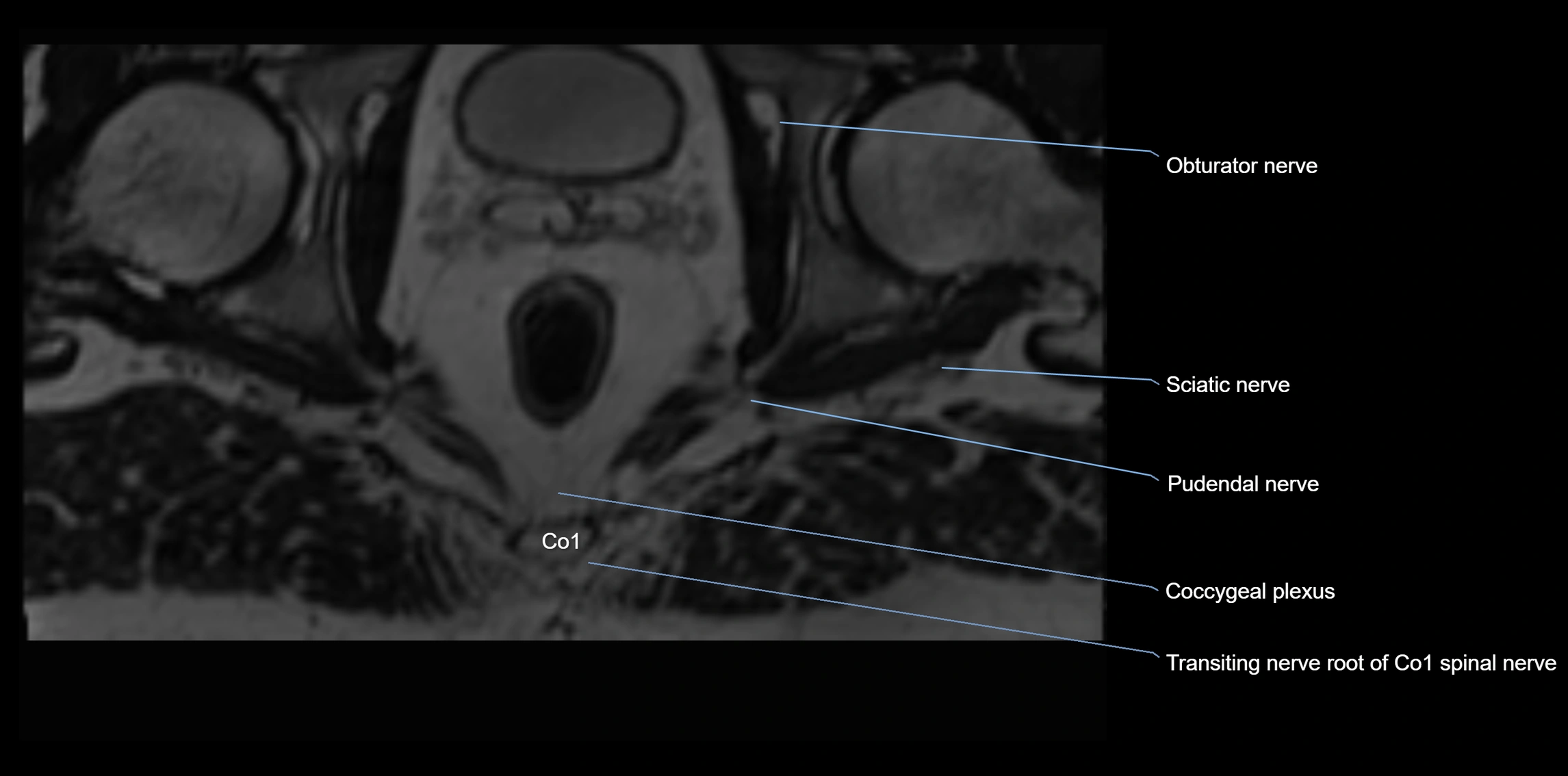
