






Topic
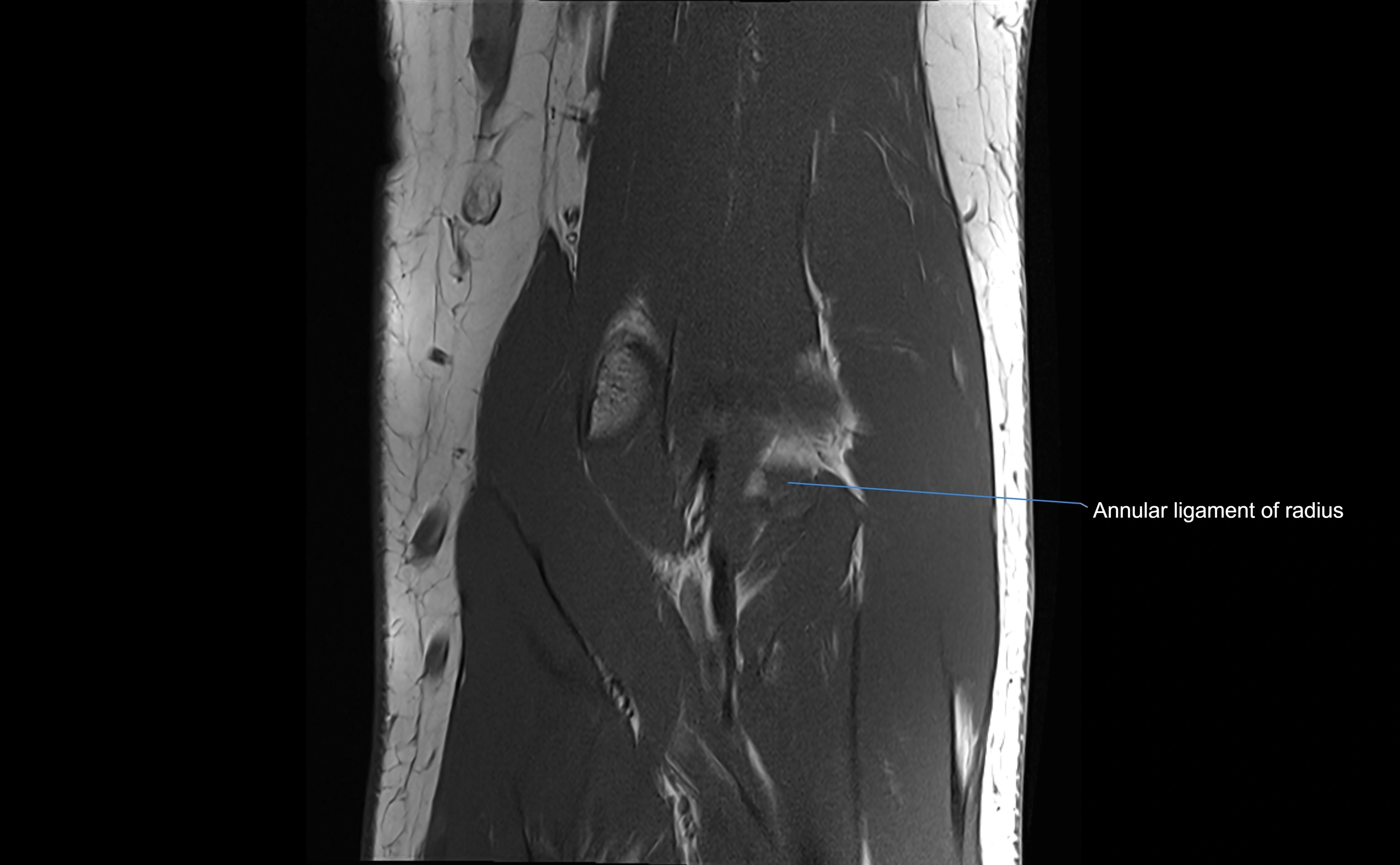
The annular ligament of the radius is a strong, circular band of fibers that encircles the head and neck of the radius, holding it securely against the radial notch of the ulna. It forms part of the proximal radioulnar joint, permitting smooth rotation of the radius during pronation and supination of the forearm.
The ligament acts like a collar or loop, maintaining radial head stability while allowing rotation. It is essential for forearm motion, elbow stability, and load transmission from the radius to the ulna and humerus.
Synonyms
-
Orbicular ligament
-
Radial head collar ligament
Origin, Course, and Insertion
-
Origin: Arises from the anterior margin of the radial notch of the ulna.
-
Course: Forms a strong circular band that wraps around the radial head and neck, maintaining them within the radial notch.
-
