Topic
The abductor pollicis longus (APL) tendon is a strong, flat tendon that arises from the abductor pollicis longus muscle in the posterior compartment of the forearm. It is one of the key tendons of the first dorsal compartment of the wrist, alongside the extensor pollicis brevis (EPB) tendon. Its main function is to abduct and extend the thumb at the carpometacarpal (CMC) joint, assisting in grasp and pinch movements.
The APL tendon is highly variable and often has multiple slips, sometimes inserting onto both the base of the first metacarpal and the trapezium. Due to its close anatomical relationship with the EPB tendon within a tight fibro-osseous tunnel, the APL is commonly involved in De Quervain’s tenosynovitis, a painful inflammatory condition of the radial wrist.
Synonyms
-
APL tendon
-
Long abductor tendon of the thumb
-
First dorsal compartment tendon (with EPB)
Origin, Course, and Insertion
-
Origin: Posterior surface of the ulna and radius, and the adjacent interosseous membrane, distal to the supinator muscle
-
Course:
-
Tendon forms in the distal third of the forearm and passes obliquely downward and laterally.
-
Travels beneath the extensor retinaculum within the first dorsal compartment of the wrist.
-
Often runs in a common synovial sheath with the extensor pollicis brevis tendon.
-
-
Insertion:
-
Main insertion on the lateral base of the first metacarpal bone.
-
Accessory slips may insert into the trapezium, thenar fascia, or abductor pollicis brevis tendon.
-
Tendon Attachments
-
Firmly attached to the first metacarpal base, facilitating thumb abduction.
-
May send fibrous expansions to the thenar muscles or joint capsule.
-
Accessory tendons occasionally merge with the opponens pollicis or abductor pollicis brevis.
Relations
-
