


Topic
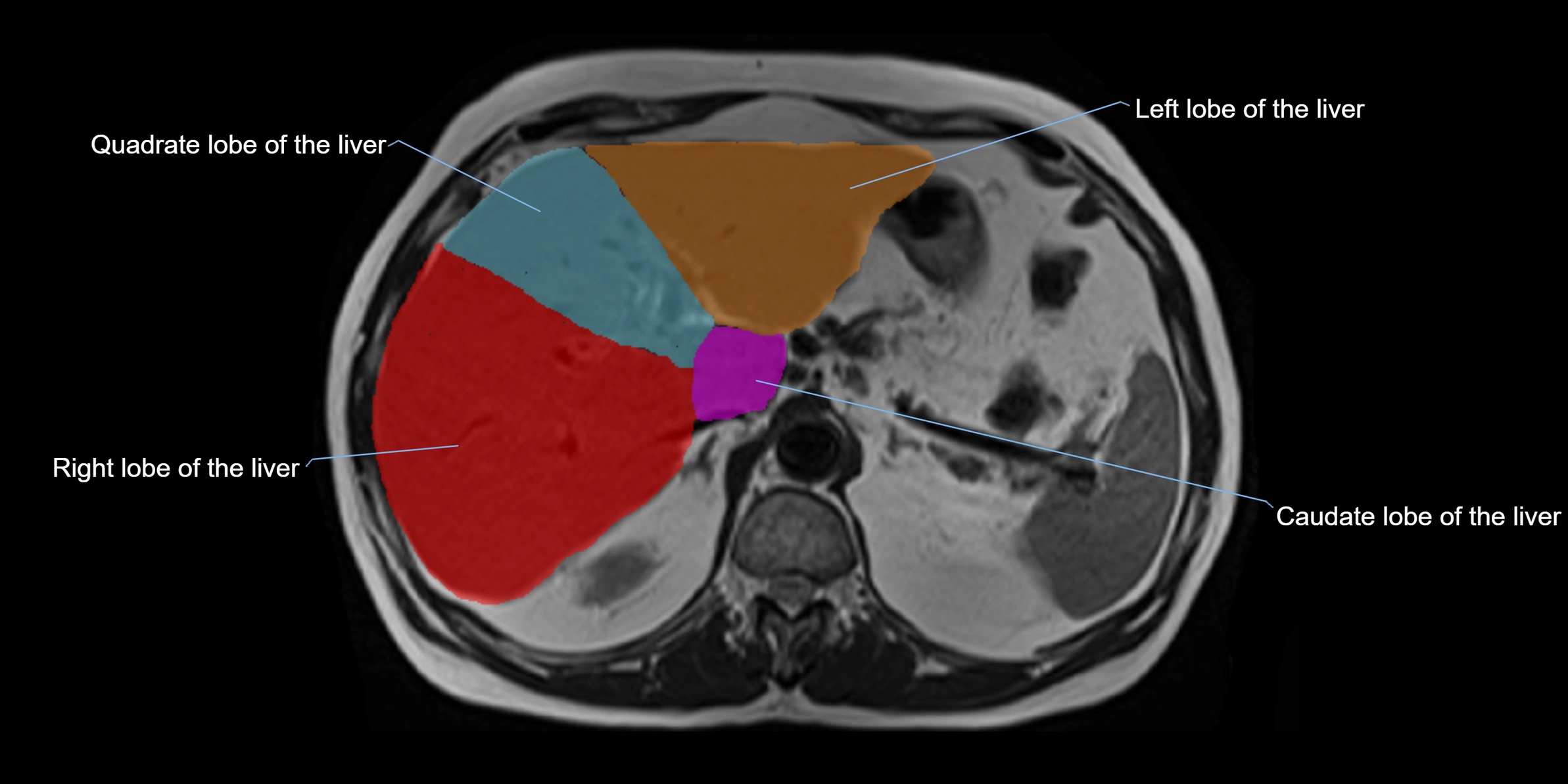
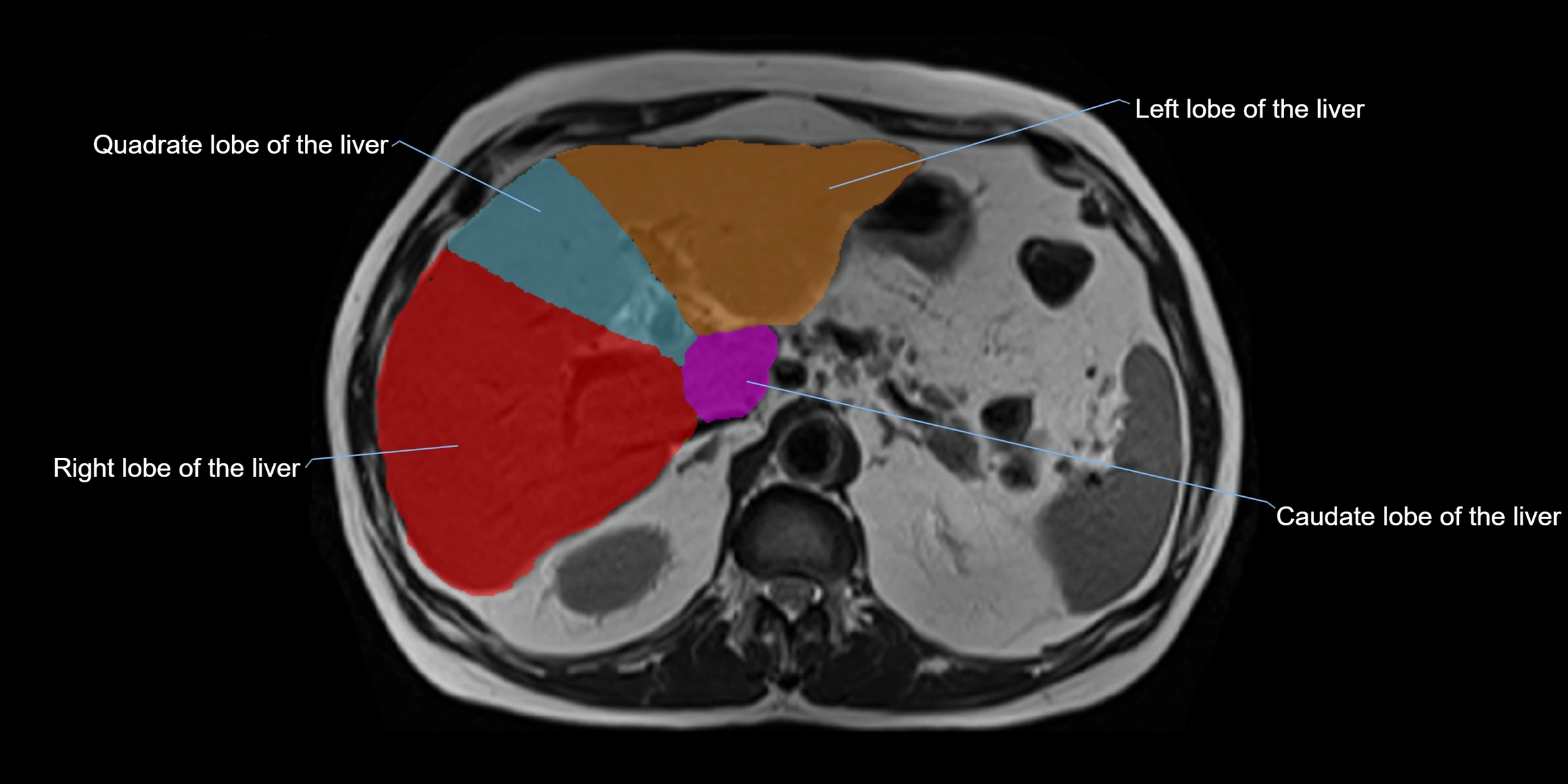
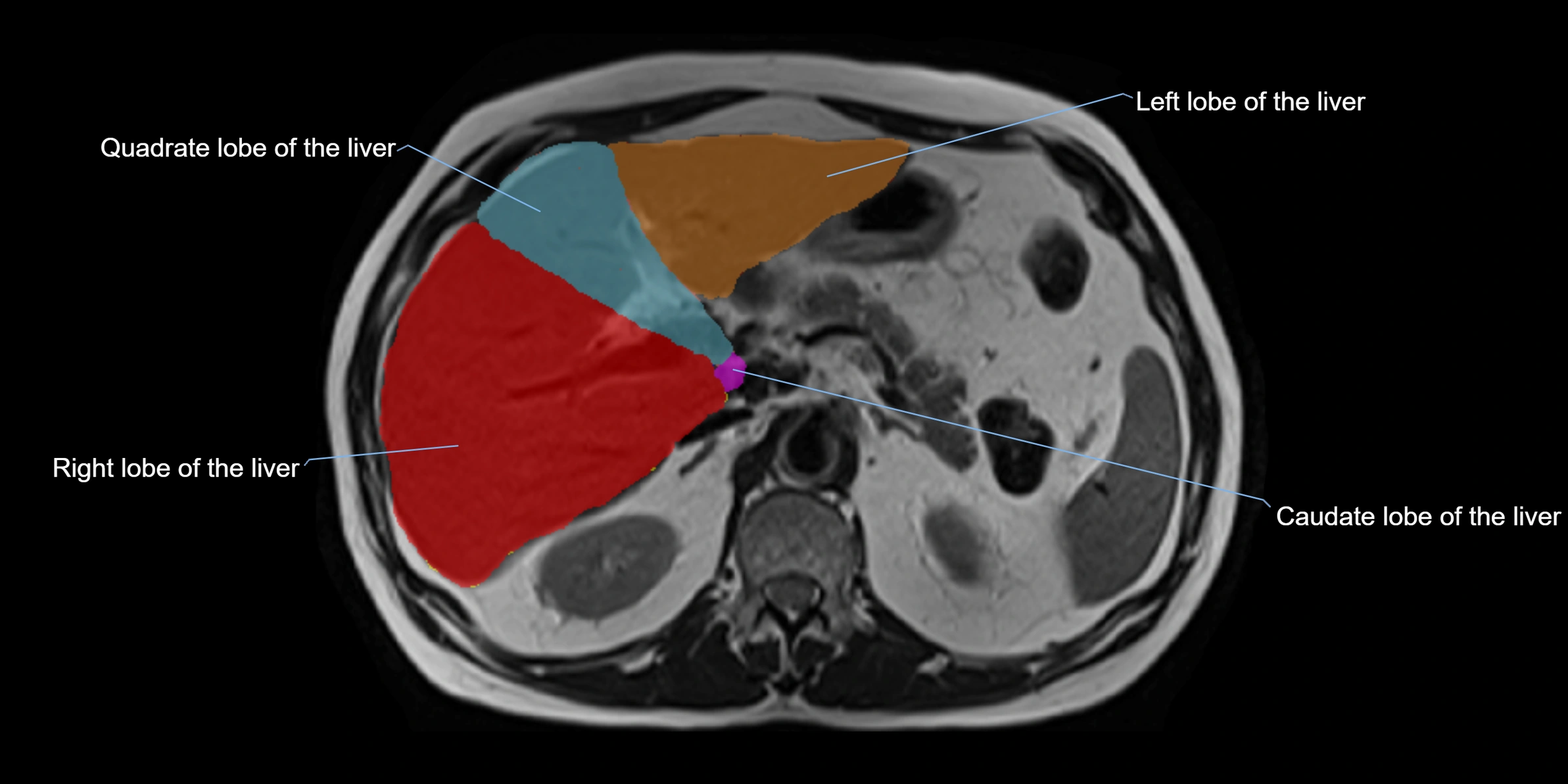
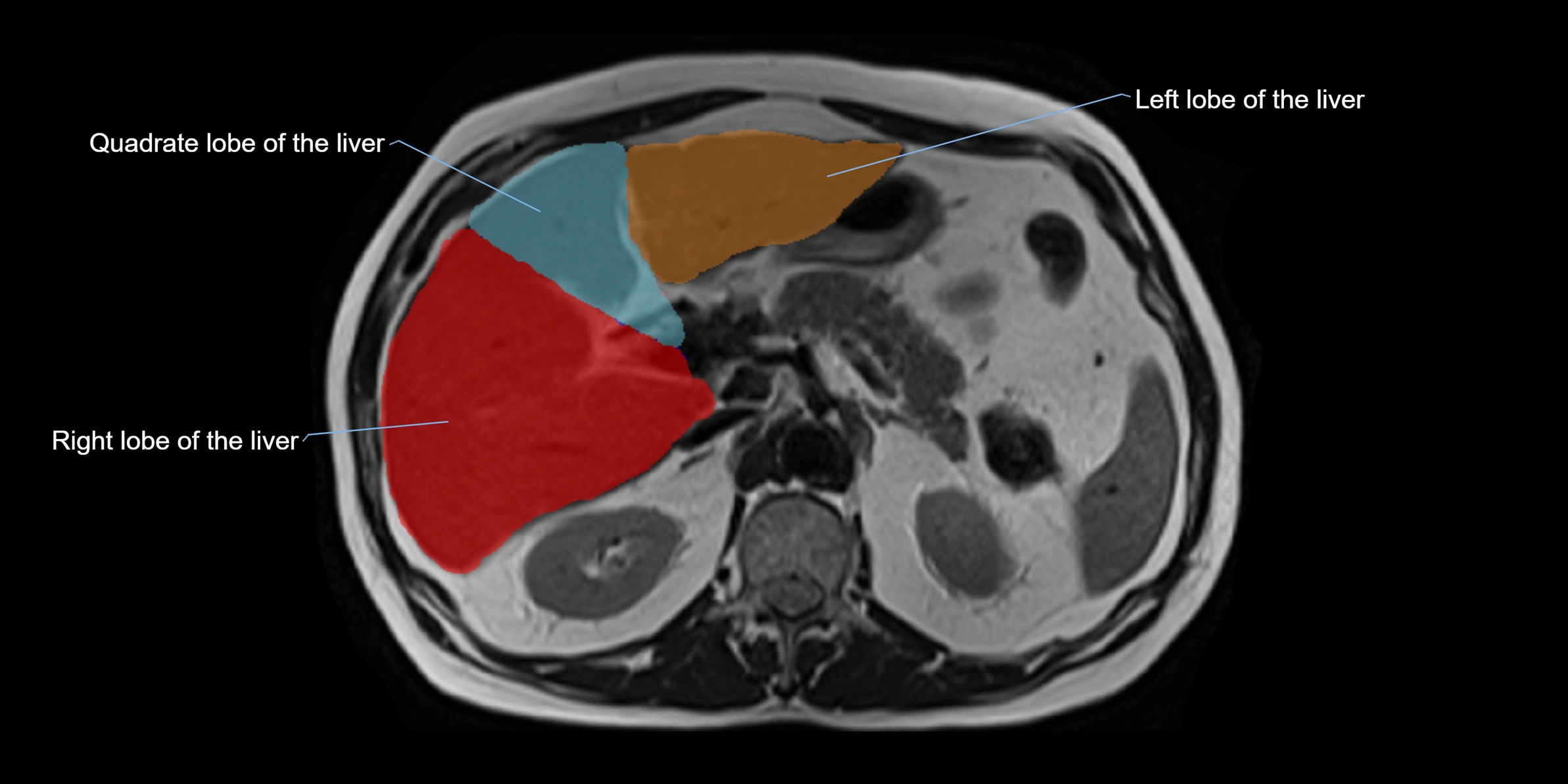
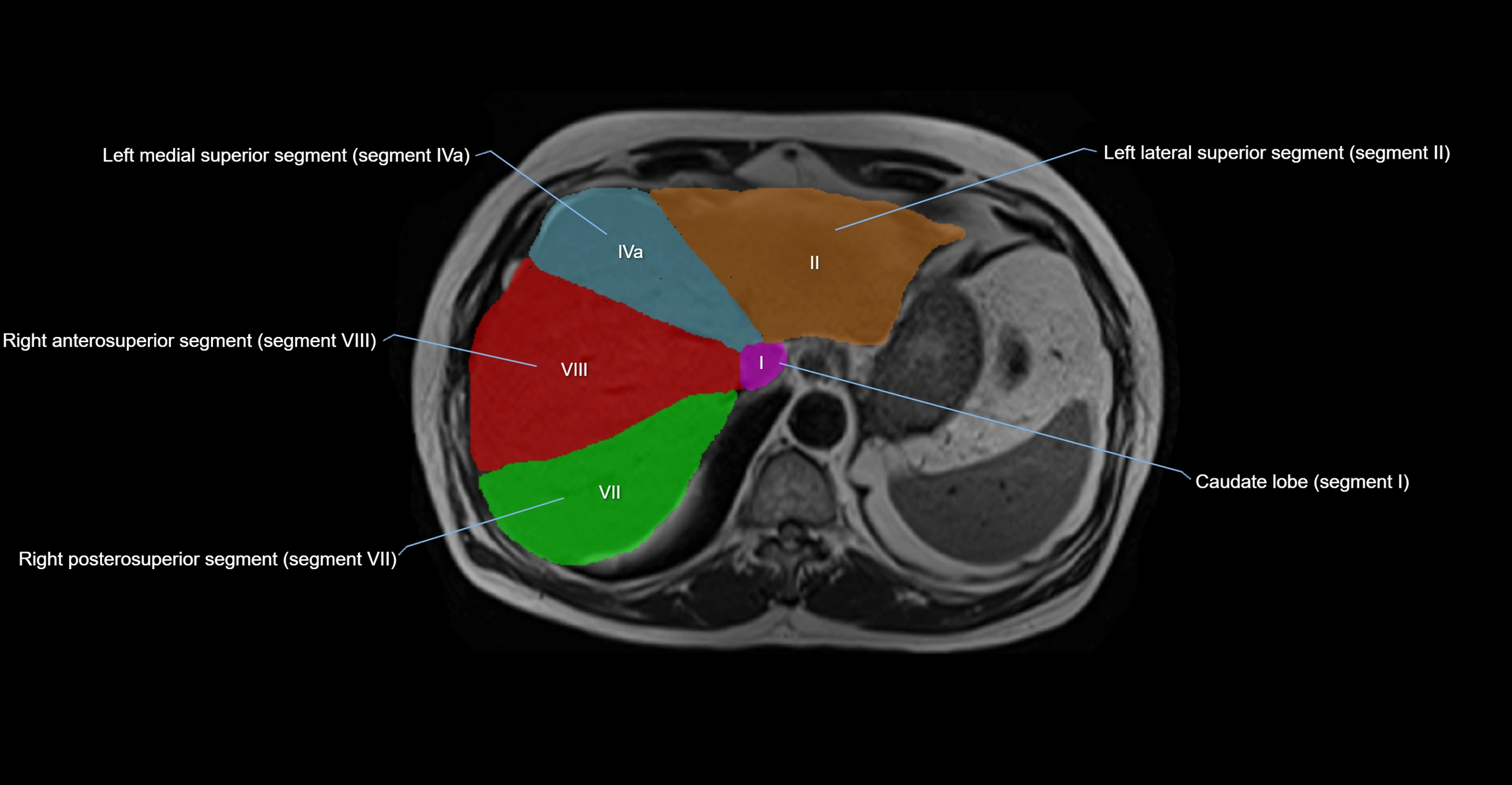
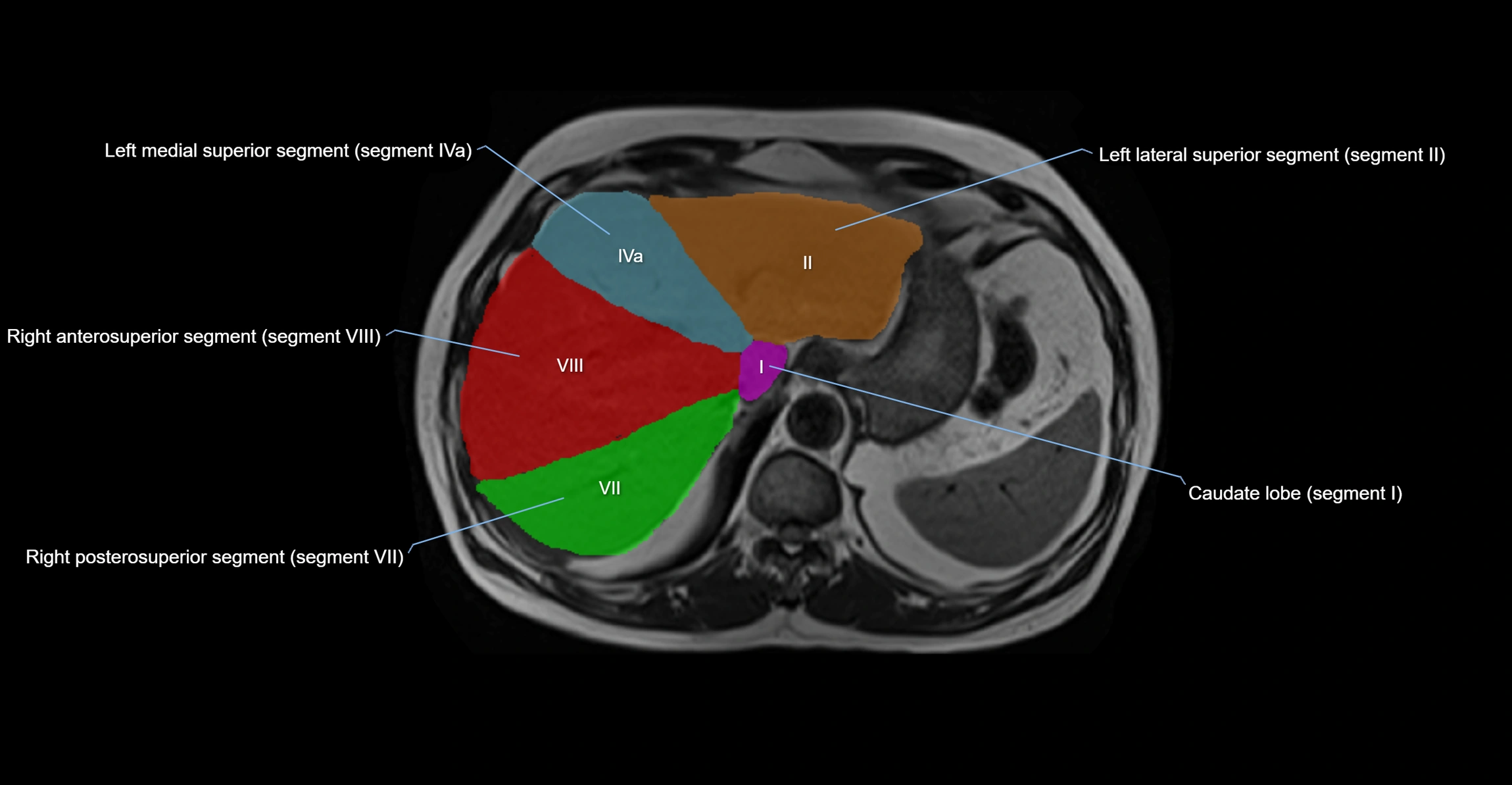
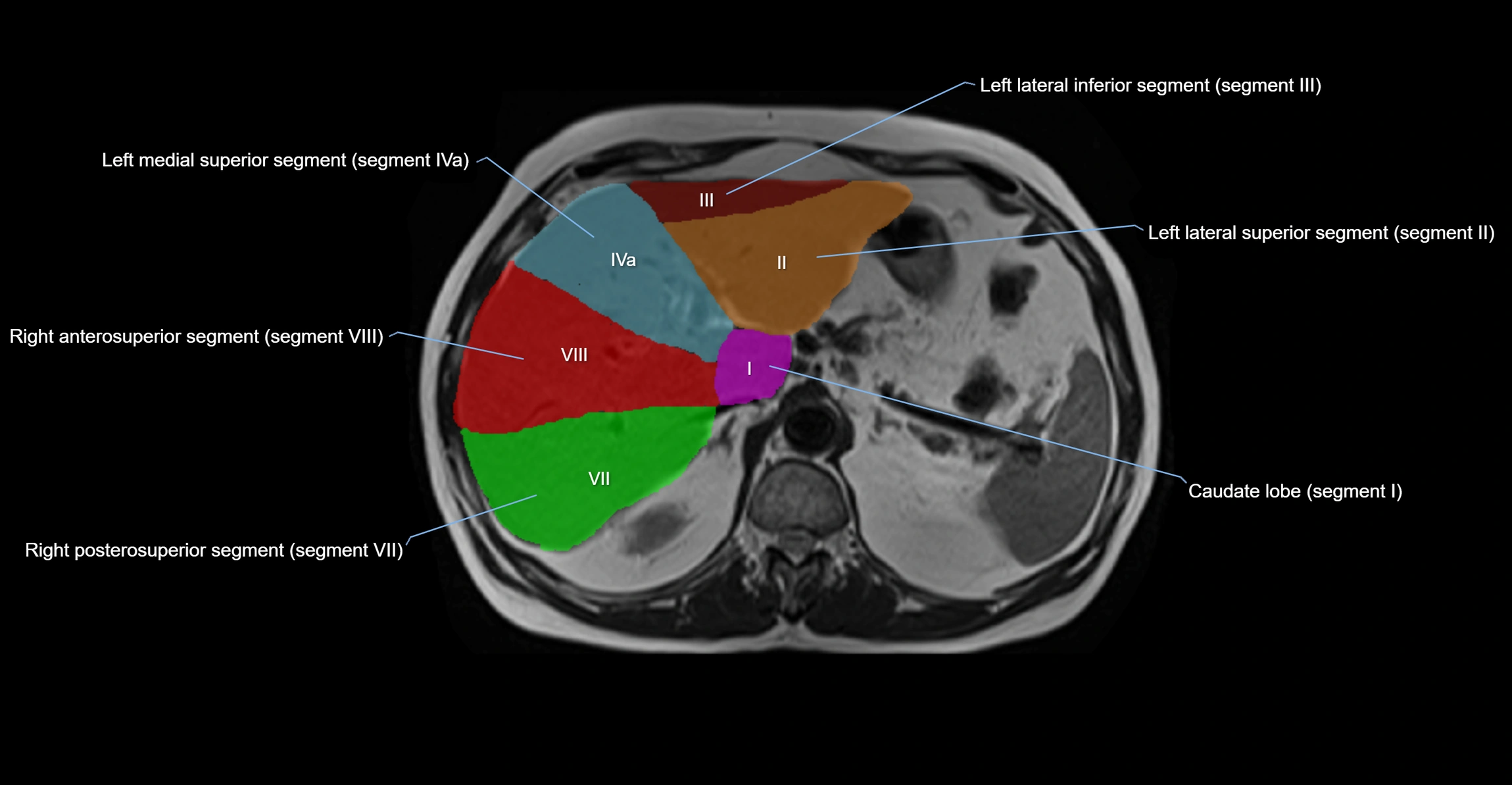
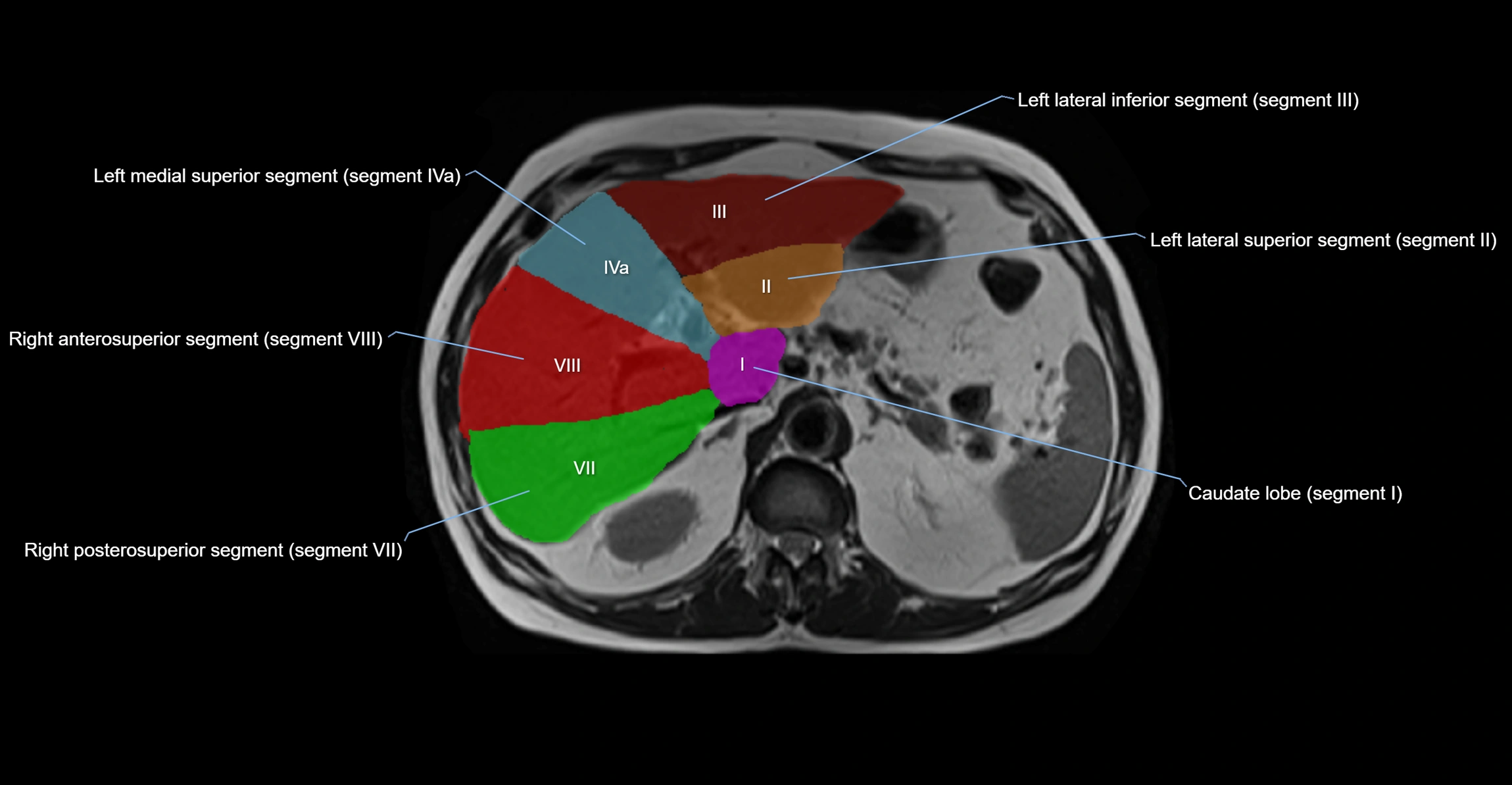
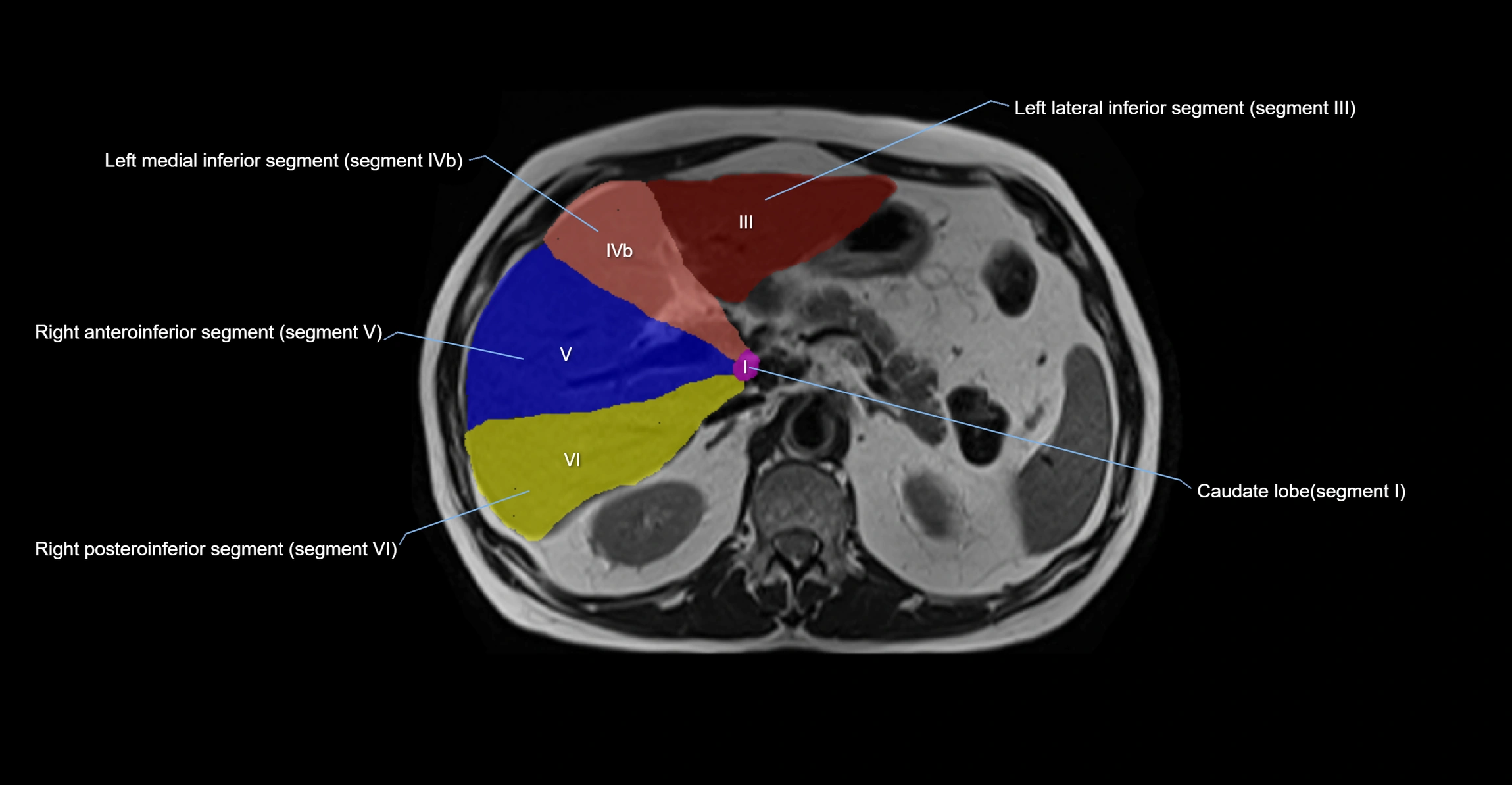
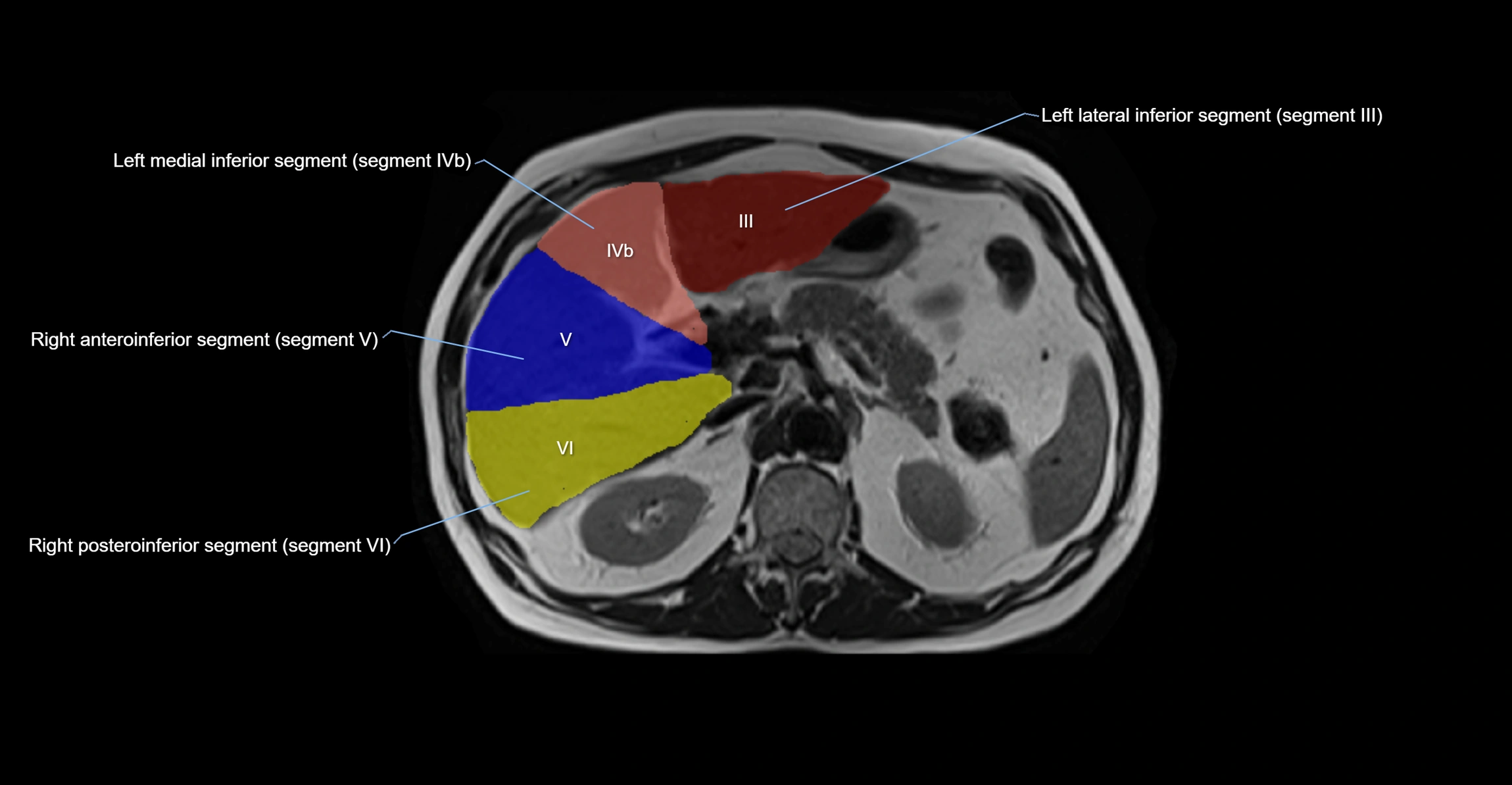
The caudate lobe of the liver is a distinct anatomical subdivision of the liver, designated as segment I in Couinaud’s classification. It lies on the posterior surface of the liver, between the fissure for the ligamentum venosum (left boundary) and the groove for the inferior vena cava (IVC) (right boundary). Superiorly, it is related to the posterior liver surface, and inferiorly it is separated from the left lobe by the porta hepatis.