Insertion: Attaches to the posterior margin of the radial notch, completing a fibrous ring around the radial head.
-
The inner surface of the ligament is lined with synovial membrane, allowing frictionless rotation.
Relations
-
Superiorly: Blends with the capsule of the elbow joint.
-
Inferiorly: Supported by the quadrate ligament at the neck of the radius.
-
Medially: Attached to the ulnar radial notch.
-
Laterally: In contact with the radial head and its articular cartilage.
-
Anteriorly: Related to the radial collateral ligament of the elbow.
-
Posteriorly: Continuous with the elbow joint capsule.
Function
-
Stabilization: Holds the radial head against the ulna, forming a pivot joint.
-
Movement: Allows smooth rotation of the radius during pronation and supination.
-
Force transmission: Distributes load from the hand and wrist through the radius to the ulna and humerus.
-
Joint integrity: Prevents anterior and posterior displacement of the radial head.
Clinical Significance
-
Nursemaid’s elbow (radial head subluxation): Common in children when the radial head slips out from the annular ligament due to traction injury.
-
Ligament laxity or tear: May cause instability of the proximal radioulnar joint.
-
Traumatic dislocation: May occur with elbow fractures or high-energy rotational injuries.
-
Inflammation or synovitis: Can cause restricted forearm motion and pain.
-
Post-surgical importance: Crucial for restoring forearm stability in reconstructive procedures.
MRI Appearance
T1-weighted images:
-
Ligament: low signal intensity (dark), appearing as a continuous band around the radial head.
-
Adjacent fat and marrow: bright, creating contrast with the ligament.
-
Thickening or disruption indicates injury or fibrosis.
-
Joint capsule and synovium seen as thin low-signal lines contiguous with ligament margins.