Anteriorly: Radial artery and tendons of the flexor carpi radialis and brachioradialis.
-
Posteriorly: Radius and the insertion area of the extensor pollicis longus.
-
Laterally: Extensor pollicis brevis tendon (in same compartment).
-
Medially: Extensor carpi radialis longus and brevis tendons.
-
Superiorly: Extensor retinaculum and subcutaneous tissues of the radial wrist.
Nerve Supply
-
Supplied by the posterior interosseous nerve (branch of the radial nerve, C7–C8).
Function
-
Abduction of the thumb: Moves the thumb away from the palm at the carpometacarpal joint.
-
Extension of thumb: Assists in extending the thumb and rotating the metacarpal laterally.
-
Stabilization: Supports the first metacarpal during grasp and pinching motions.
-
Synergy: Works with abductor pollicis brevis and extensor pollicis longus for coordinated thumb motion.
Clinical Significance
-
De Quervain’s tenosynovitis: Inflammation of the APL and EPB tendons in their shared compartment, causing radial wrist pain.
-
Tendinopathy: Chronic overuse may cause thickening or fraying of the APL tendon.
-
Accessory tendons: Multiple APL slips can contribute to tenosynovial crowding and predispose to entrapment.
-
Surgical relevance: APL tendon transfers may be used for thumb reconstruction or radial nerve palsy.
-
Imaging role: MRI and ultrasound help assess tendon integrity, sheath inflammation, and compartmental anatomy.
MRI Appearance
-
T1-weighted images:
-
Tendon: Low signal (dark) continuous band extending to the first metacarpal base.
-
Muscle belly: Intermediate signal.
-
Surrounding fat: Bright, aiding tendon visualization.
-
Pathology: Tendon thickening, irregularity, or focal intermediate signal in tendinopathy.
-
-
T2-weighted images:
-
Normal tendon: Low signal intensity, darker than on T1.
-