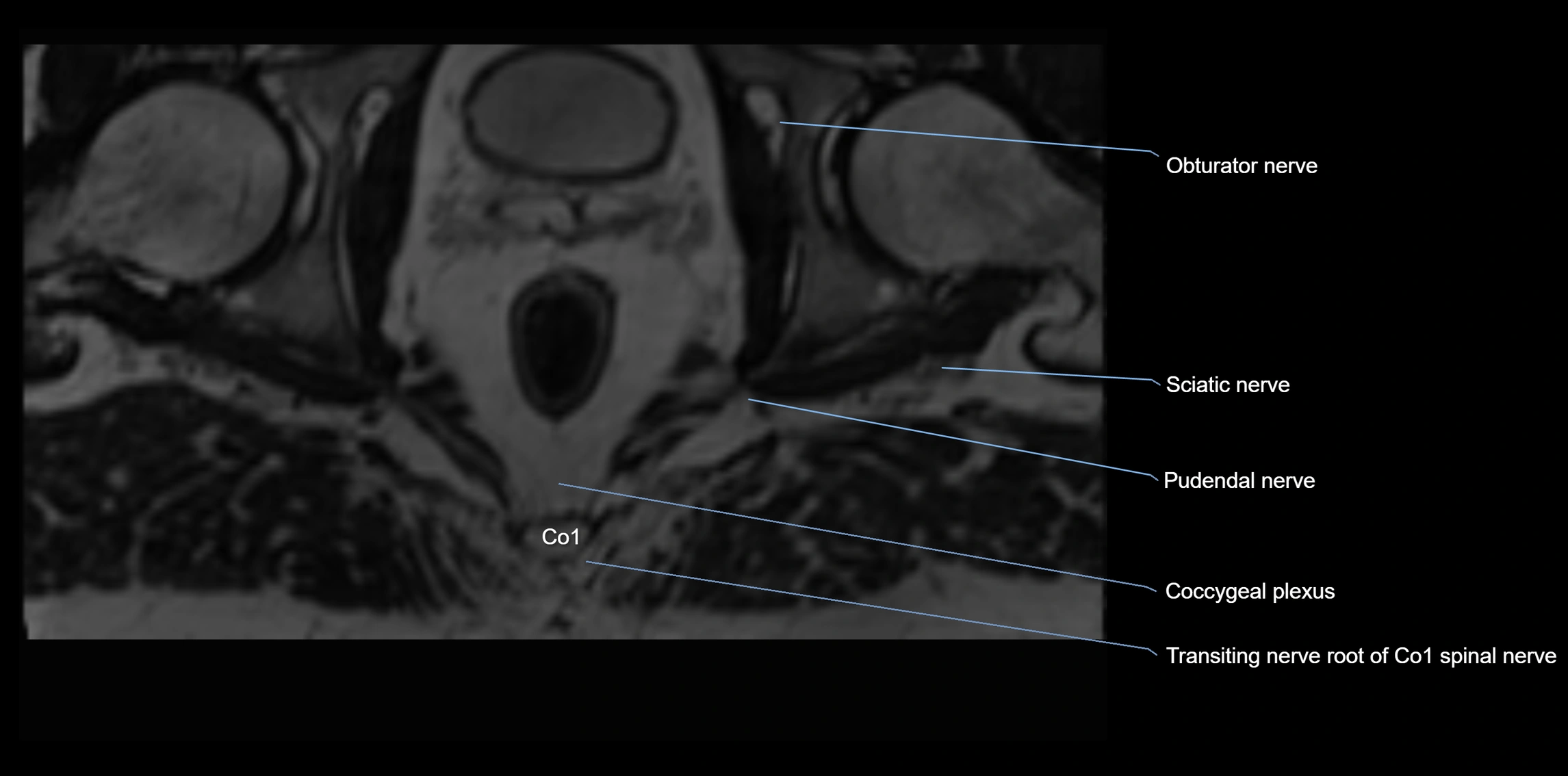