T2-weighted images:
-
Ligament: low signal (dark) with clear delineation from joint fluid.
-
Fluid or edema: bright hyperintense, separating or surrounding the ligament in partial tears.
-
Complete tear: discontinuity or non-visualization of ligament fibers, often with joint effusion.
STIR:
-
Normal ligament: dark band encircling radial head.
-
Pathology: bright hyperintense periligamentous signal suggesting edema, sprain, or partial tear.
Proton Density Fat-Saturated (PD FS):
-
Normal: dark, well-defined band outlining the radial head.
-
Partial tear: irregular or bright hyperintense signal within or adjacent to ligament fibers.
-
Joint effusion and reactive synovitis appear bright and are well visualized.
T1 Fat-Sat Post-Contrast:
-
Normal: minimal enhancement.
-
Inflamed or injured ligament: focal or diffuse enhancement.
-
Synovial enhancement in chronic instability or post-surgical changes.
MRI Arthrogram Appearance
-
Contrast outlines the proximal radioulnar joint and radial head recess.
-
Normal ligament appears as a dark ring surrounding the radial head, containing the injected contrast within the joint cavity.
-
Partial tear: contrast extends along the ligament or beneath its fibers.
-
Complete tear or subluxation: contrast extravasates around the radial head or ulna, indicating discontinuity.
-
Detects capsular defects, instability, or synovial invagination with high sensitivity.
CT Appearance
Non-Contrast CT:
-
Ligament not directly visualized due to soft-tissue density but may be inferred by the radial head’s containment in the notch.
-
Bony margins of the radial notch and radial head appear smooth and congruent in normal anatomy.
-
Avulsion injuries: subtle cortical irregularity or small bone fragments at ulnar attachment.
-