Surrounding sheath: Low to intermediate signal.
-
Pathology: Bright hyperintense signal in or around tendon in tenosynovitis.
-
Fluid in sheath: well-defined bright rim encircling tendon.
-
-
STIR:
-
Normal tendon: Dark linear structure.
-
Pathologic tendon: Bright hyperintensity in peritendinous tissues from edema or inflammation.
-
Excellent for early detection of De Quervain’s changes and soft-tissue edema.
-
-
Proton Density Fat-Saturated (PD FS):
-
Normal tendon: Dark, sharply defined.
-
Pathology: Bright intratendinous signal in partial tears or degeneration.
-
Peritendinous fluid appears hyperintense along the sheath, confirming tenosynovitis.
-
-
T1 Fat-Sat Post-Contrast:
-
Normal tendon: minimal enhancement.
-
Inflamed synovium or tendon sheath: diffuse or peripheral enhancement.
-
Chronic tendinopathy: peripheral enhancement with central low-signal fibrosis.
-
CT Appearance
Non-Contrast CT:
-
Tendon: Soft-tissue density along the radial wrist, anterior to the radius.
-
Readily distinguished from surrounding fat and bone contours.
-
Calcification or ossification may be seen in chronic tendinopathy.
-
Assists in evaluating bony anatomy of the first dorsal compartment and metacarpal base.
Post-Contrast CT (standard):
-
Tendon itself: minimal enhancement.
-
Surrounding soft tissues may enhance in tenosynovitis, postoperative changes, or scarring.
-
Useful for assessing bony insertions, synovial proliferation, or enthesopathic changes.
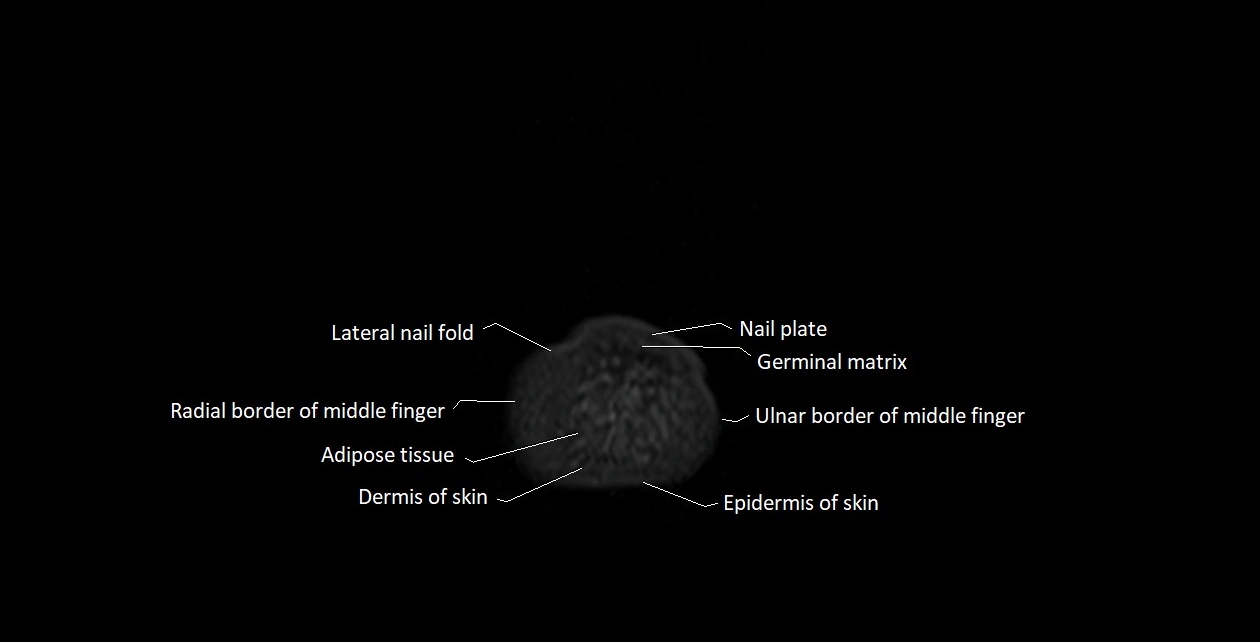
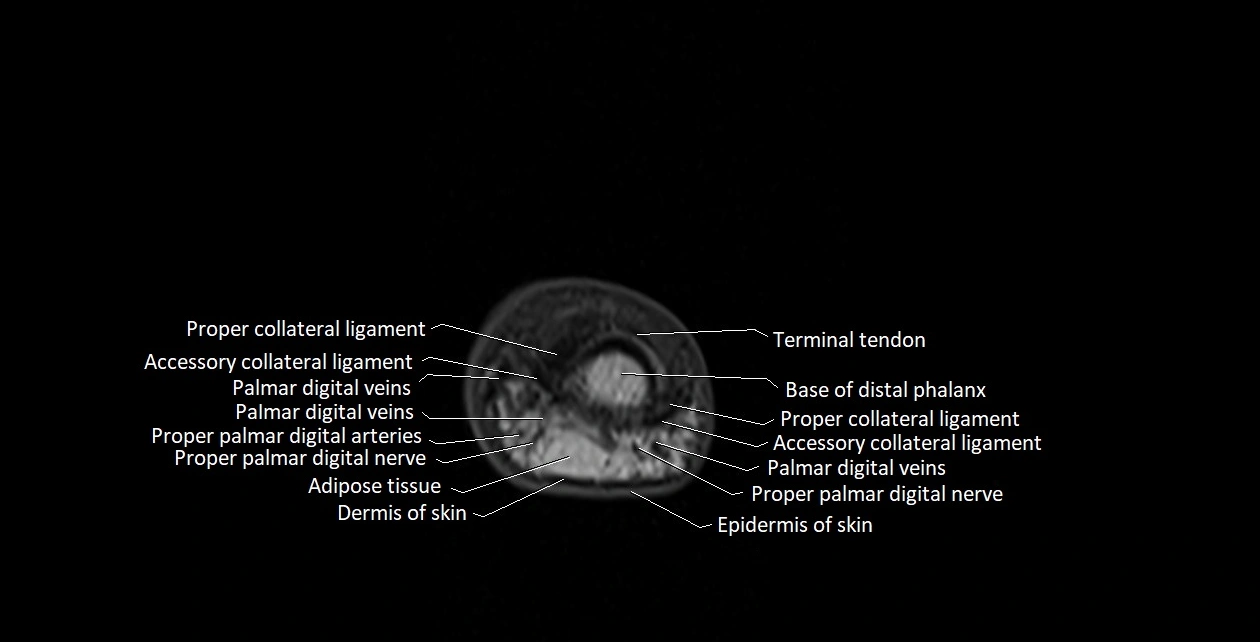
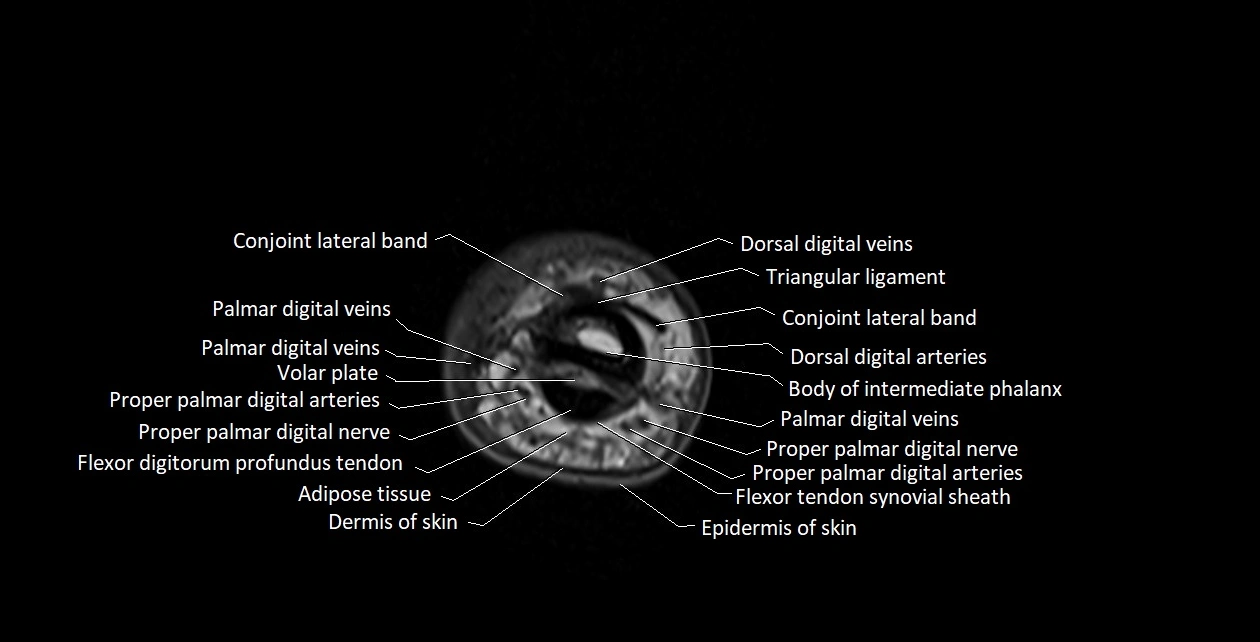
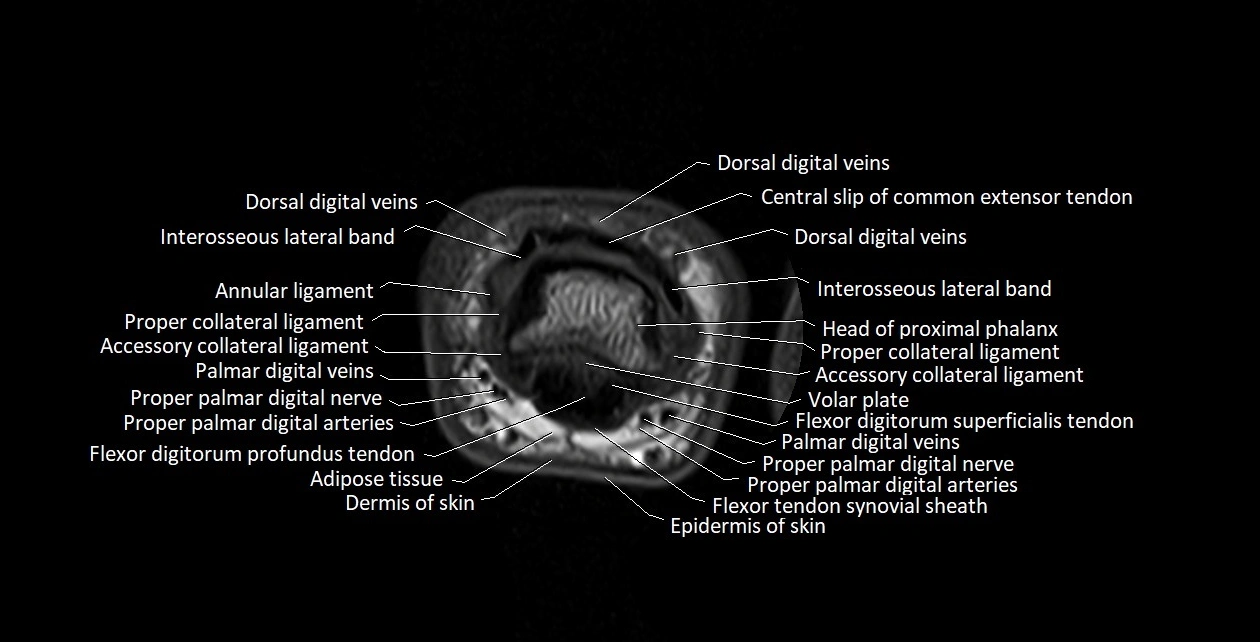
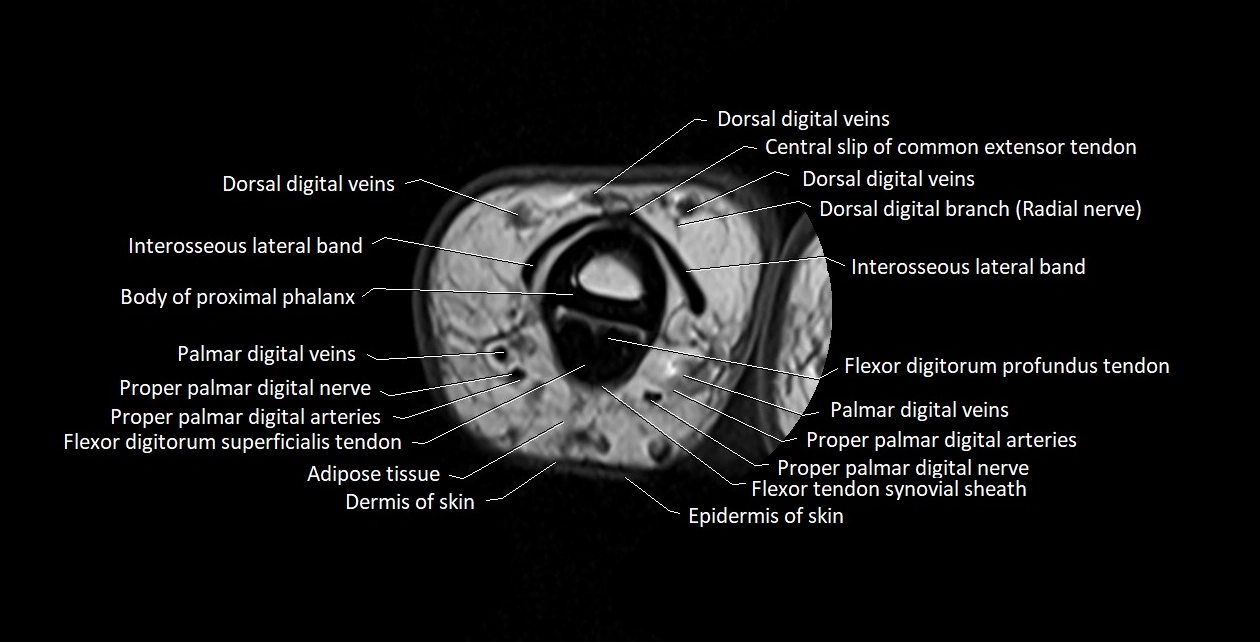
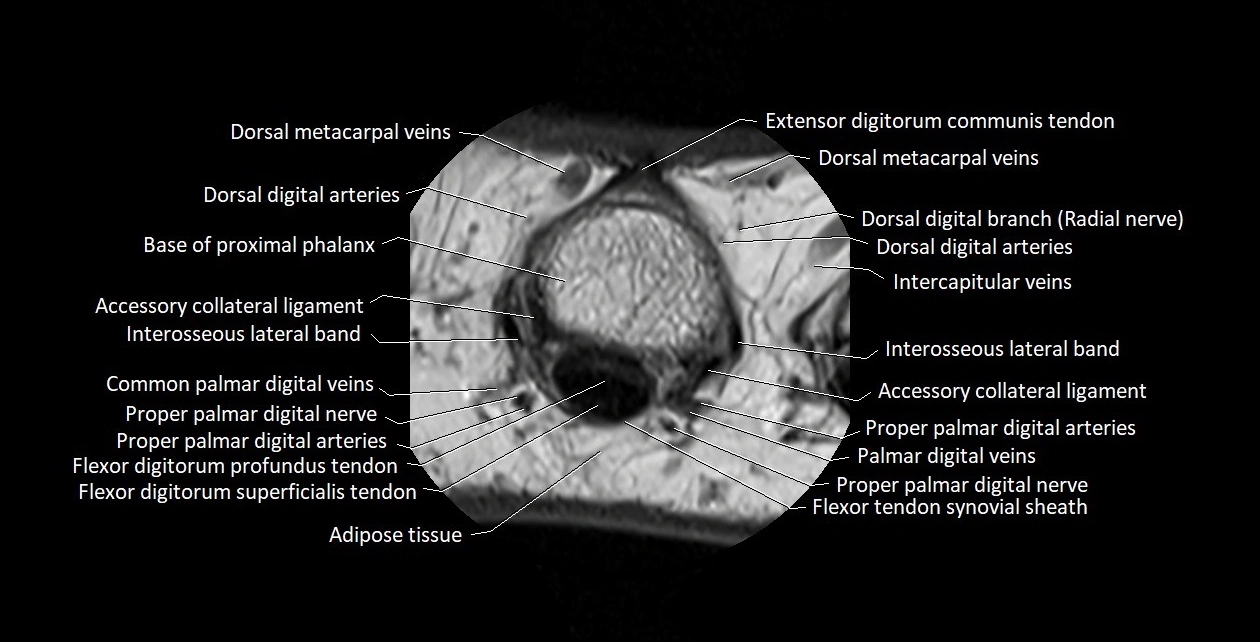
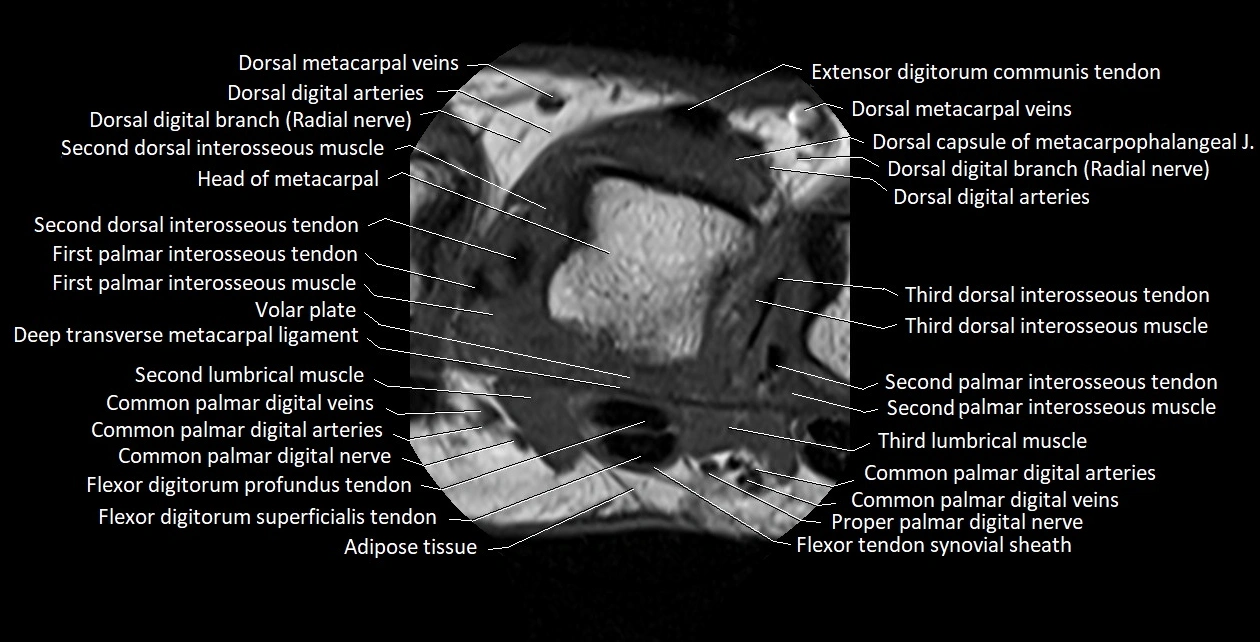
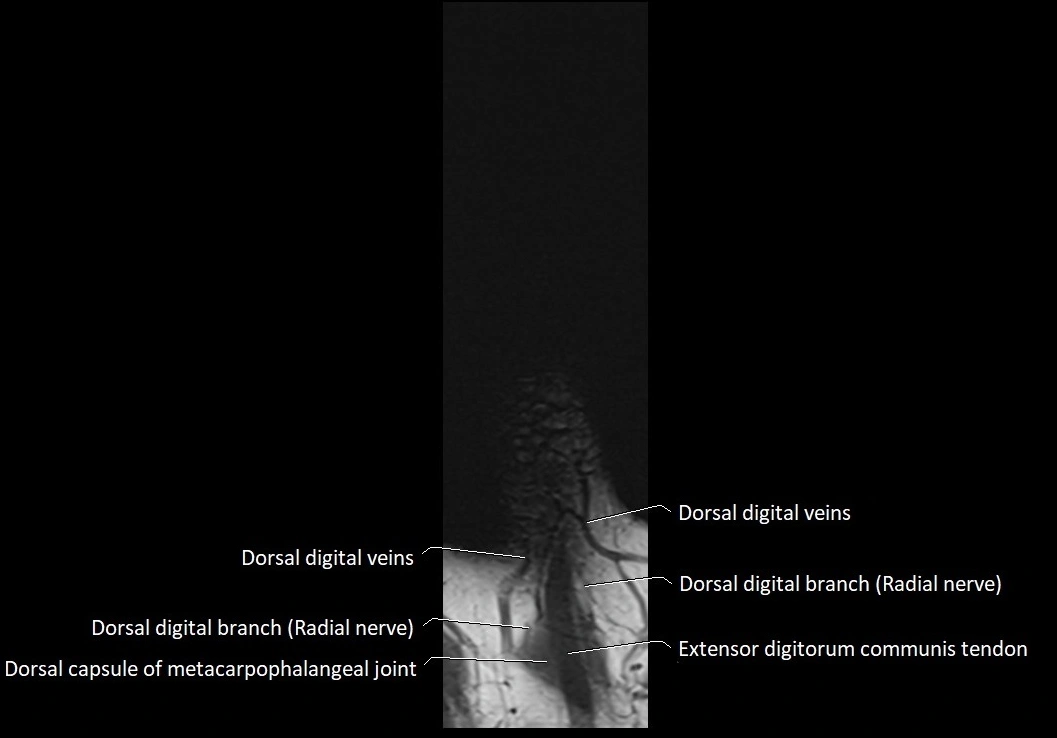