The caudate lobe is unique because it receives dual portal venous and arterial inflow from both the right and left portal veins and hepatic arteries. It also has independent venous drainage directly into the IVC via multiple small hepatic veins, unlike other lobes that drain through the three main hepatic veins.
This anatomical autonomy makes the caudate lobe especially significant in liver surgery, transplantation, and hepatic venous outflow obstruction syndromes (e.g., Budd–Chiari syndrome). Enlargement of the caudate lobe is a characteristic imaging feature in chronic liver disease and cirrhosis.
Synonyms
-
Segment I (Couinaud classification)
-
Lobus caudatus
-
Spiegel’s lobe (left portion)
Function
-
Contributes to hepatic metabolism, detoxification, and bile production like other lobes
-
Unique dual vascular supply and direct IVC drainage allow it to maintain function even in hepatic venous obstruction
-
Plays a protective role in maintaining liver function during cirrhosis or portal hypertension
Nerve Supply
-
Hepatic plexus (sympathetic fibers from celiac plexus and parasympathetic fibers from vagus nerve)
Arterial Supply
-
Branches from both right and left hepatic arteries (dual supply)
Venous Drainage
-
Portal inflow from both right and left portal veins
-
Venous outflow directly into the IVC via multiple short hepatic veins, independent of the main hepatic veins