Chronic cases: periarticular calcifications or ossification along ligament attachment.
Post-Contrast CT (standard):
-
Highlights synovium and periligamentous soft tissue.
-
Enhancing tissue around ligament may indicate capsulitis, synovitis, or post-traumatic inflammation.
-
Assesses associated fractures and bone healing after surgical repair.
CT Arthrogram Appearance
-
Contrast fills the proximal radioulnar joint and outlines the radial head.
-
Normal annular ligament: appears as a smooth, thin ring confining contrast to the joint space.
-
Partial tear: contrast seeps beneath ligament or into adjacent soft tissues.
-
Complete tear or dislocation: contrast extravasates around the radial neck or ulnar radial notch.
-
Highly effective for evaluating joint congruency, ligament integrity, and subluxation when MRI is unavailable or contraindicated.
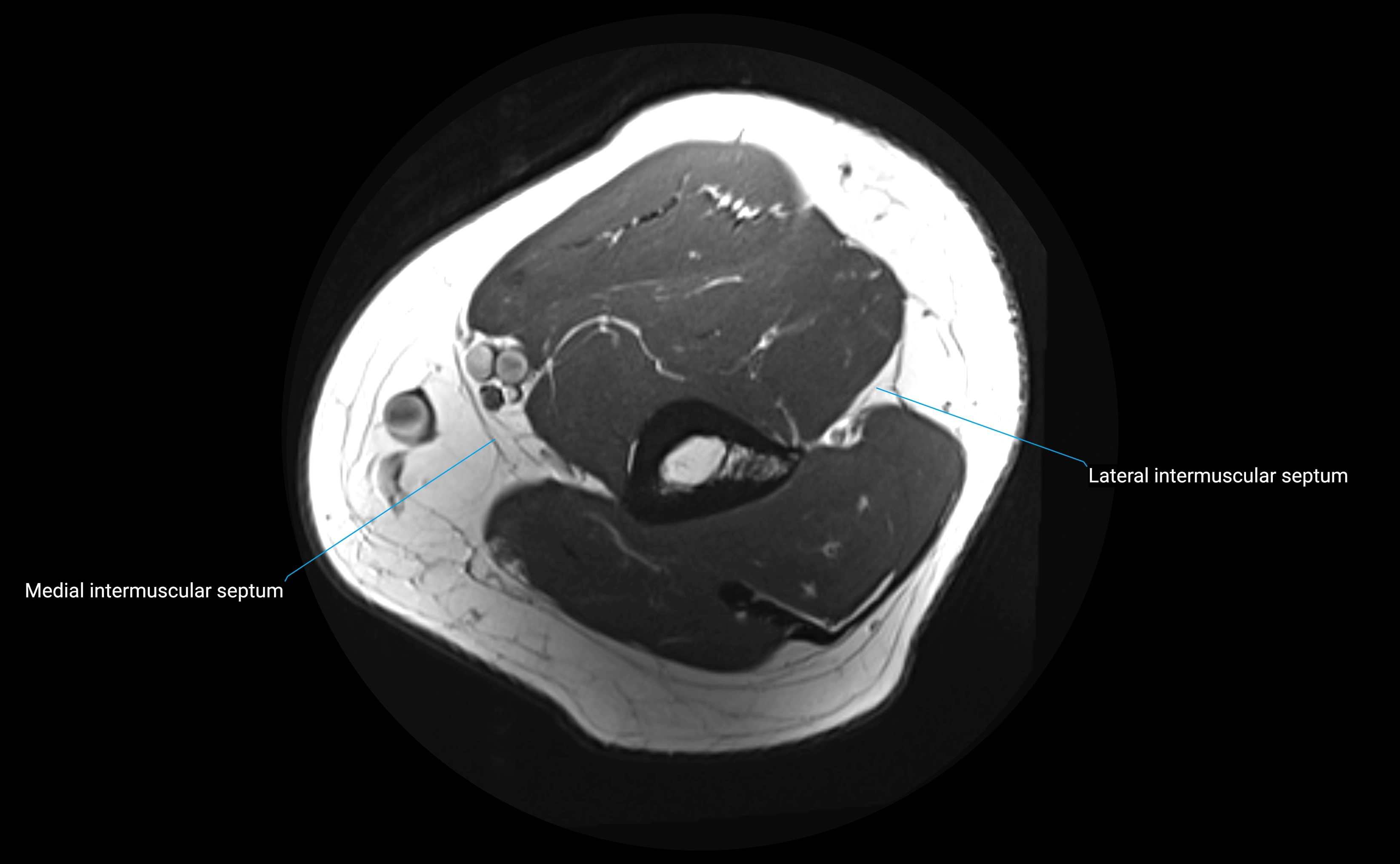
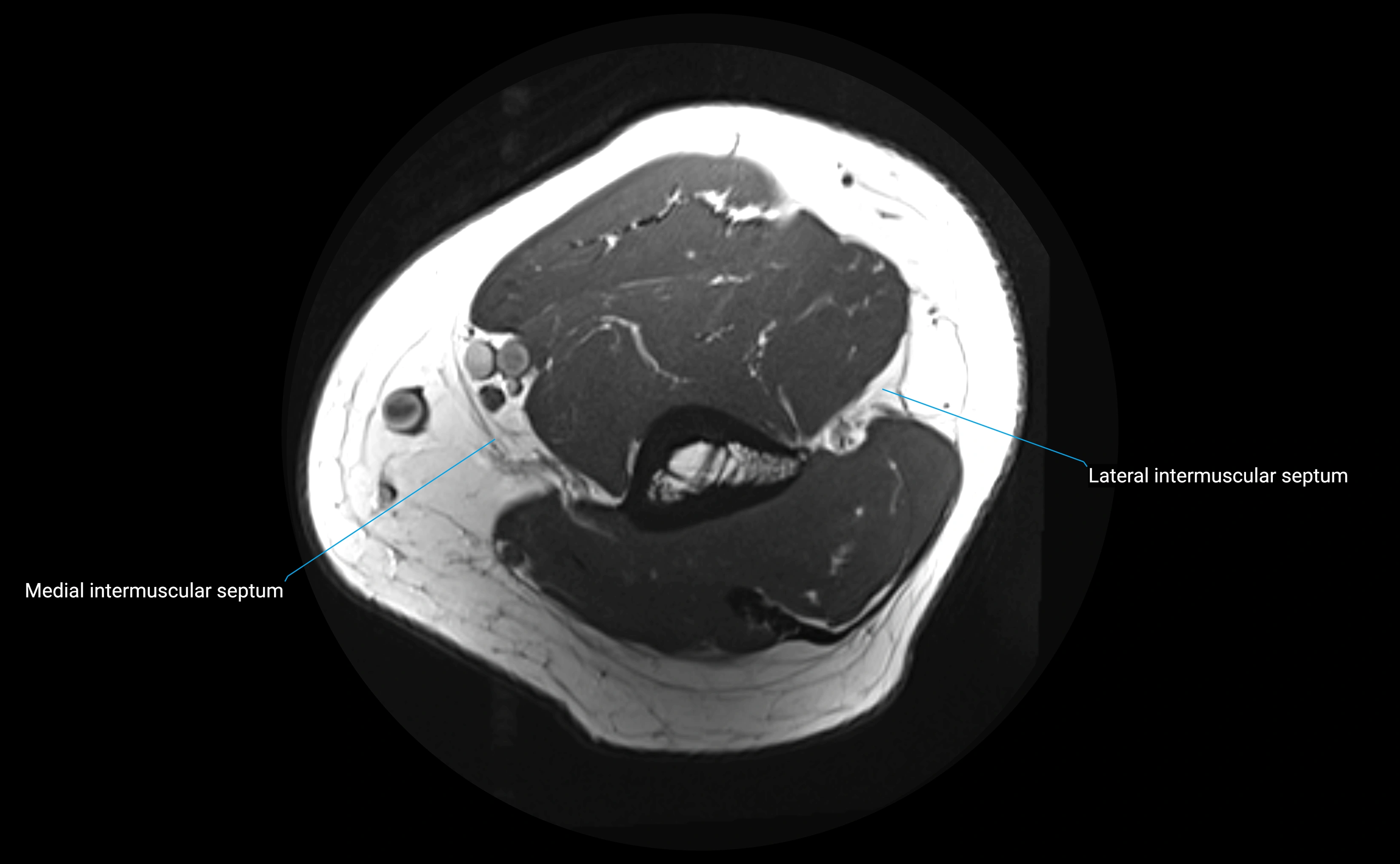