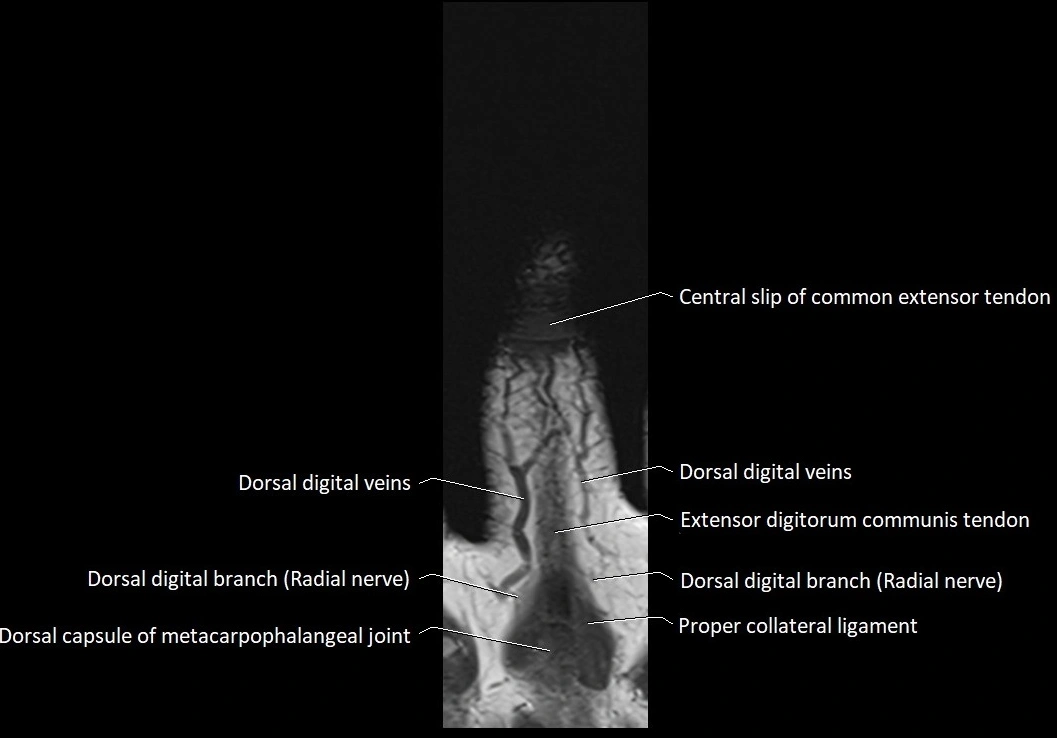
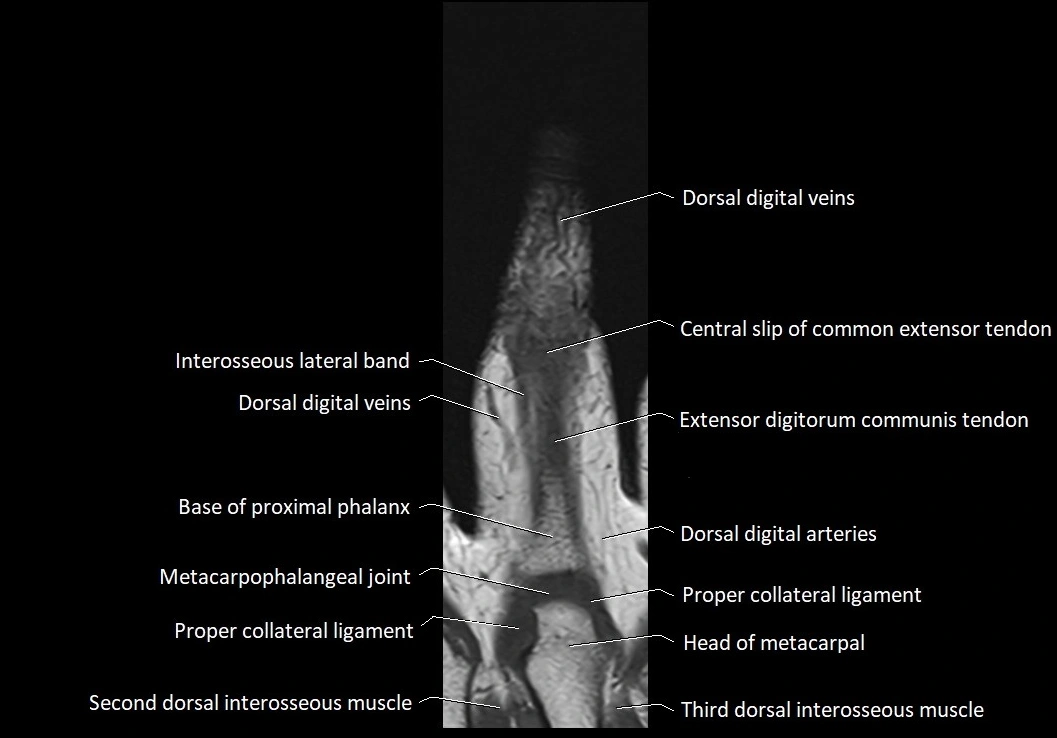
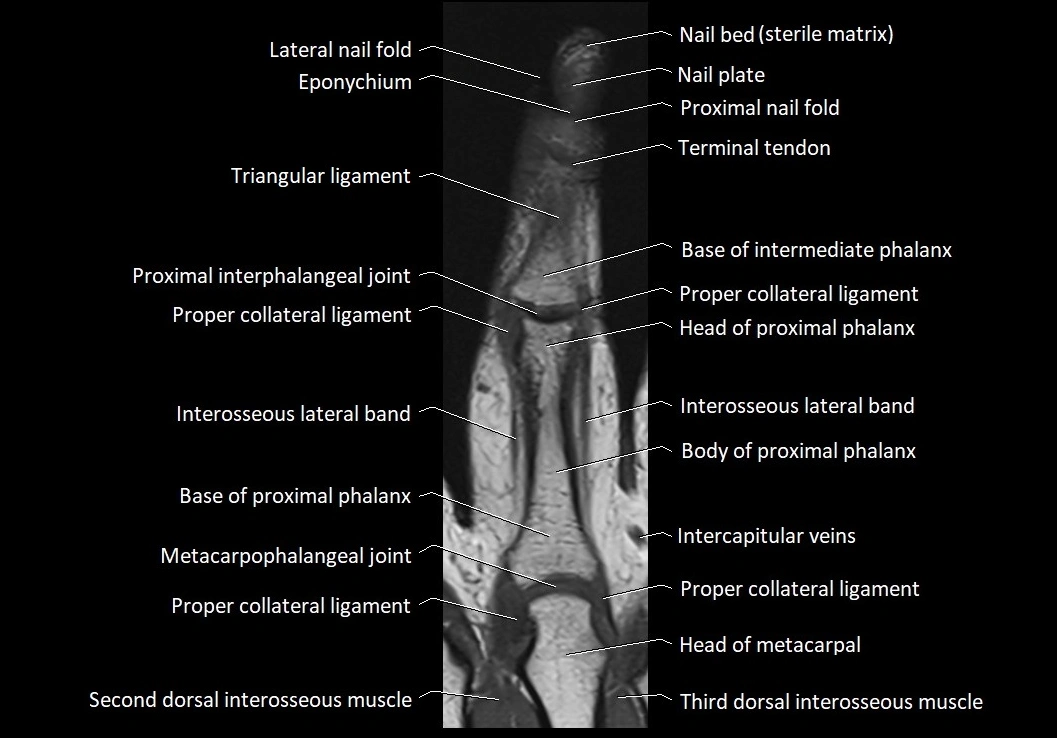
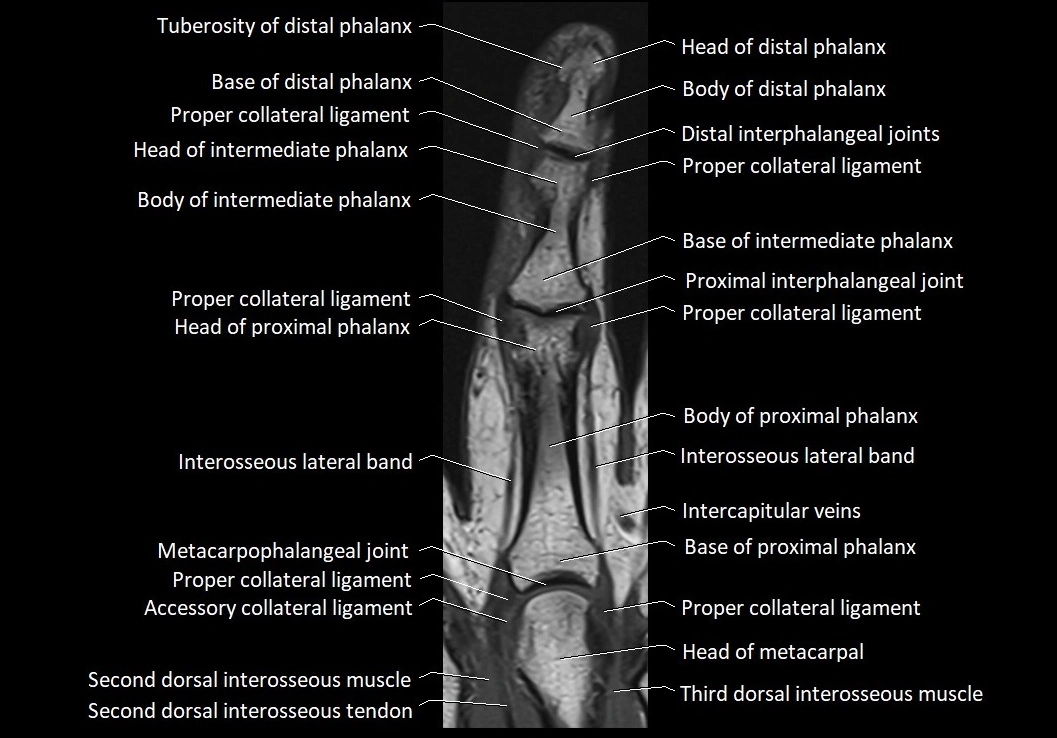
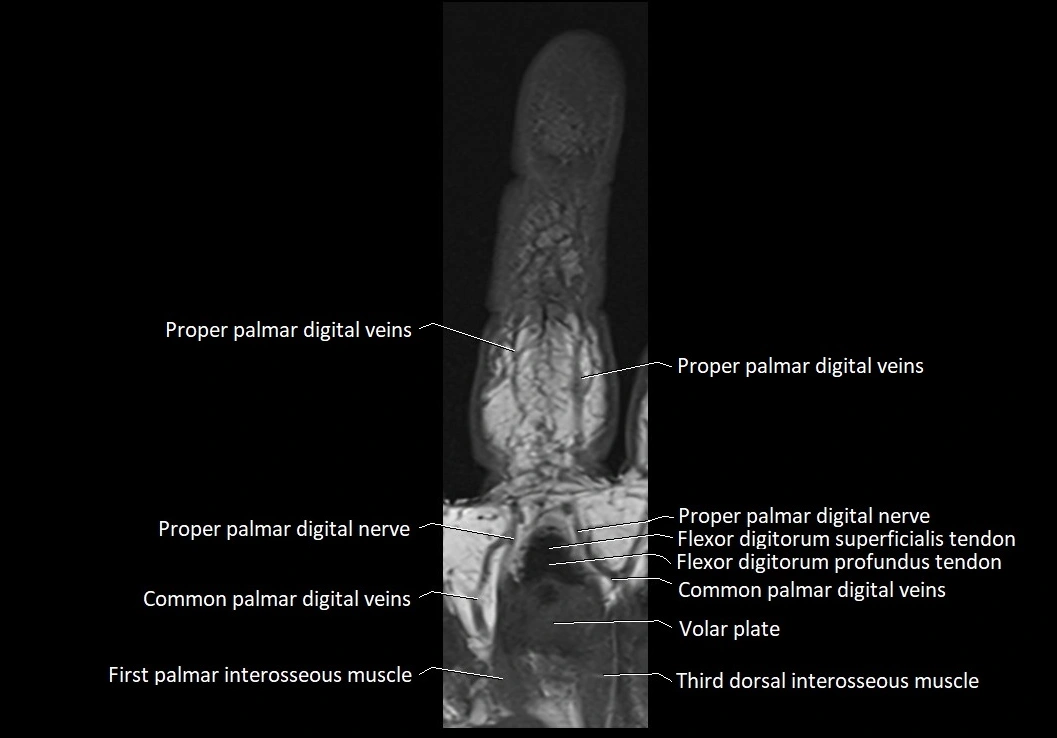
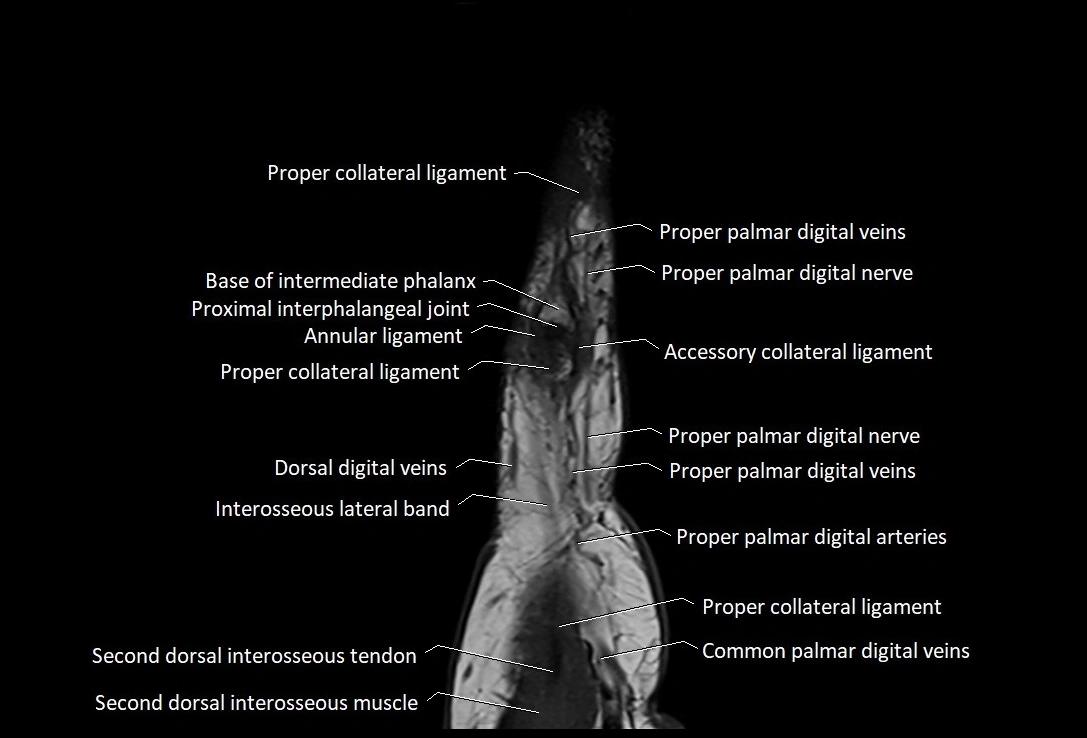
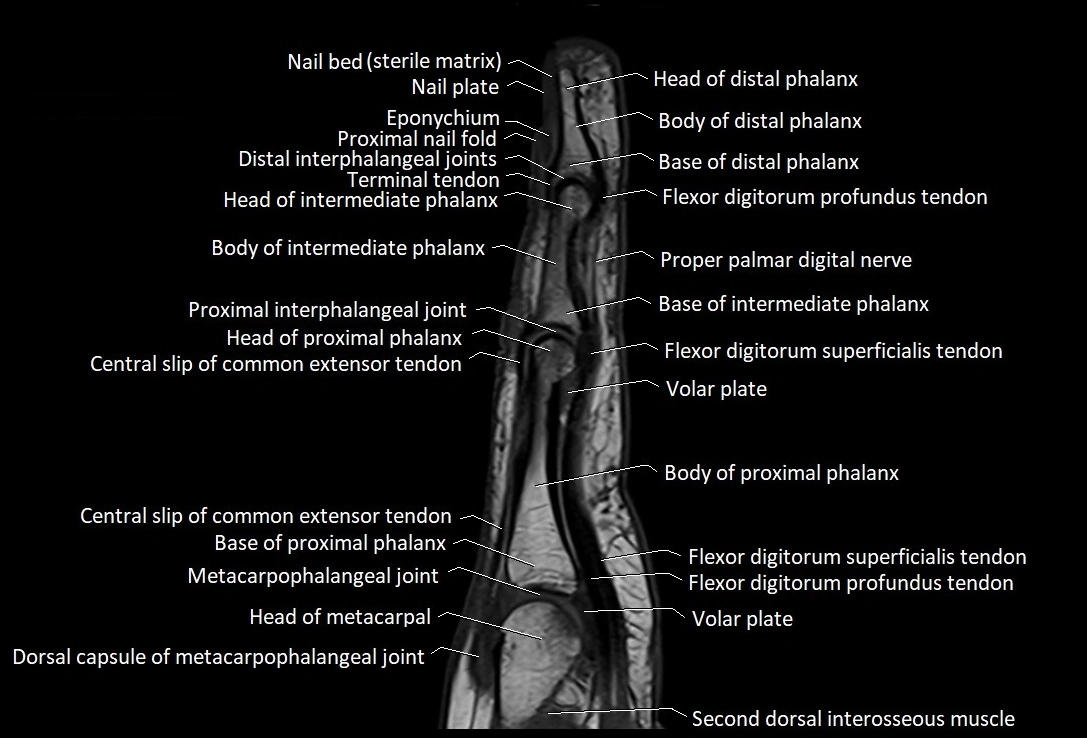
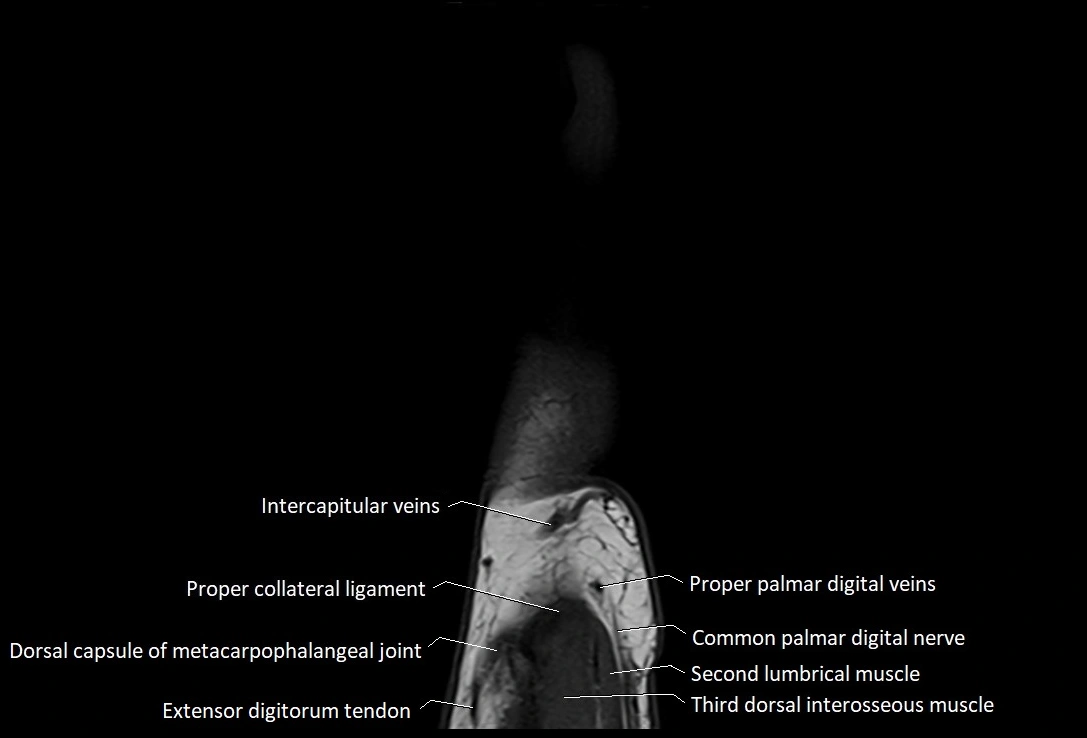
MRI images

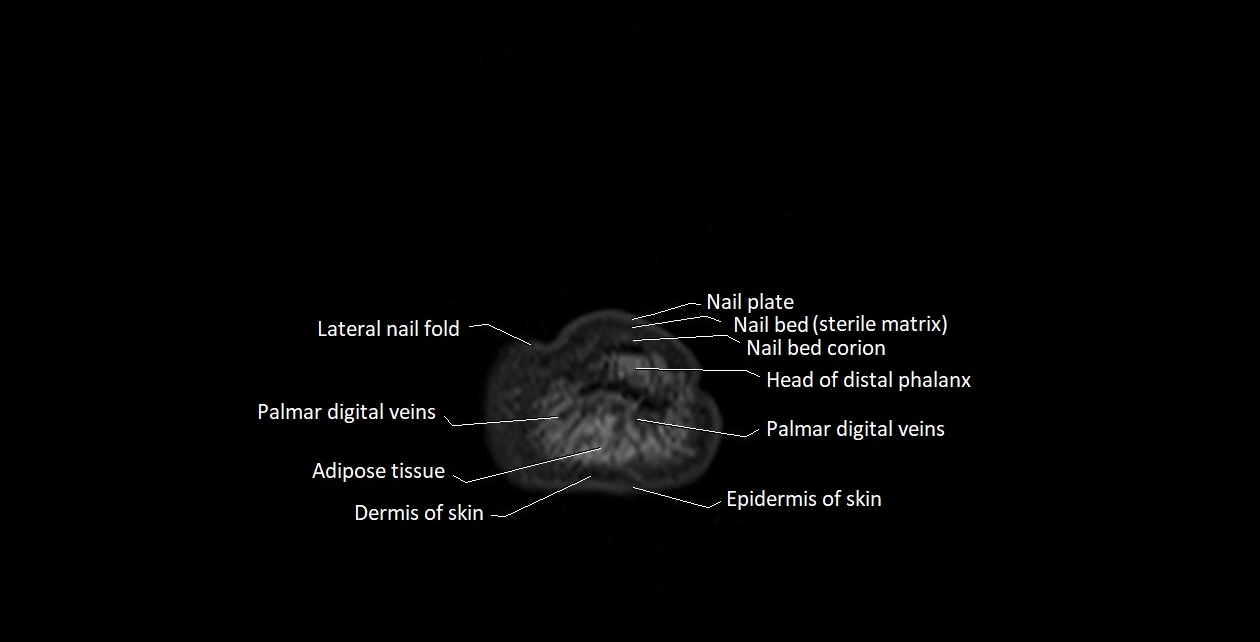
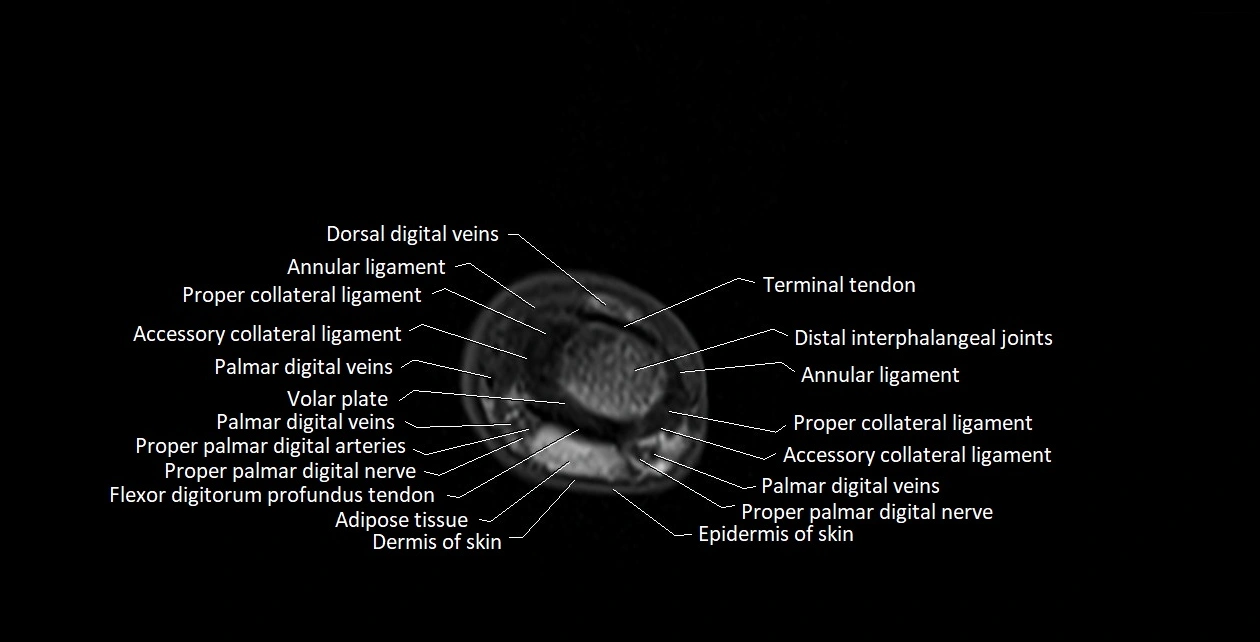
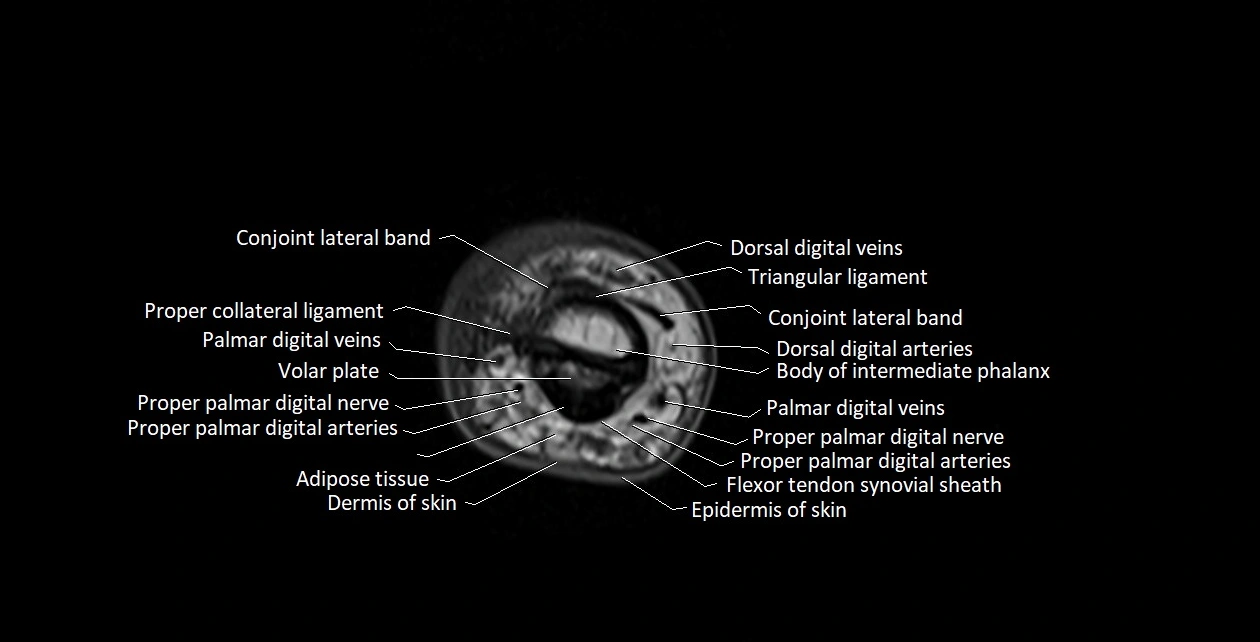
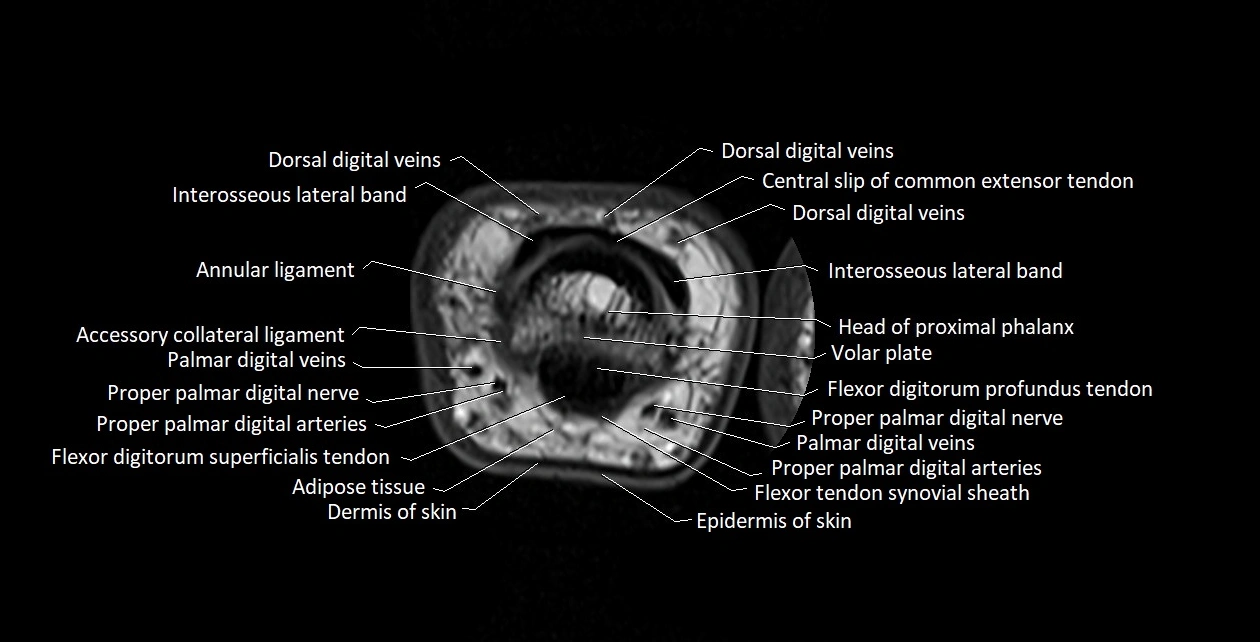
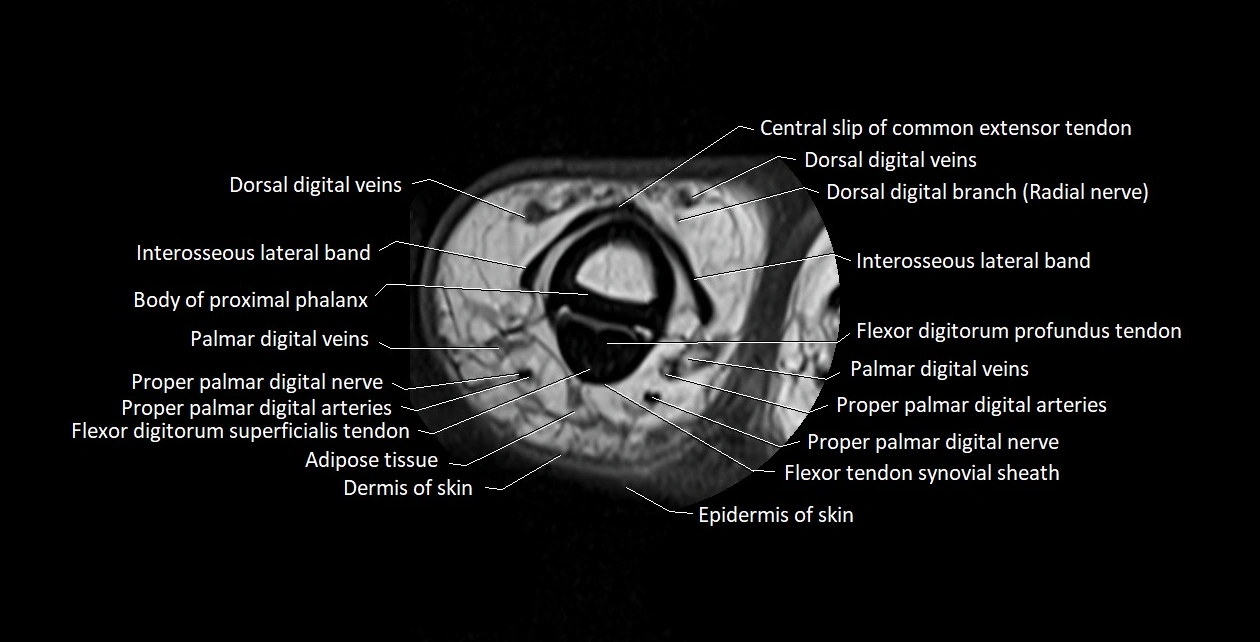
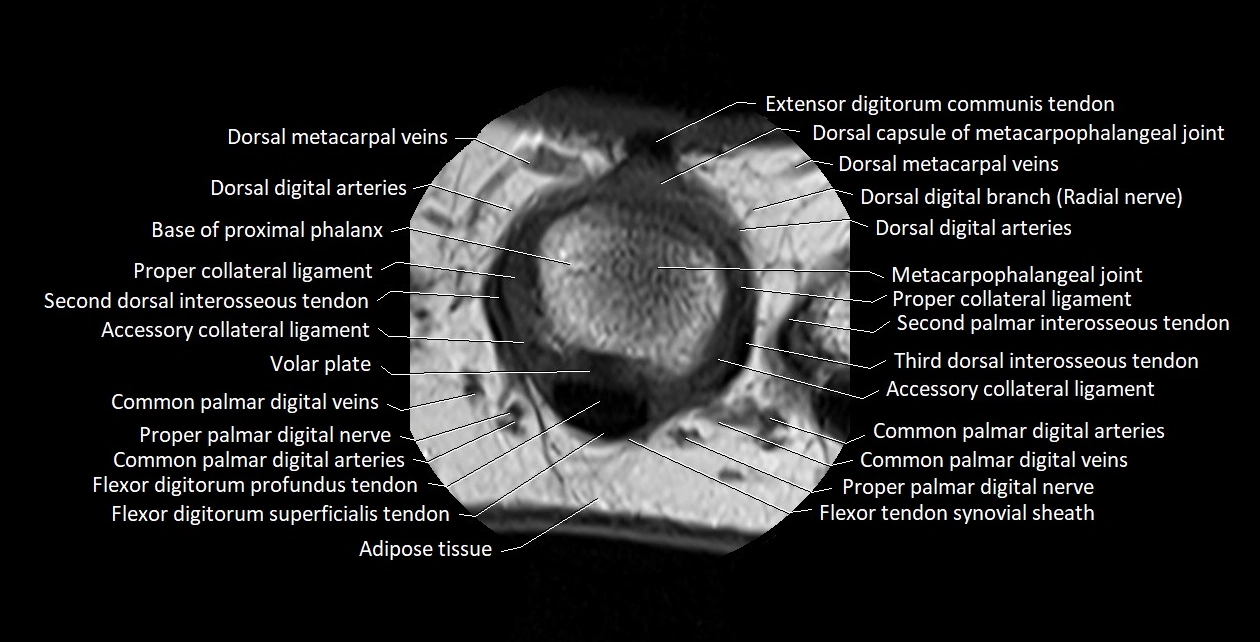
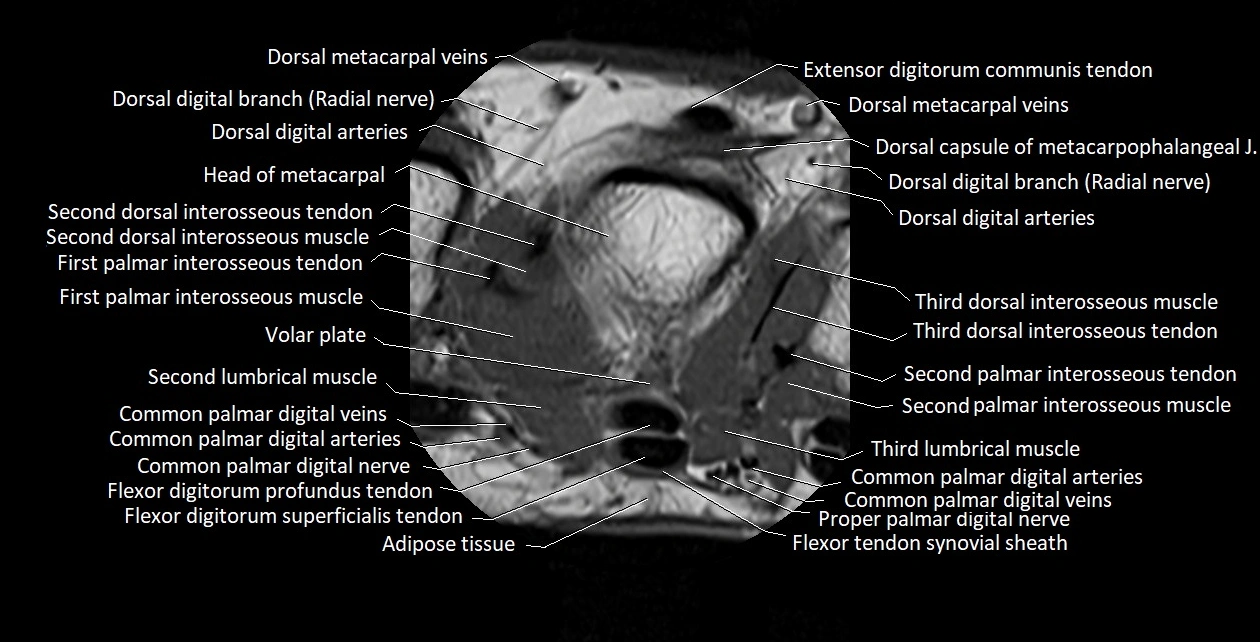
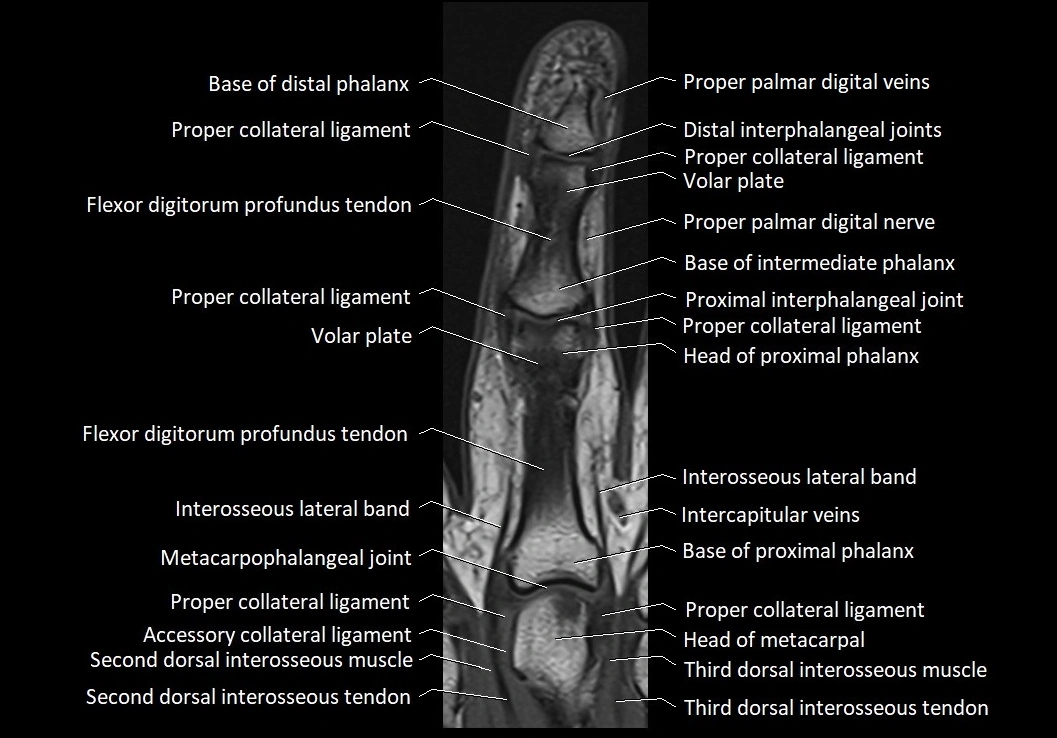
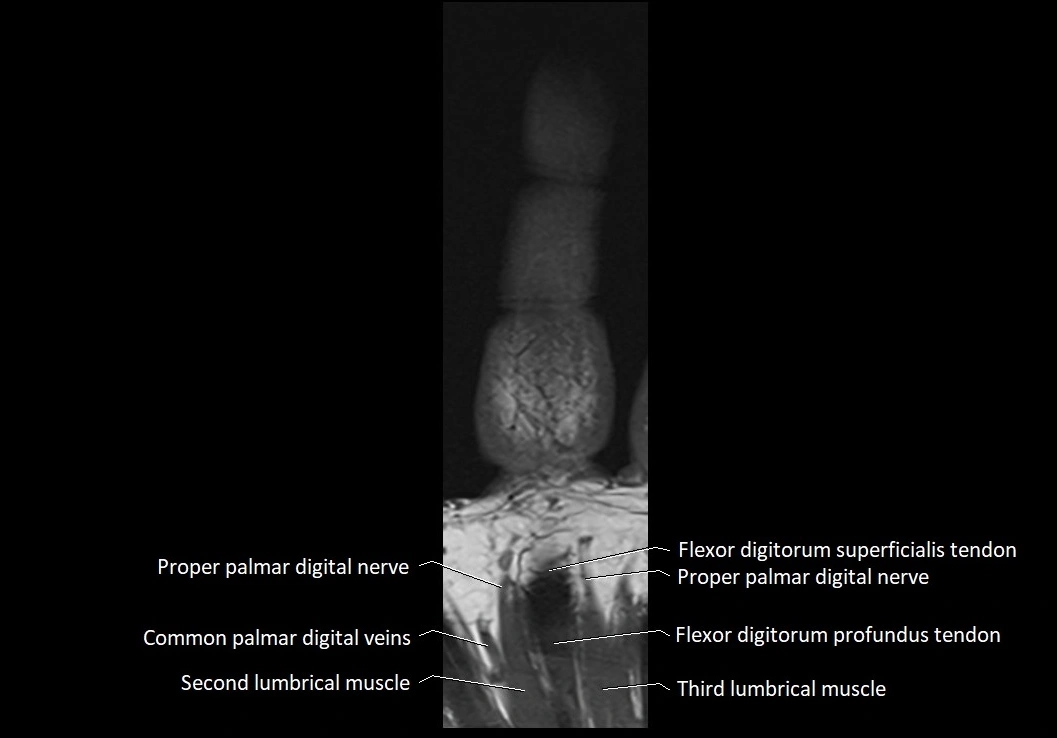
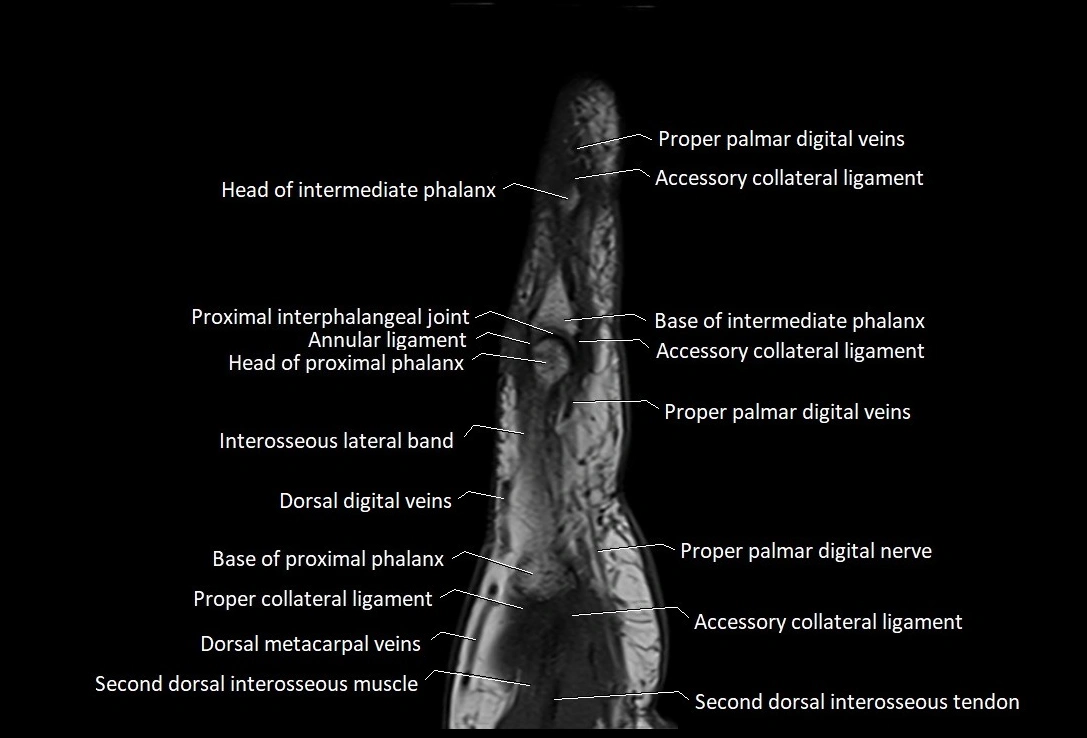
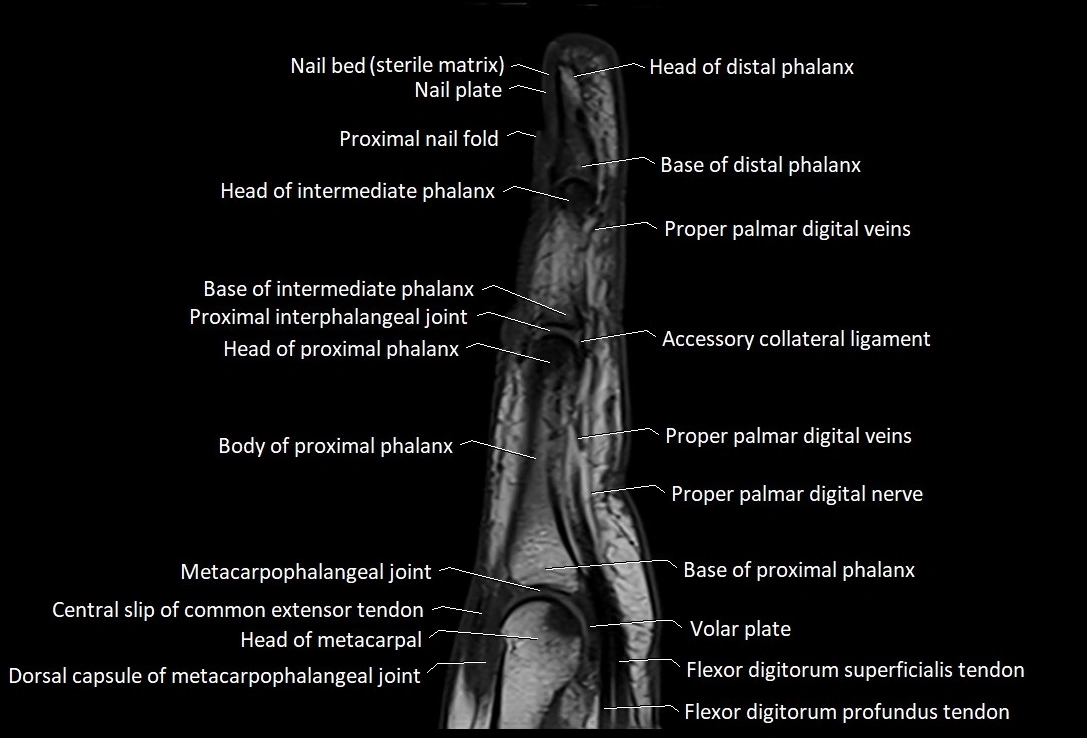
MRI images

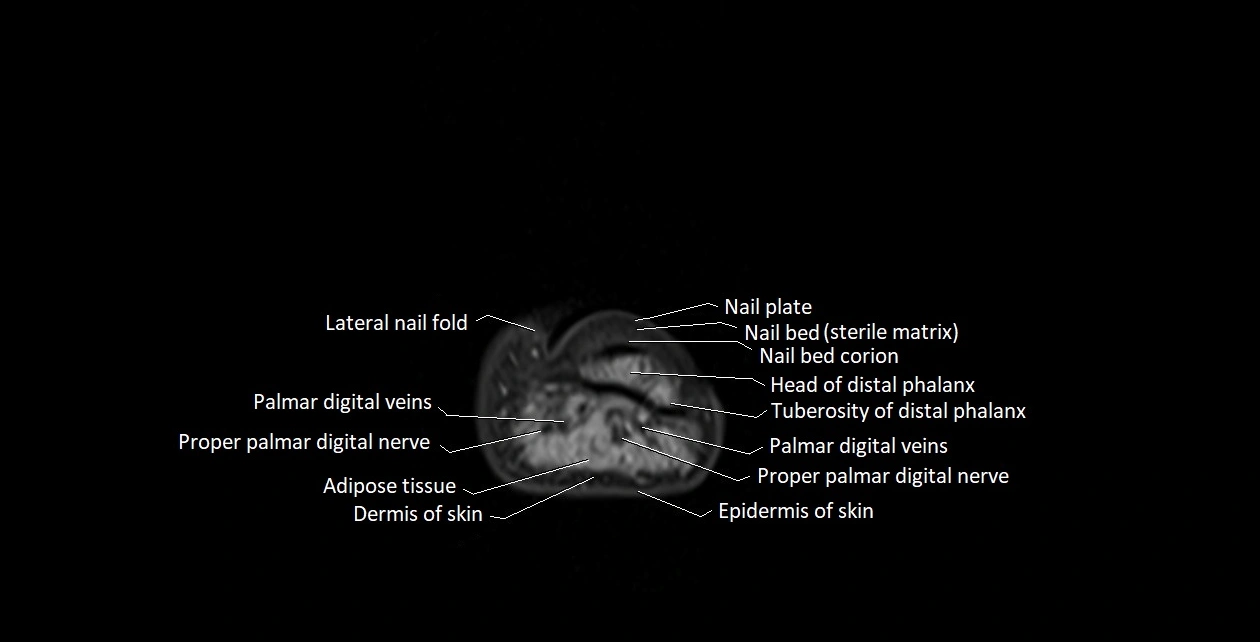
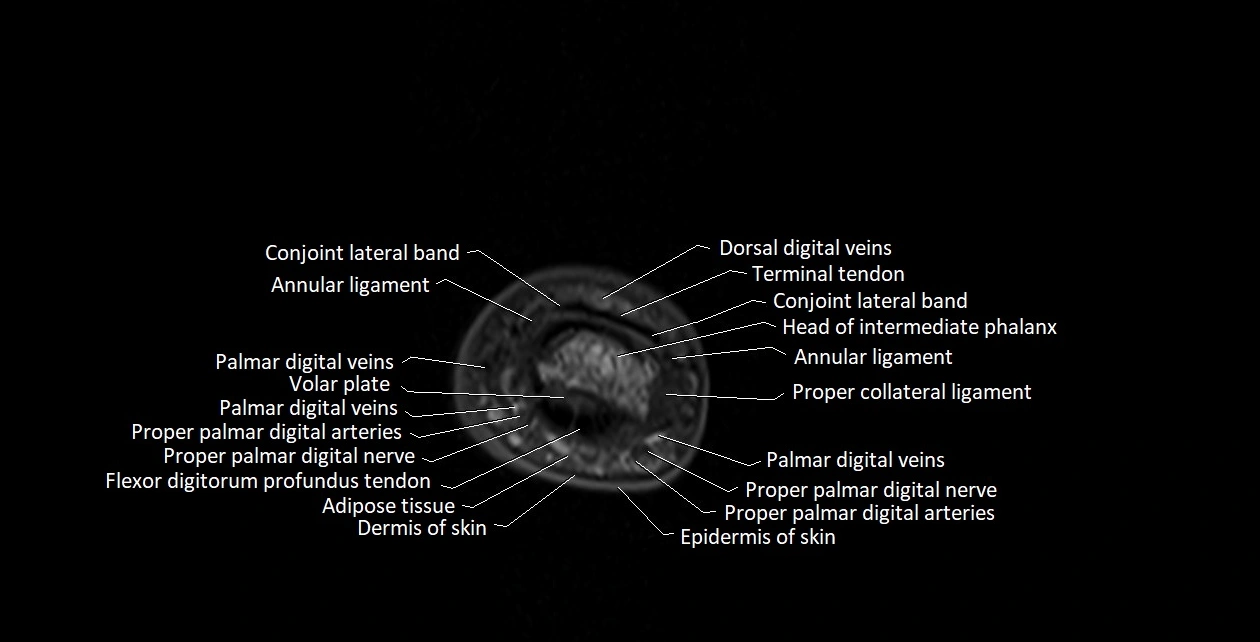