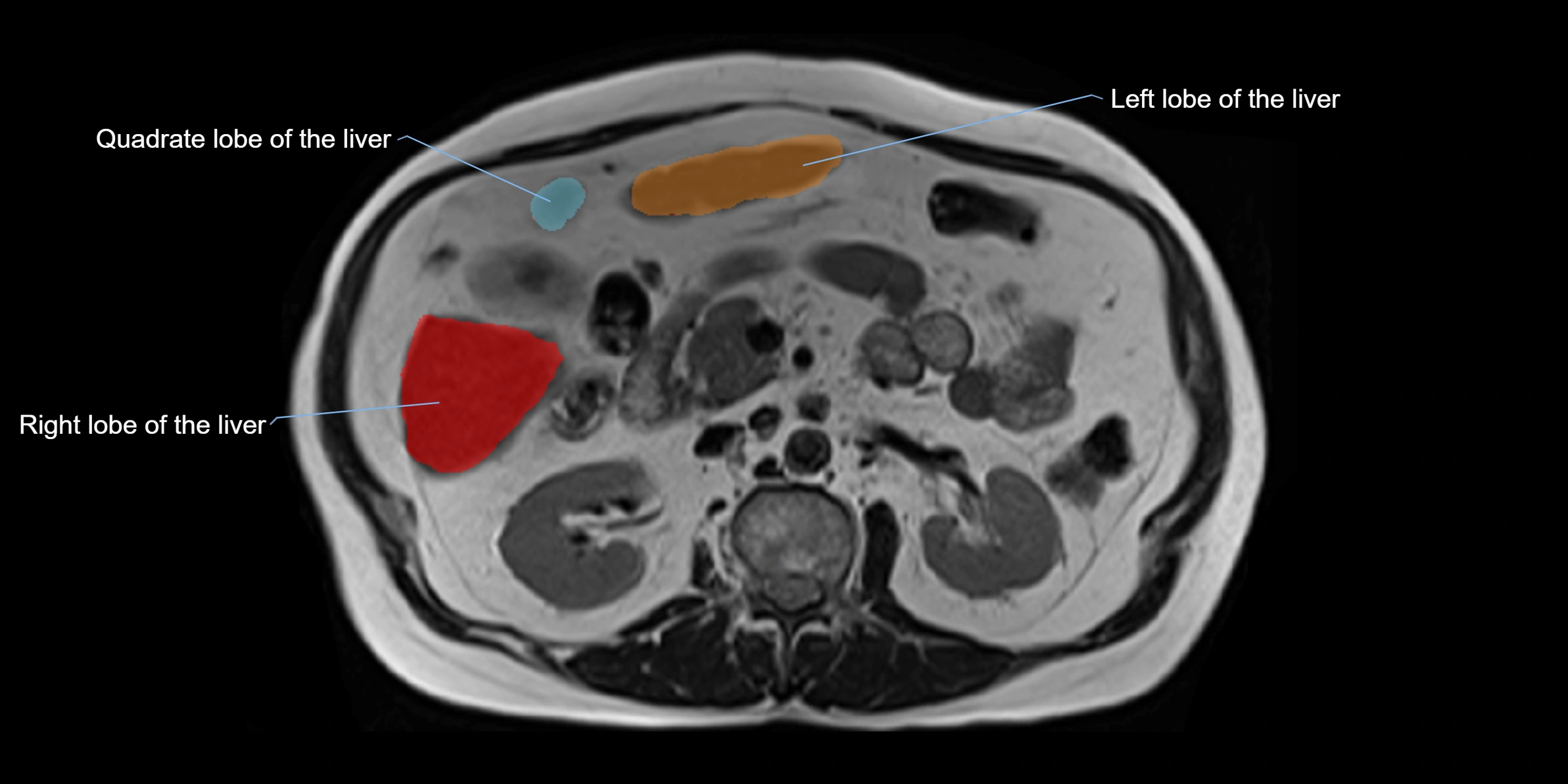
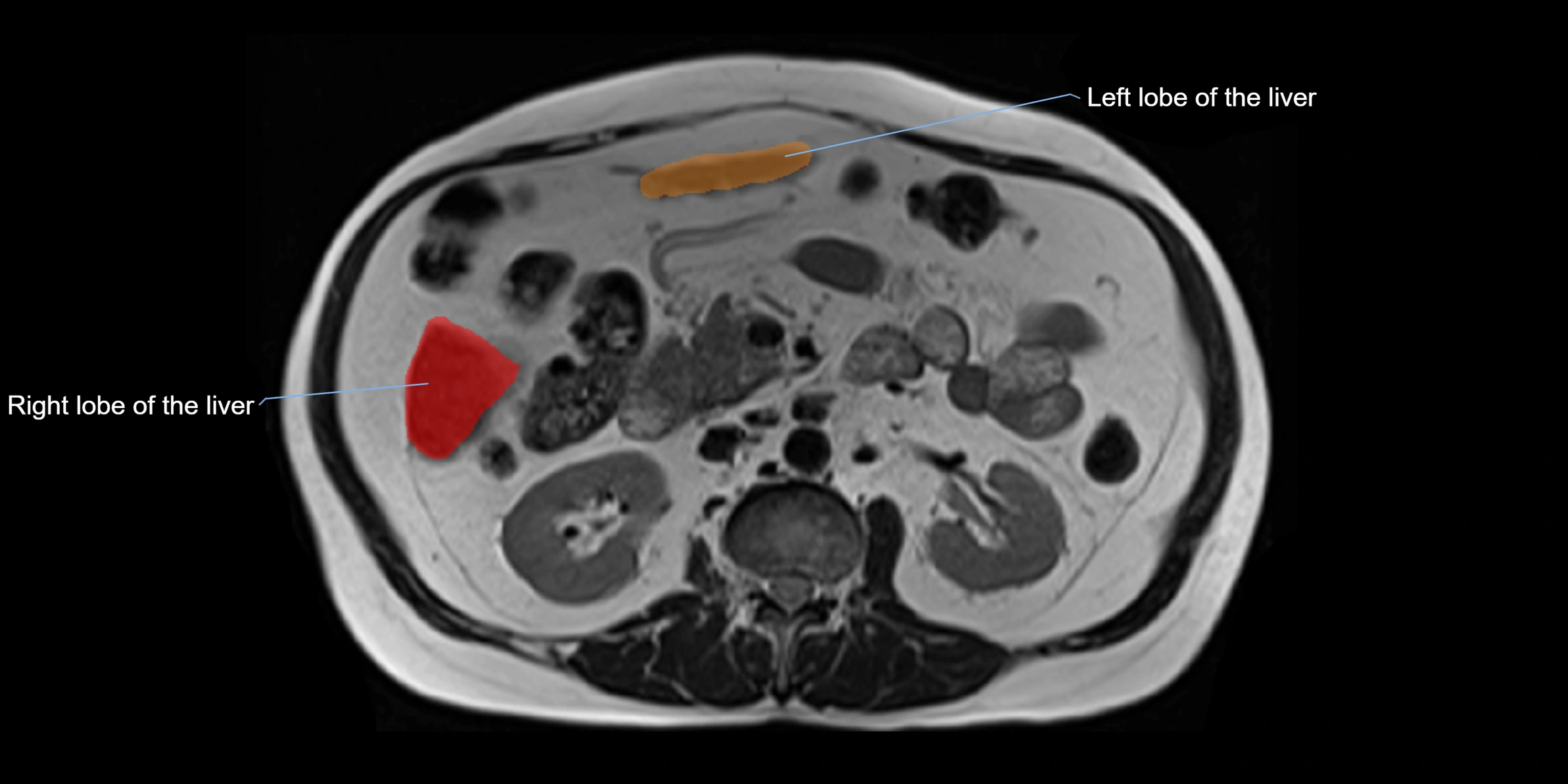
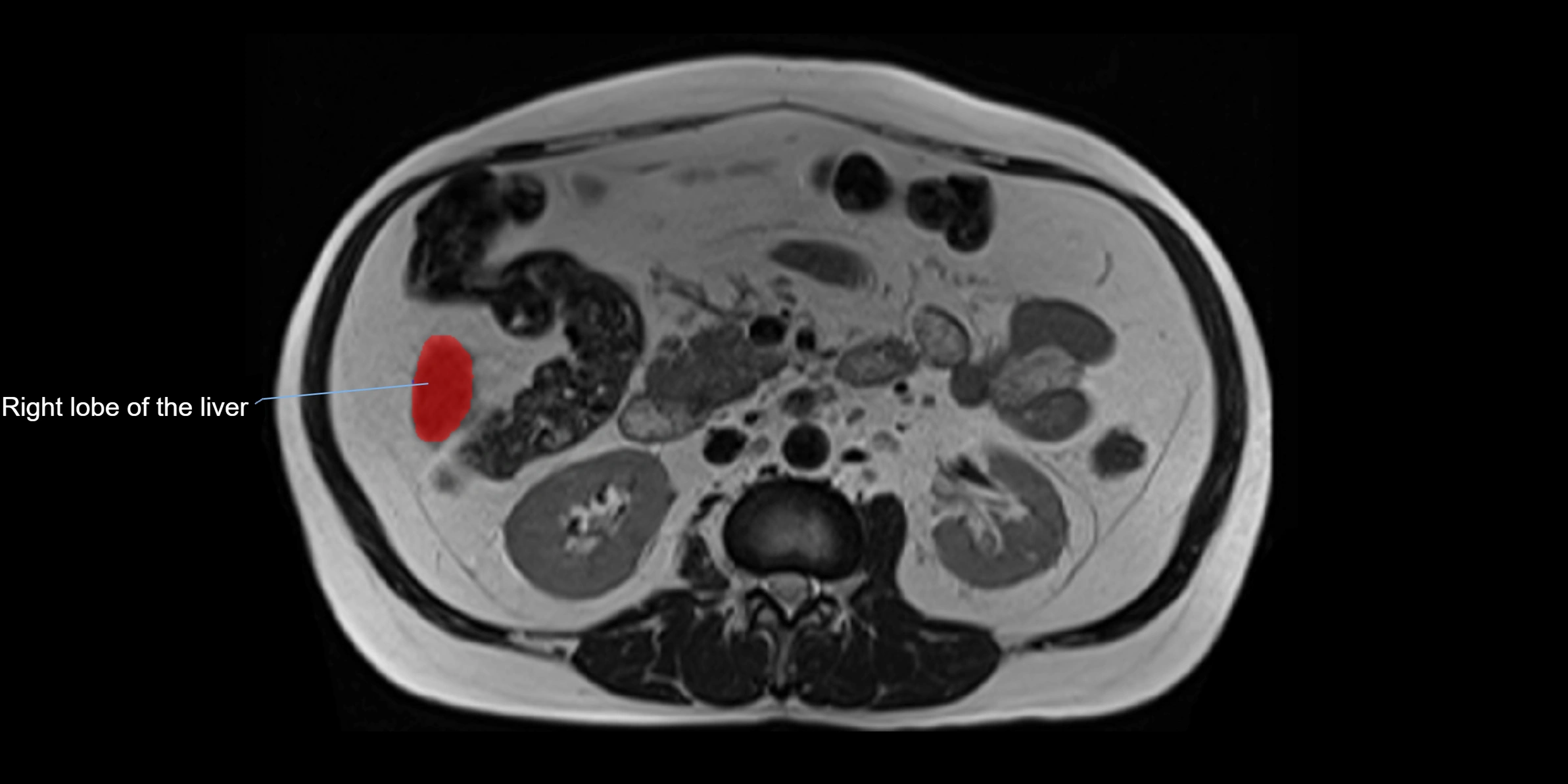
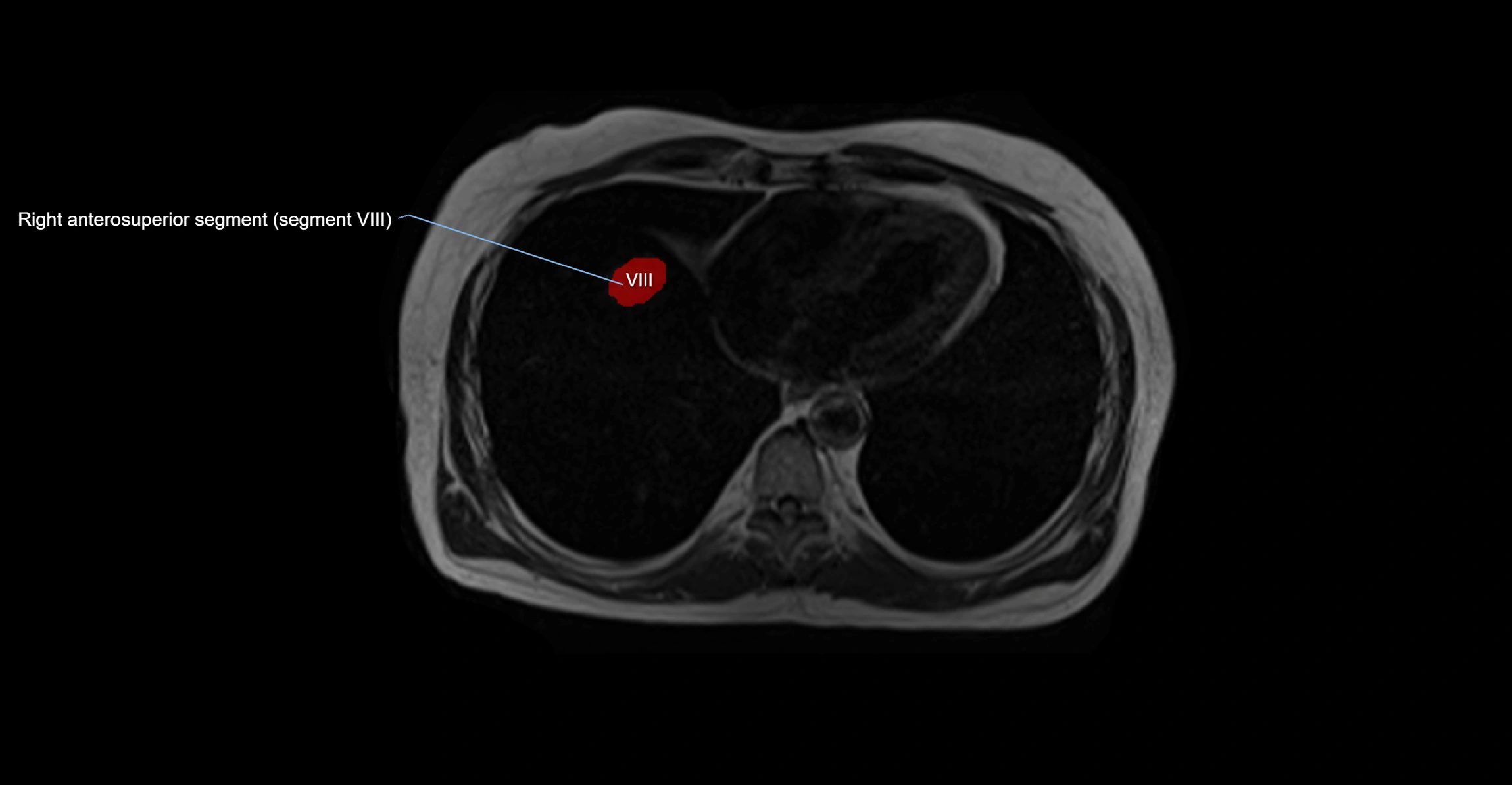
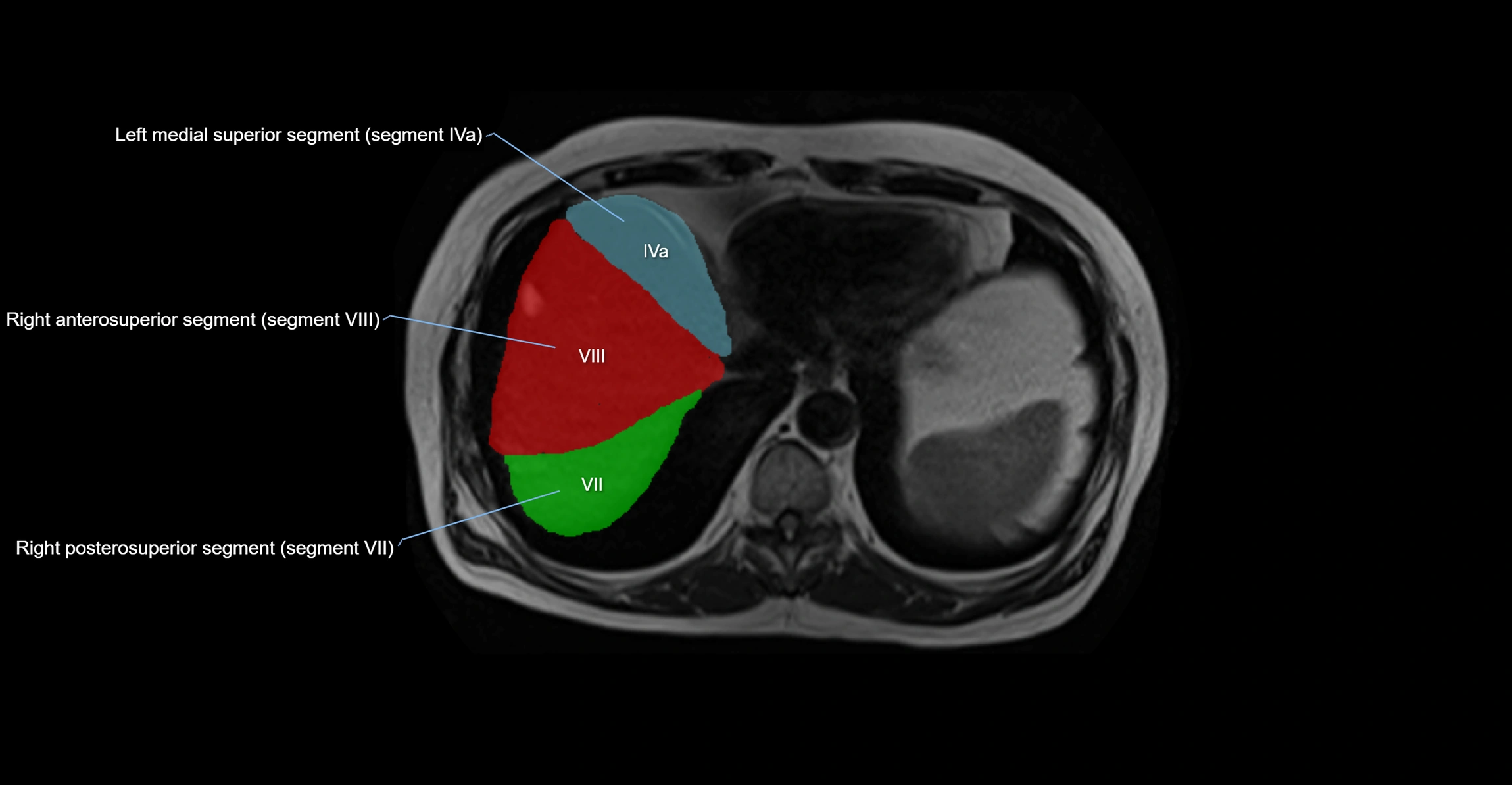
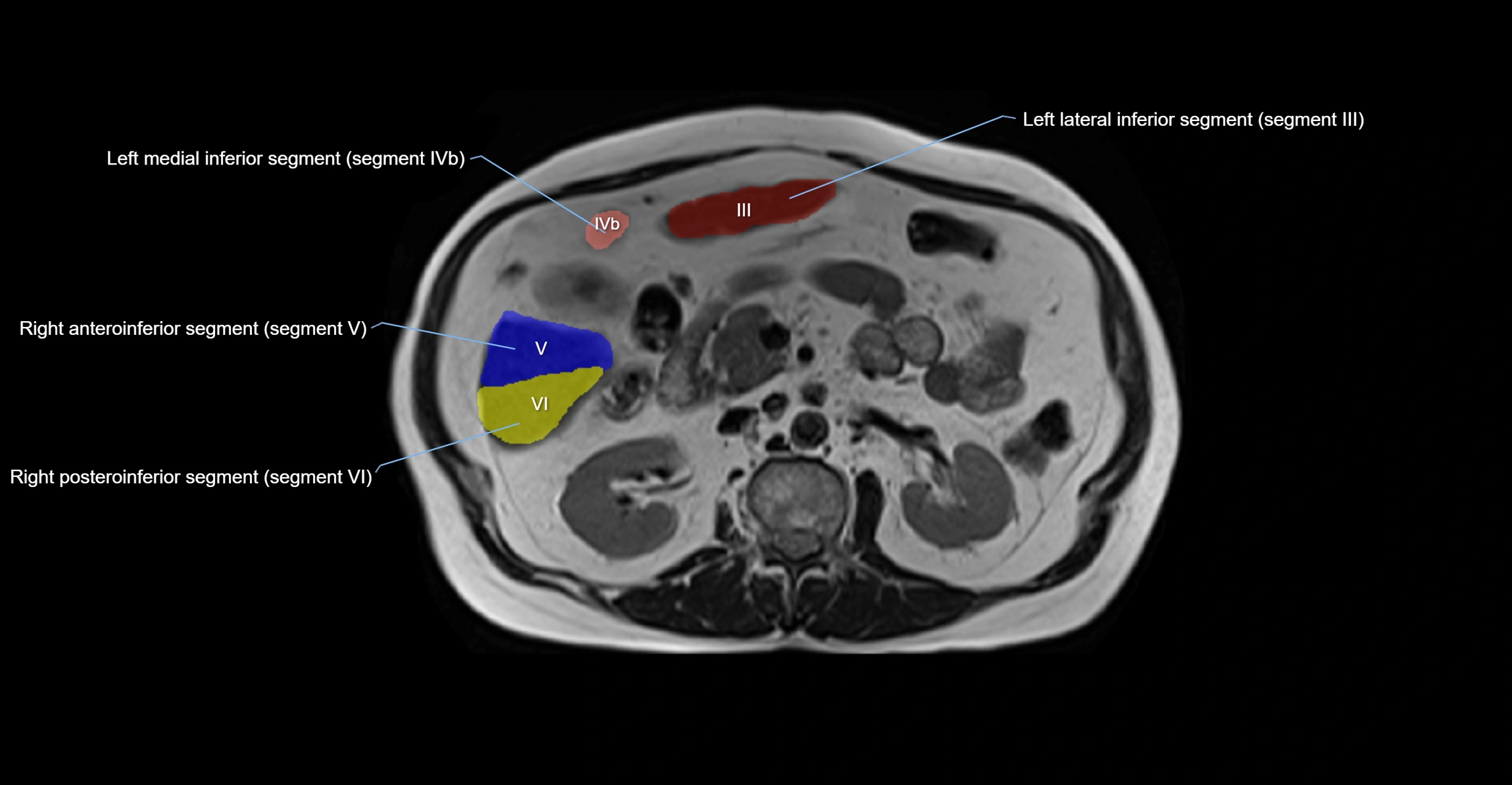
MRI Appearance
T1-weighted images:
-
Parenchyma shows intermediate signal intensity, similar to rest of liver
-
Lesions (tumors, fat, fibrosis) show altered signal compared to background liver
T2-weighted images:
-
Normal parenchyma shows intermediate to slightly hyperintense signal
-
Pathologies (cysts, hemangiomas, tumors) demonstrate variable high signal
STIR:
-