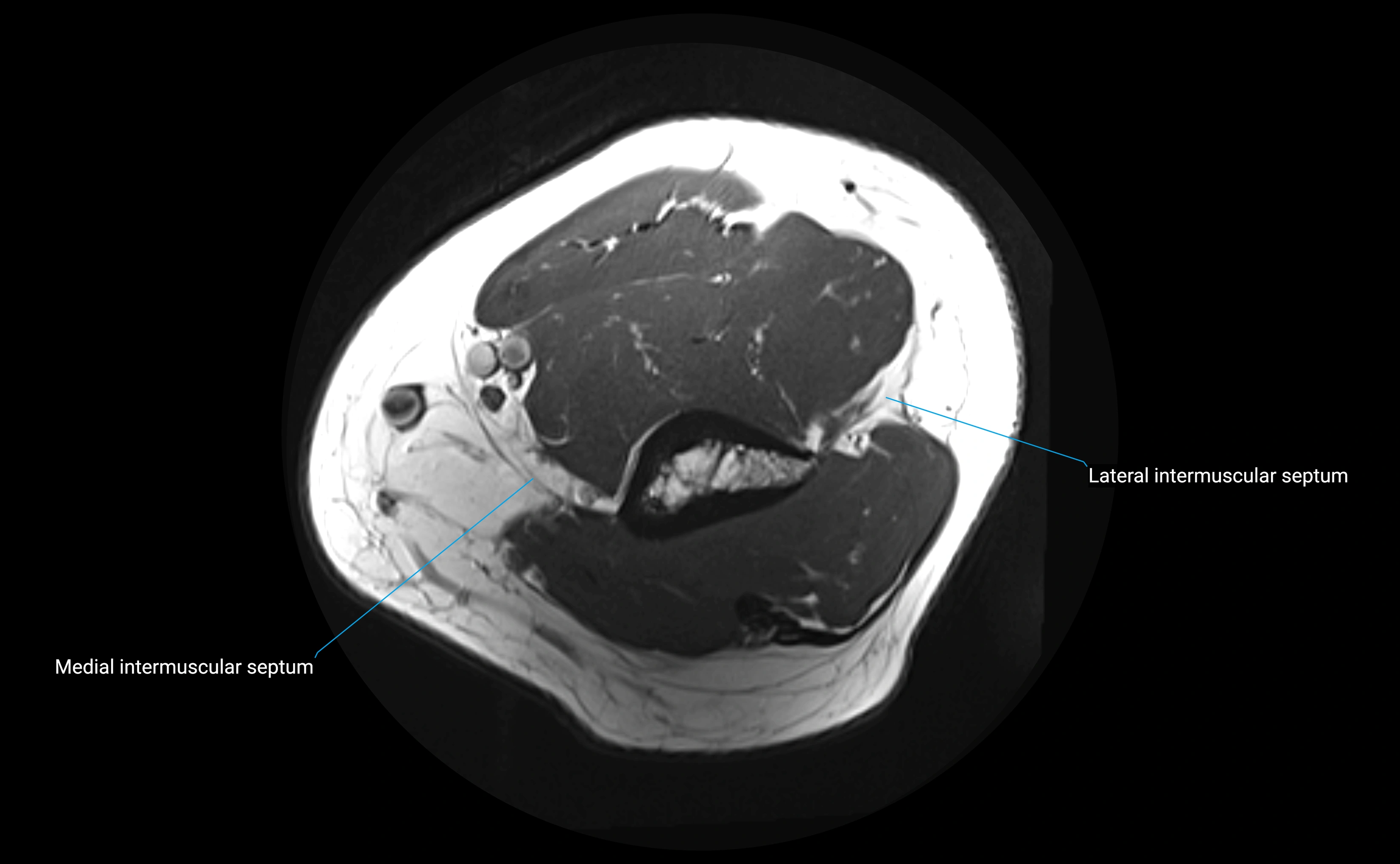
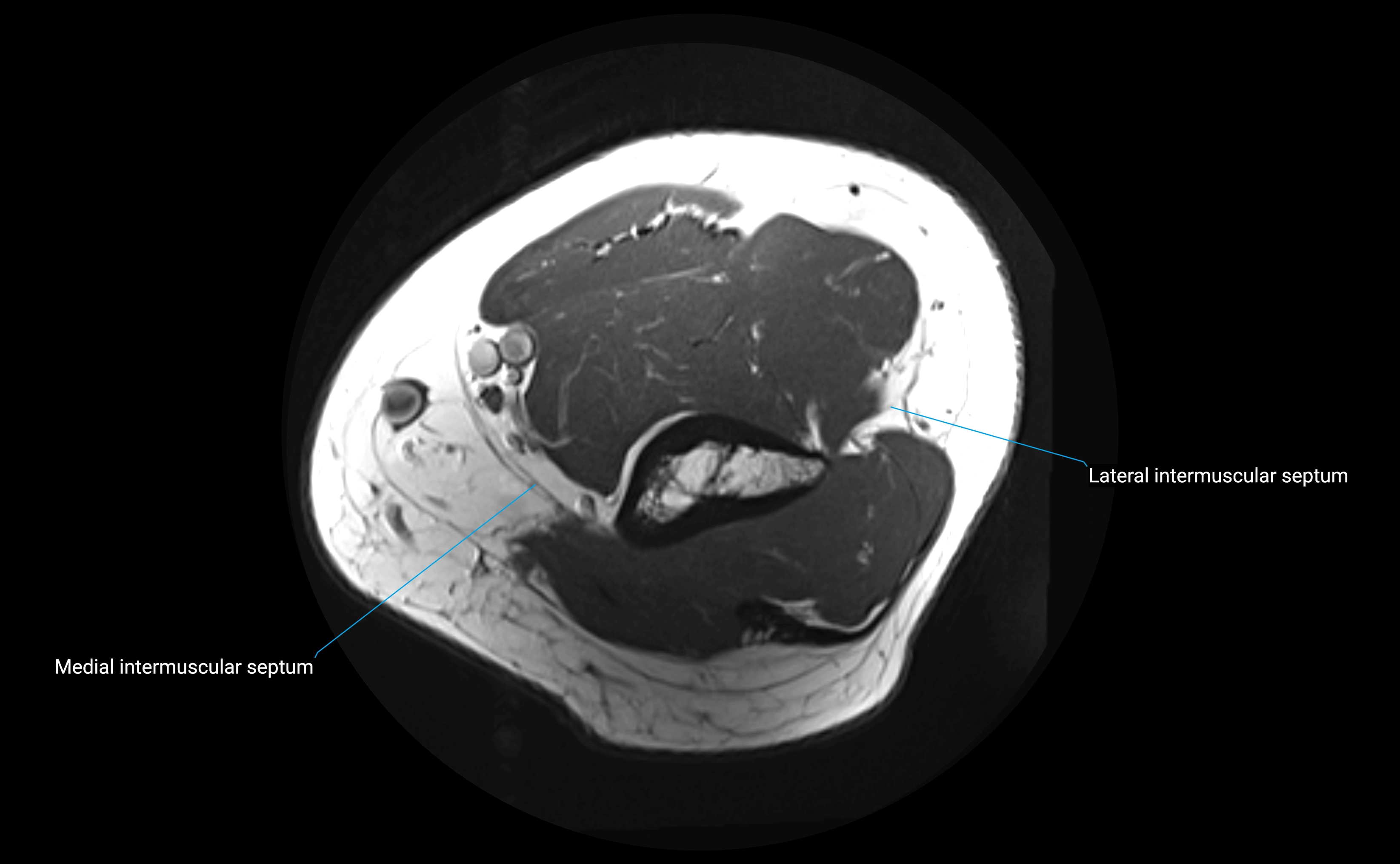
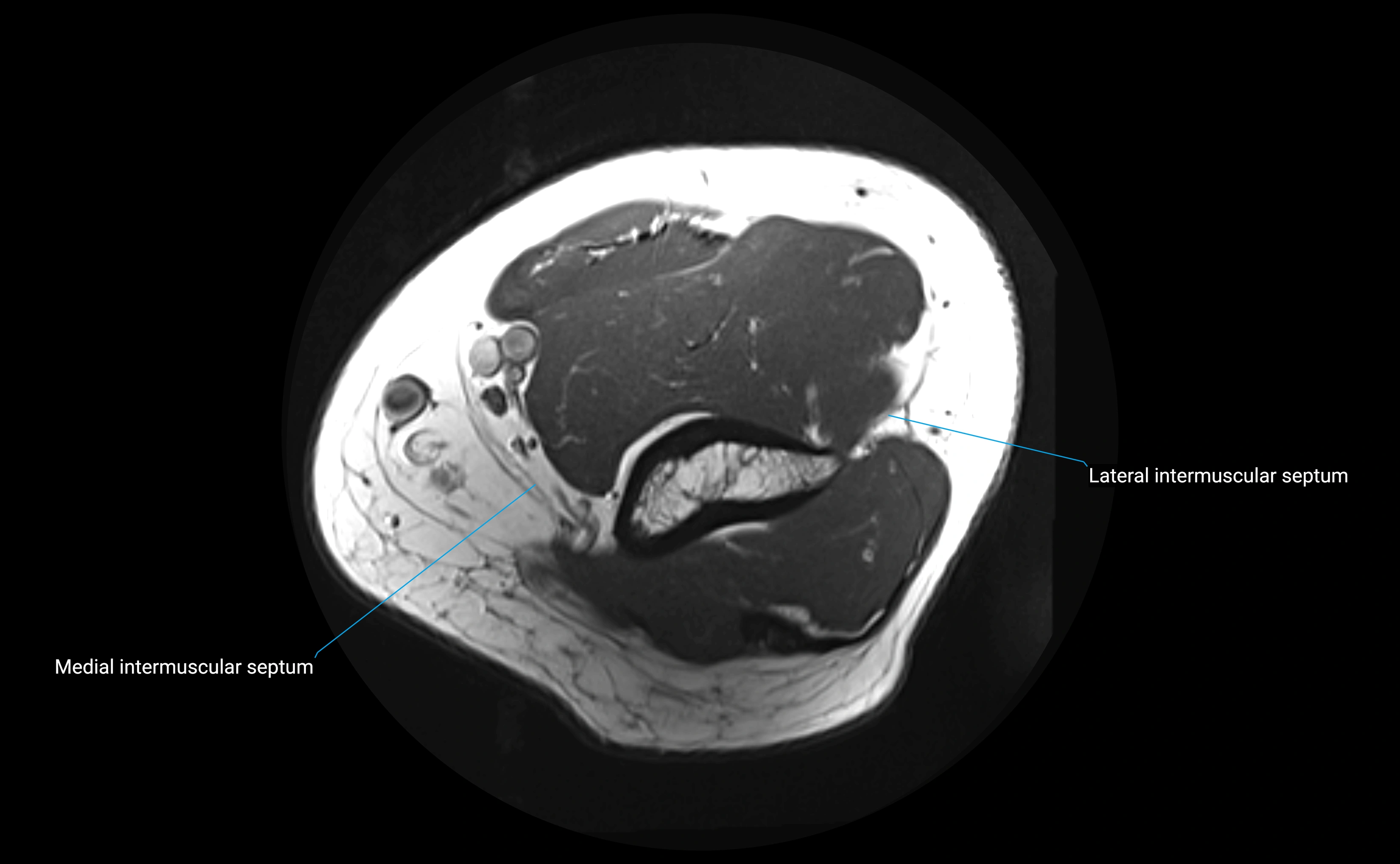
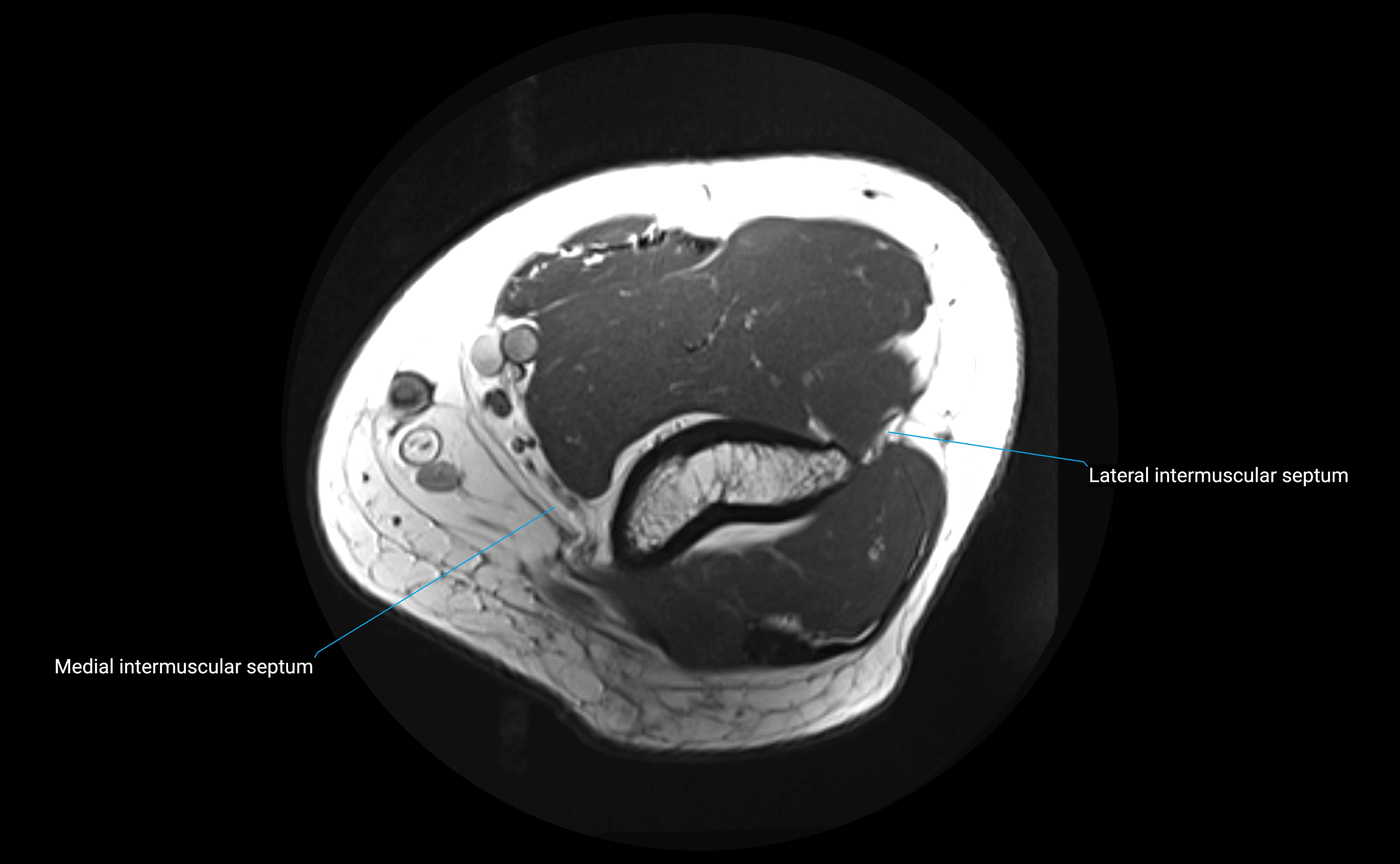
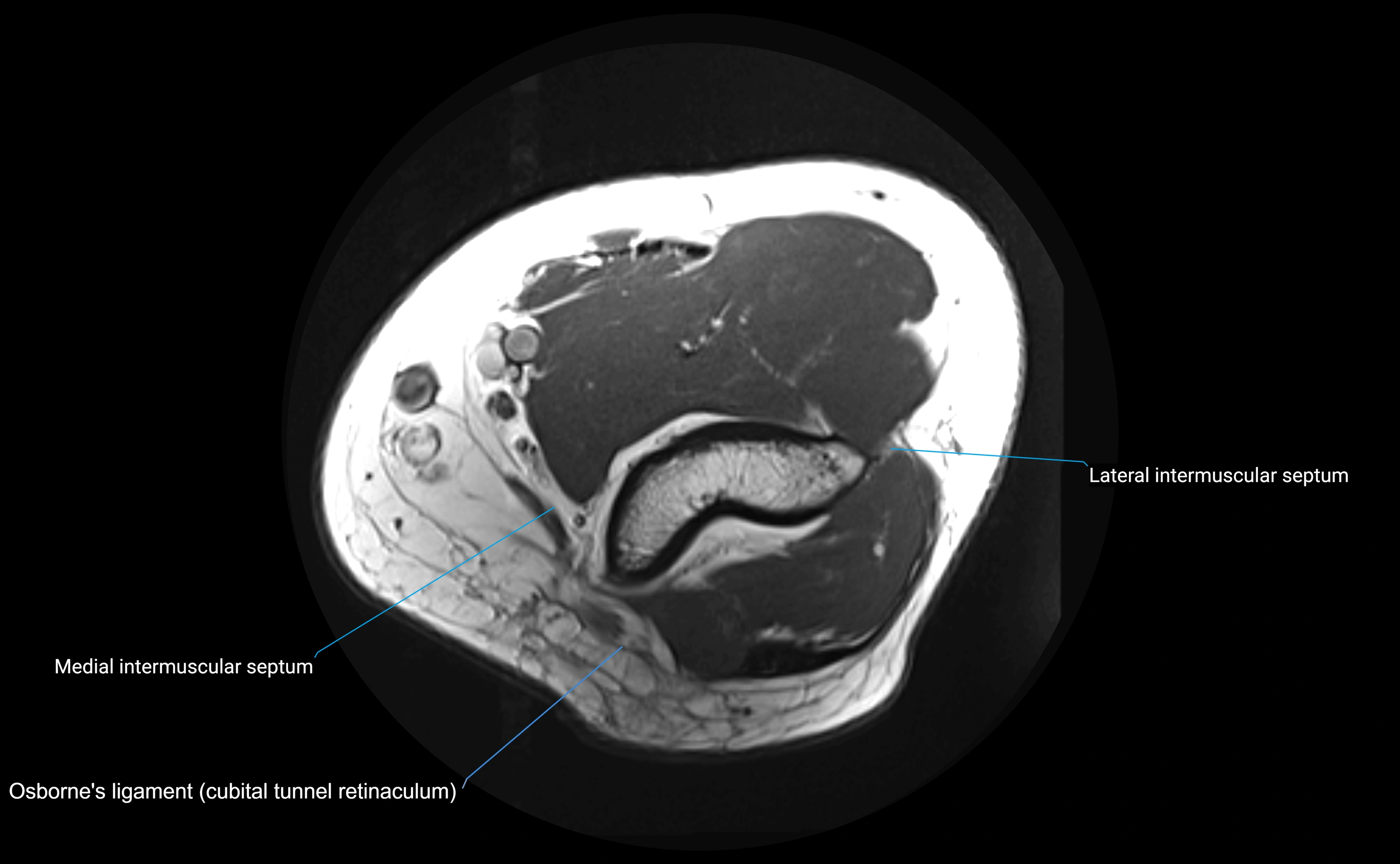
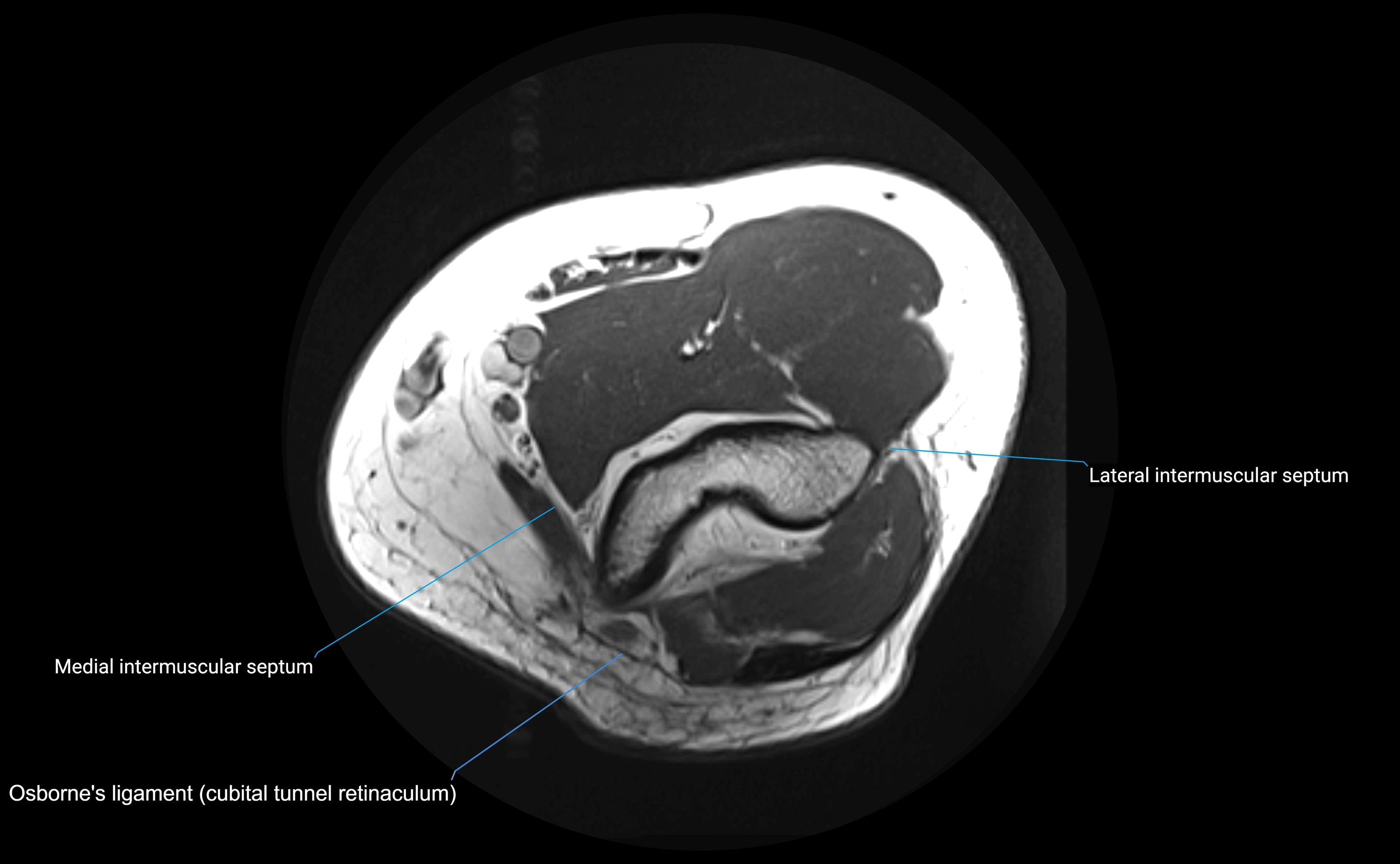
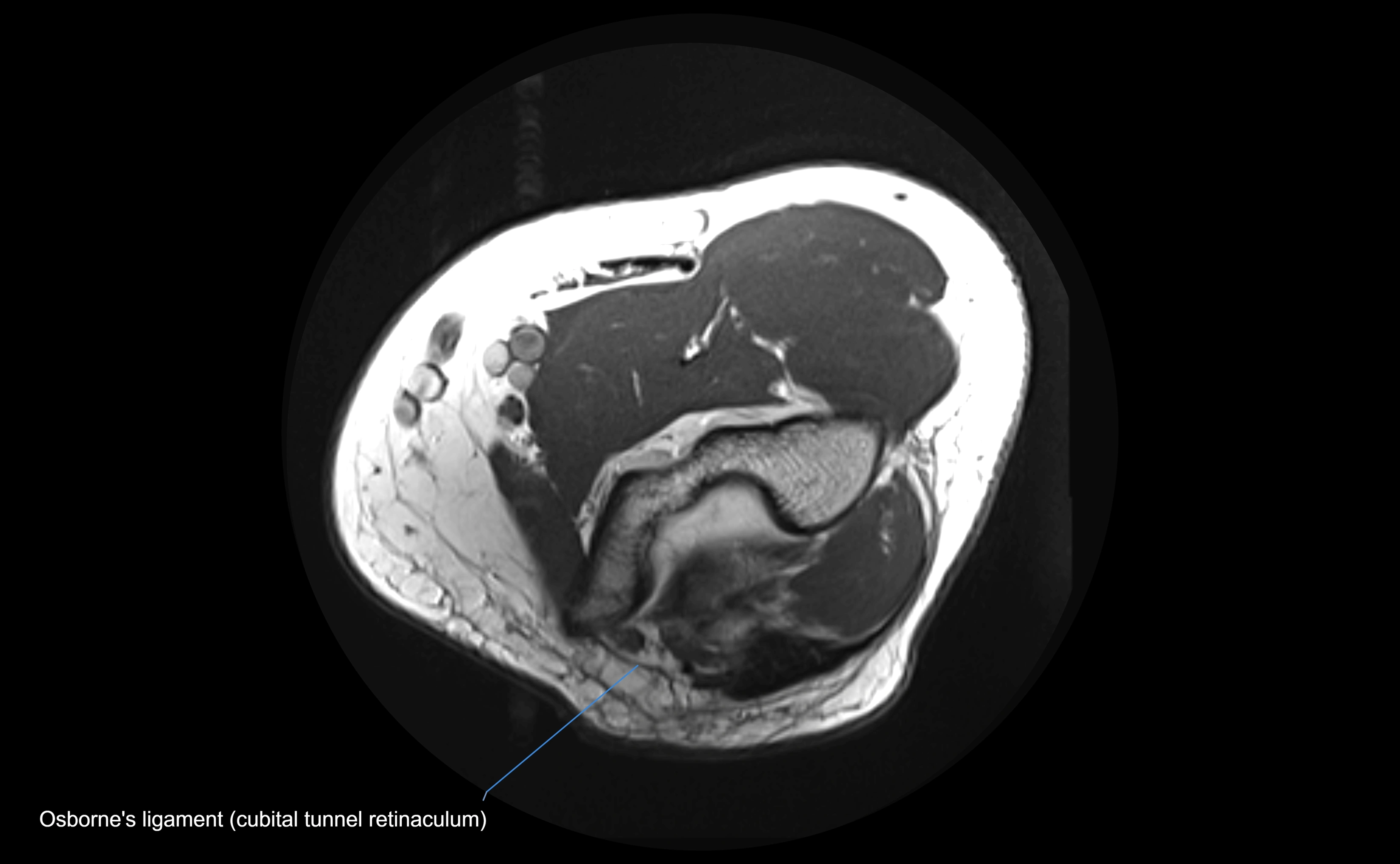
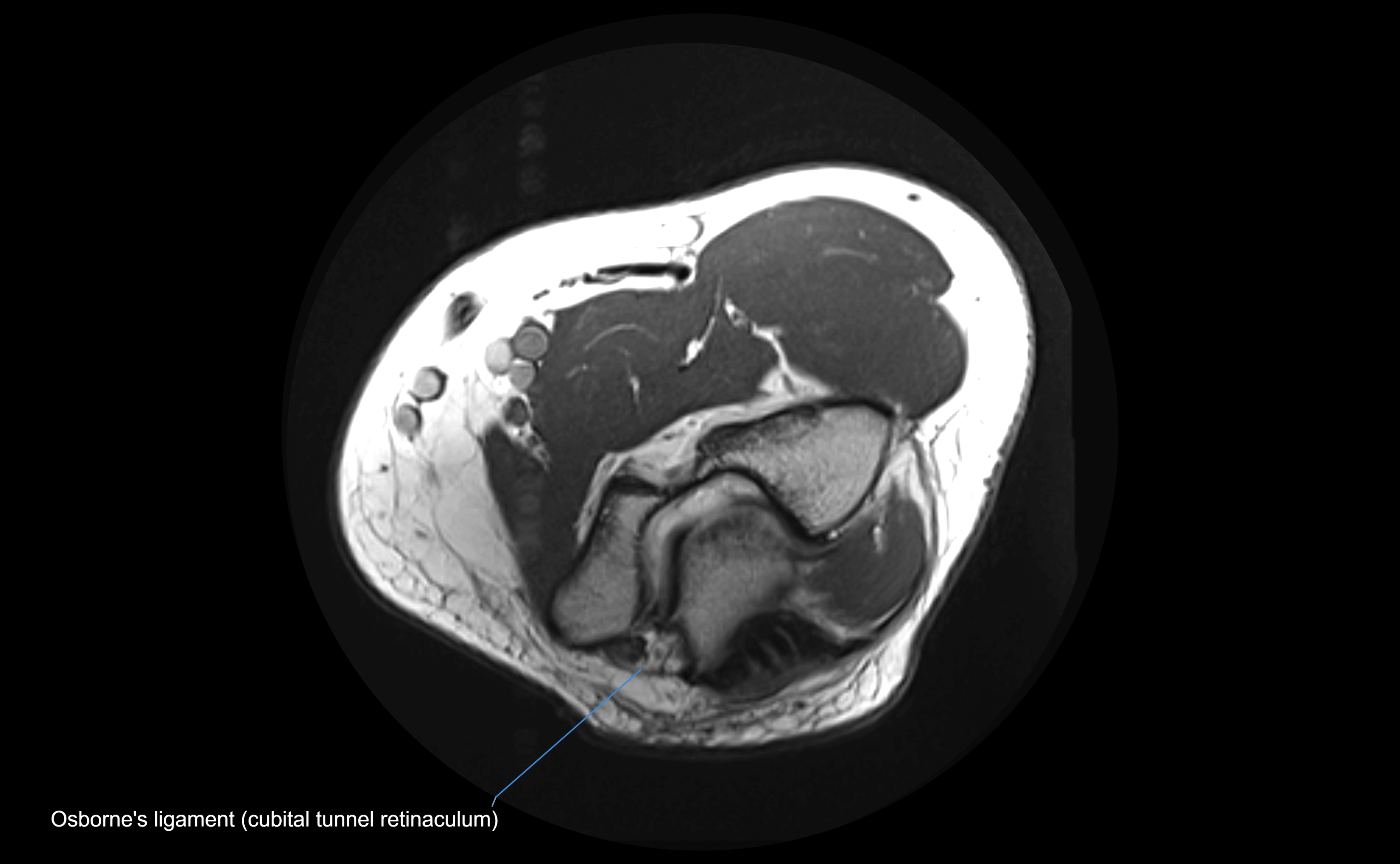
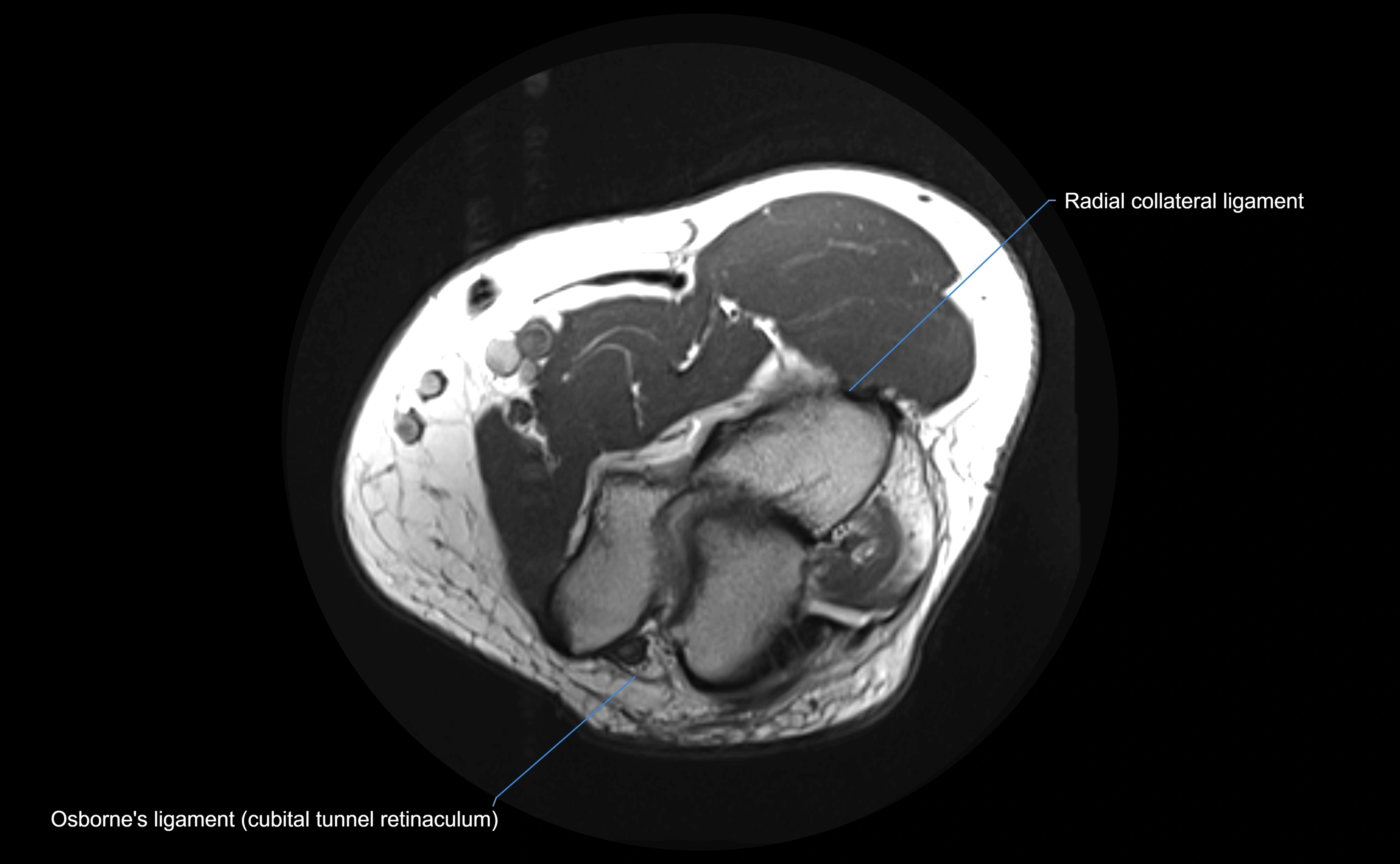
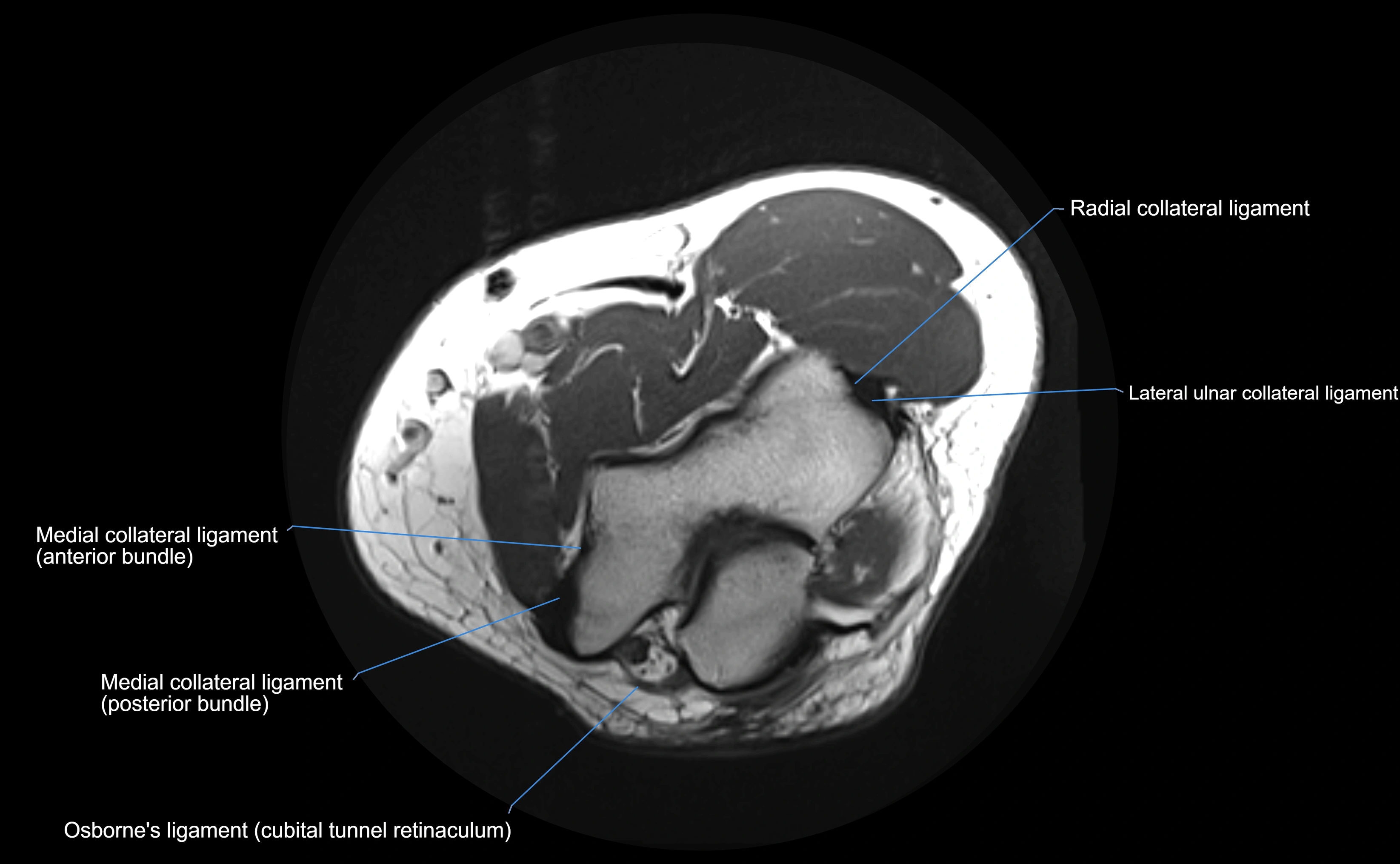
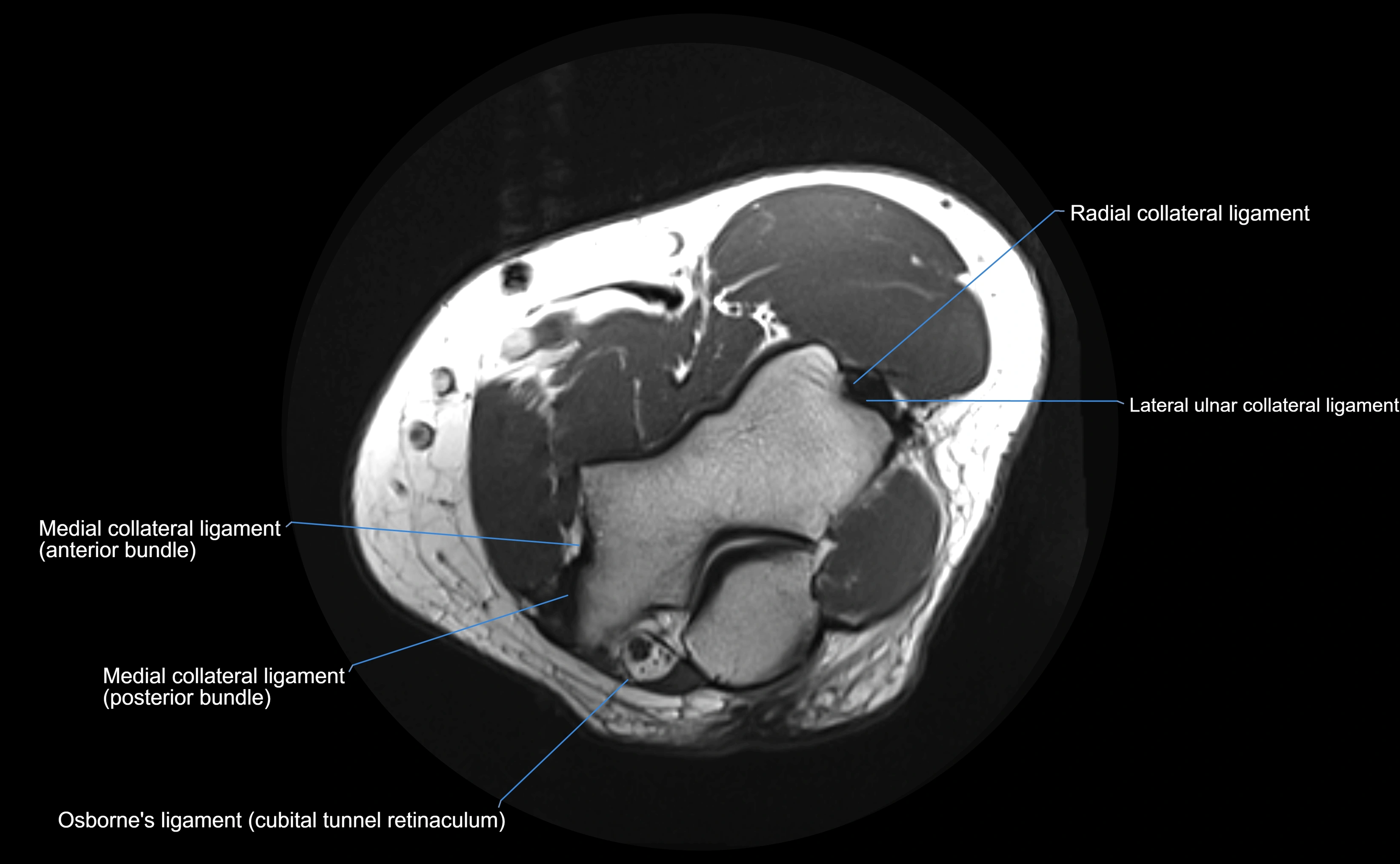
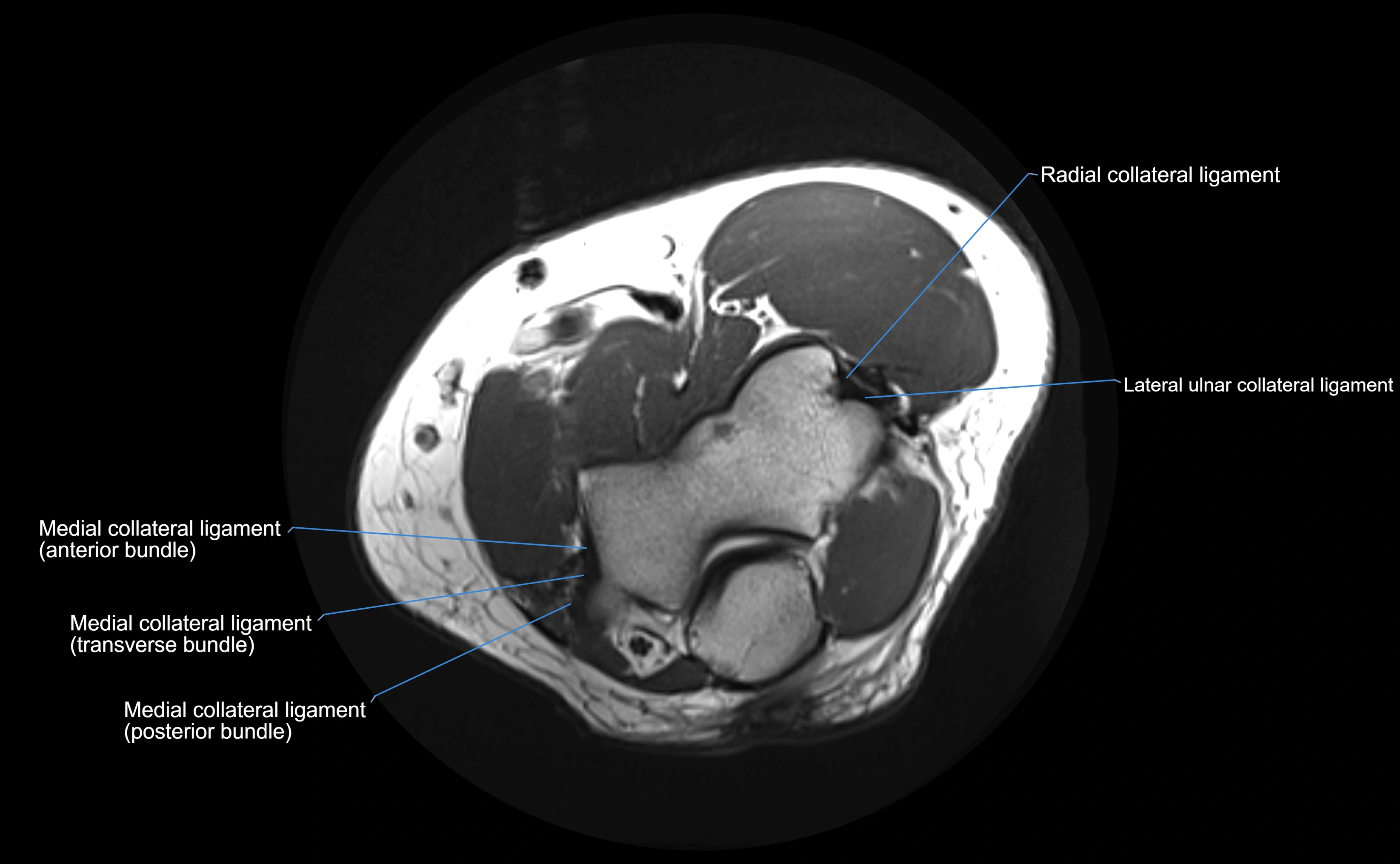
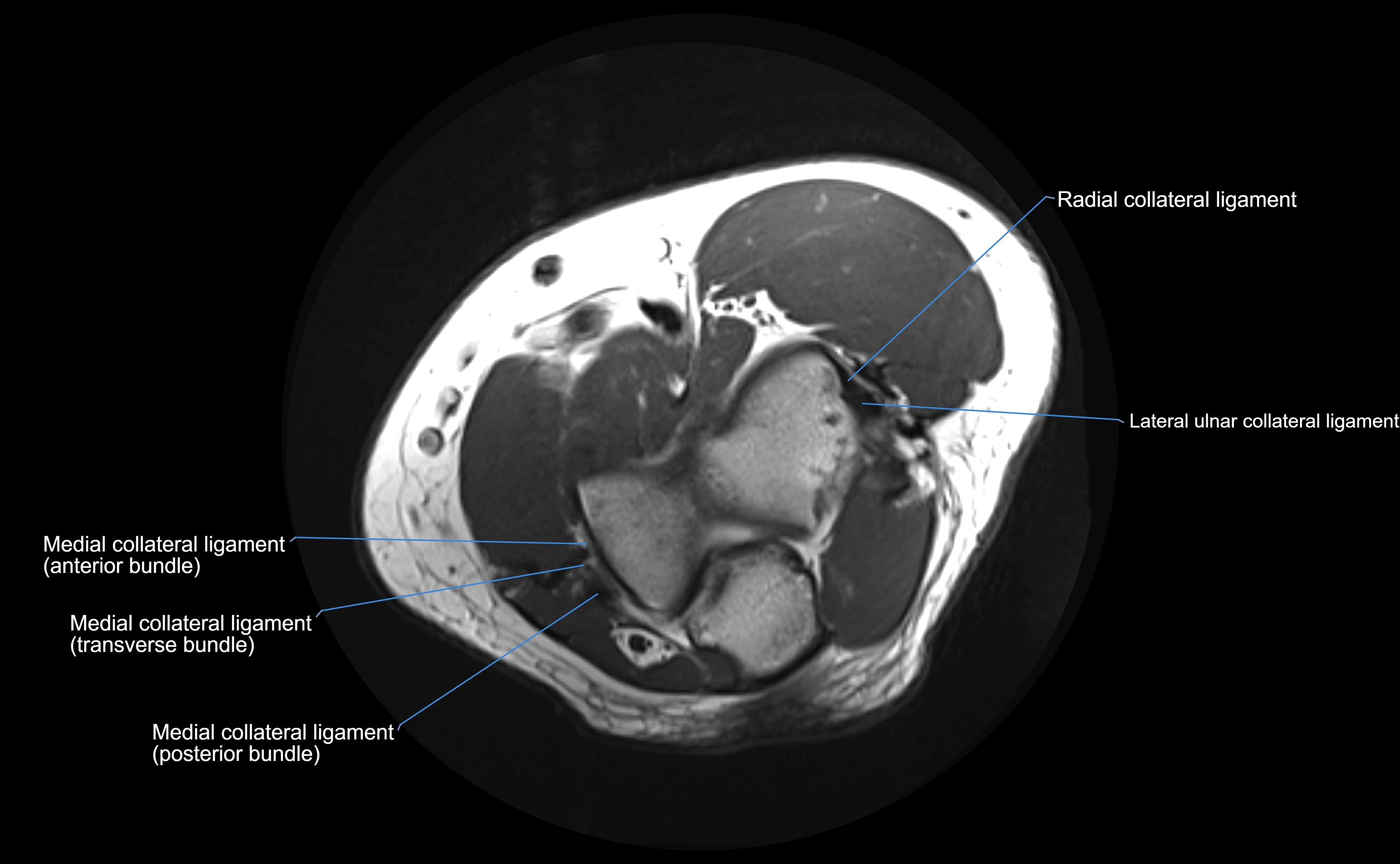
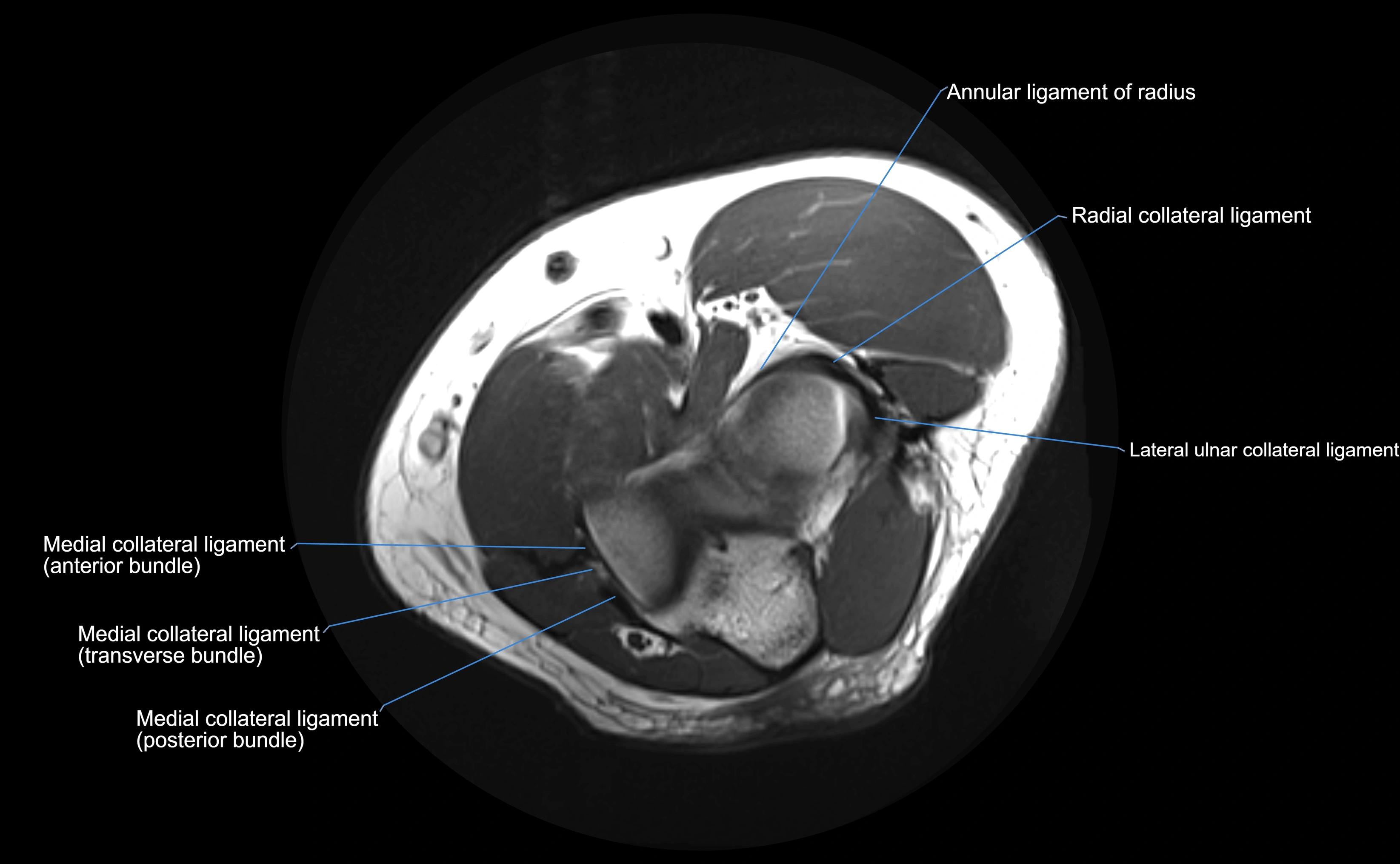
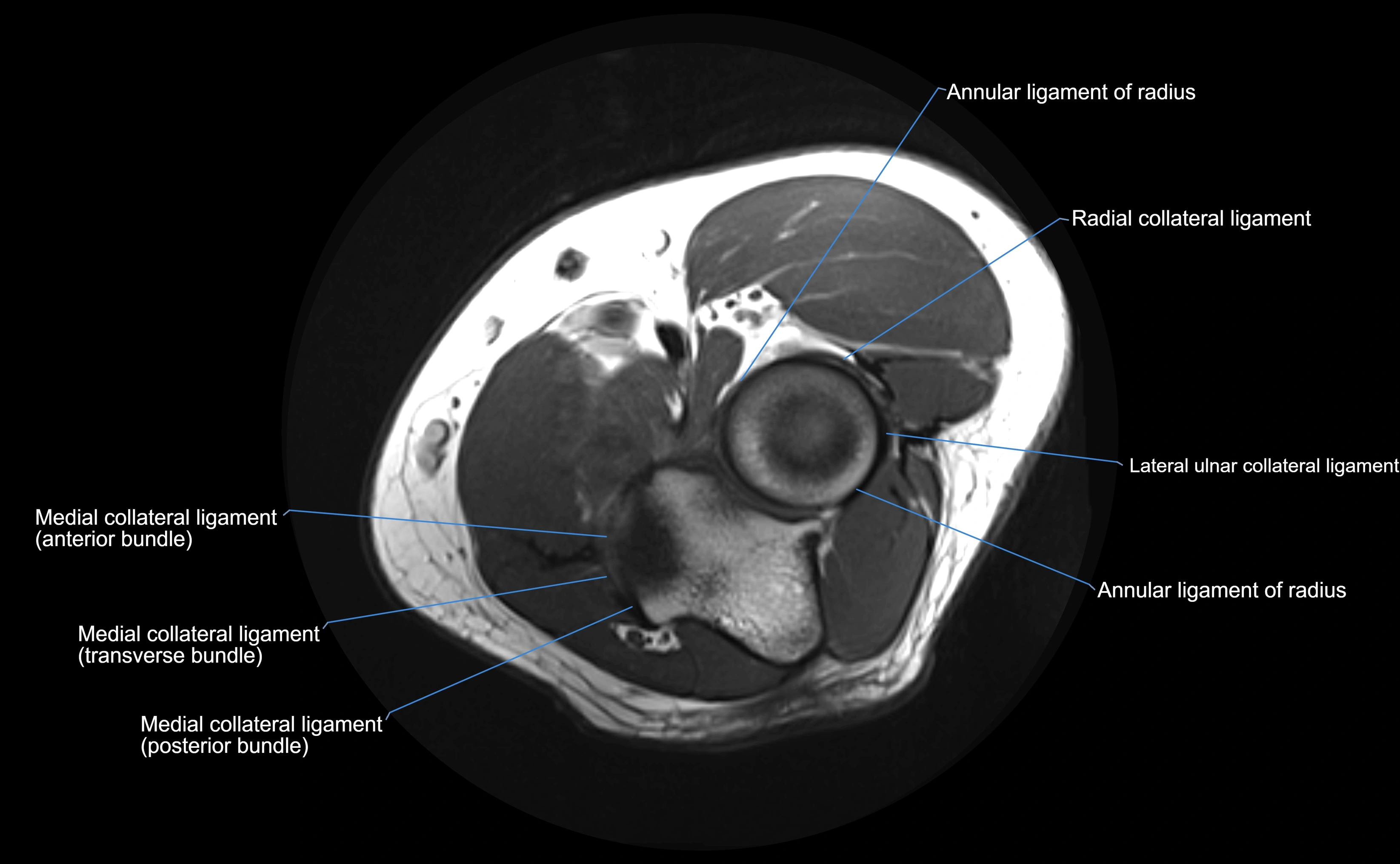
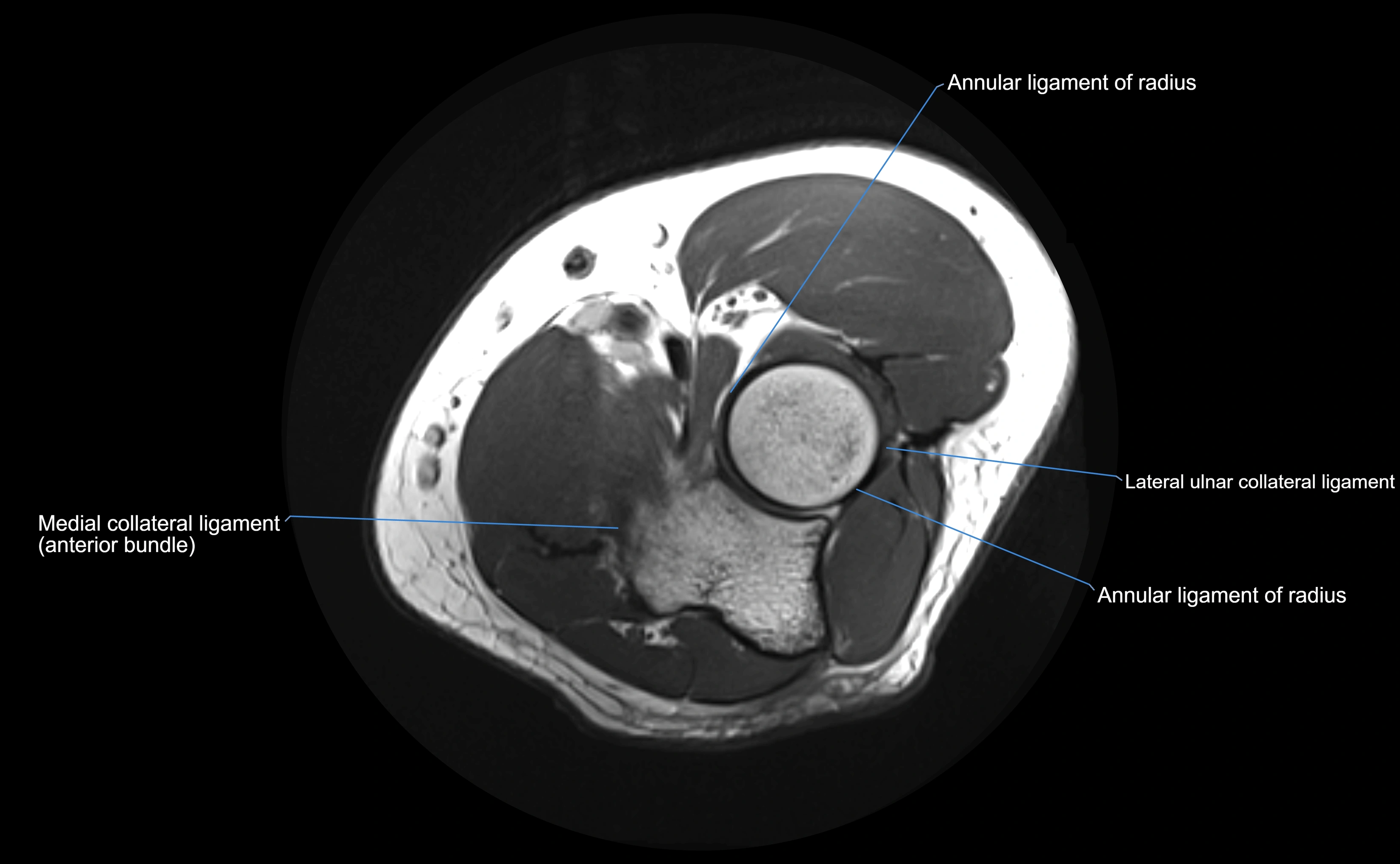
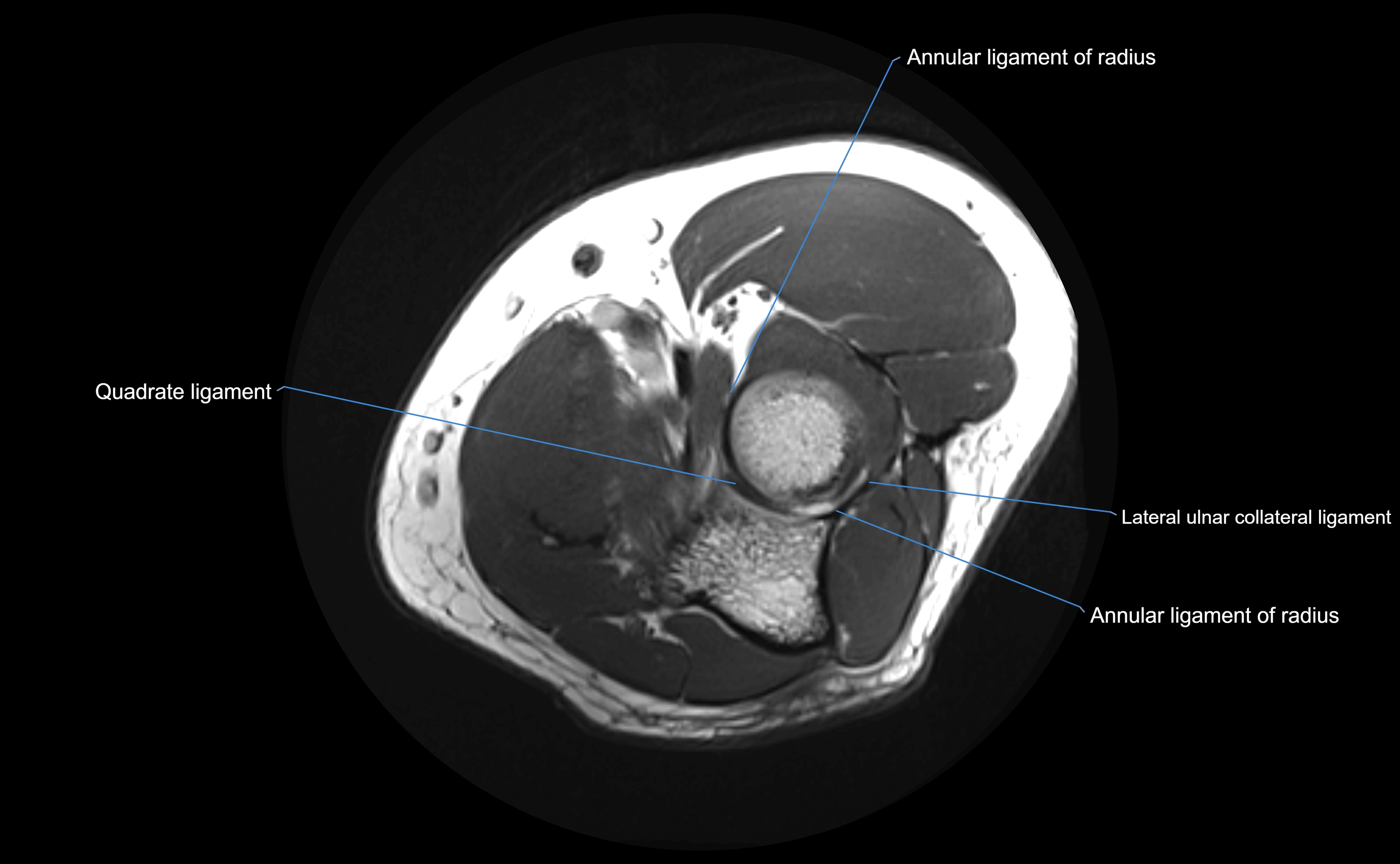
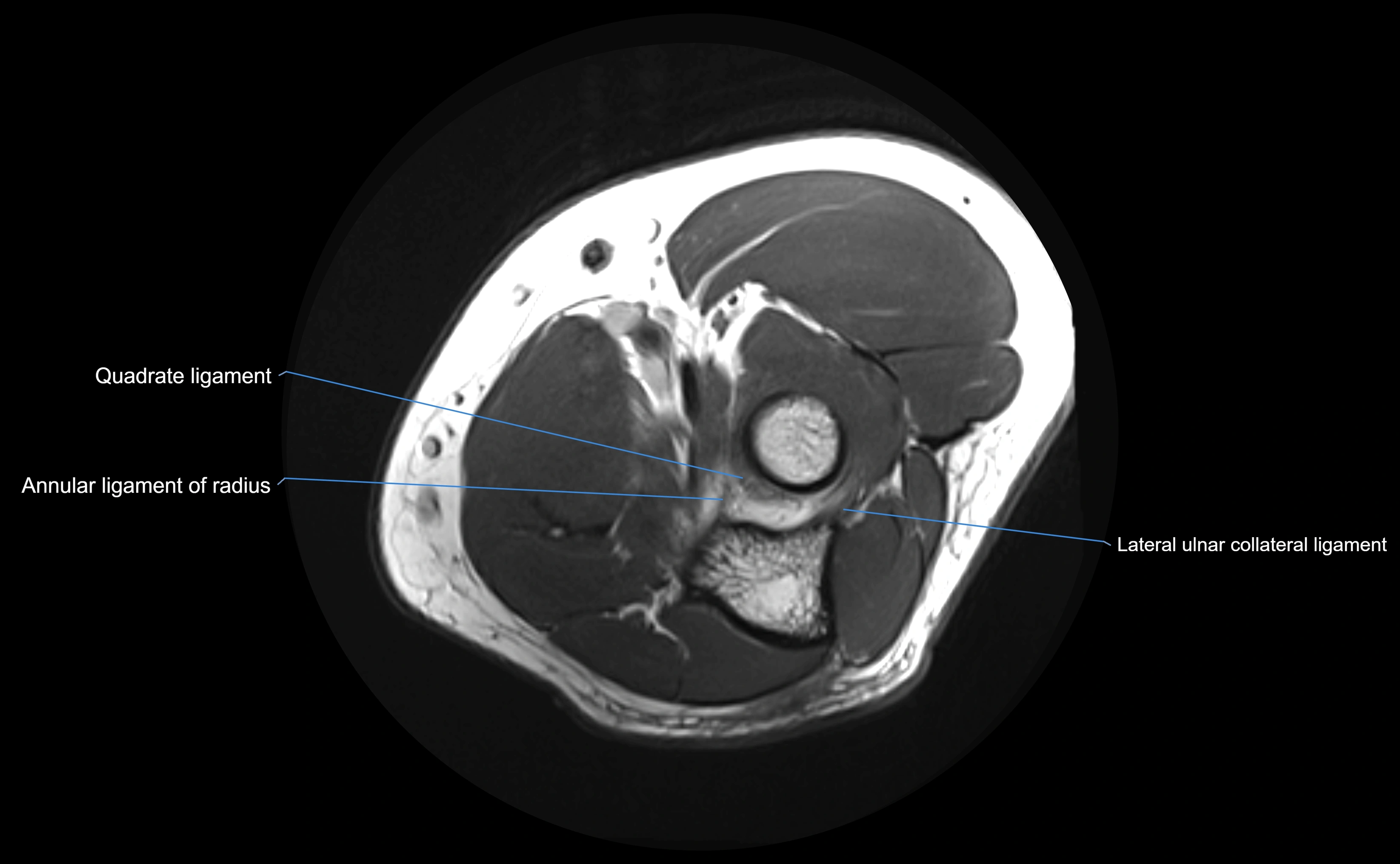
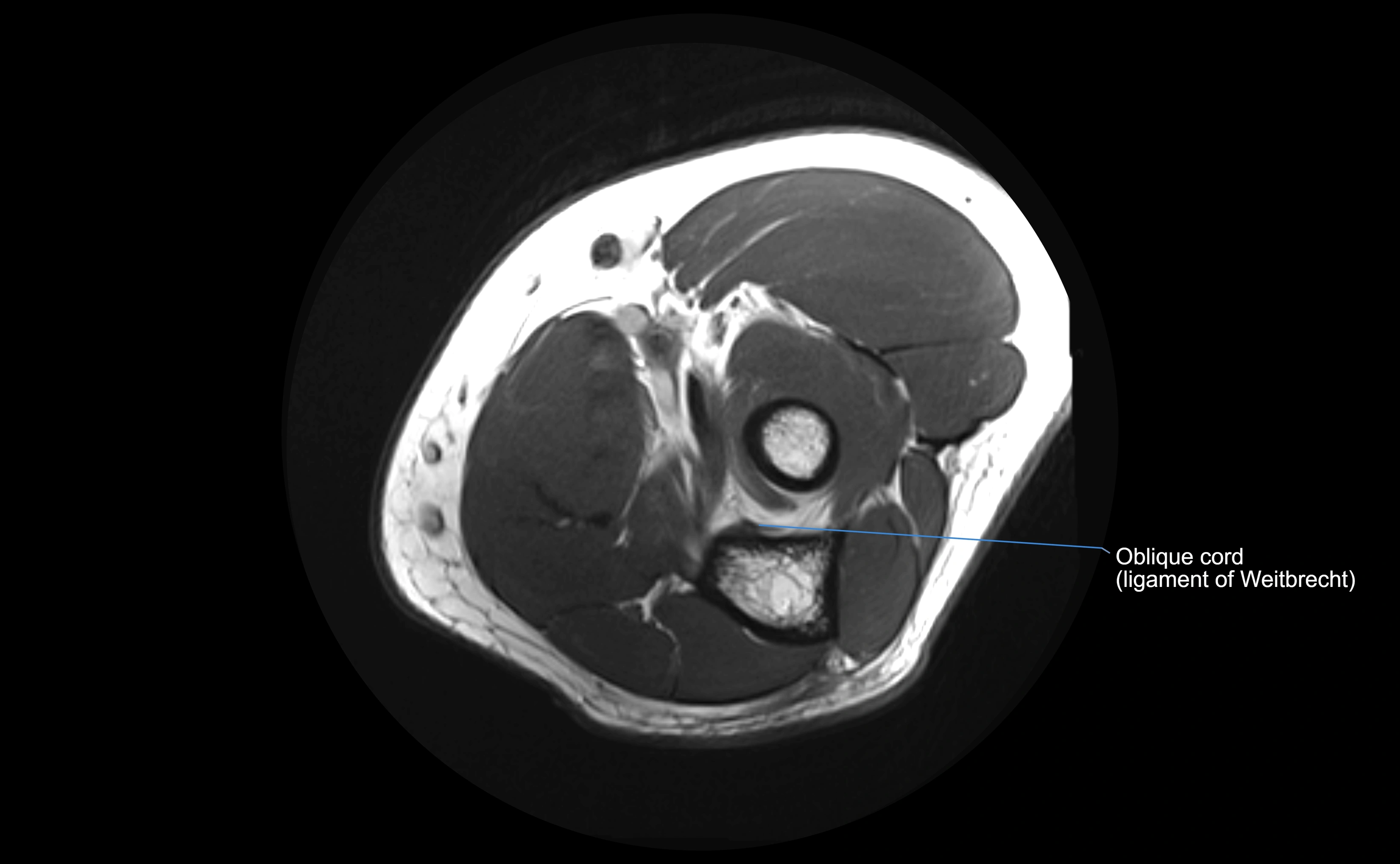
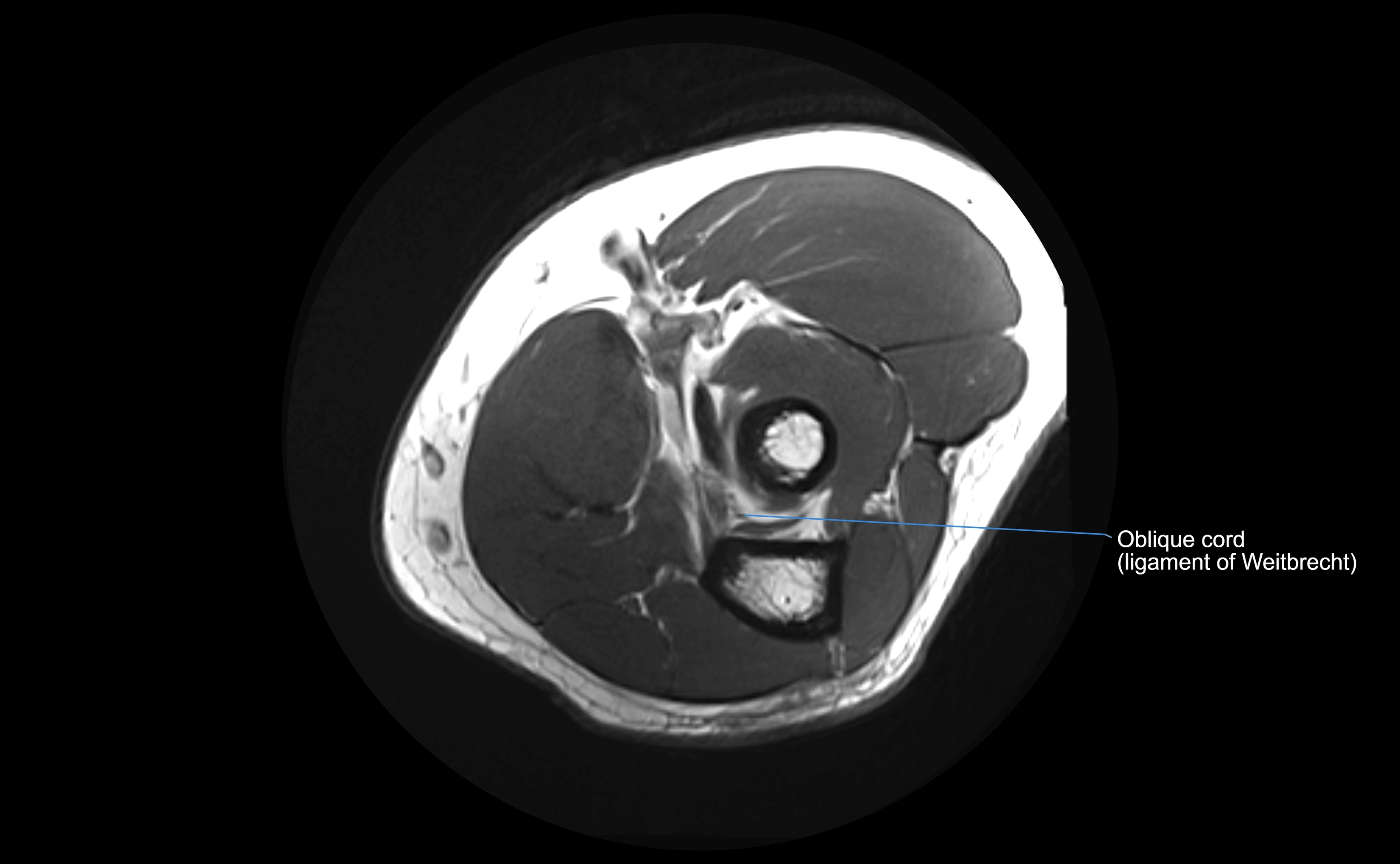
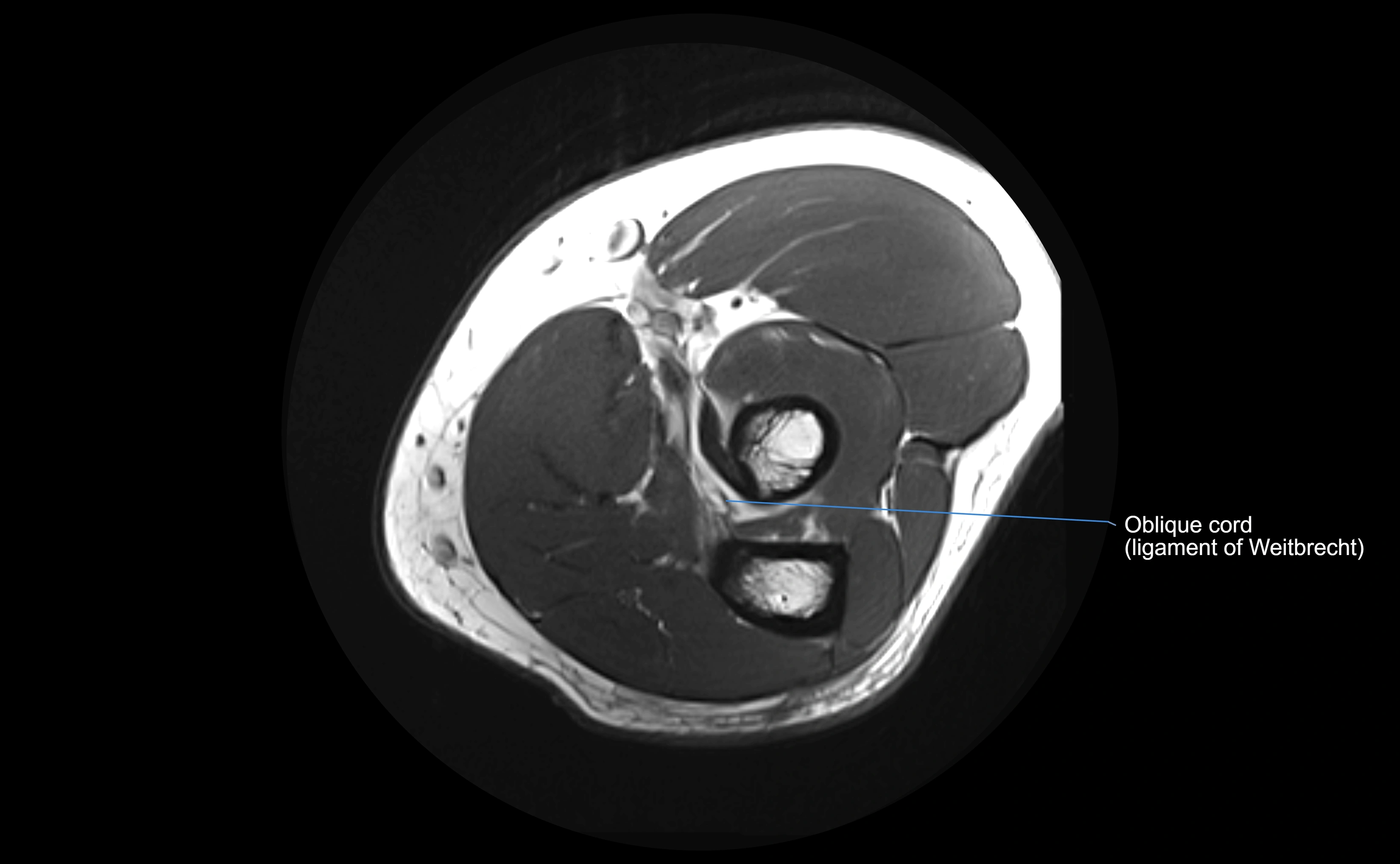
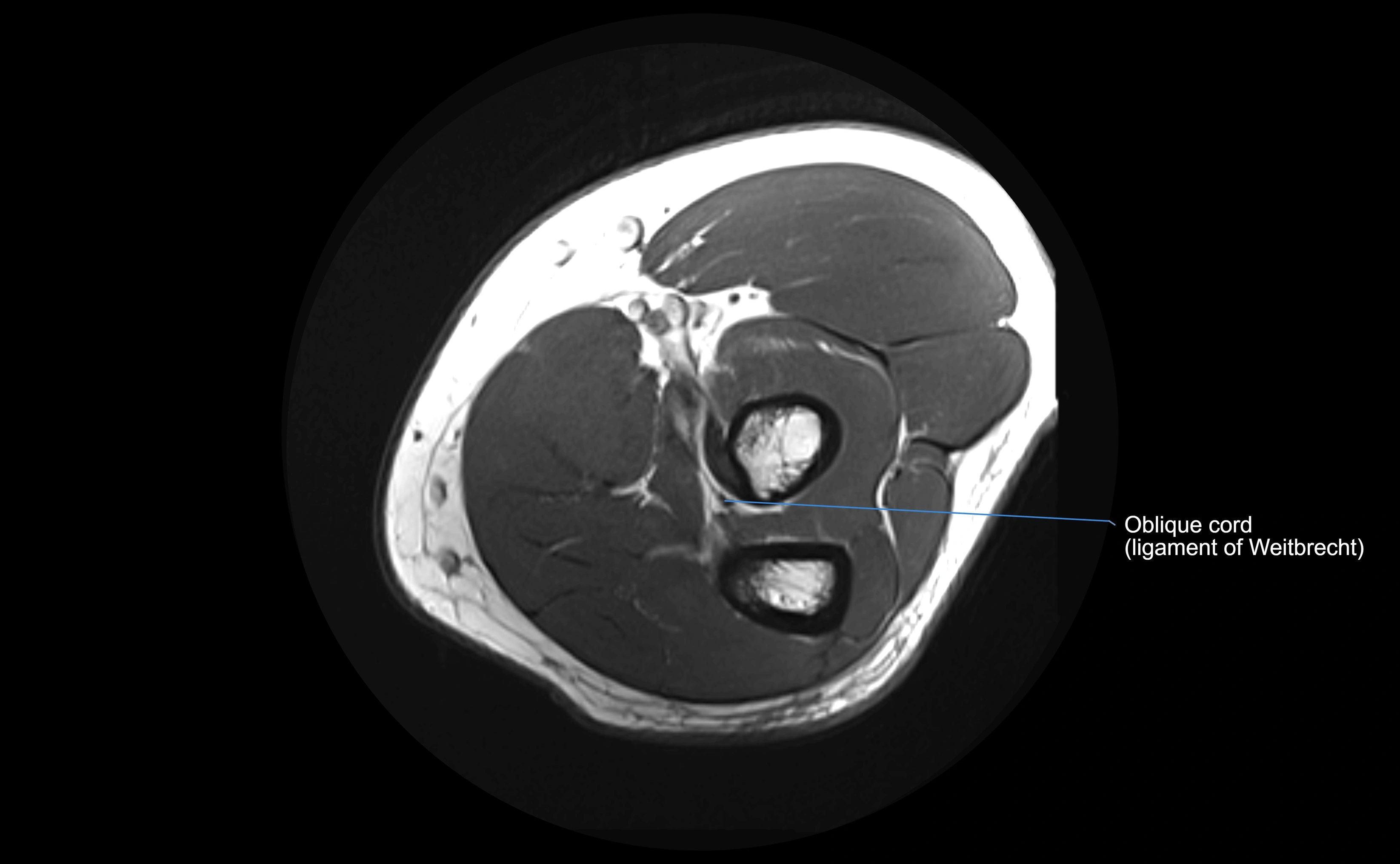