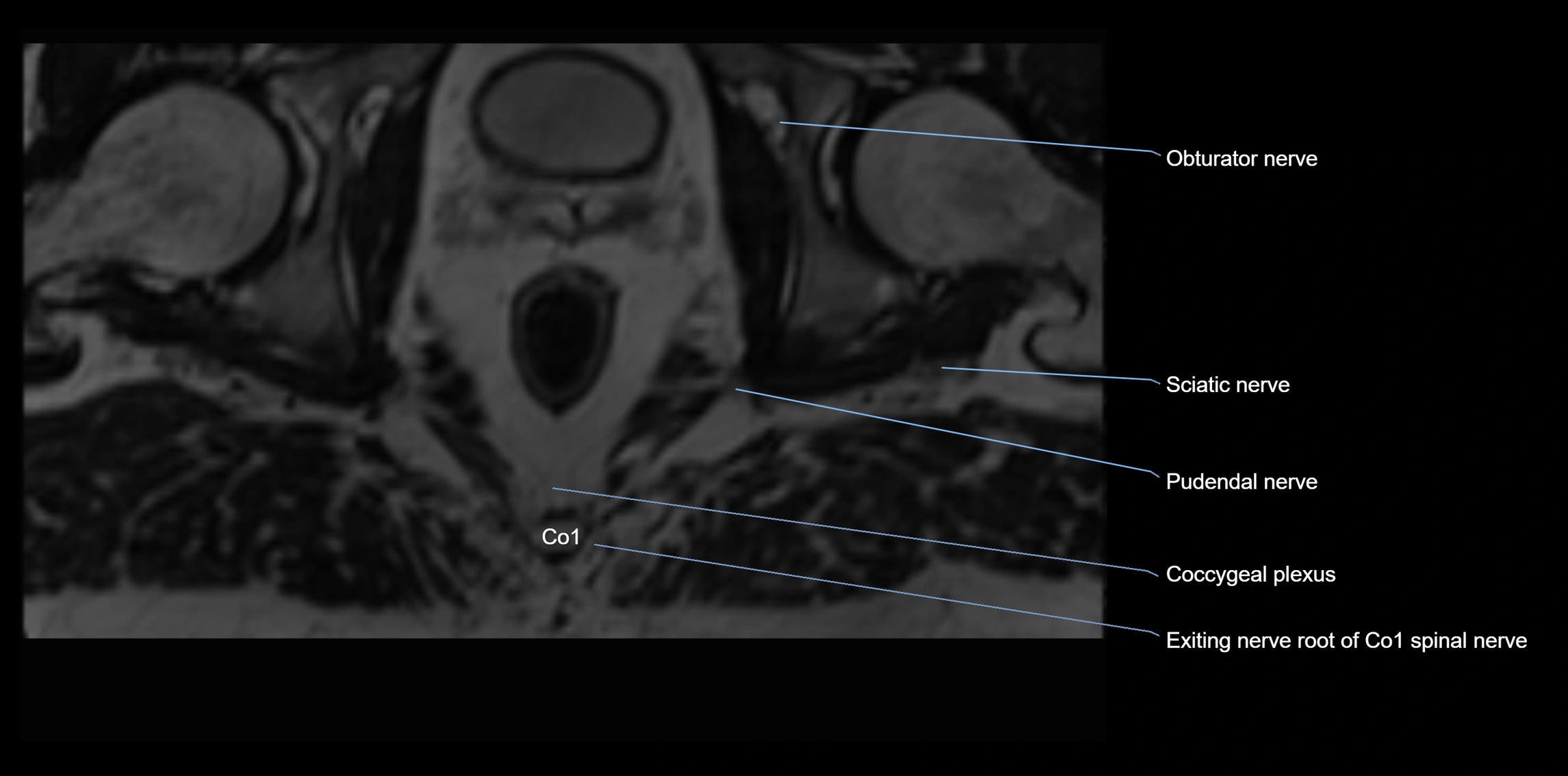