Suppresses fat, highlighting edema, inflammation, or lesion signal
-
Useful in detecting caudate lobe hypertrophy in cirrhosis
T1 Fat-Saturated (Pre-contrast):
-
Caudate lobe appears as intermediate signal parenchyma against suppressed fat
T1 Fat-Saturated Post-Contrast (Gadolinium):
-
Homogeneous enhancement in normal parenchyma during portal venous phase
-
Lesions (HCC, metastasis, hemangiomas) enhance with characteristic dynamic patterns
-
Important in detecting vascular invasion and caudate hypertrophy
CT Appearance
CT Pre-Contrast:
-
Caudate lobe appears as a soft-tissue density, isodense to the rest of the liver
-
Enlargement may be appreciated in cirrhosis or Budd–Chiari syndrome
CT Post-Contrast:
-
Homogeneous enhancement in the portal venous phase, similar to rest of liver
-
Independent venous drainage into the IVC may be visualized
-
Lesions follow characteristic CT enhancement patterns (HCC: arterial hyperenhancement with washout; hemangiomas: peripheral nodular enhancement with centripetal fill-in)
CT Venous Phase (functional significance):
-
Caudate lobe often enhances relatively more than other lobes in Budd–Chiari syndrome, due to preserved venous outflow
CT Image

CT Image
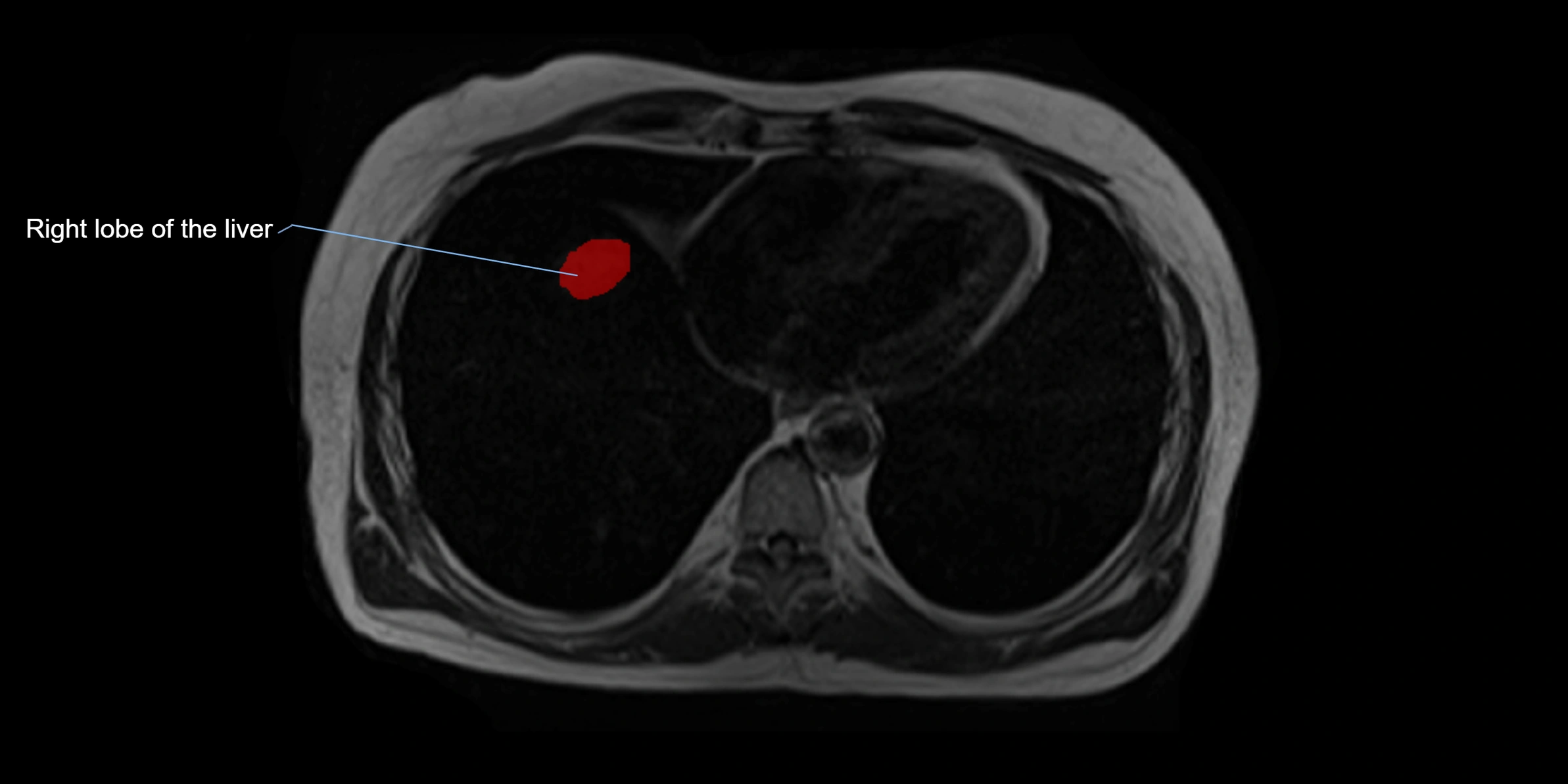
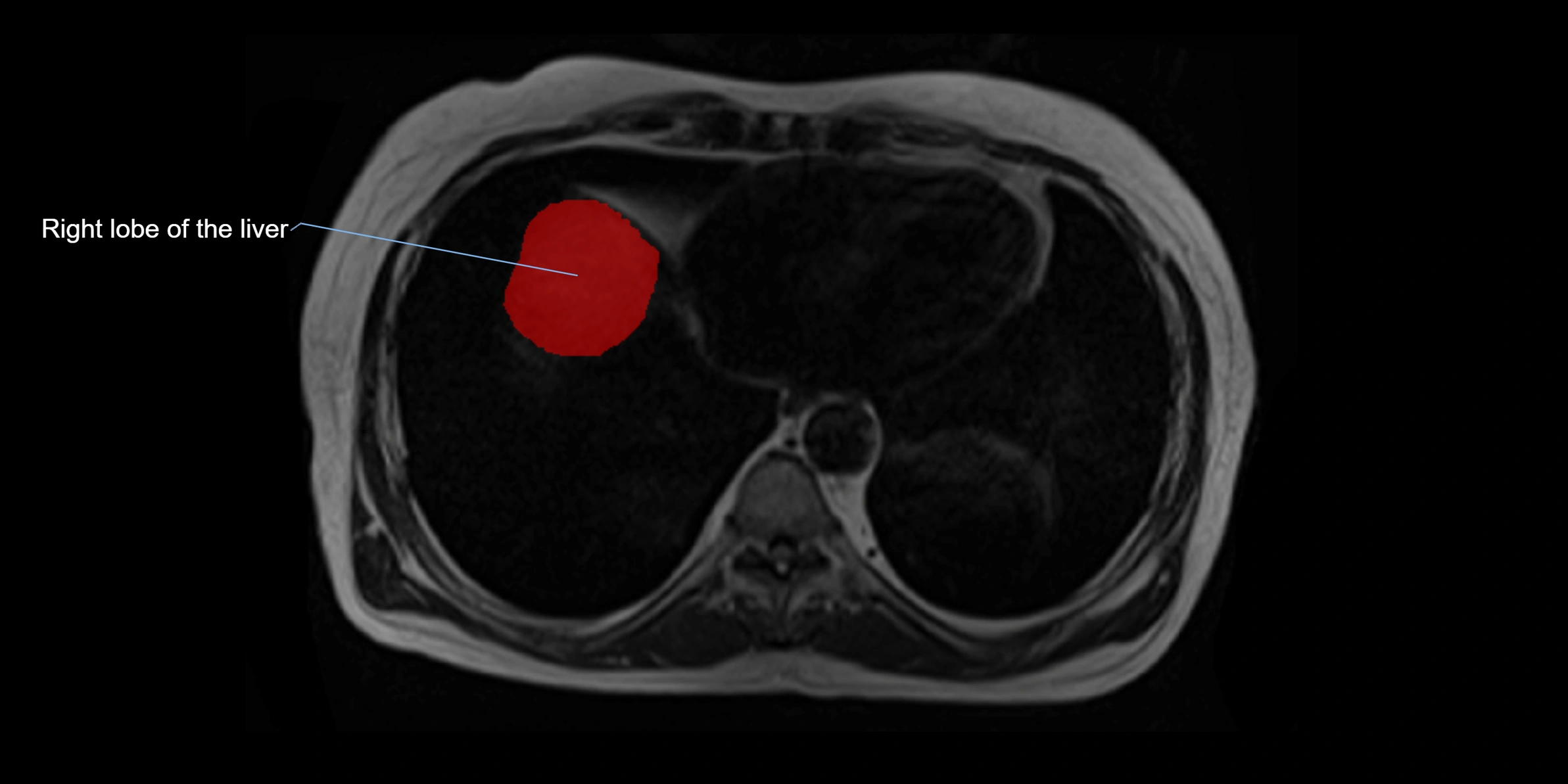
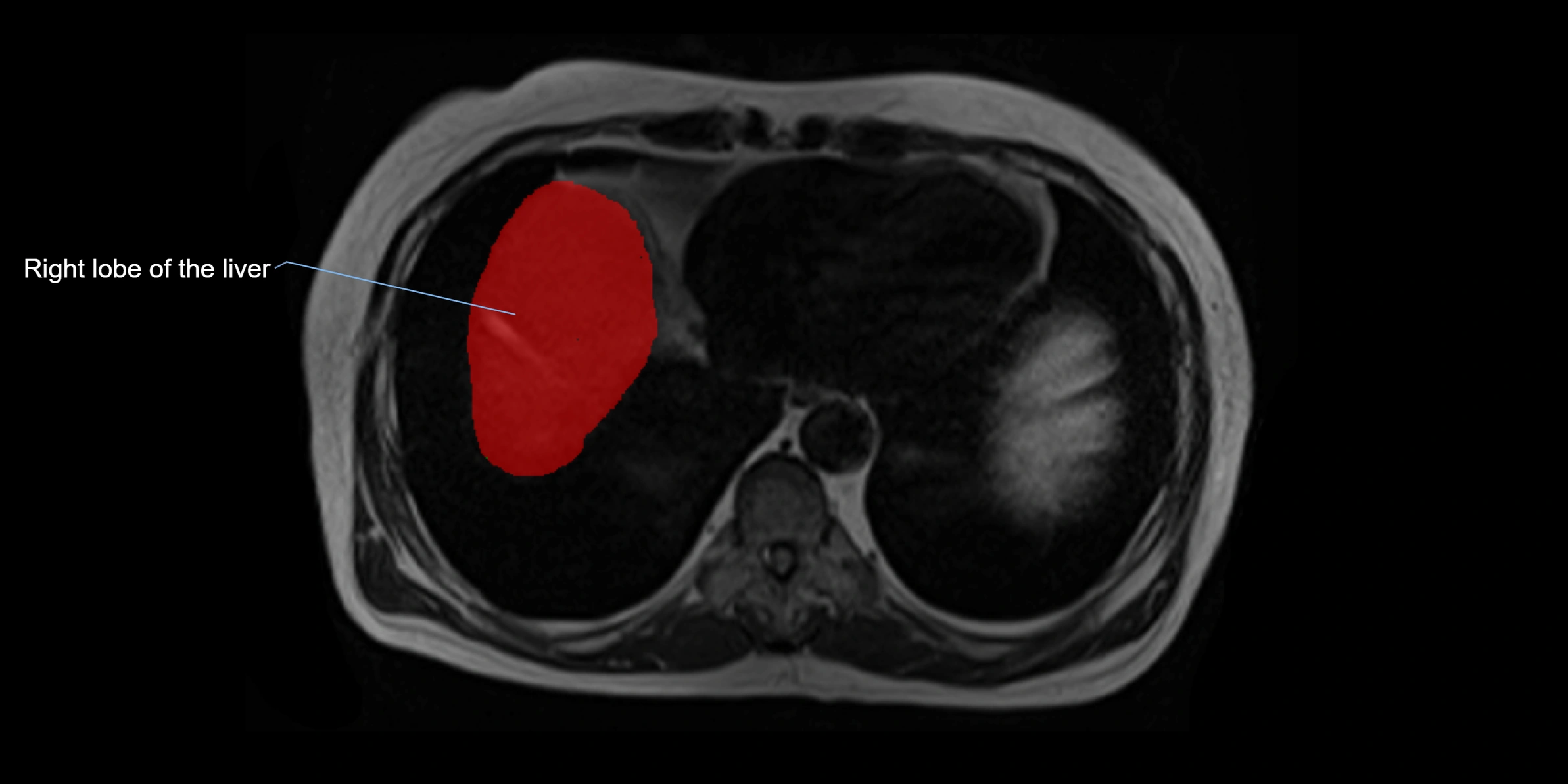
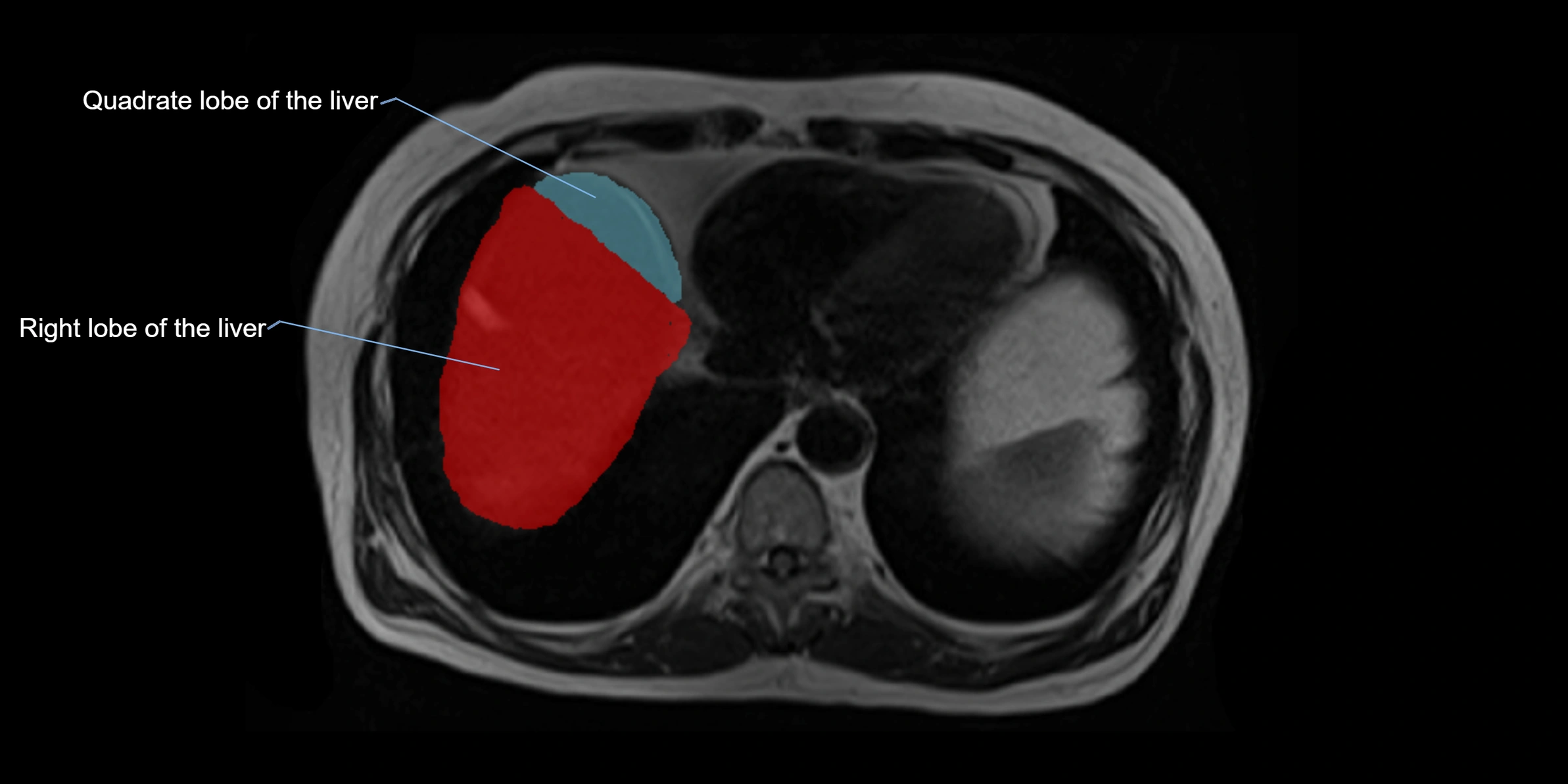