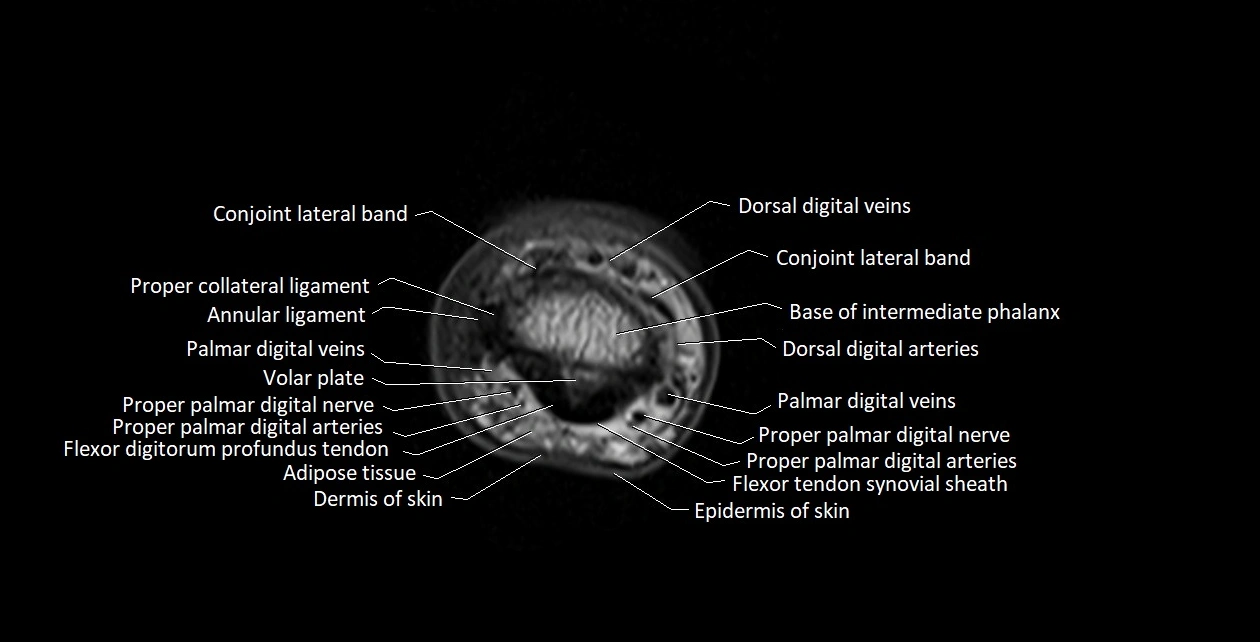
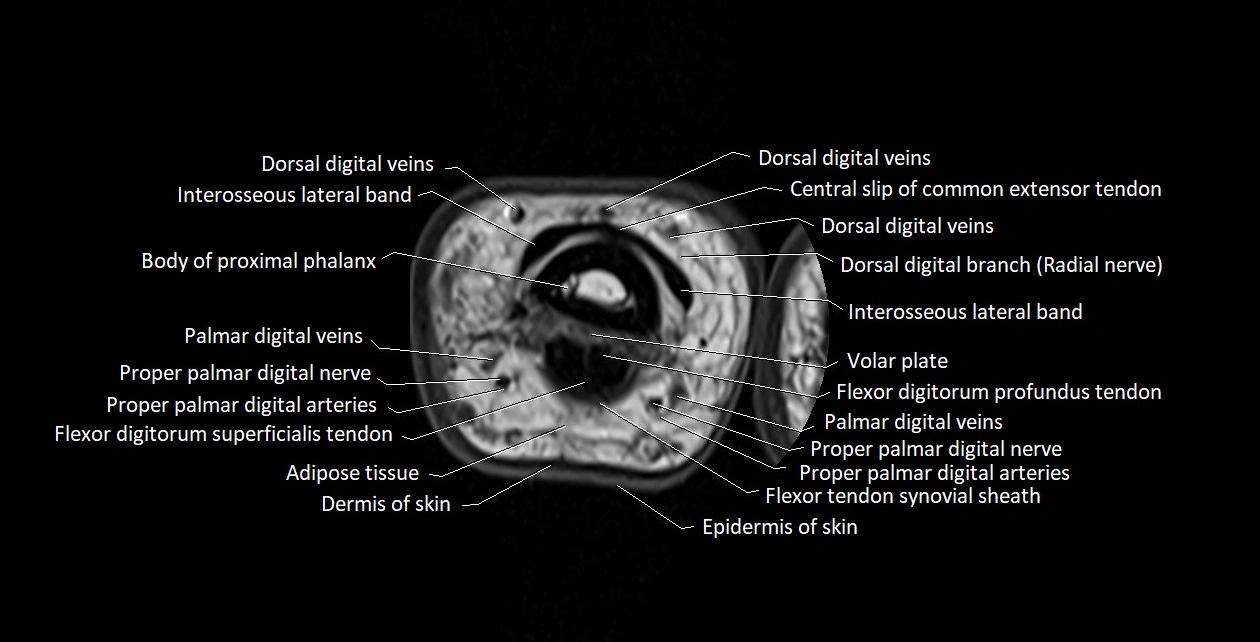
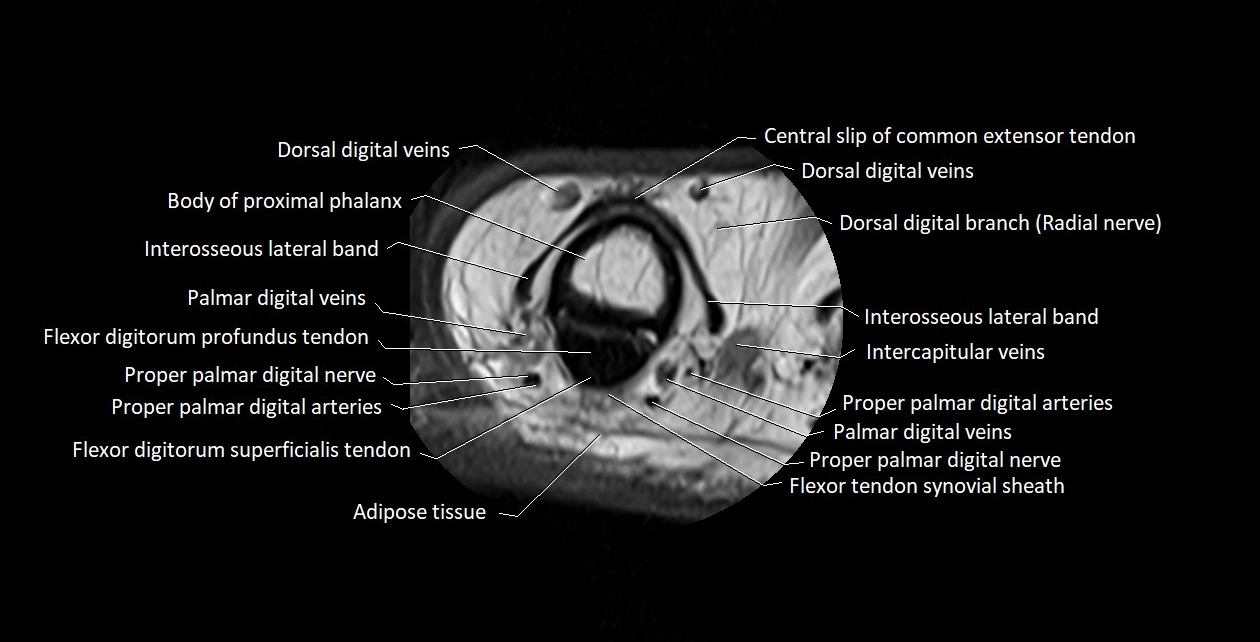
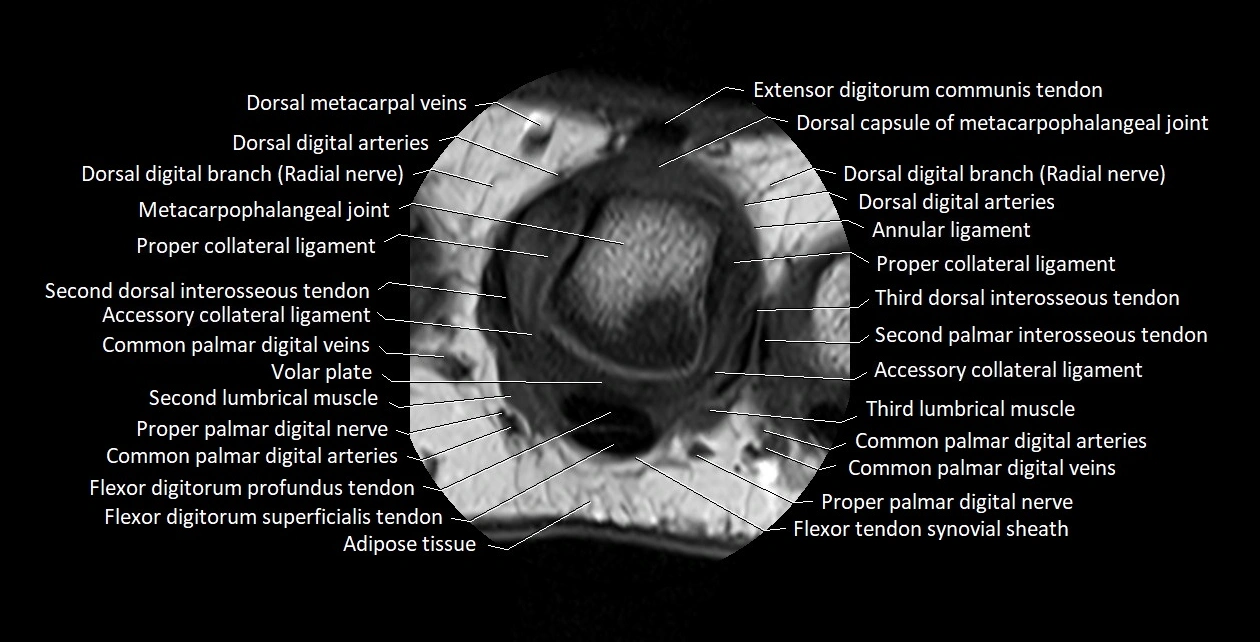
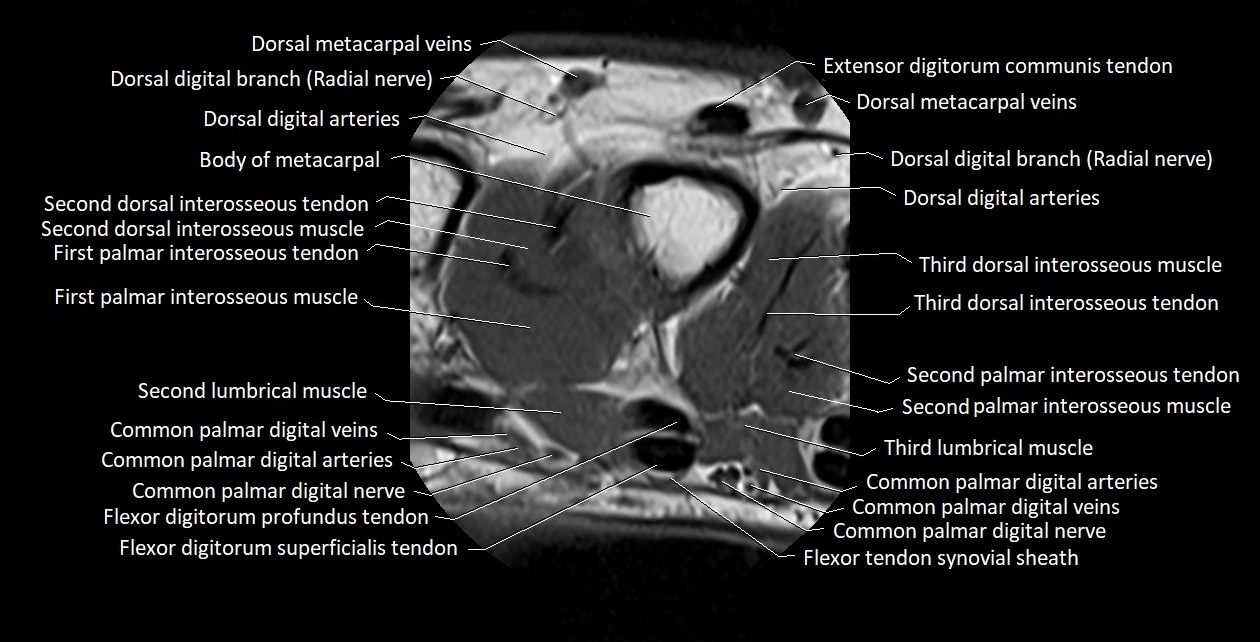
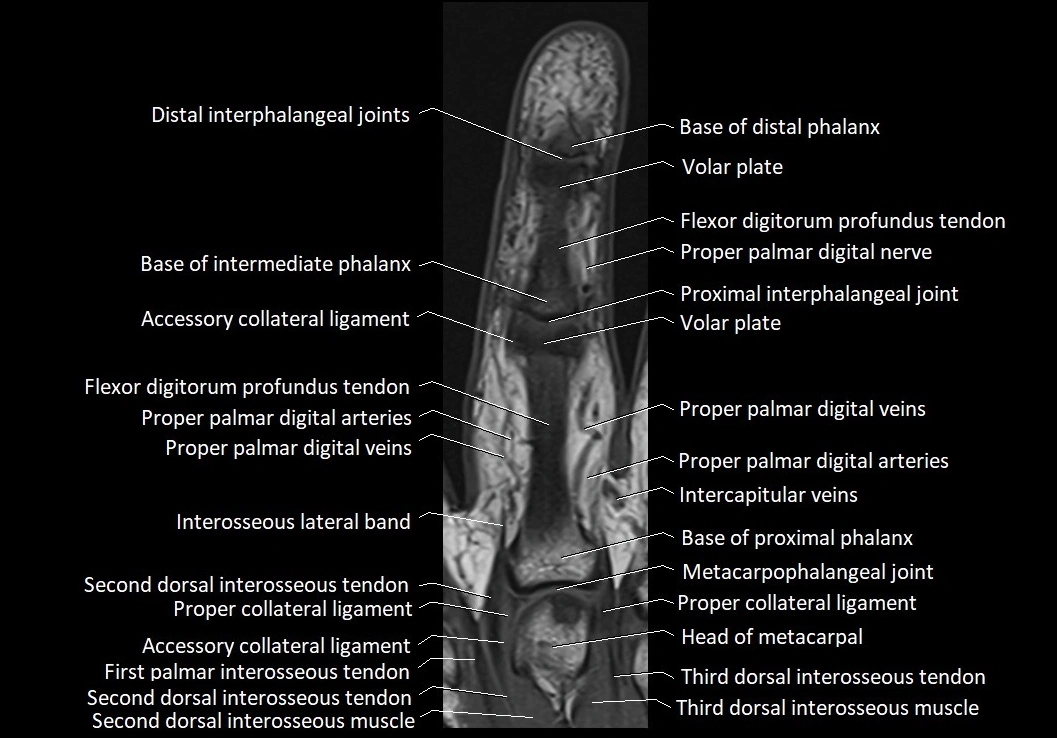
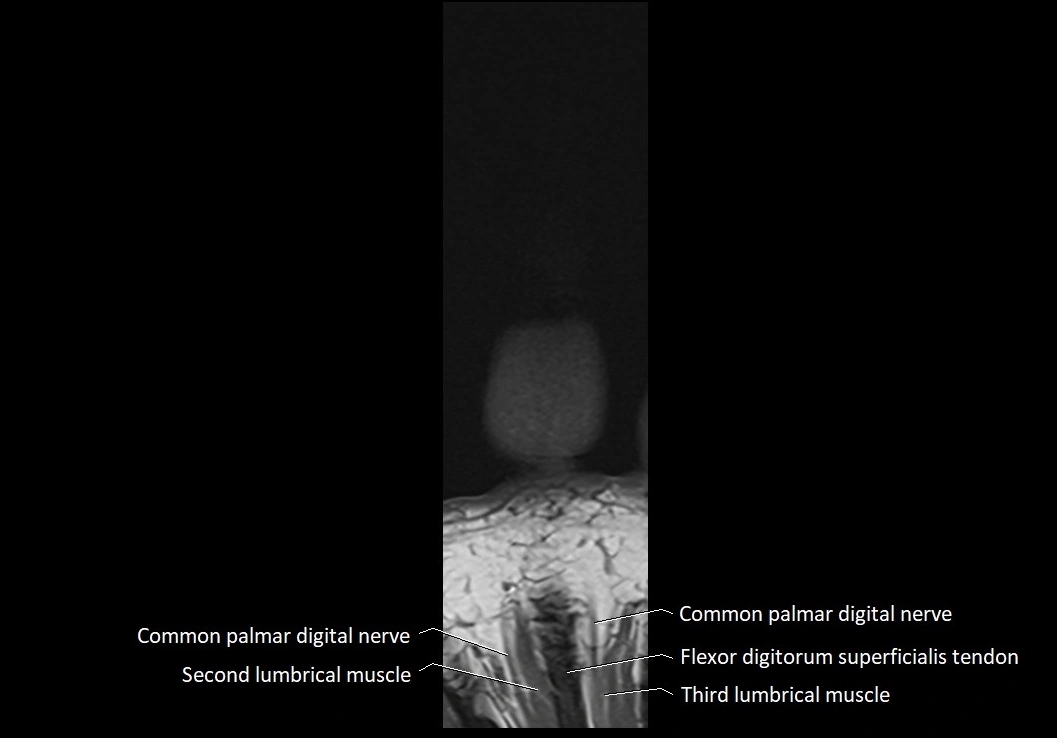
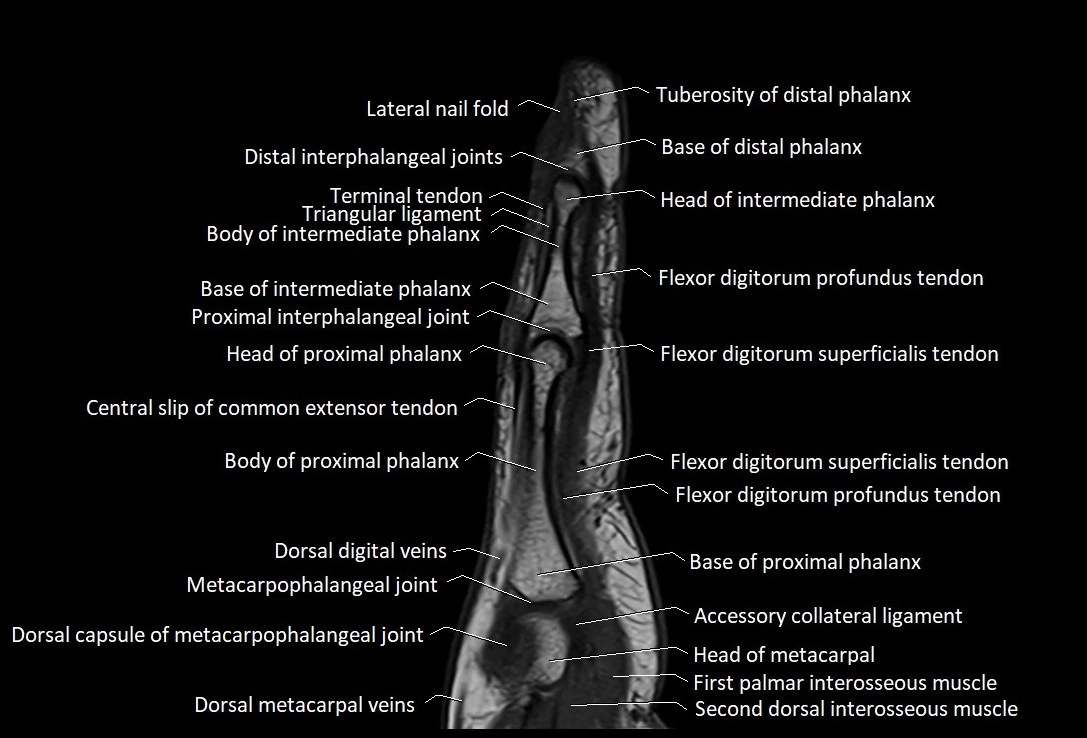
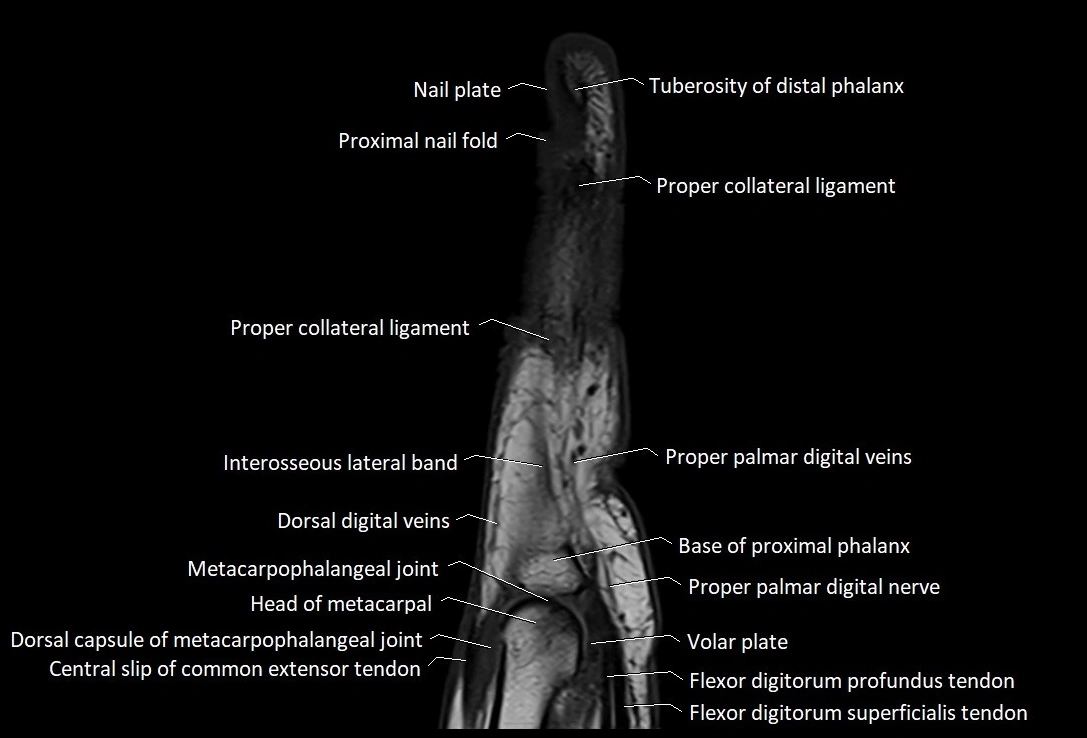
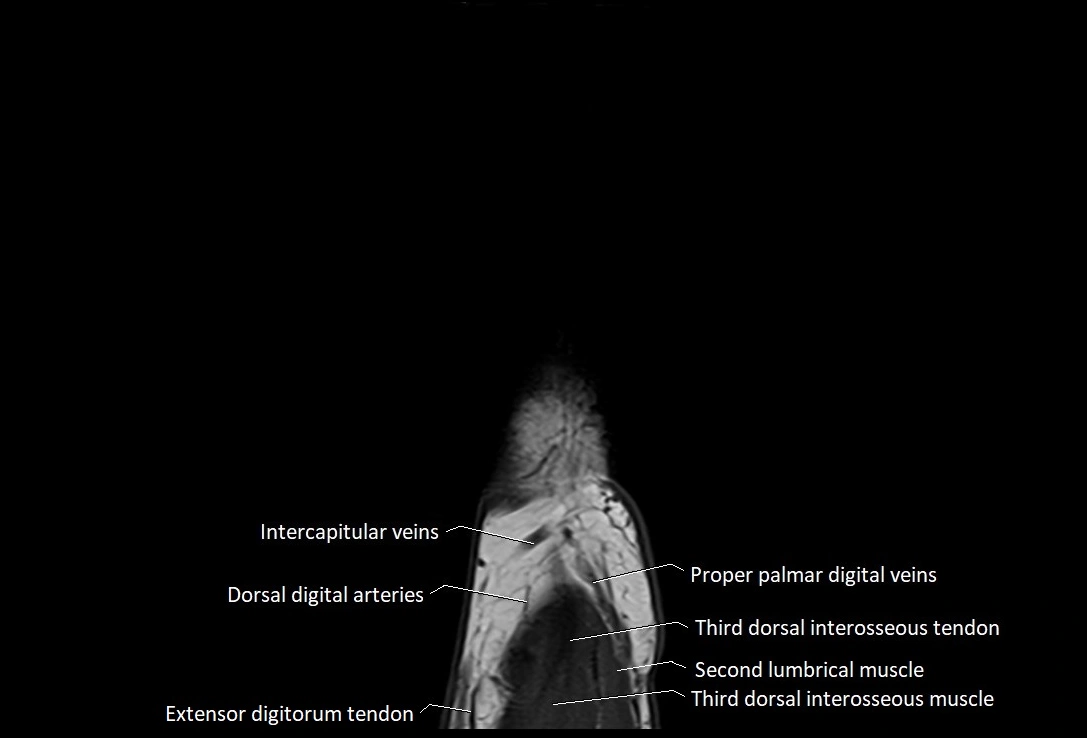
MRI images

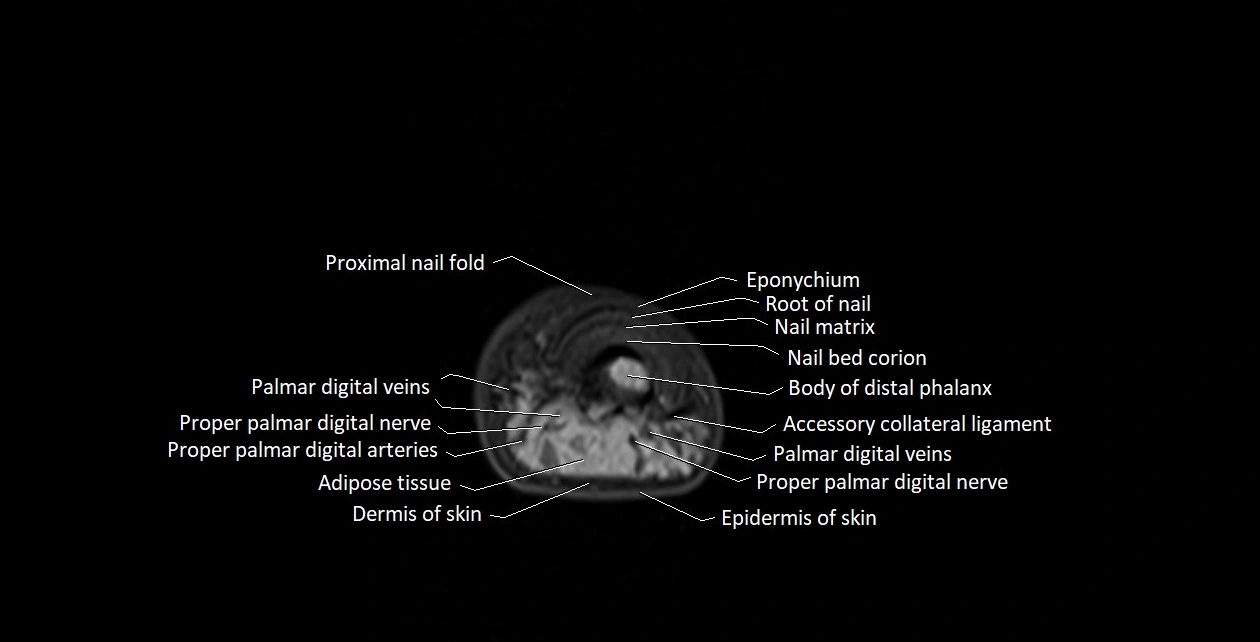
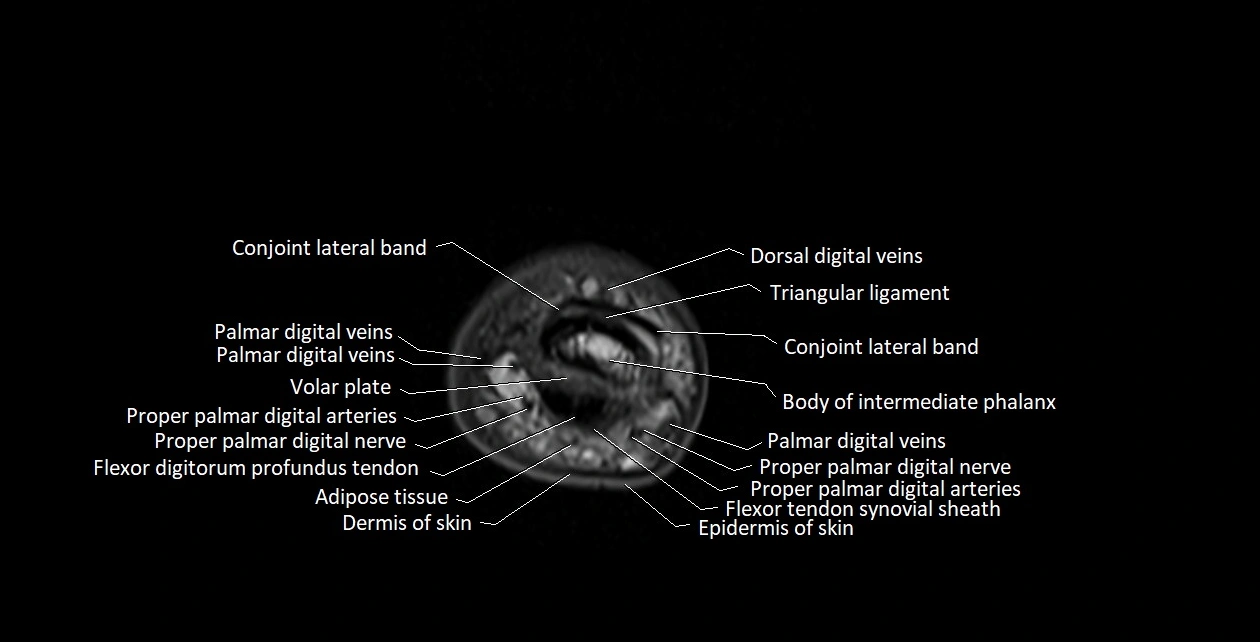
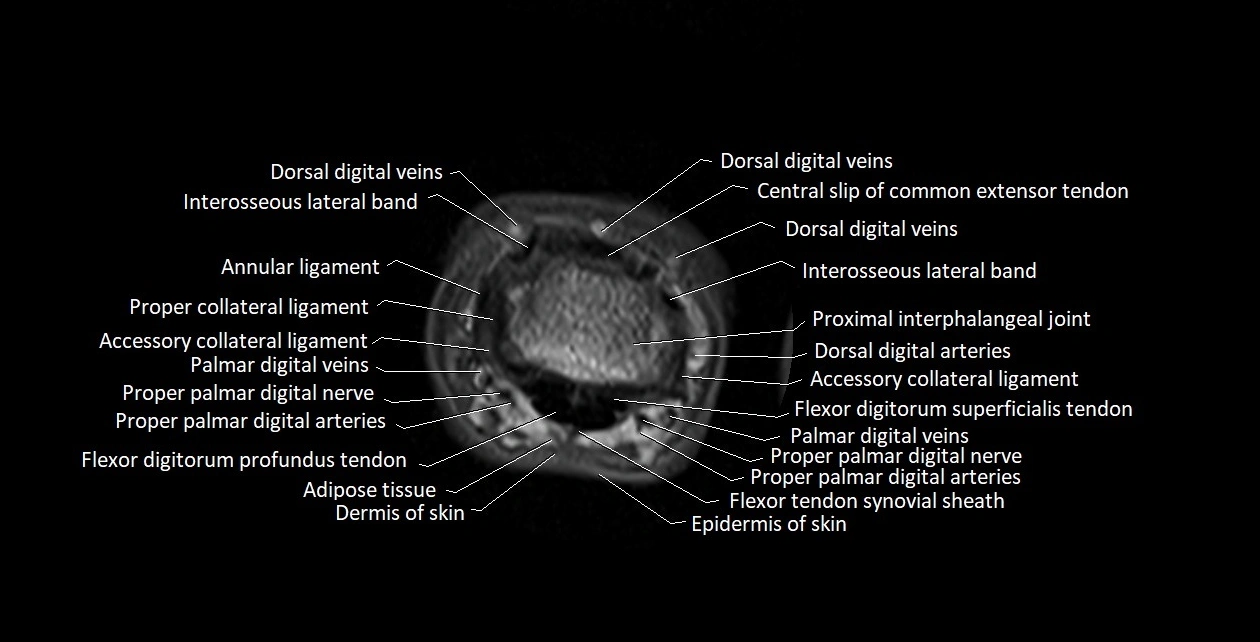
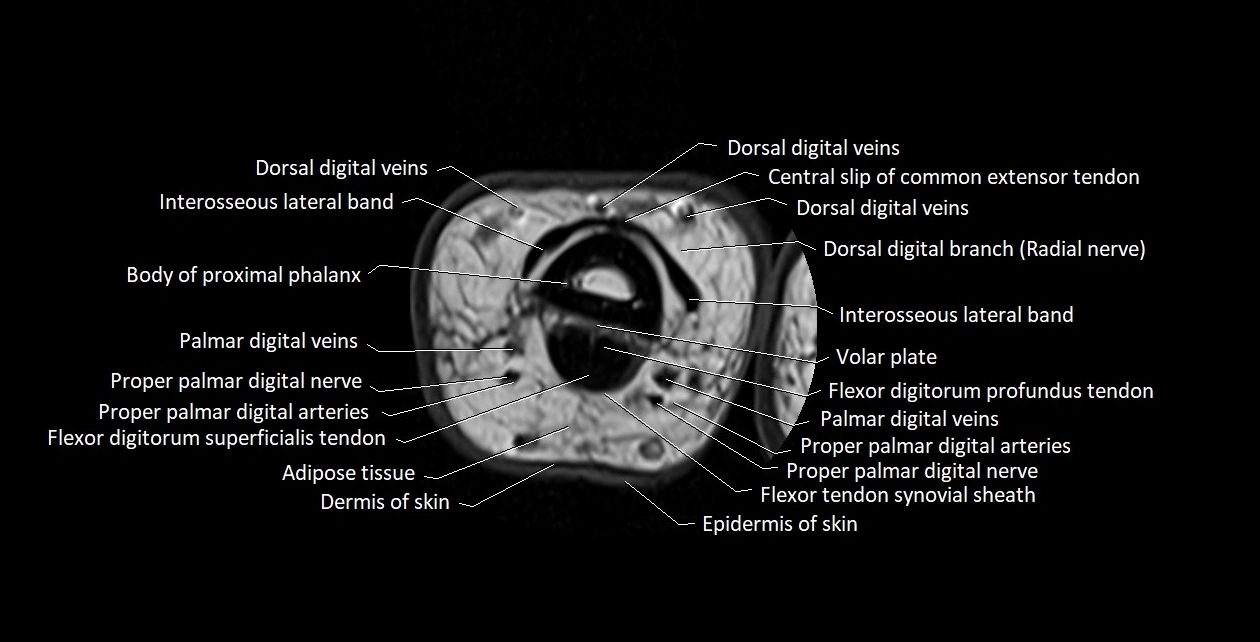
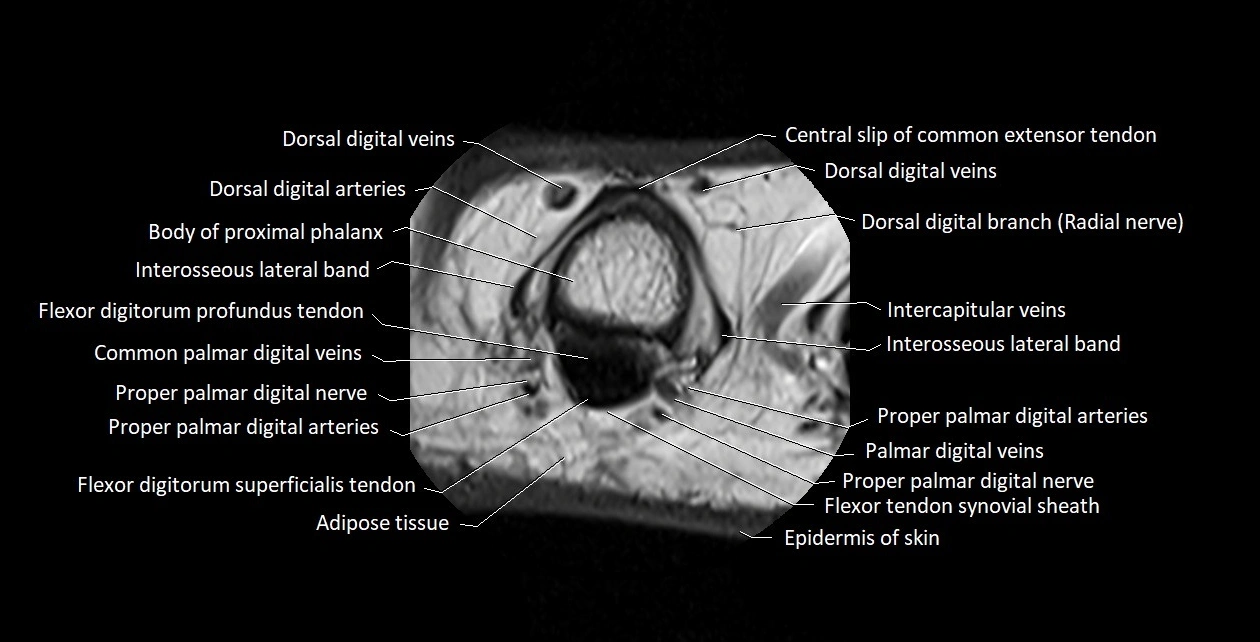
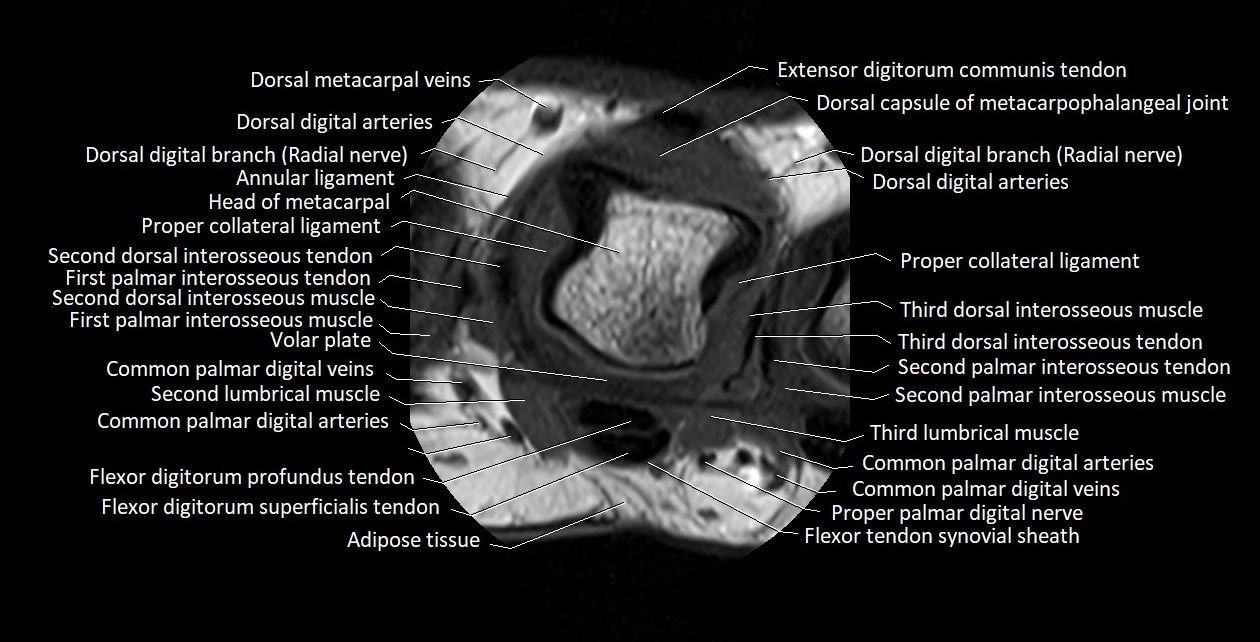
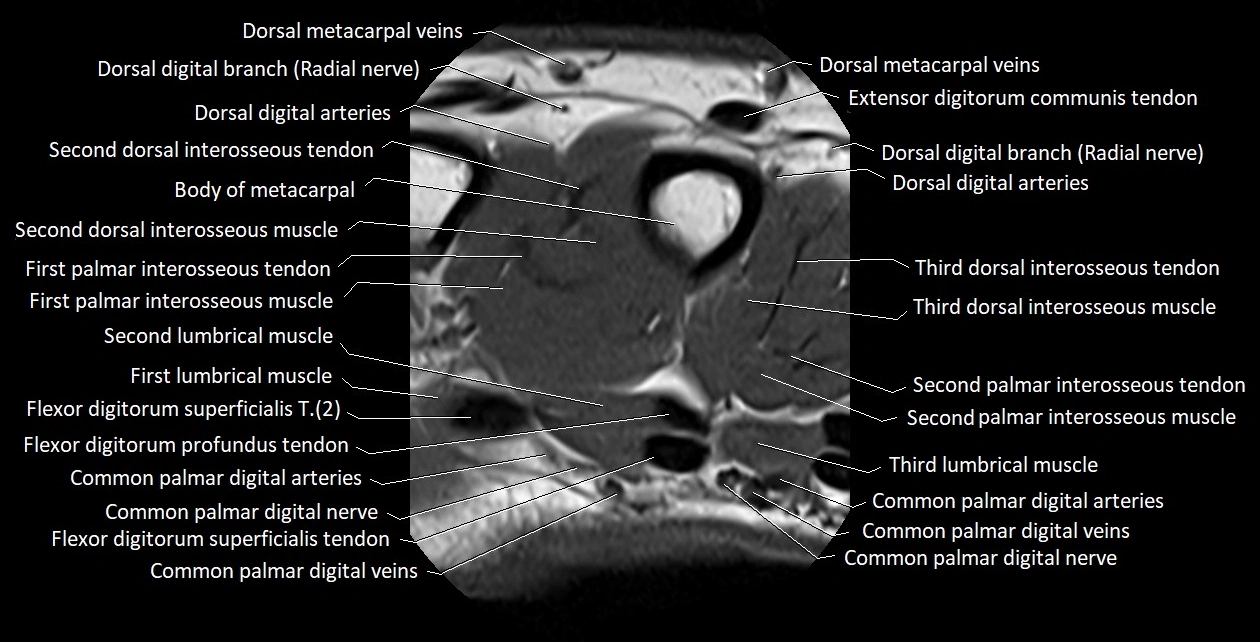
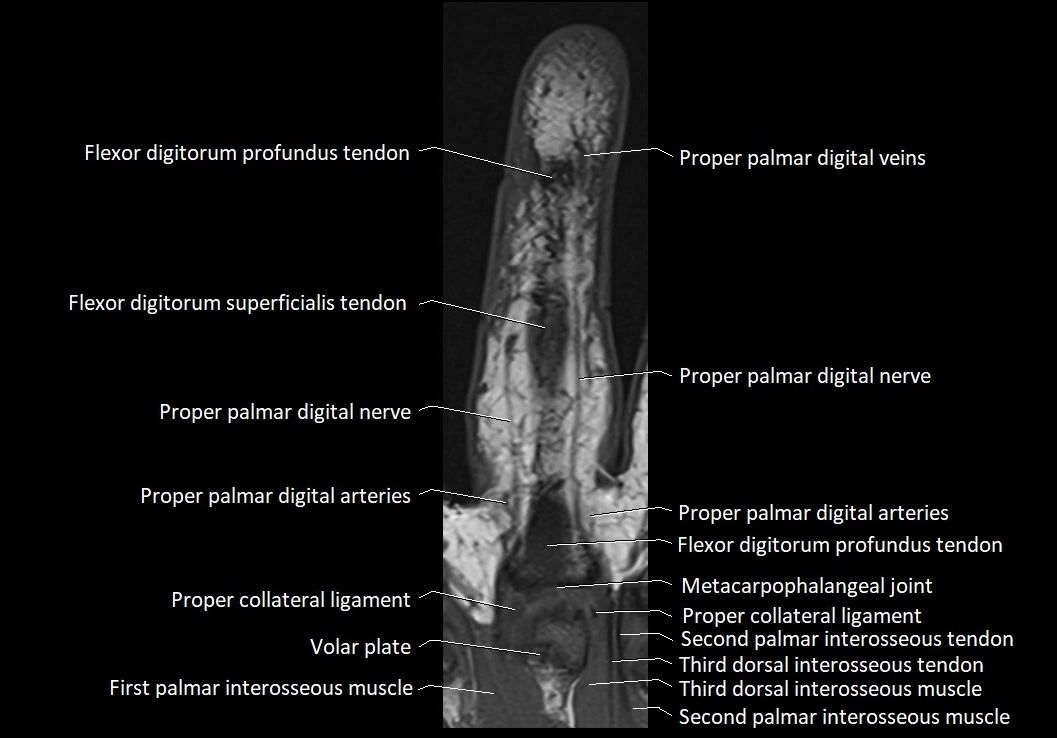
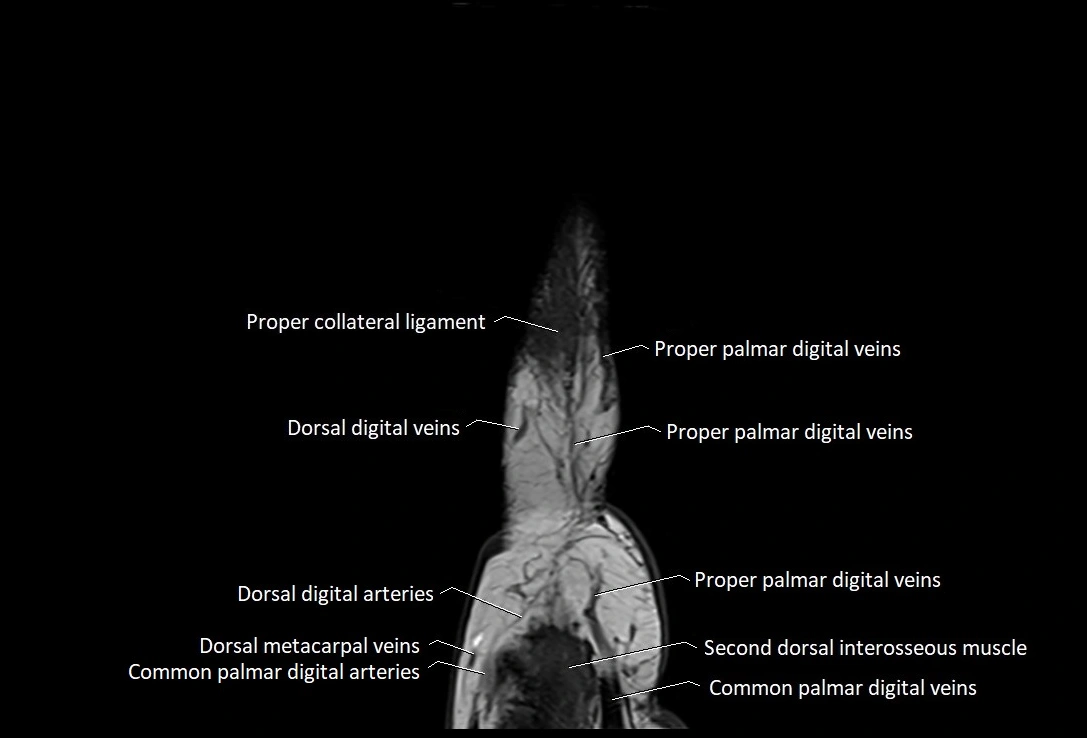
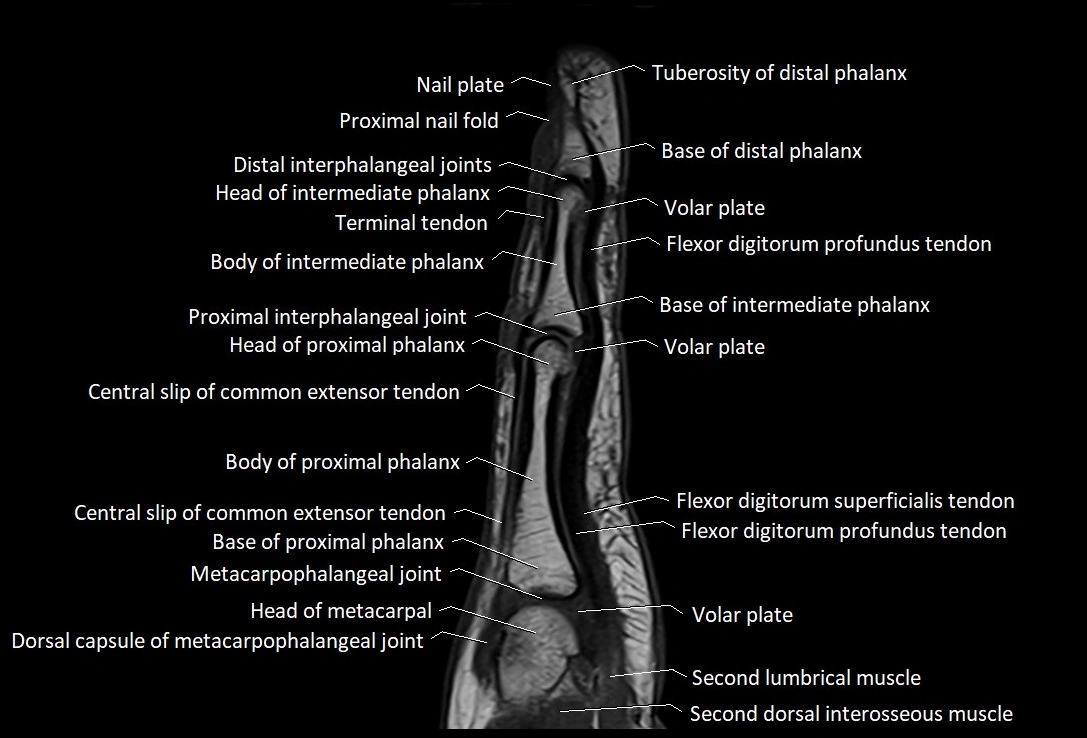
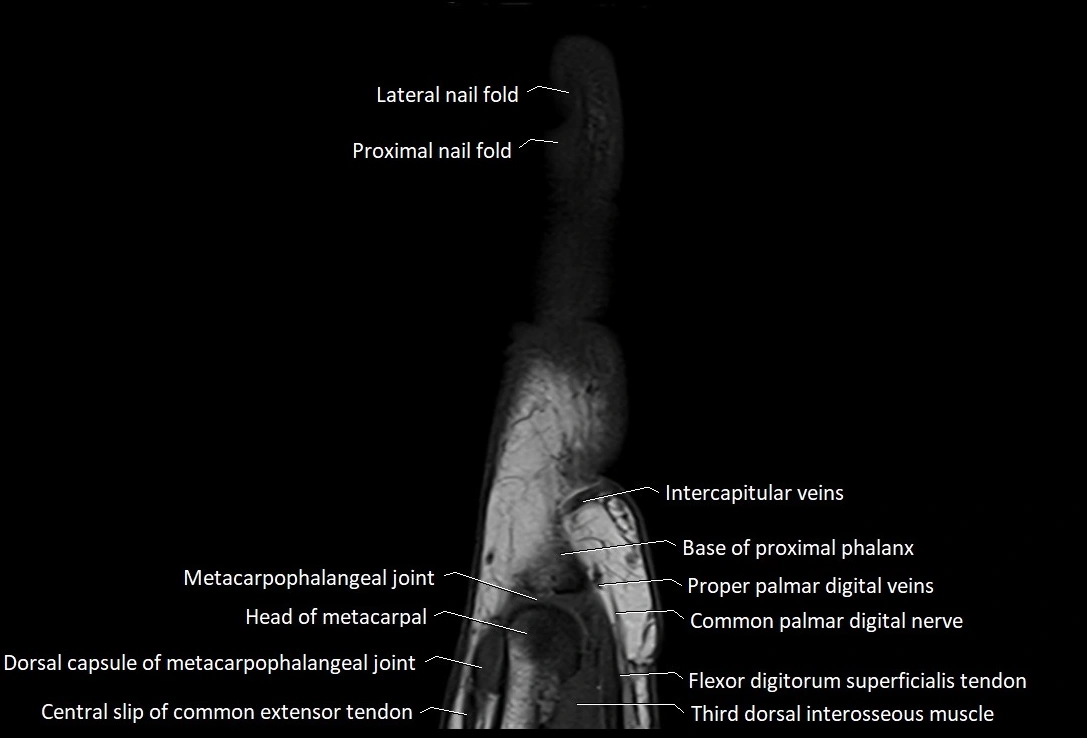
MRI images

CT images

CT images

CT images