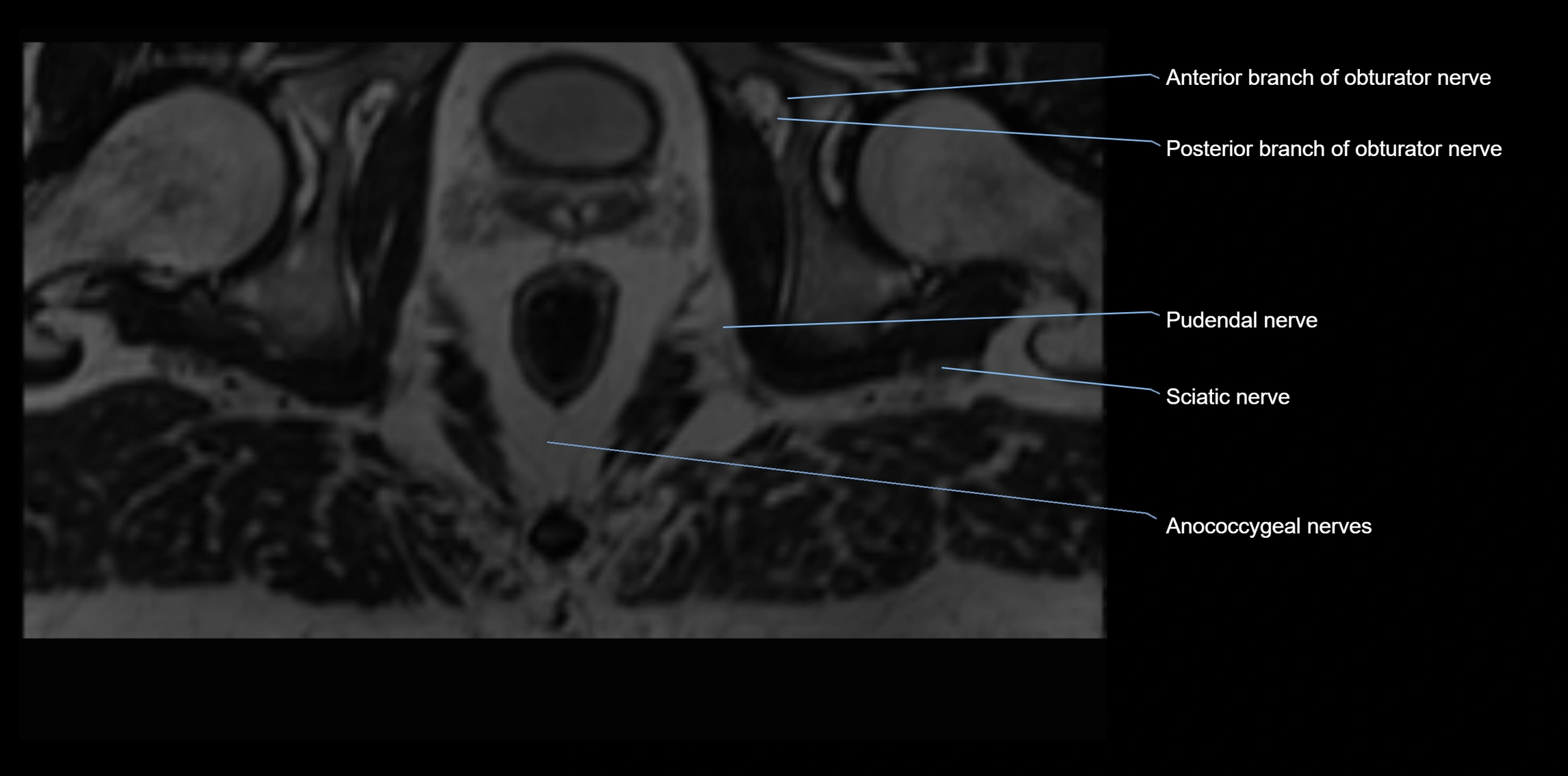