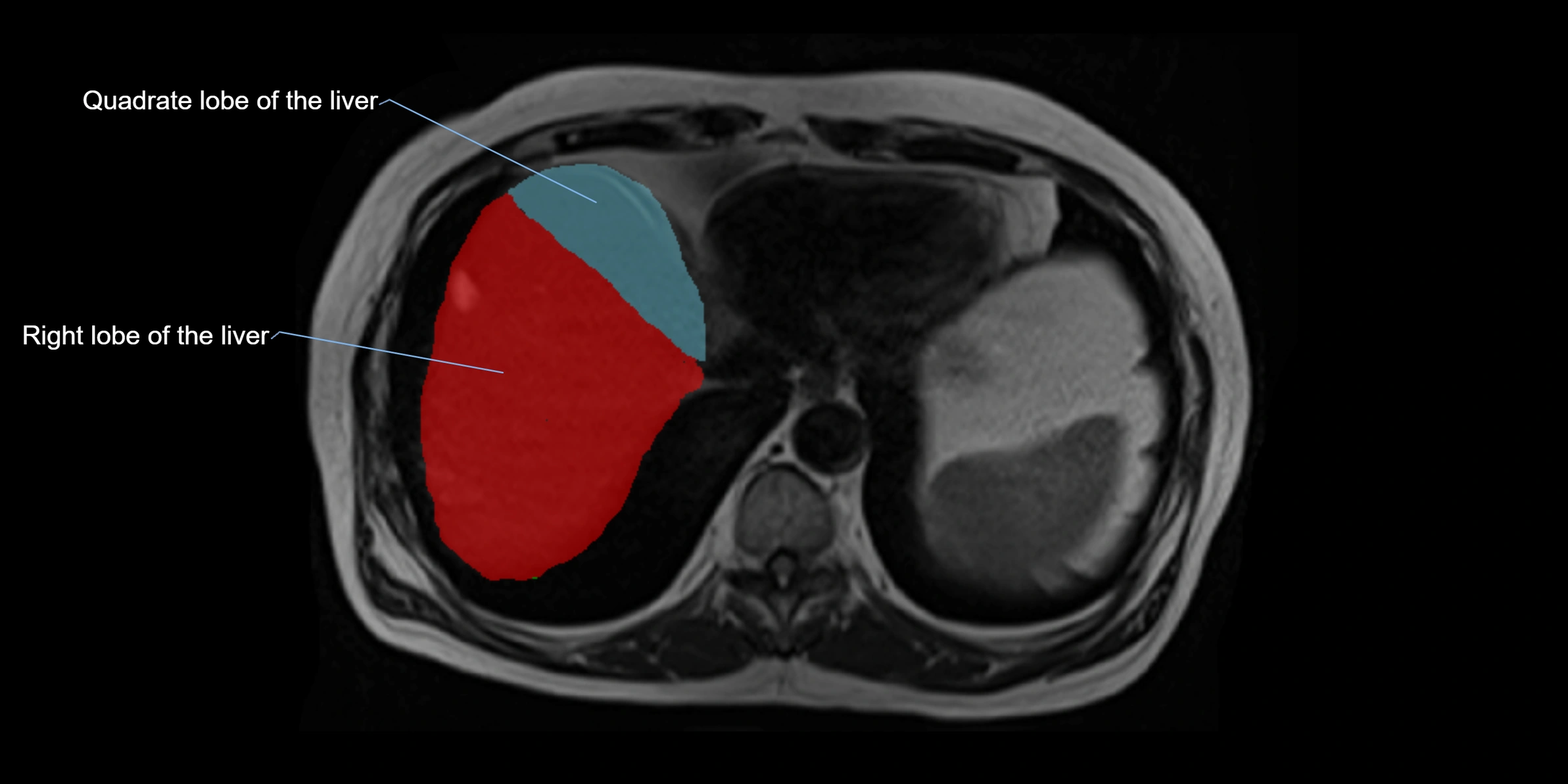
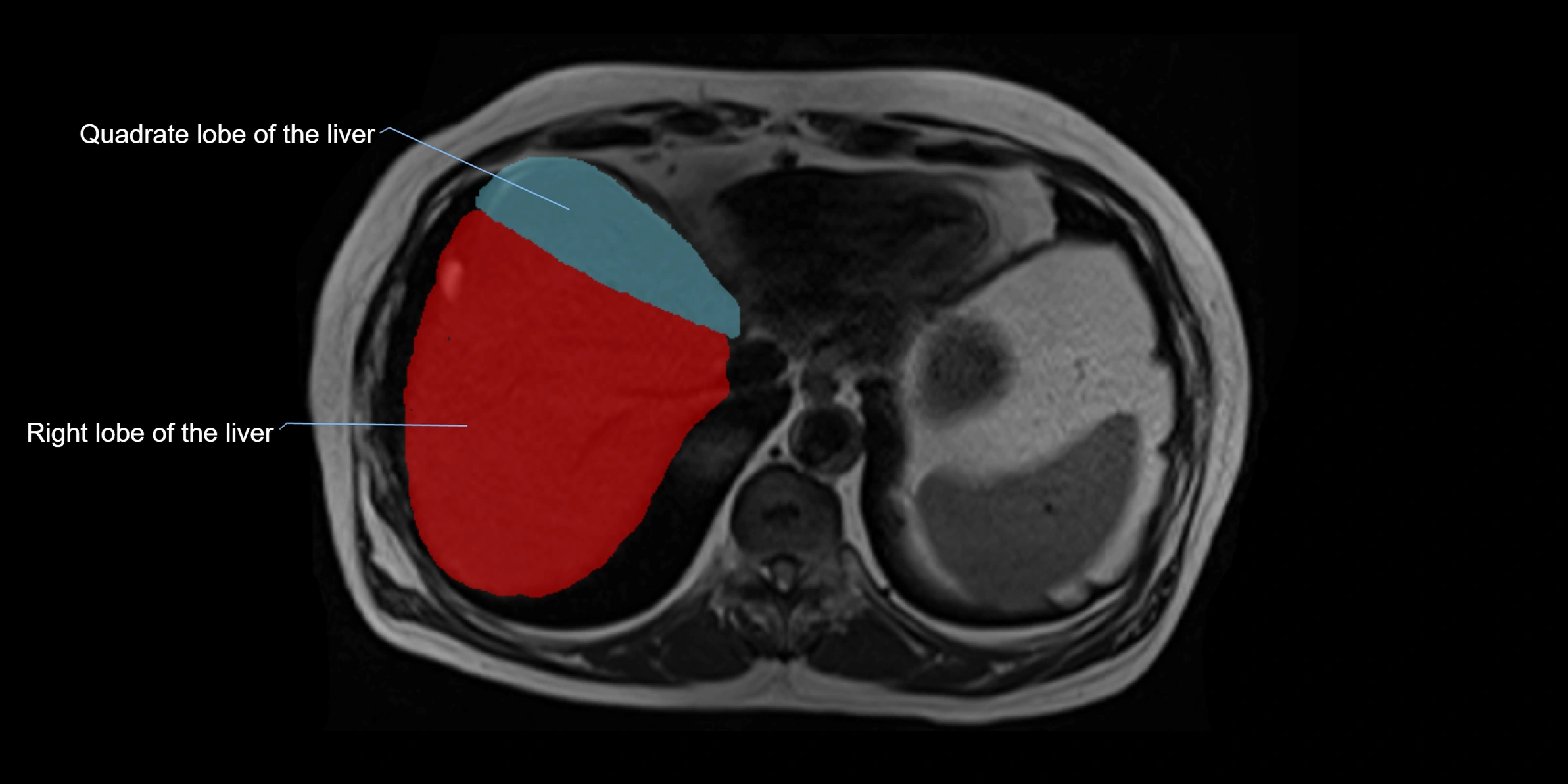
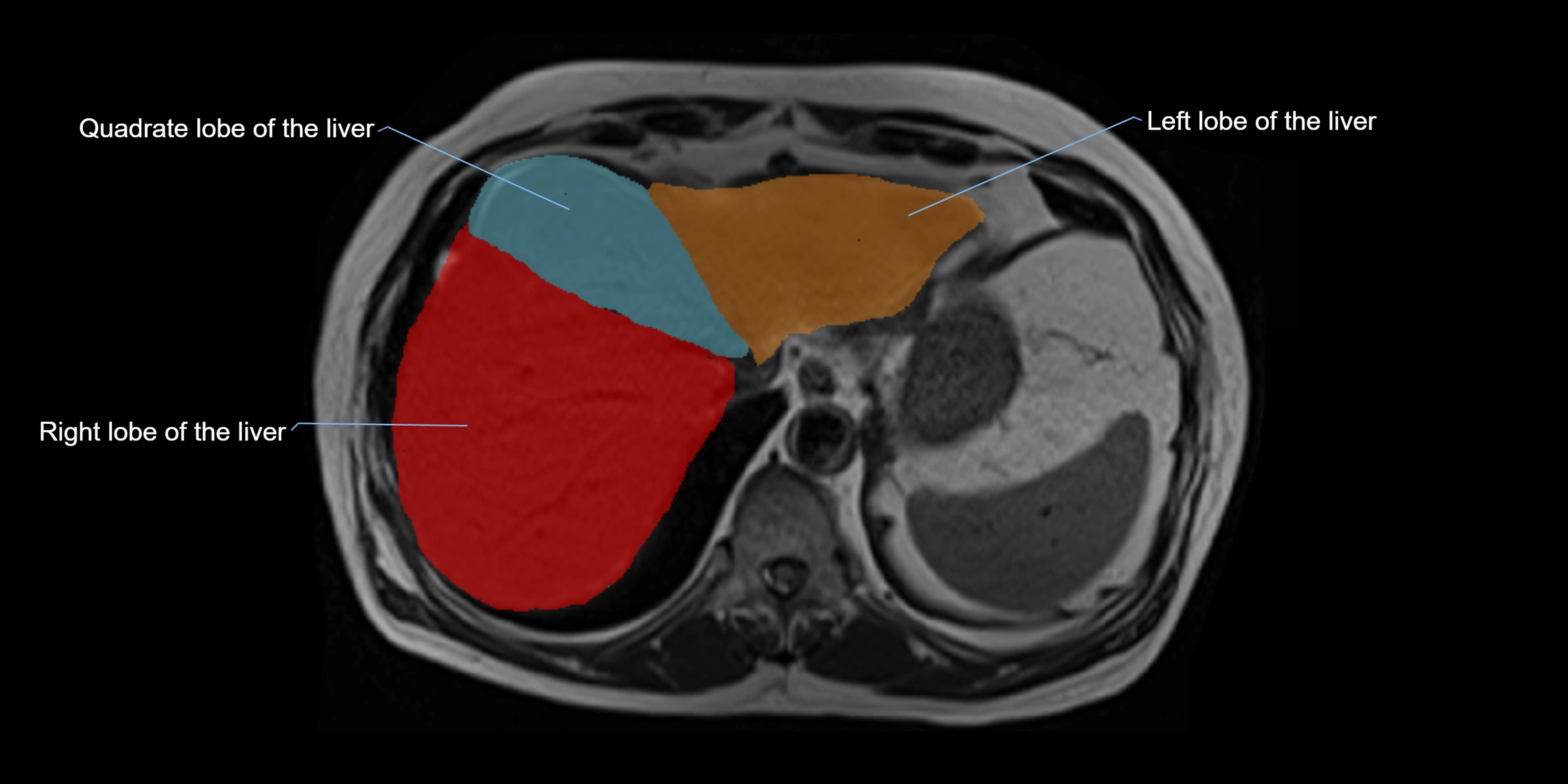
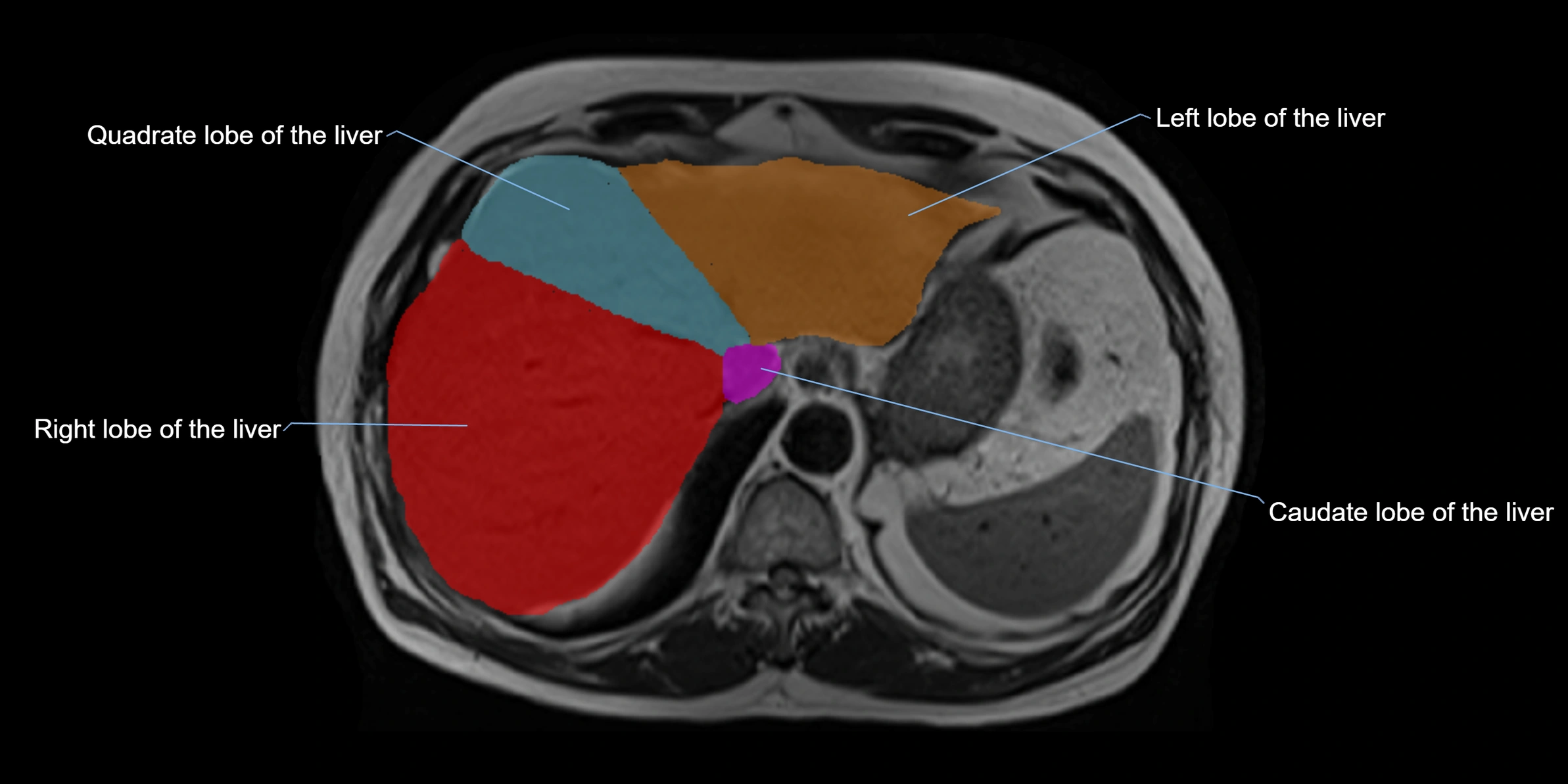
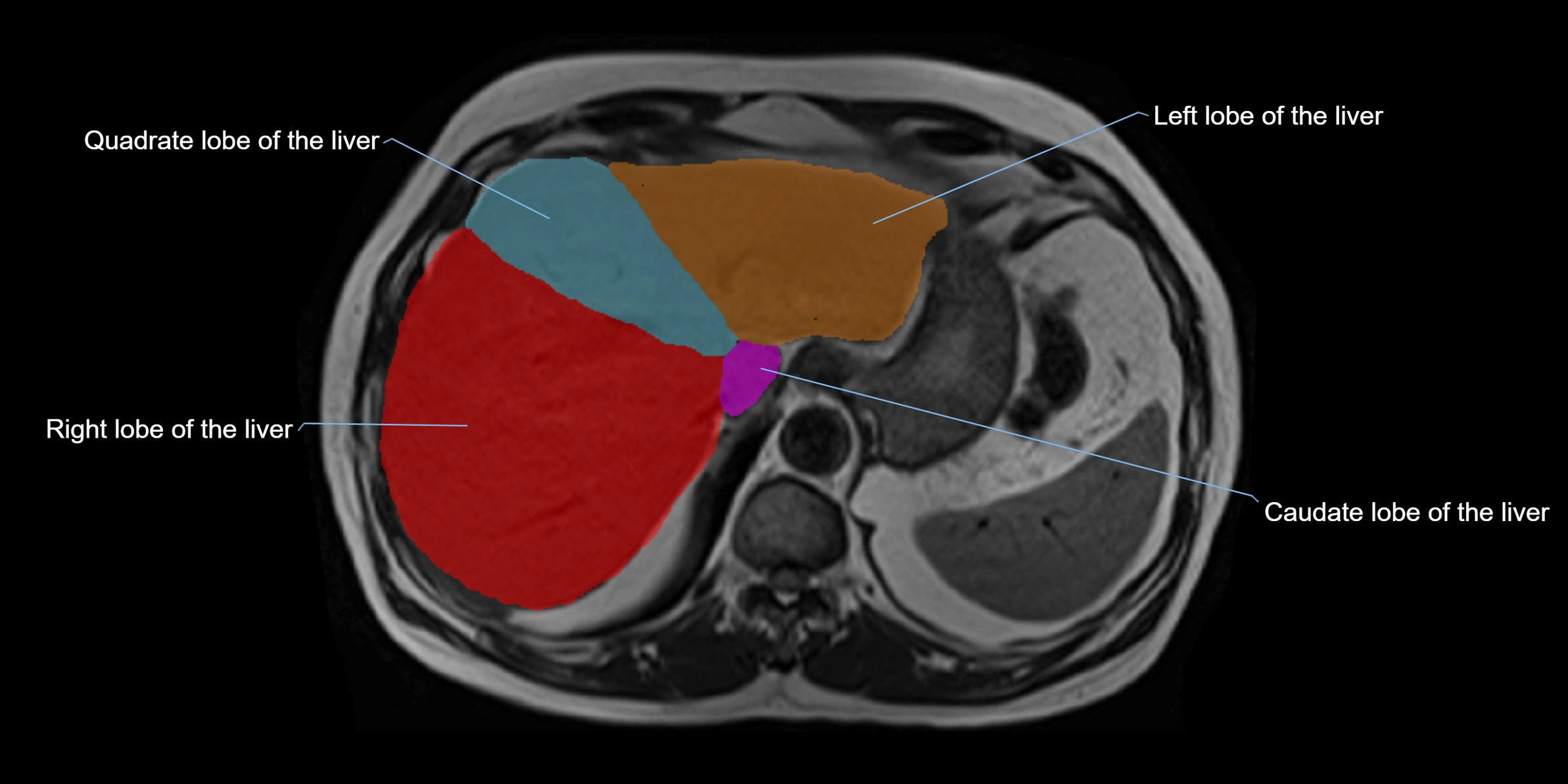
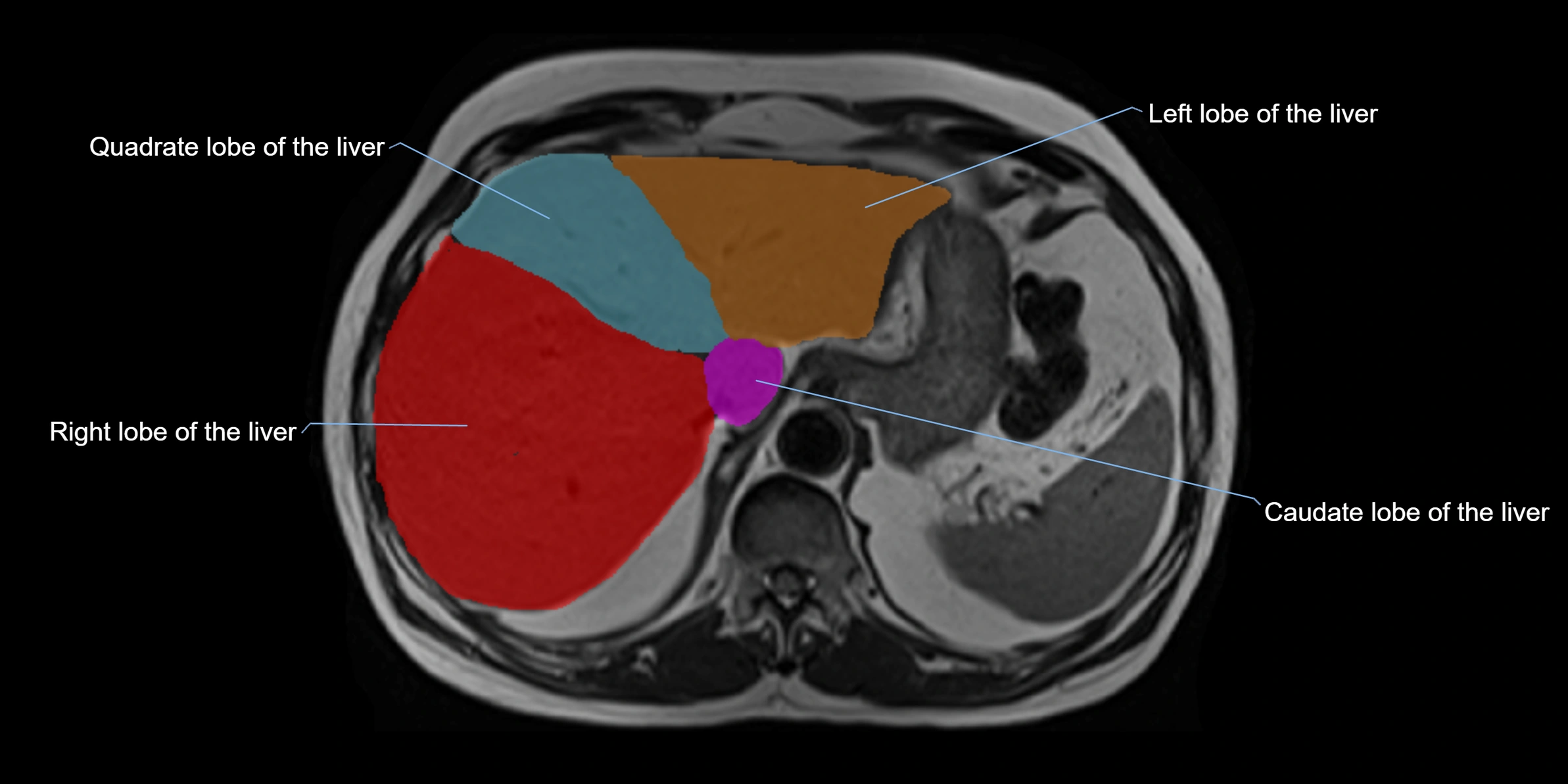
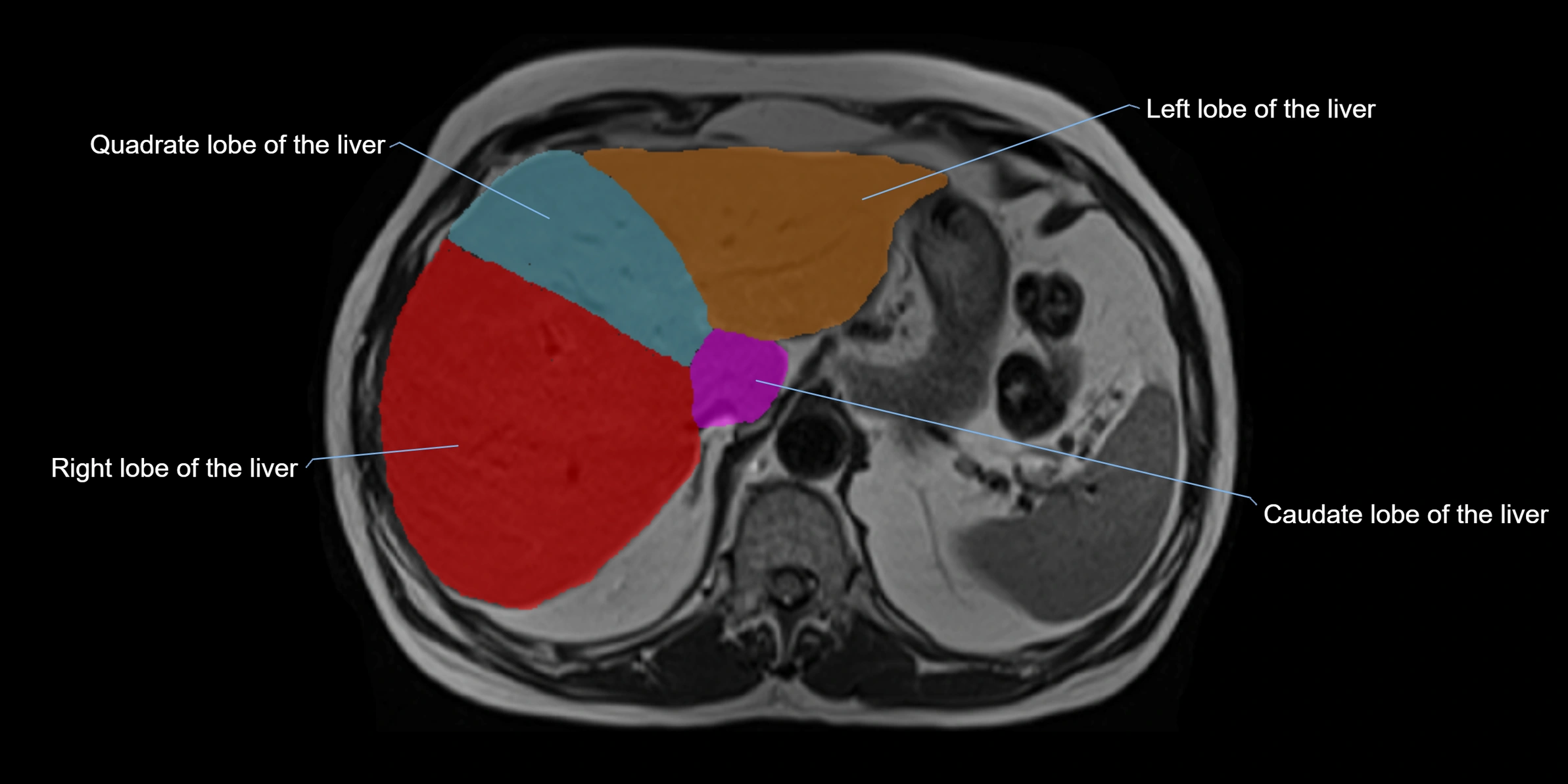
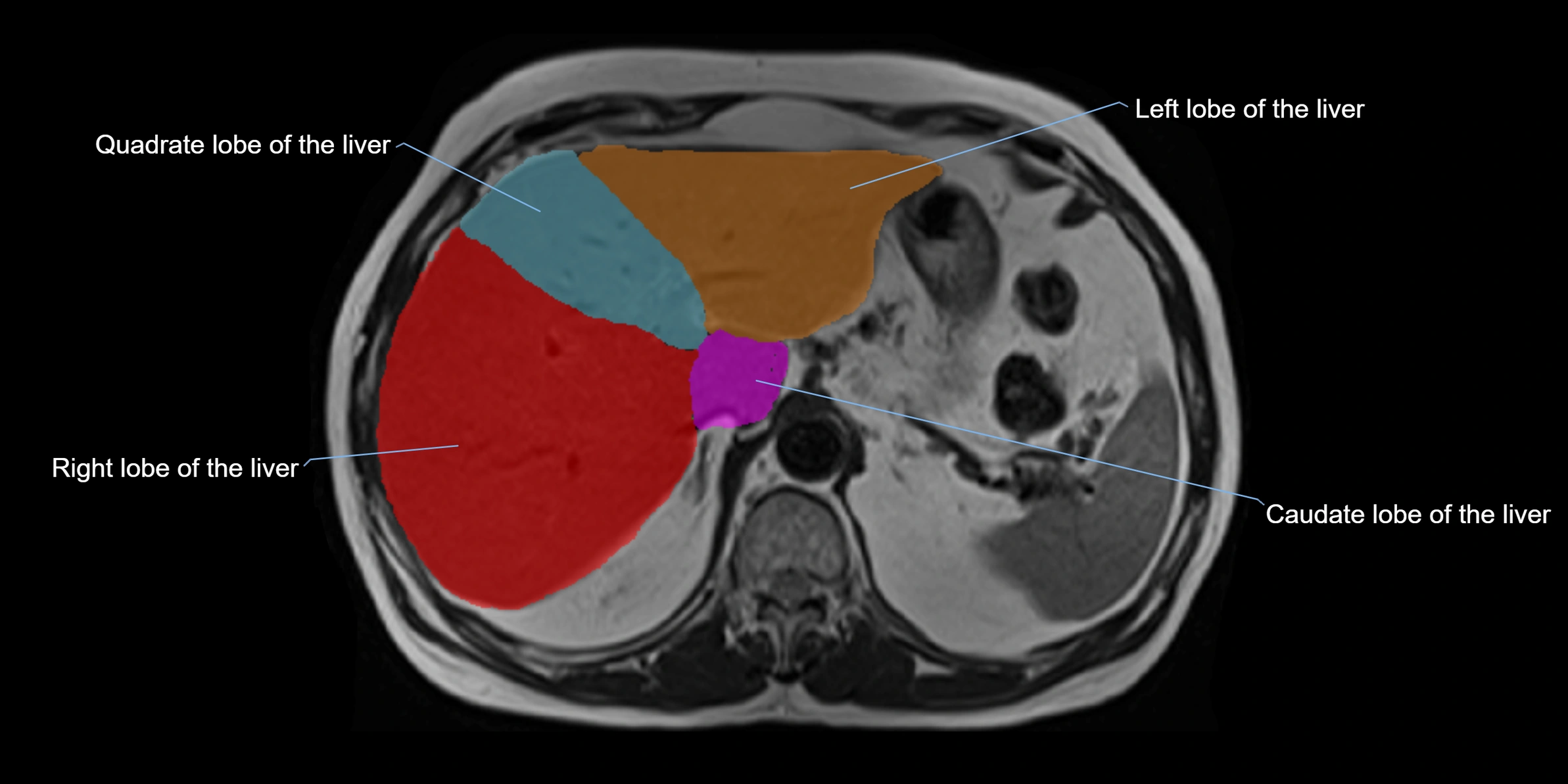
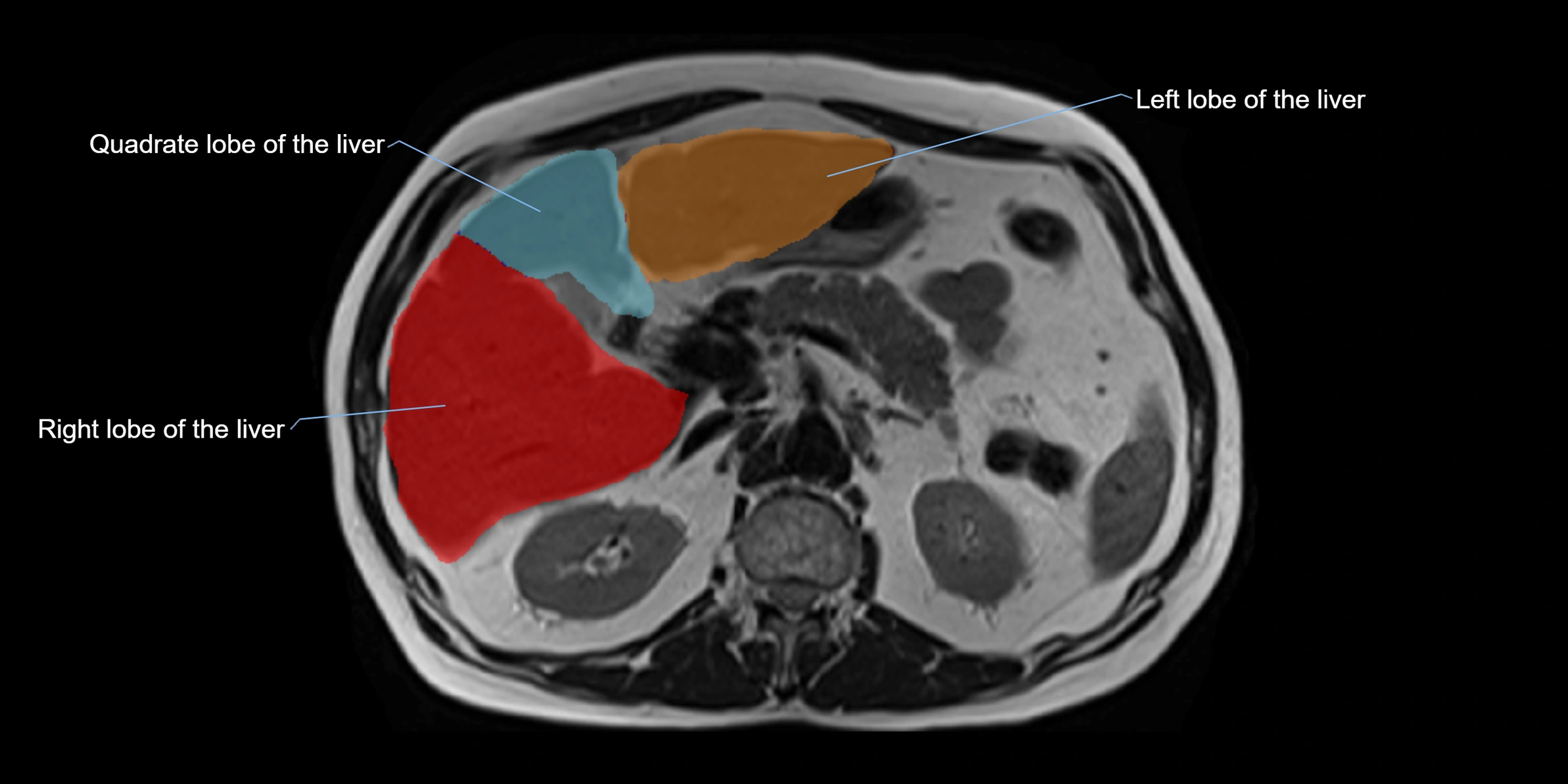
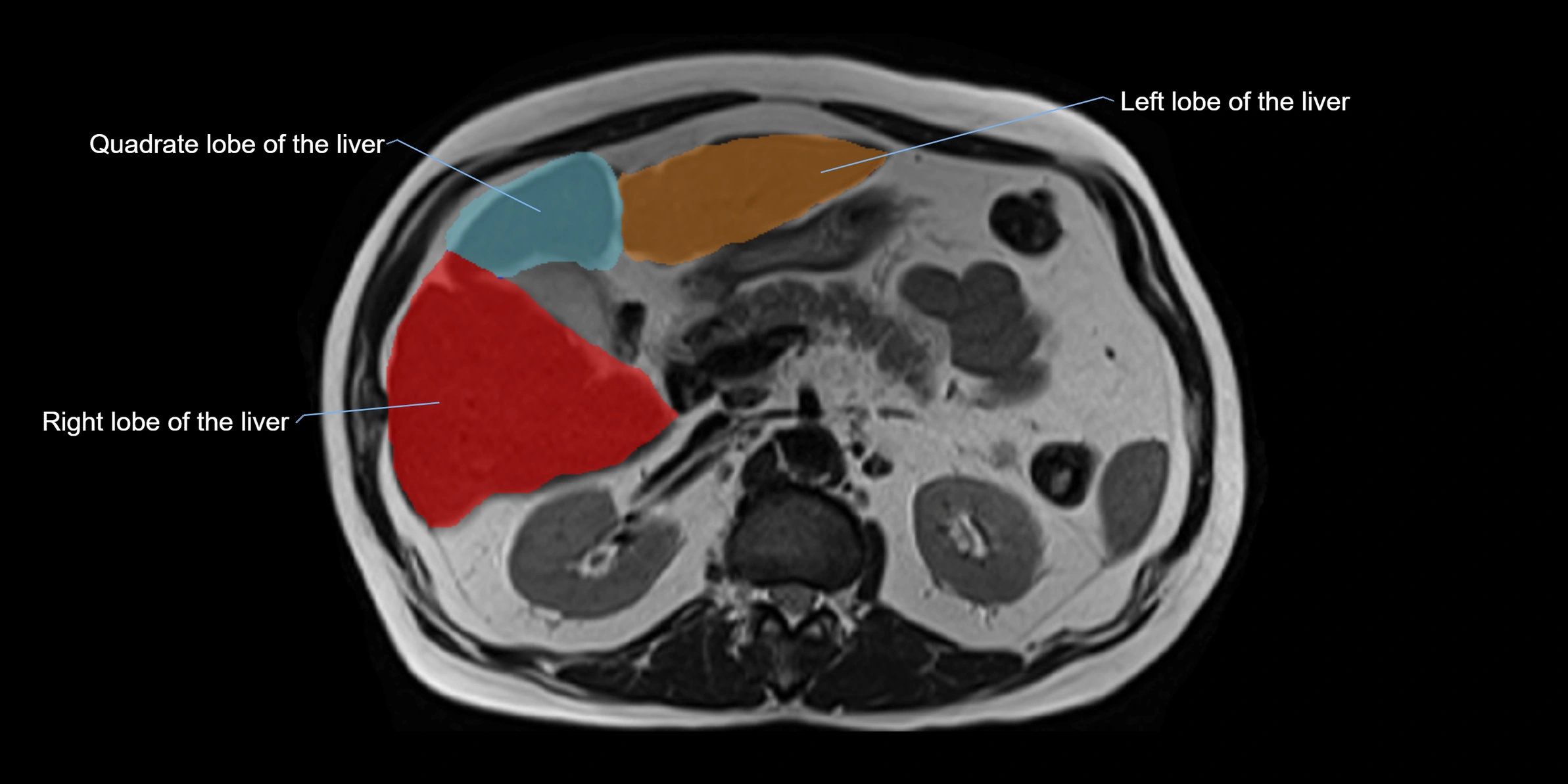
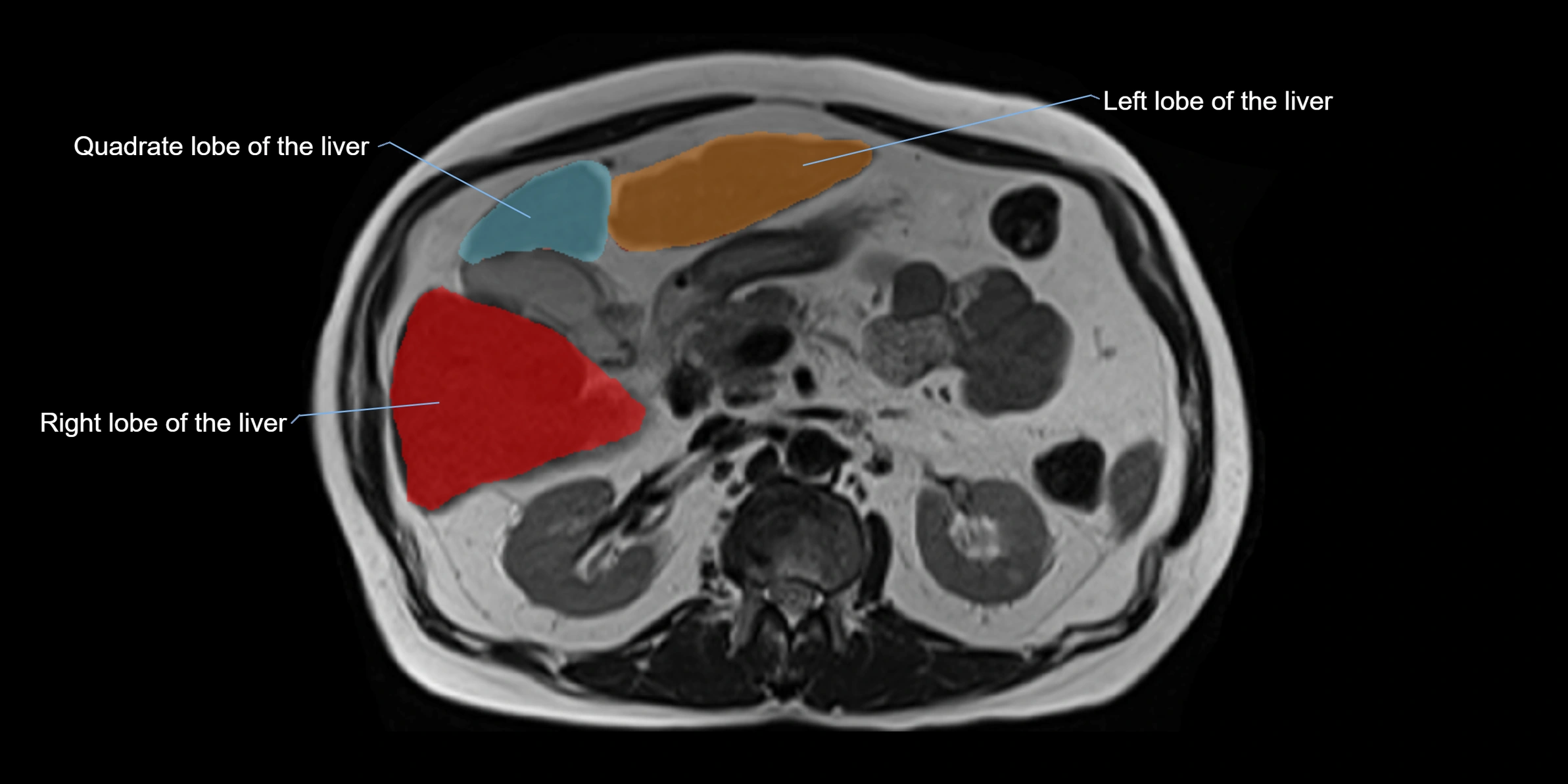
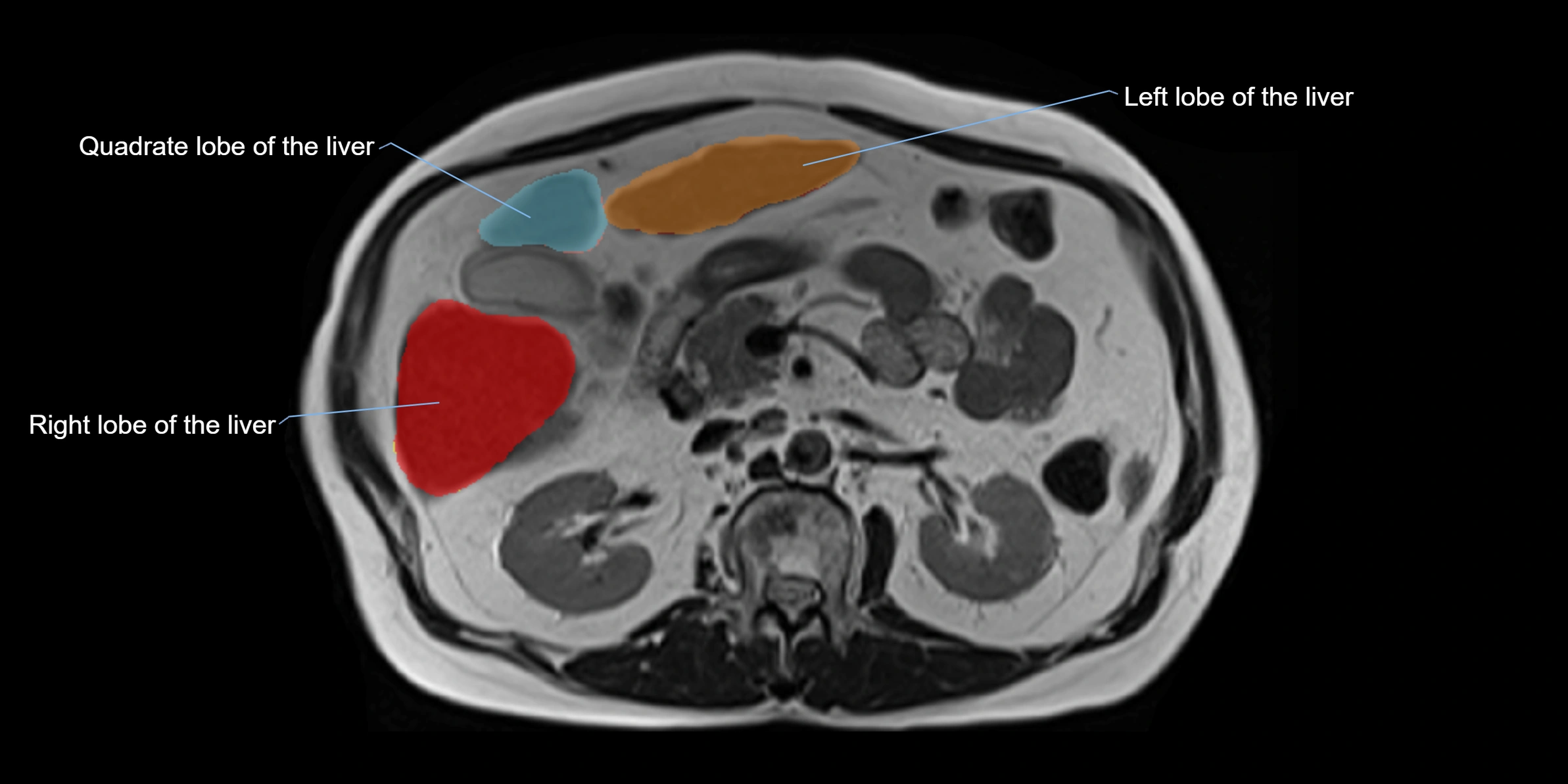
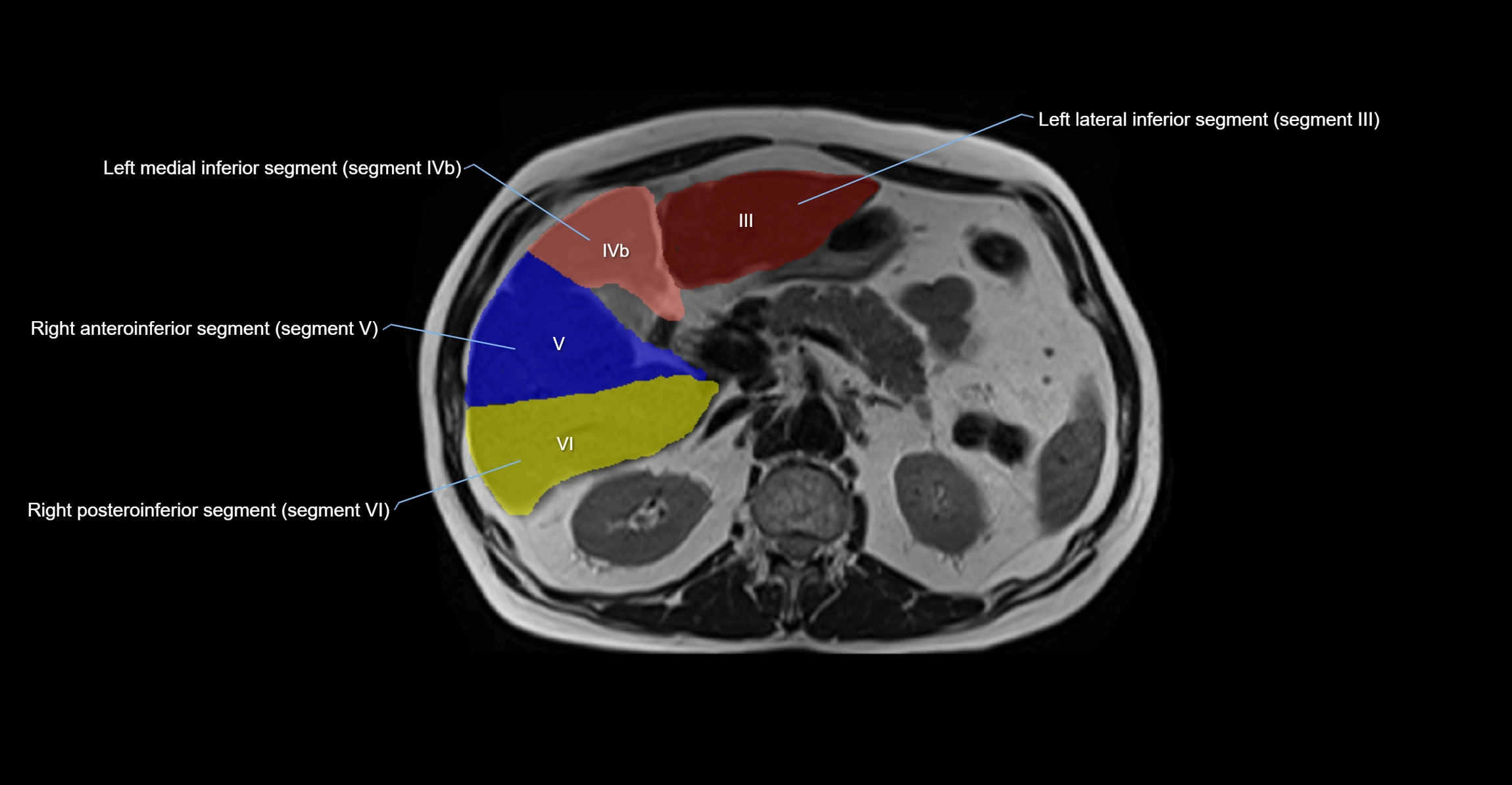
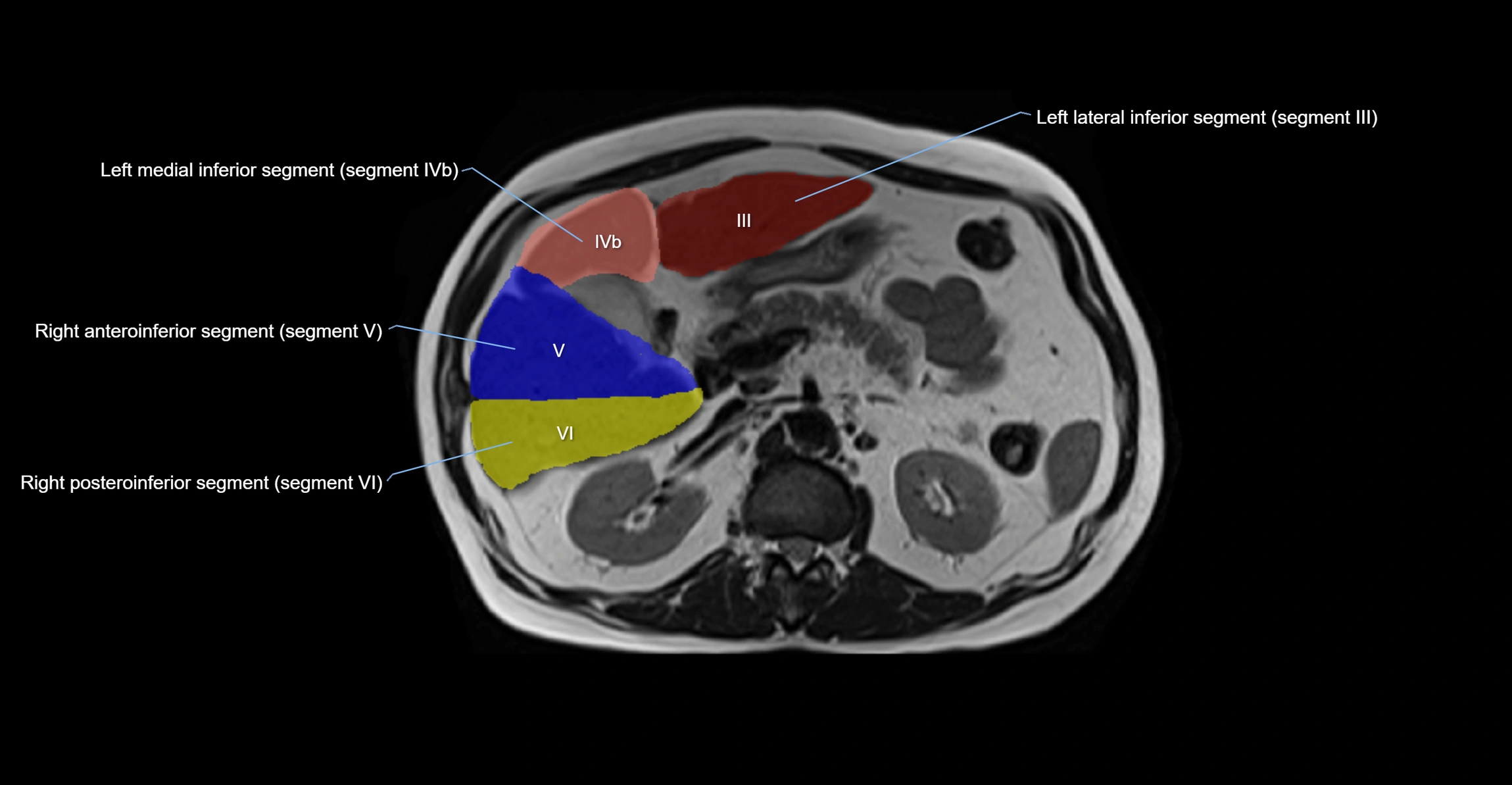
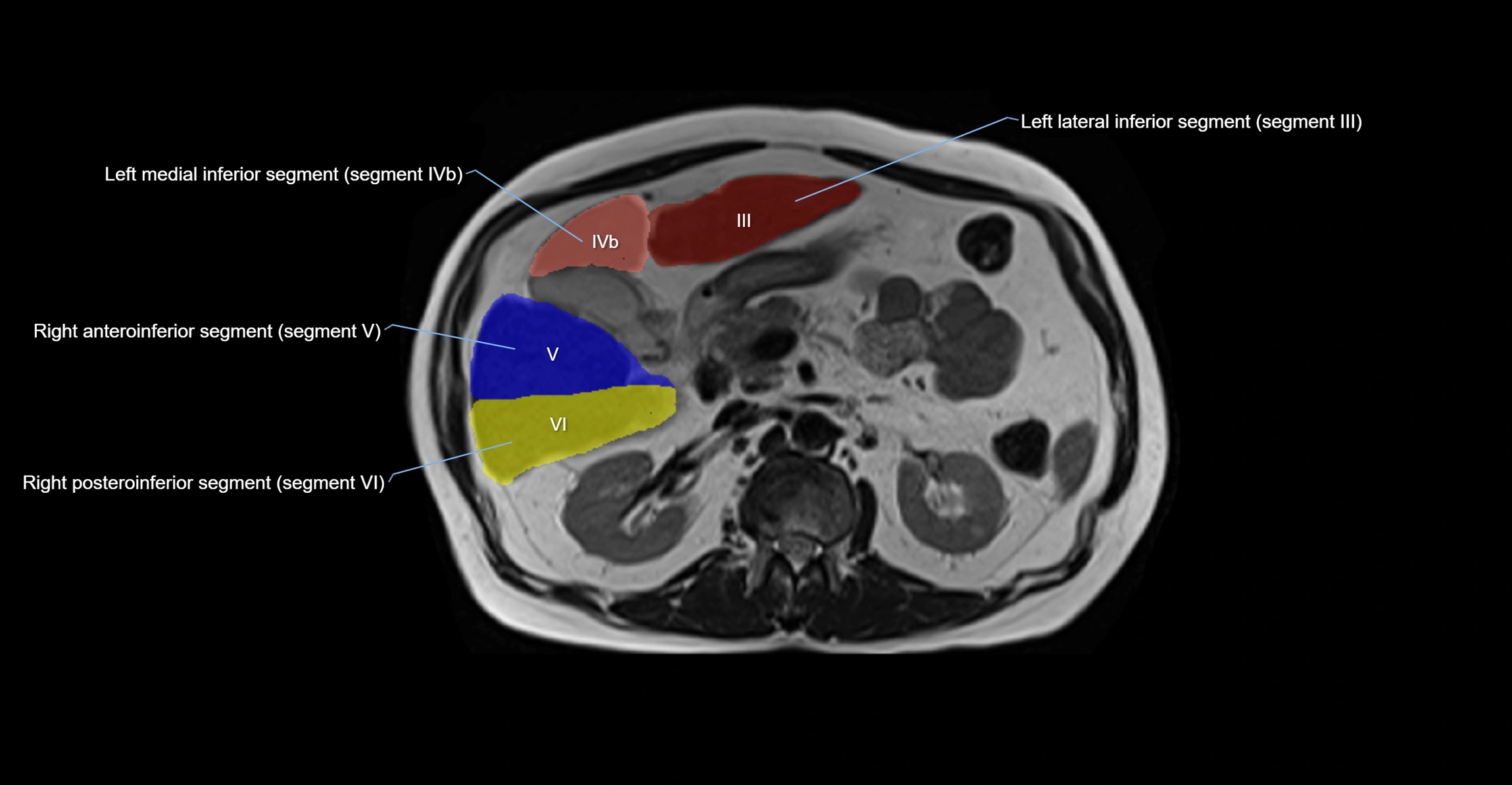
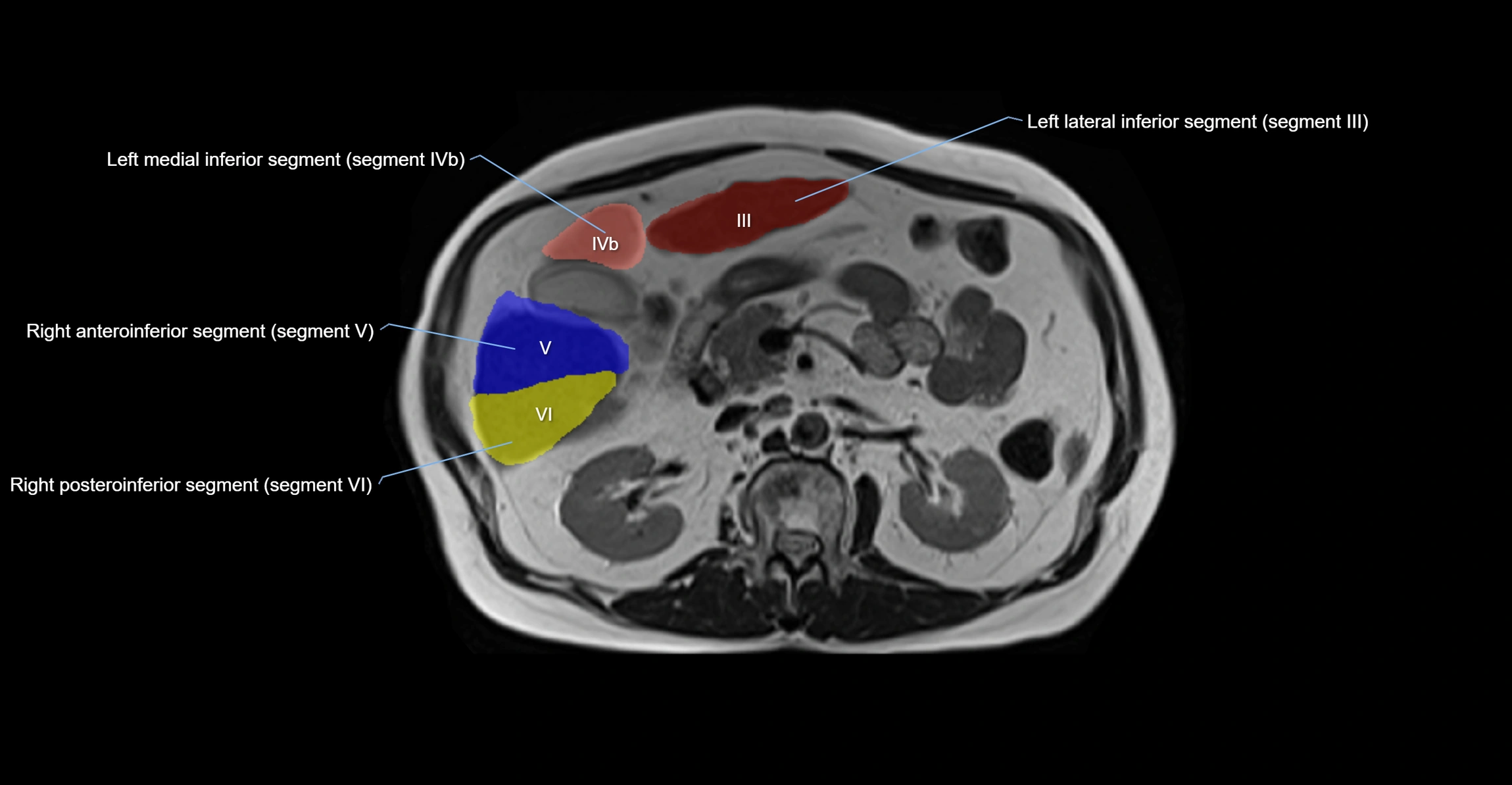
MRI image