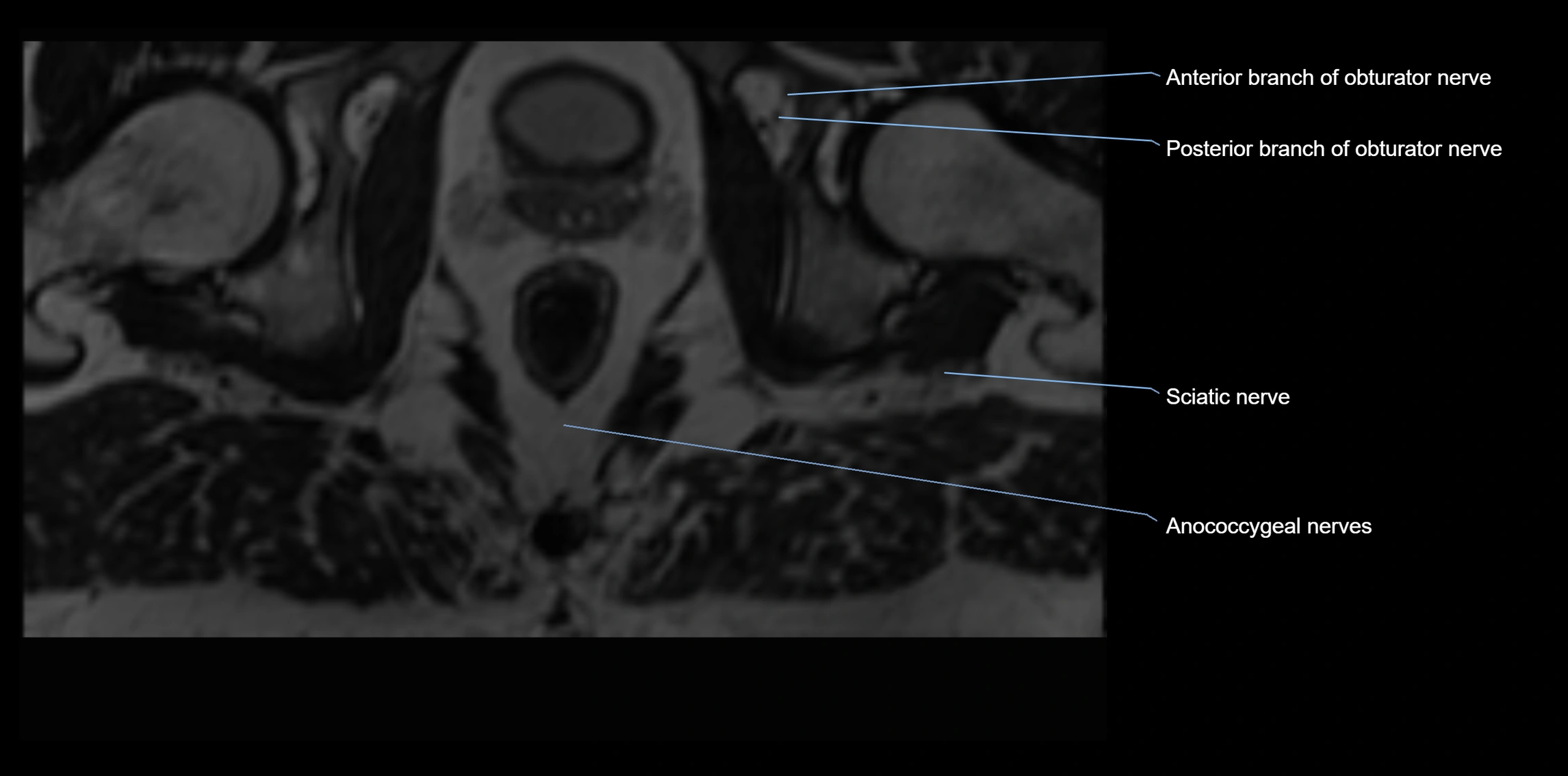
MRI image