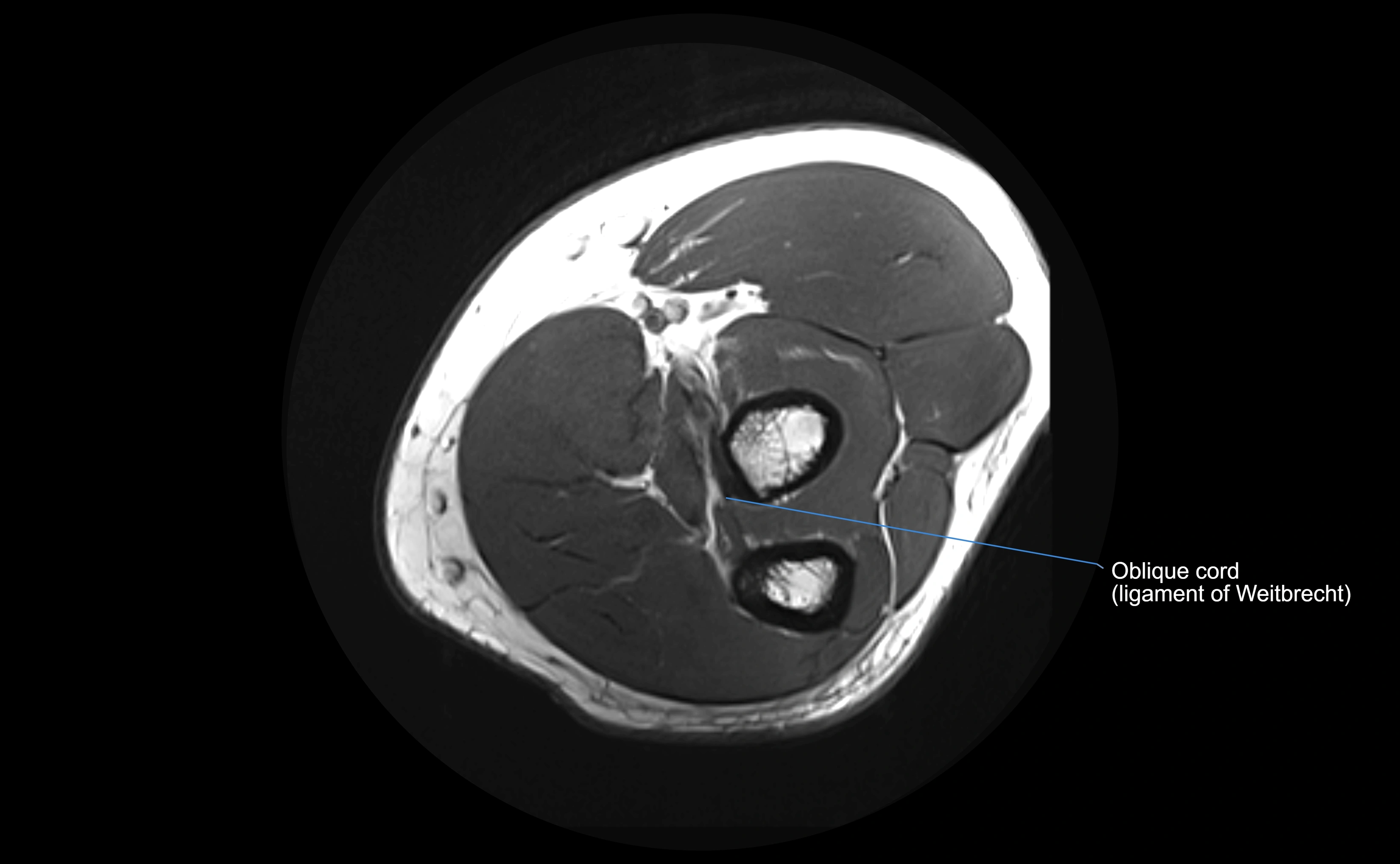
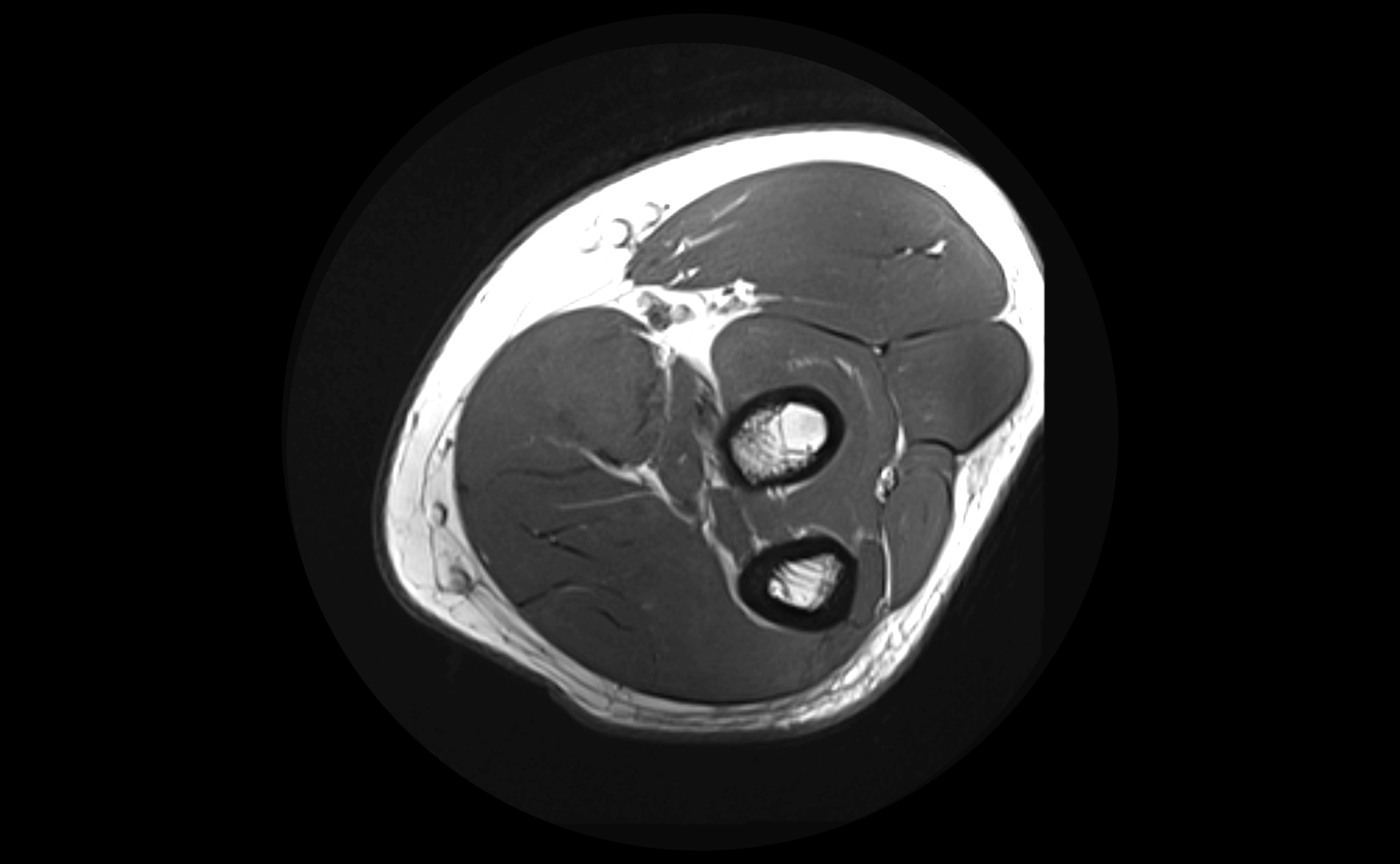
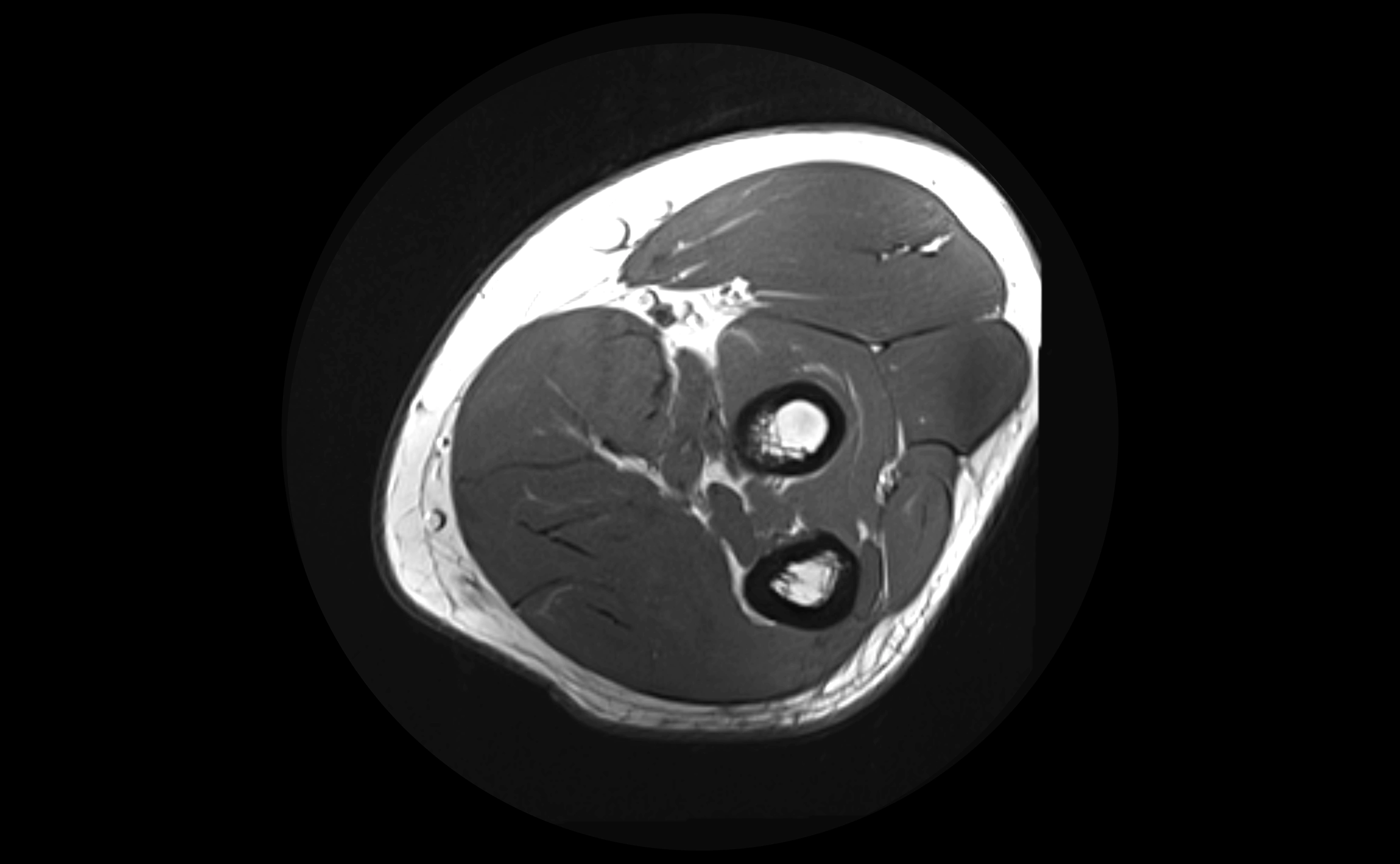
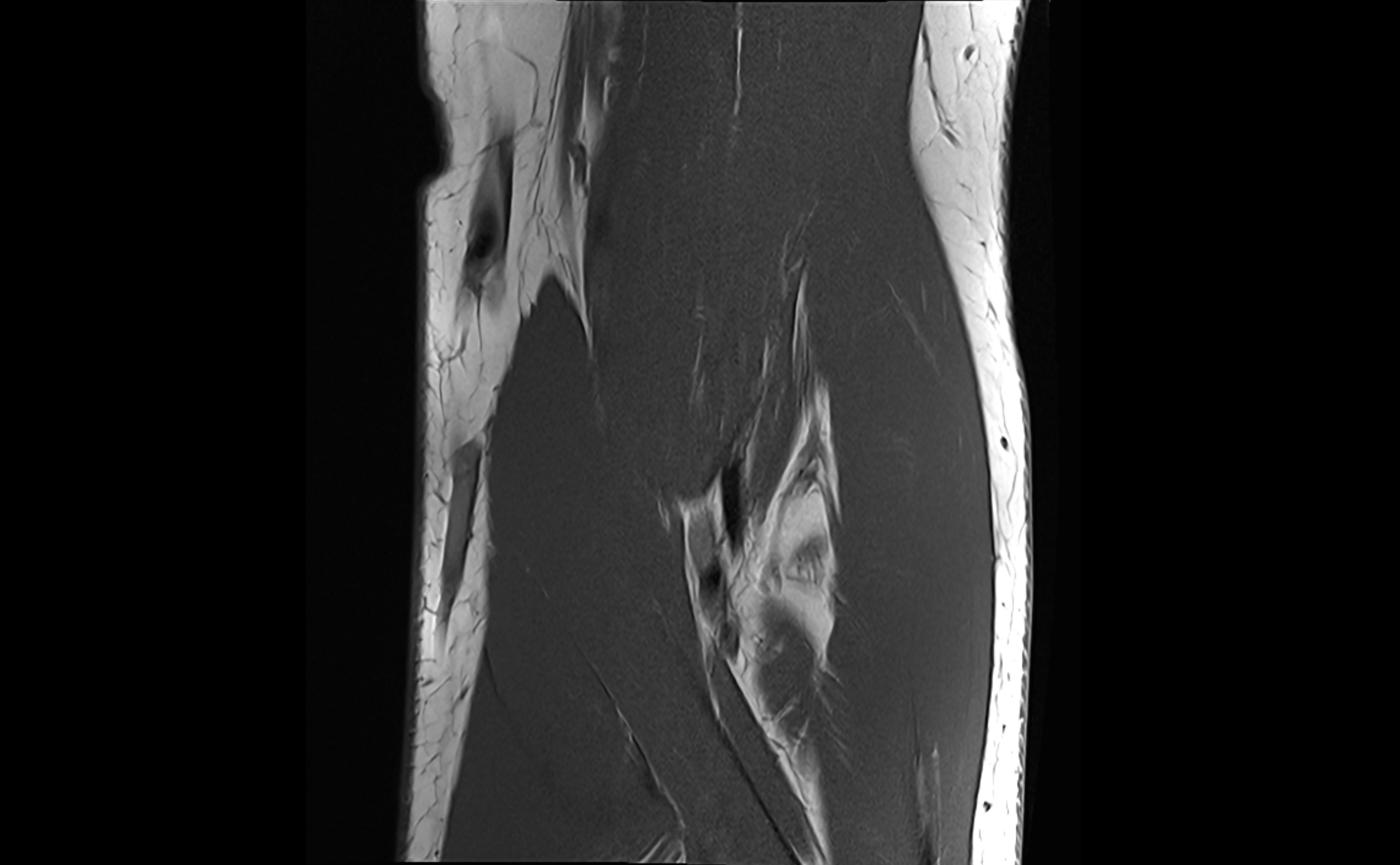
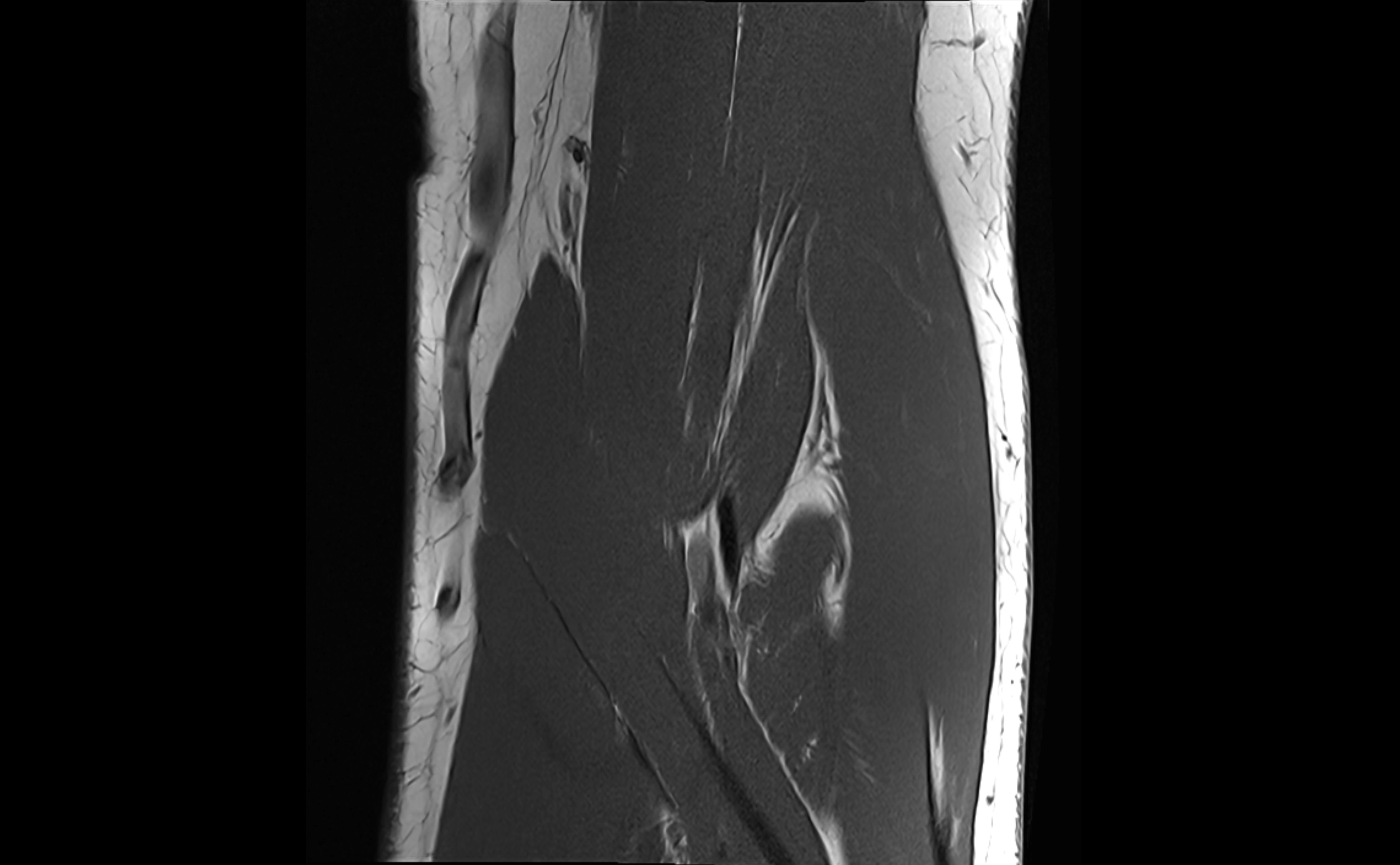
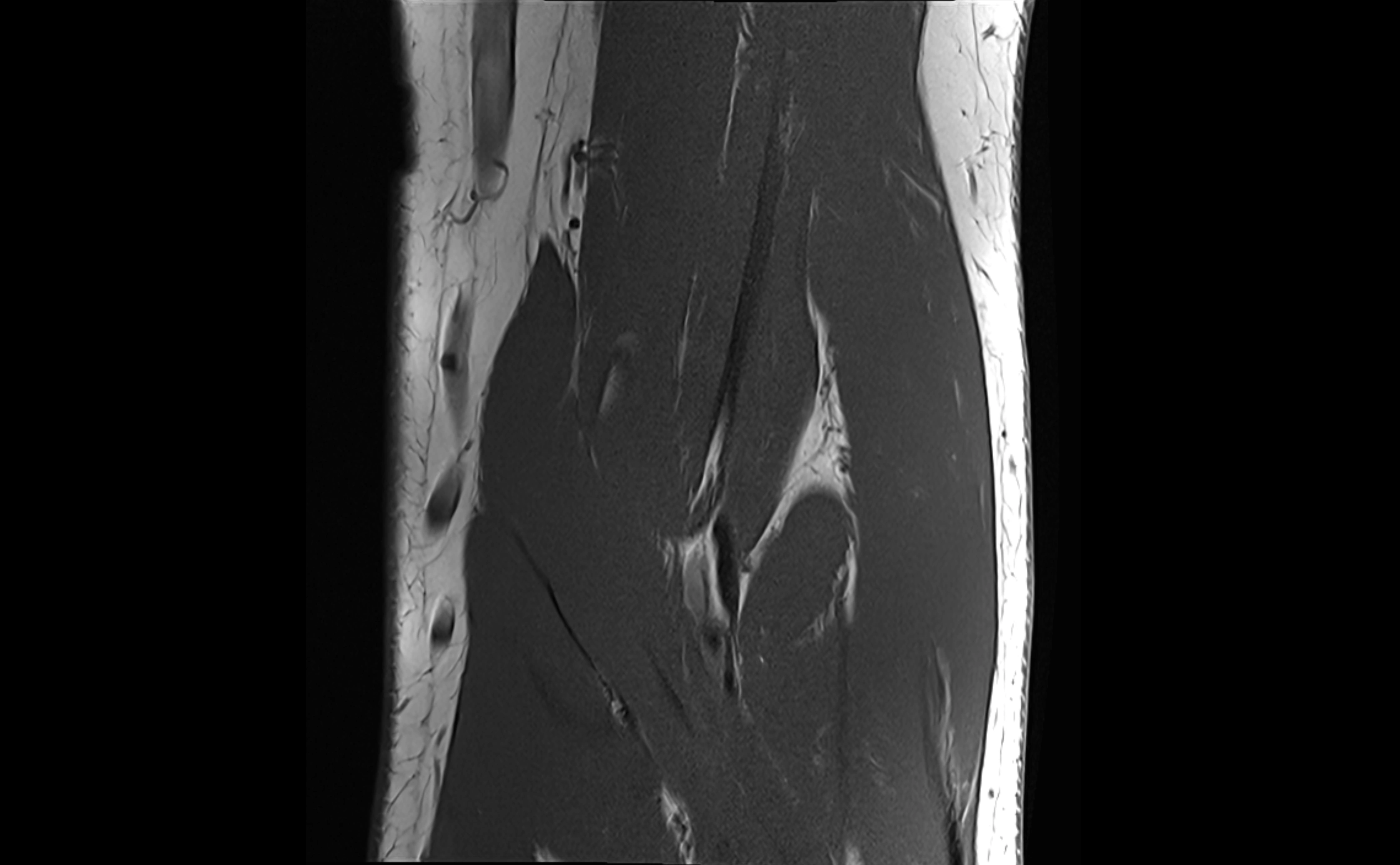
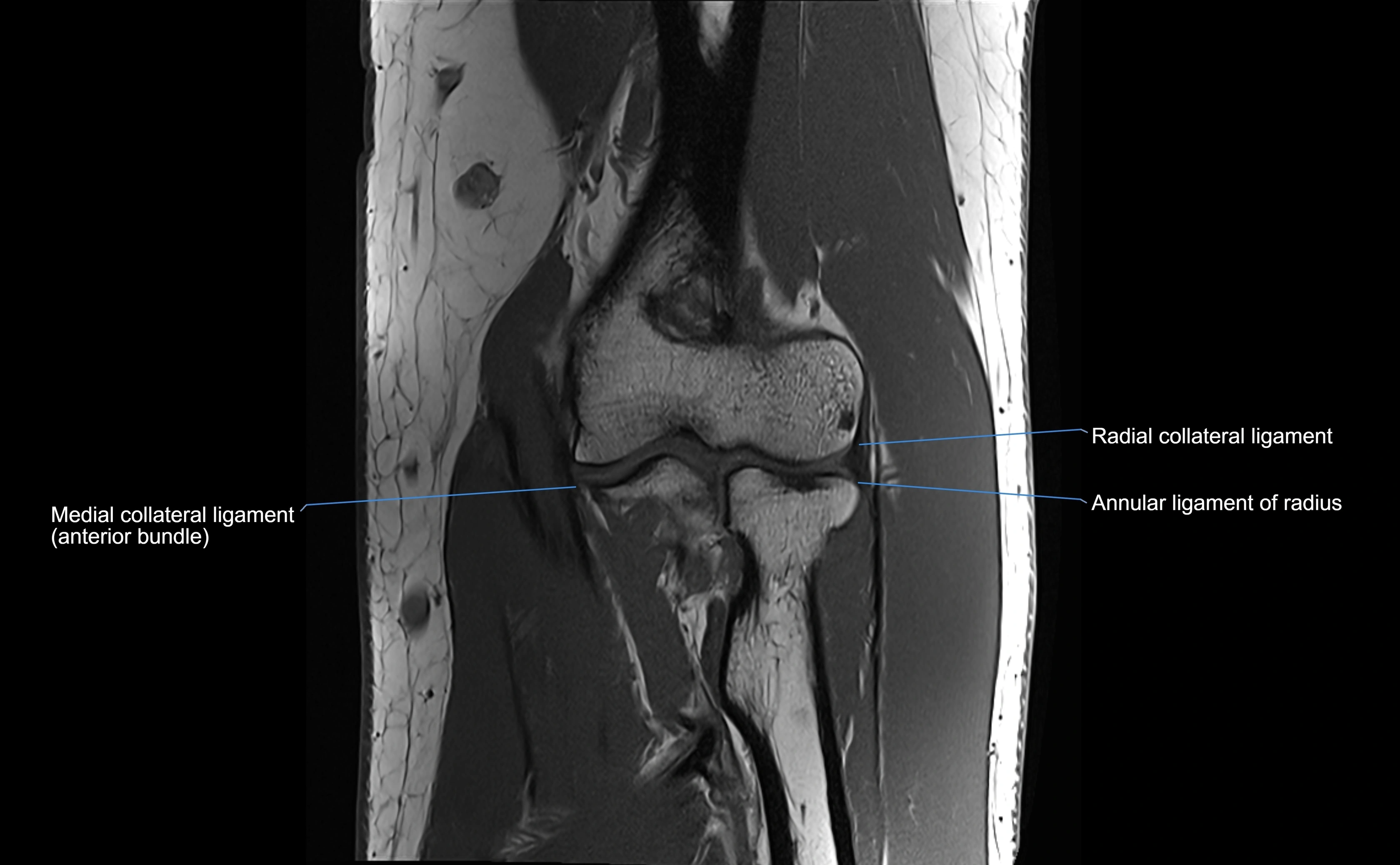
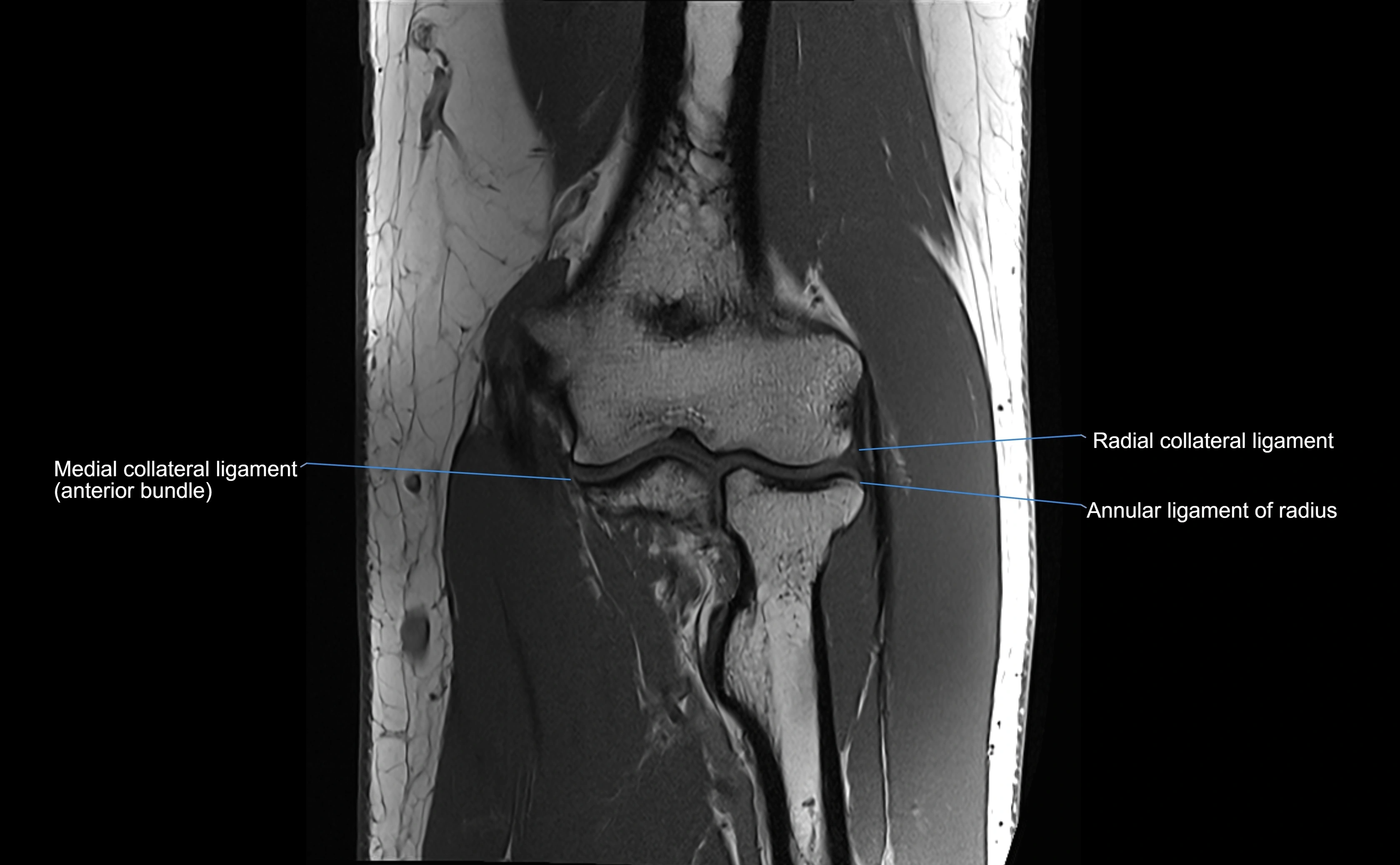
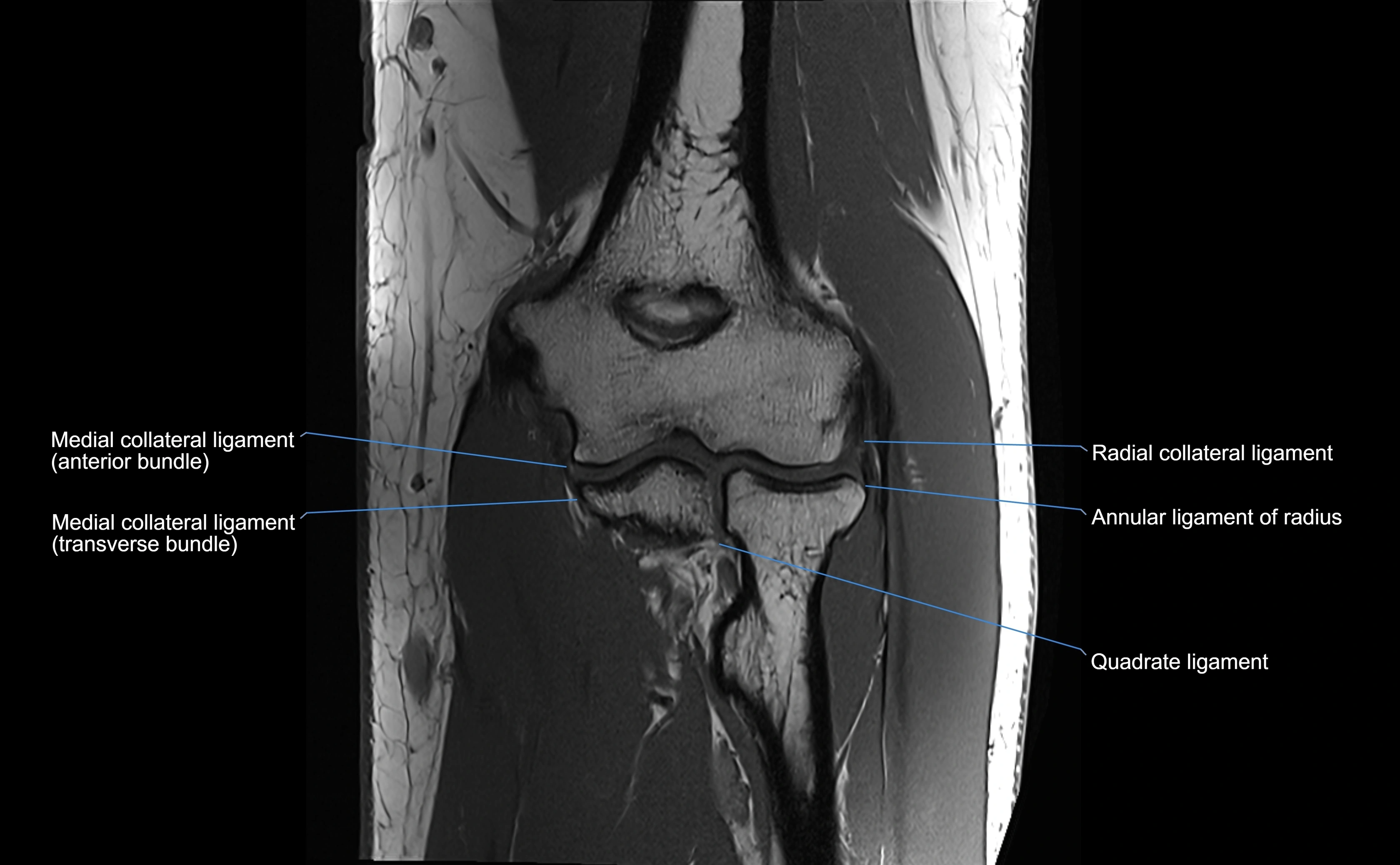
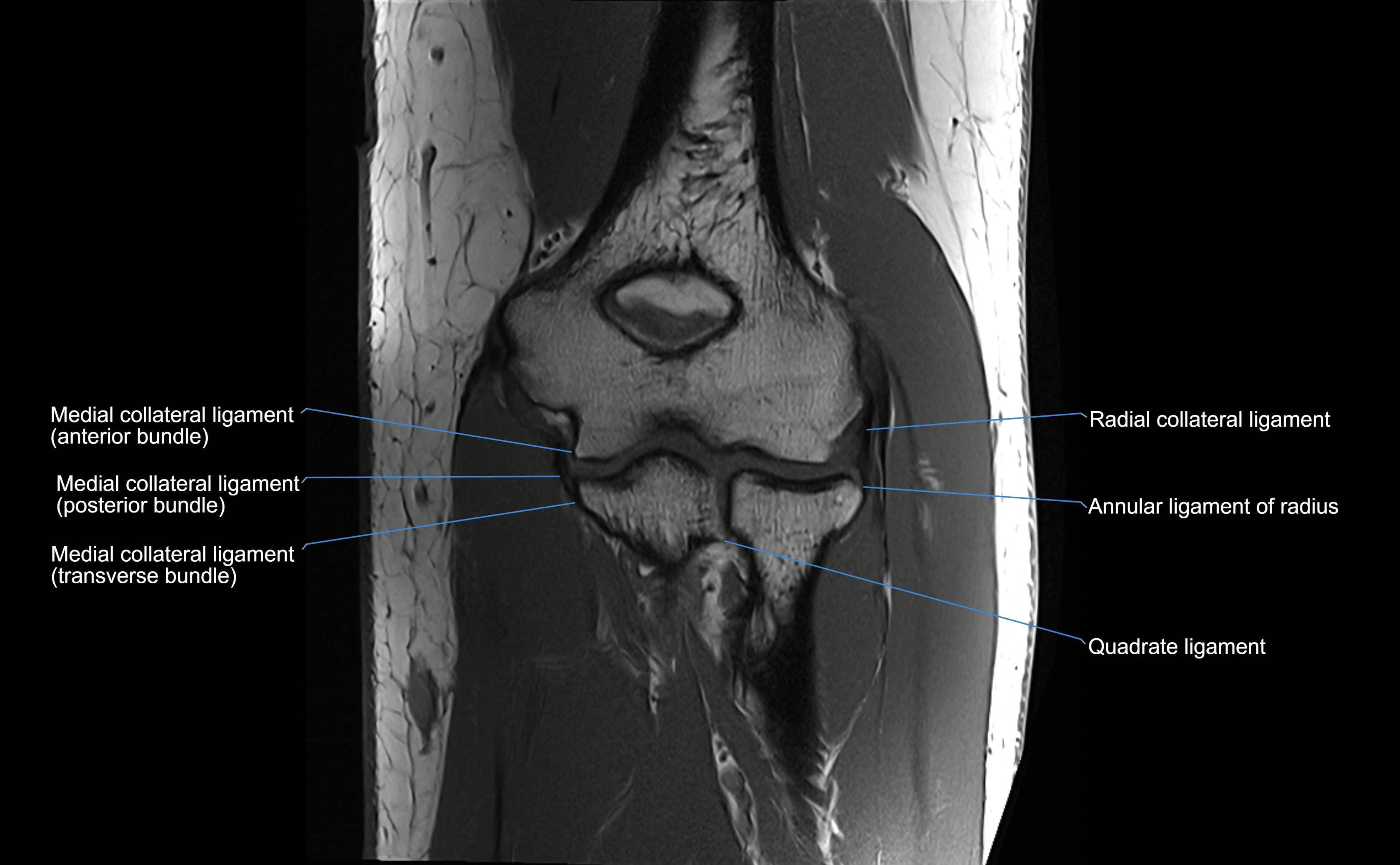
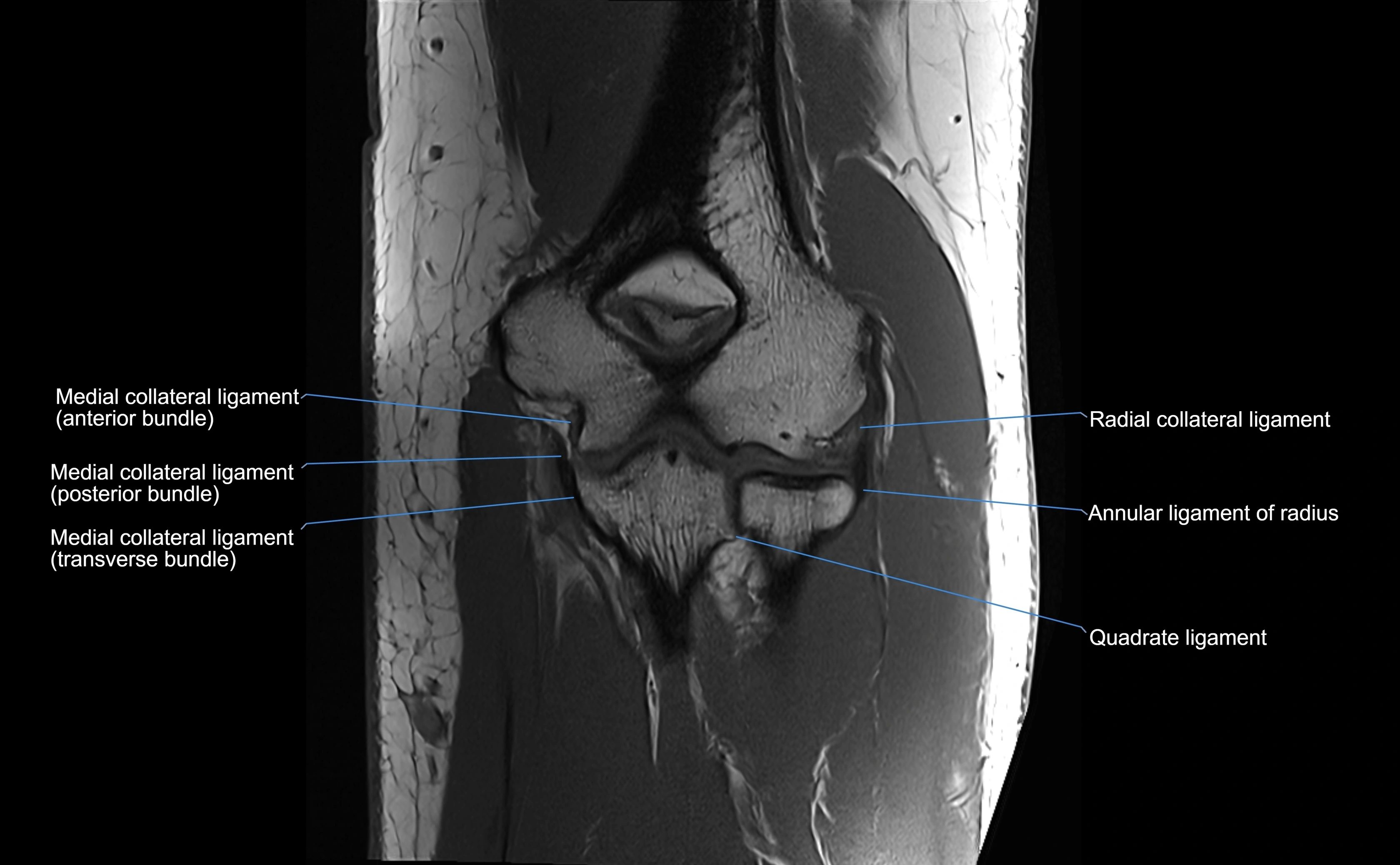
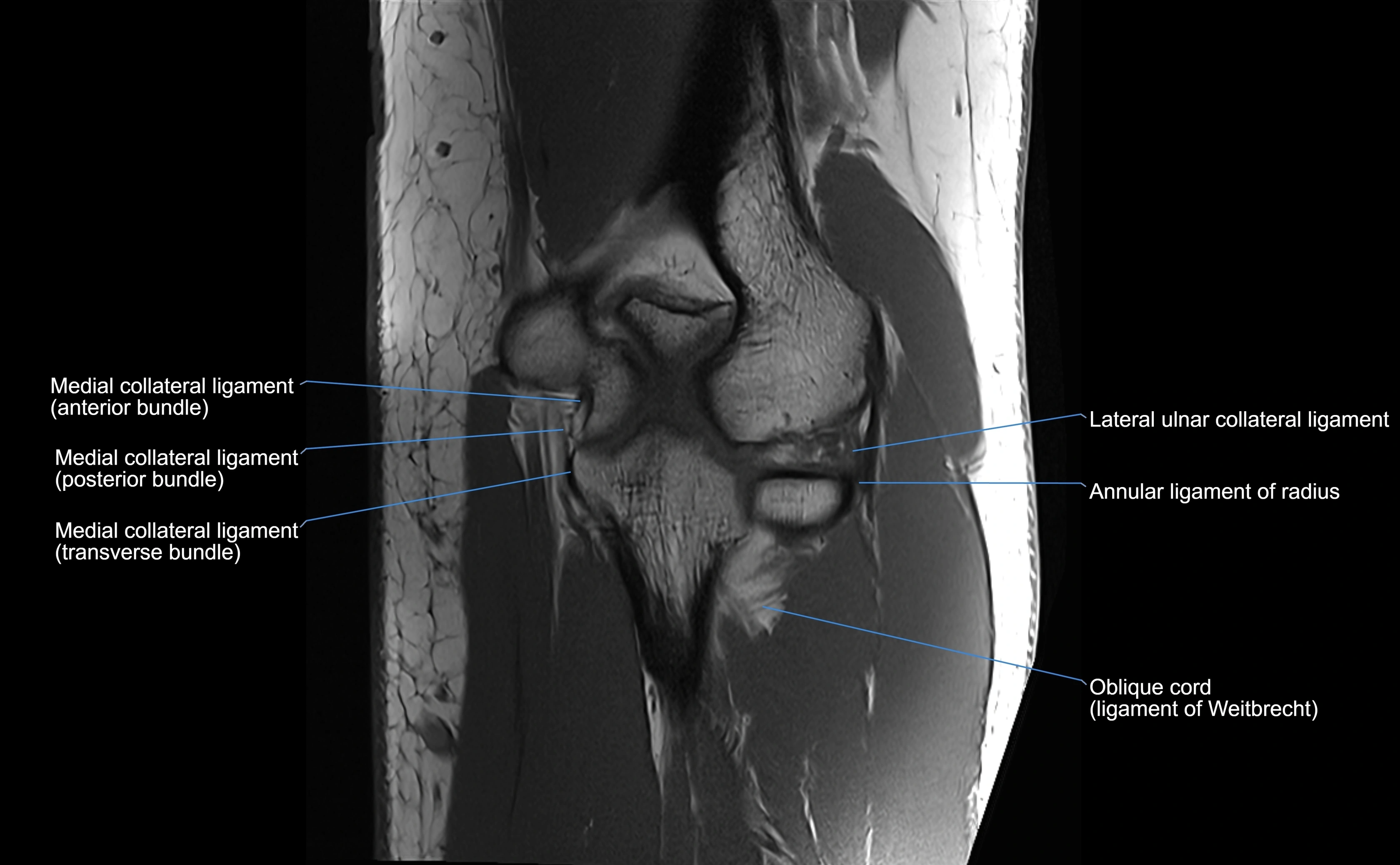
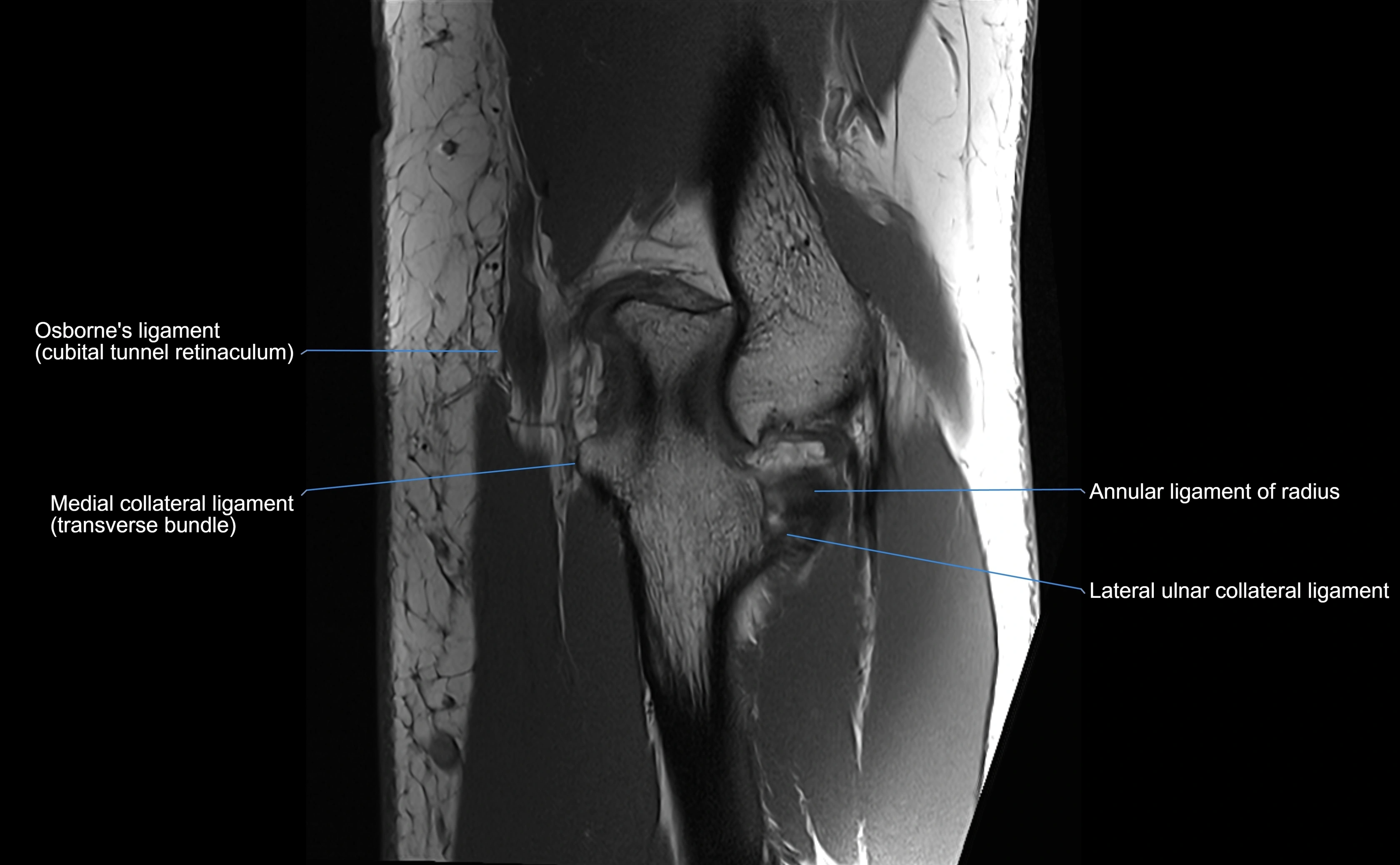
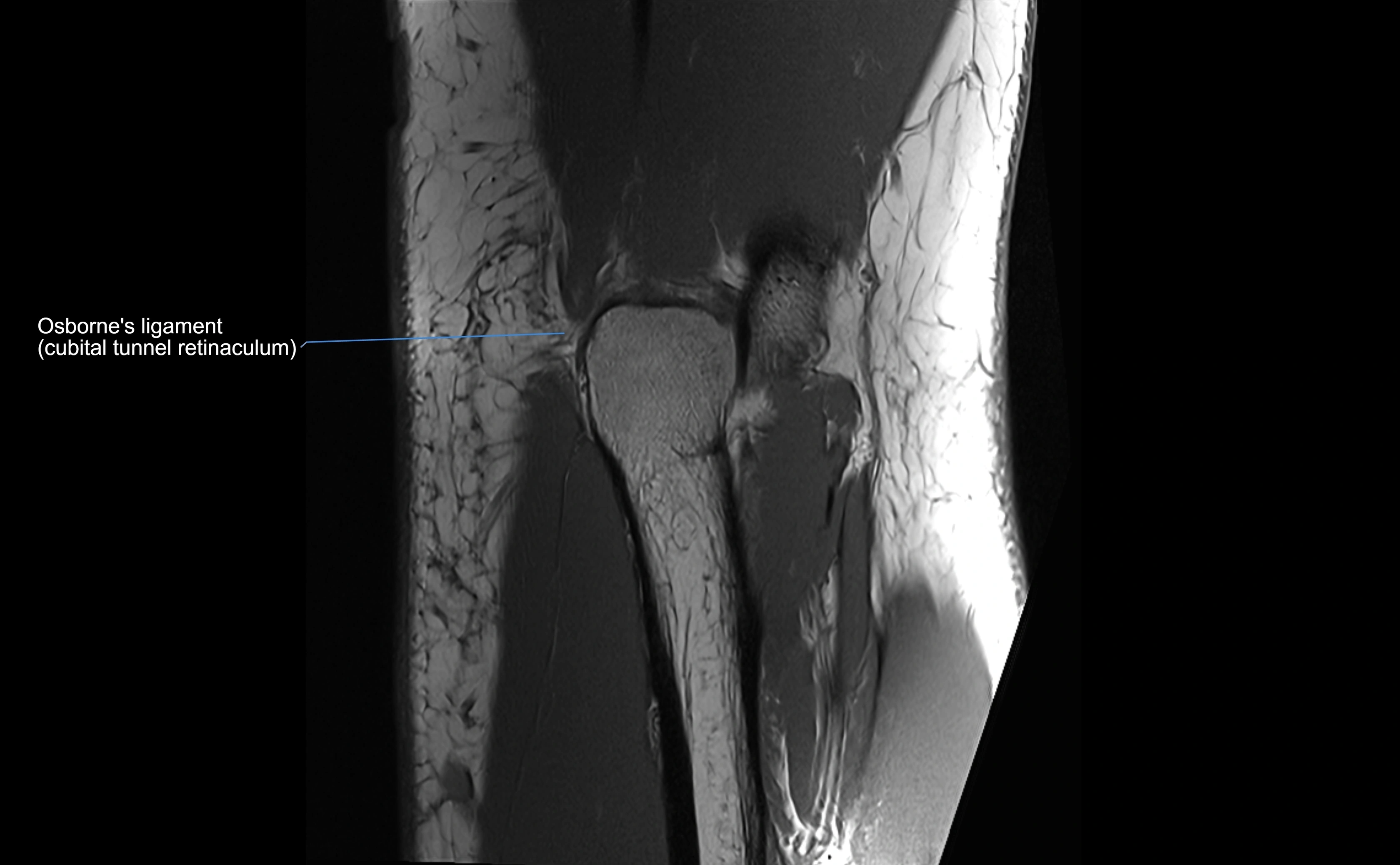
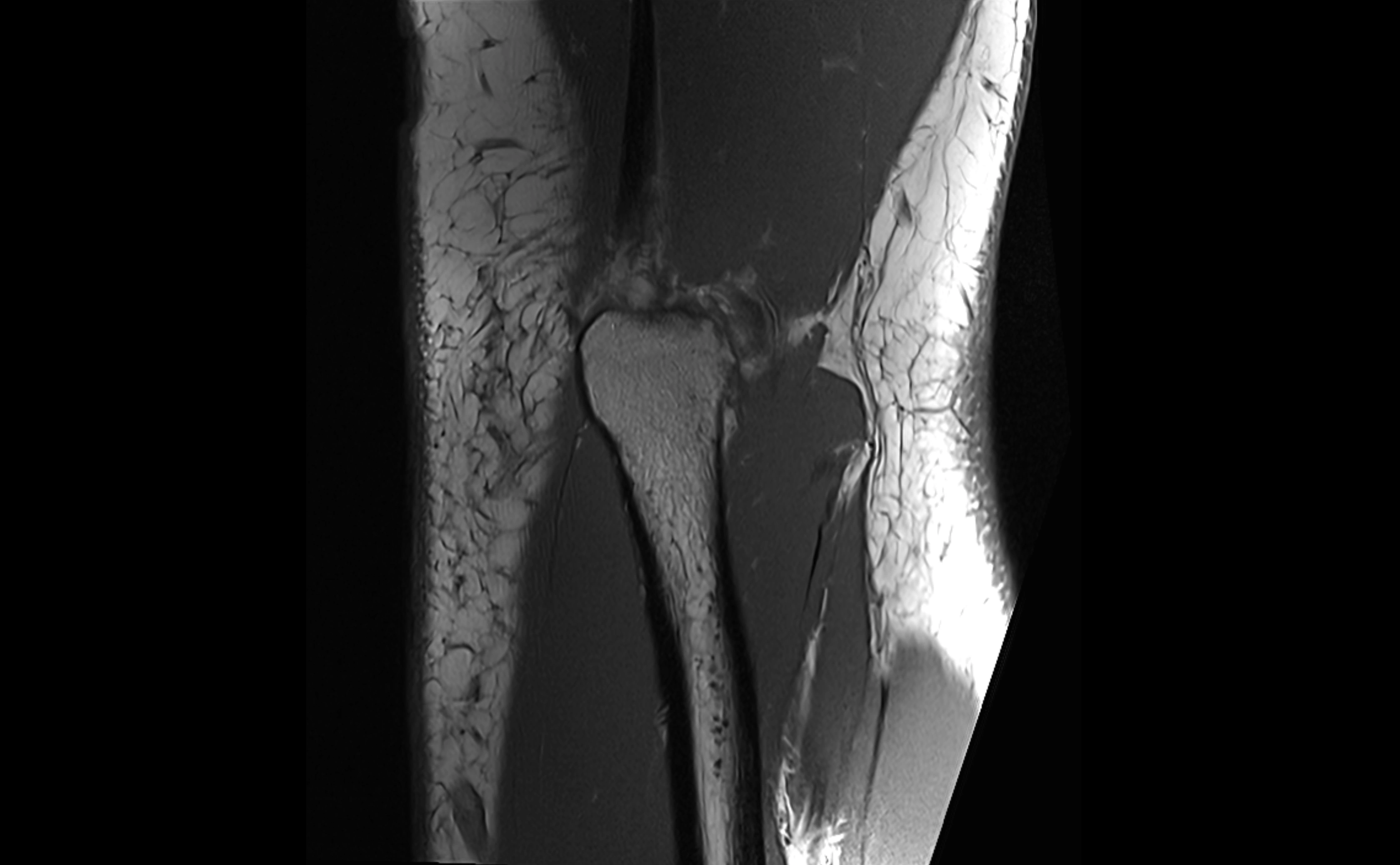
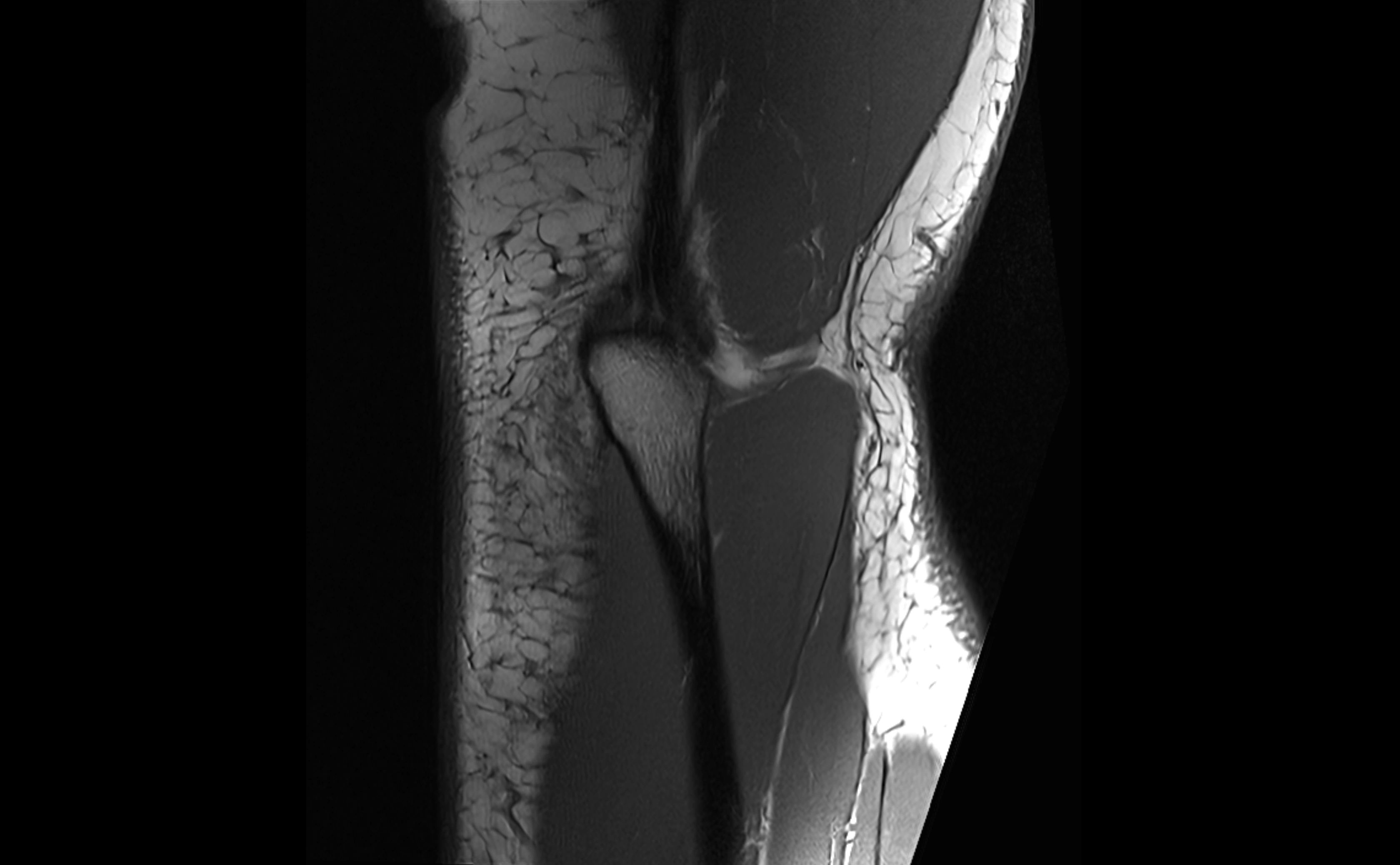
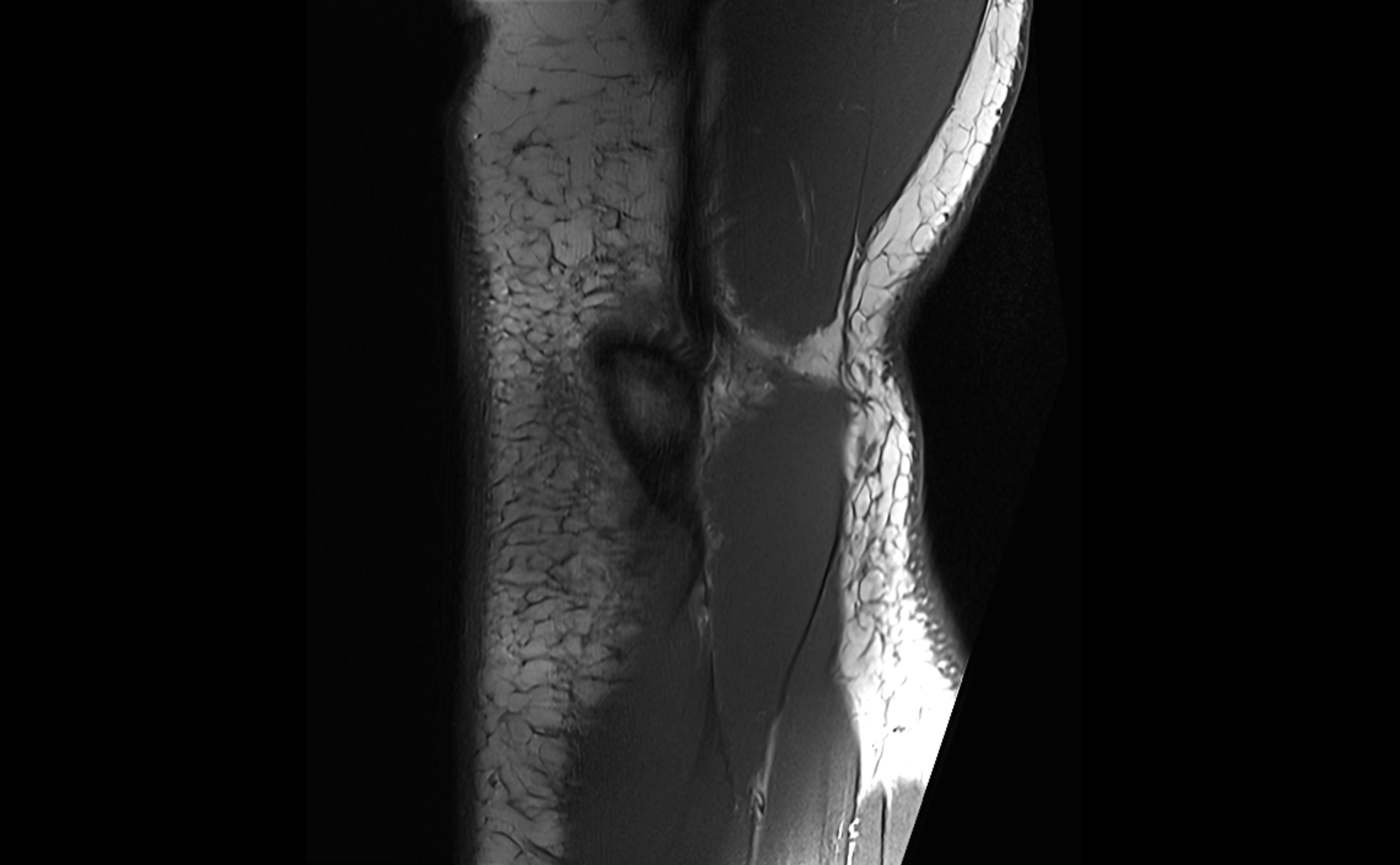
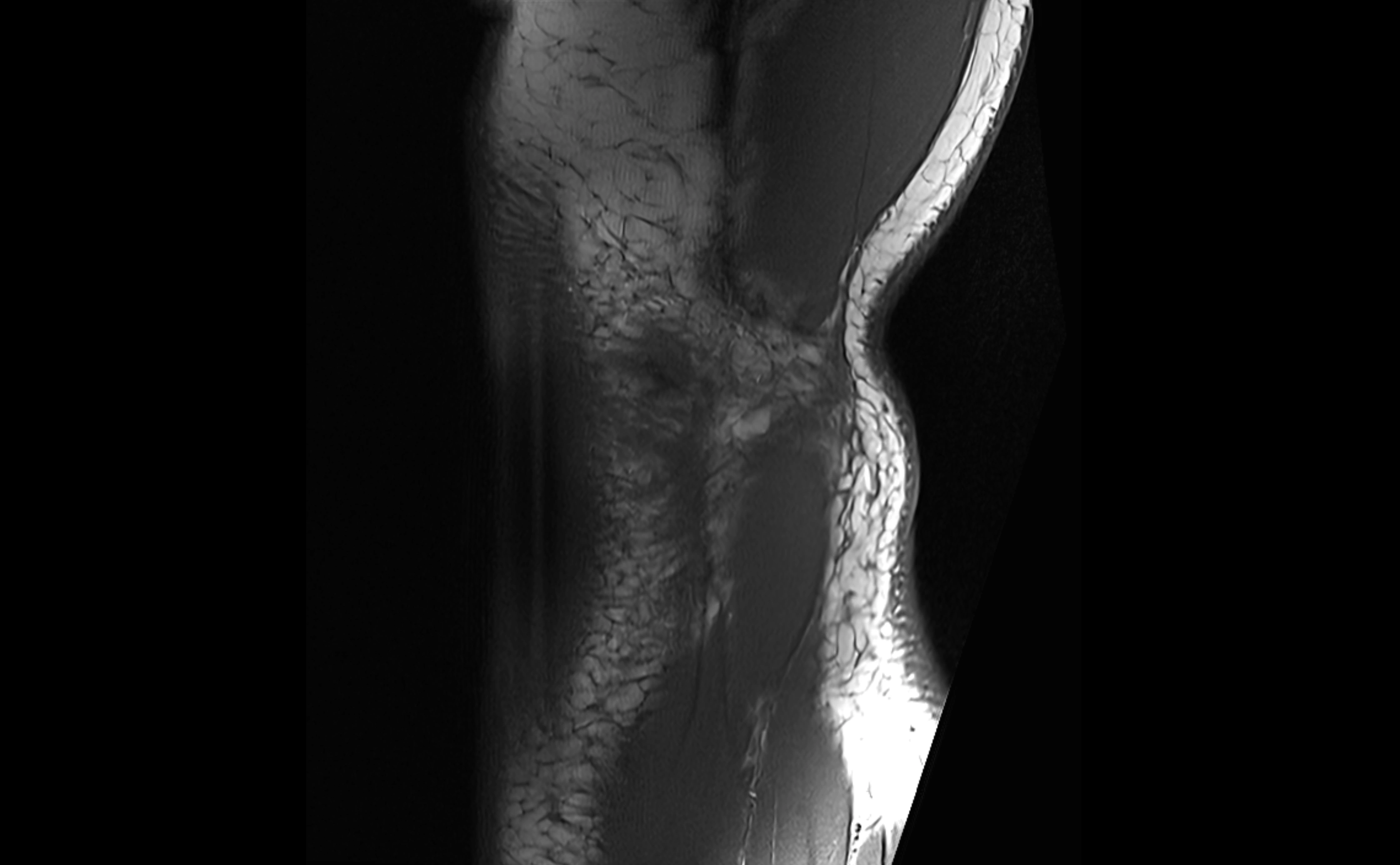
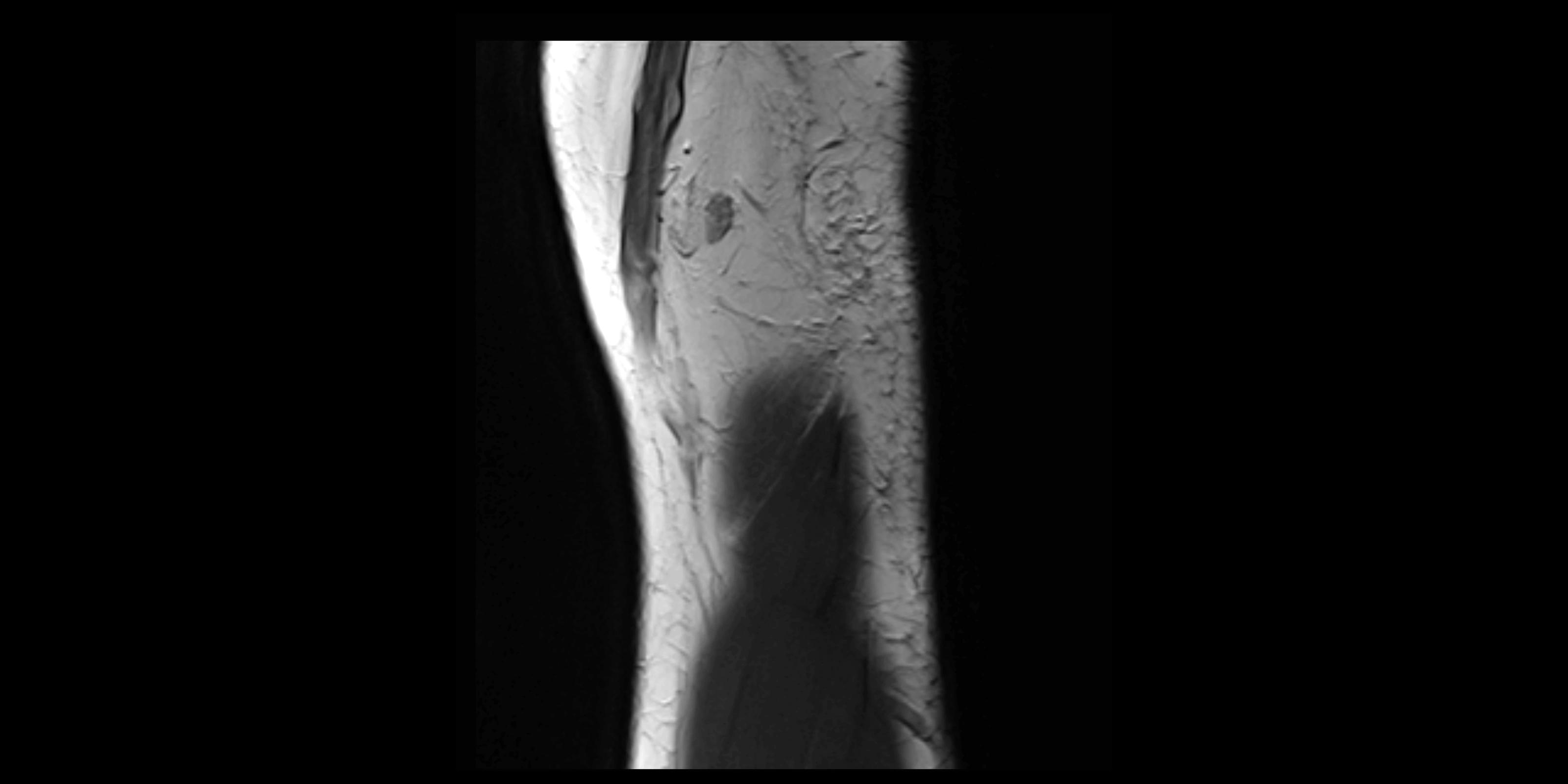
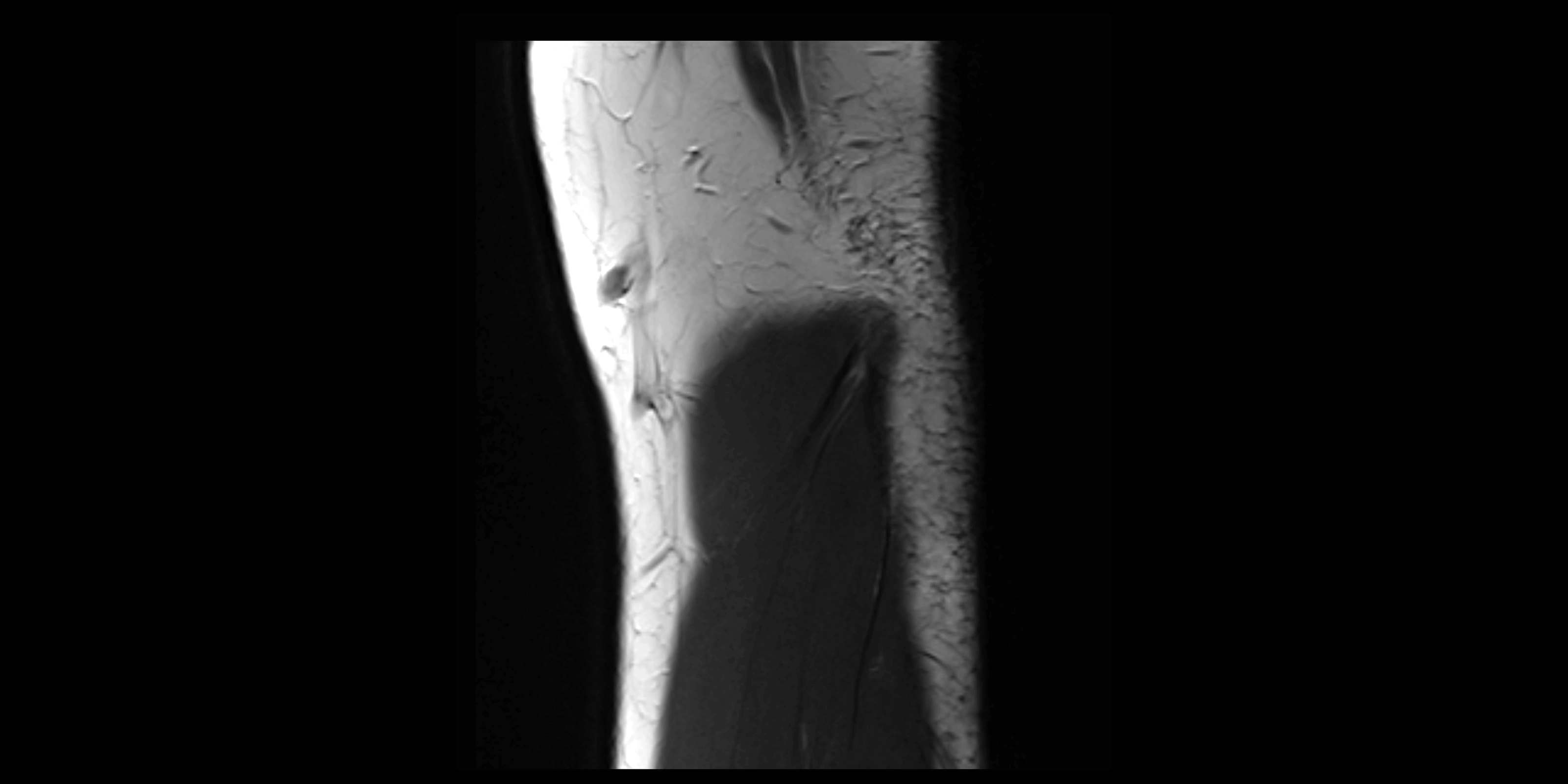
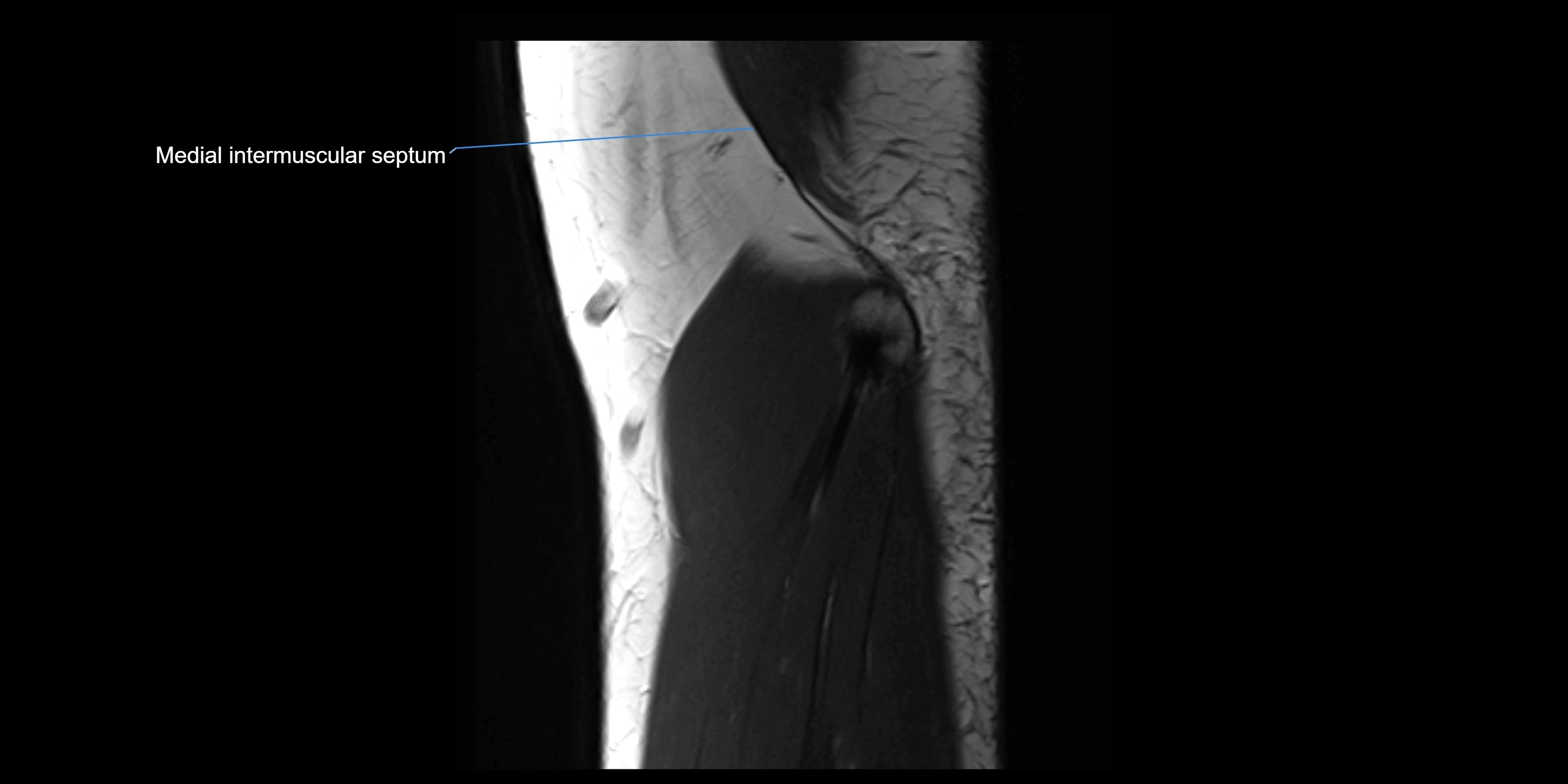
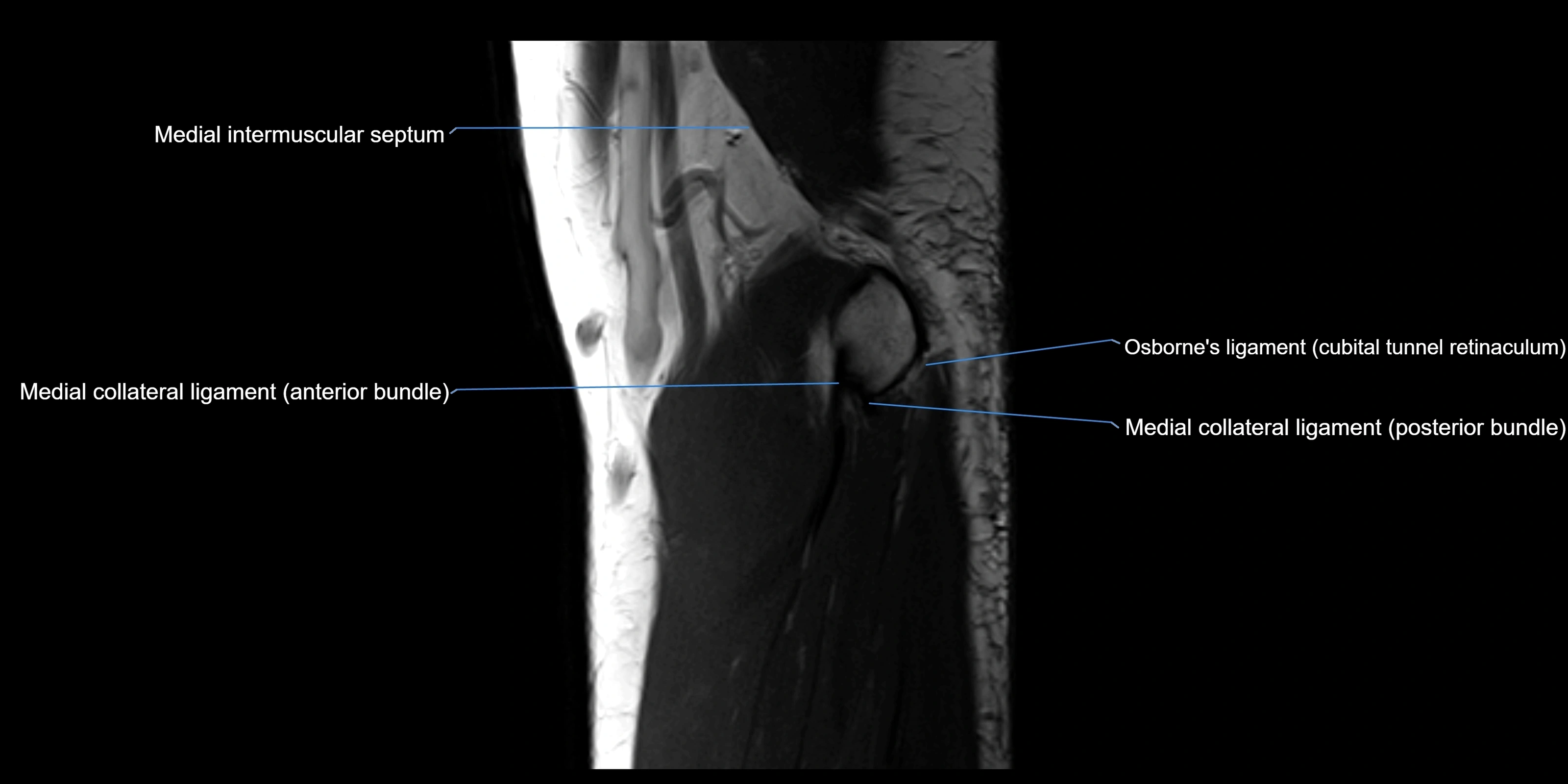
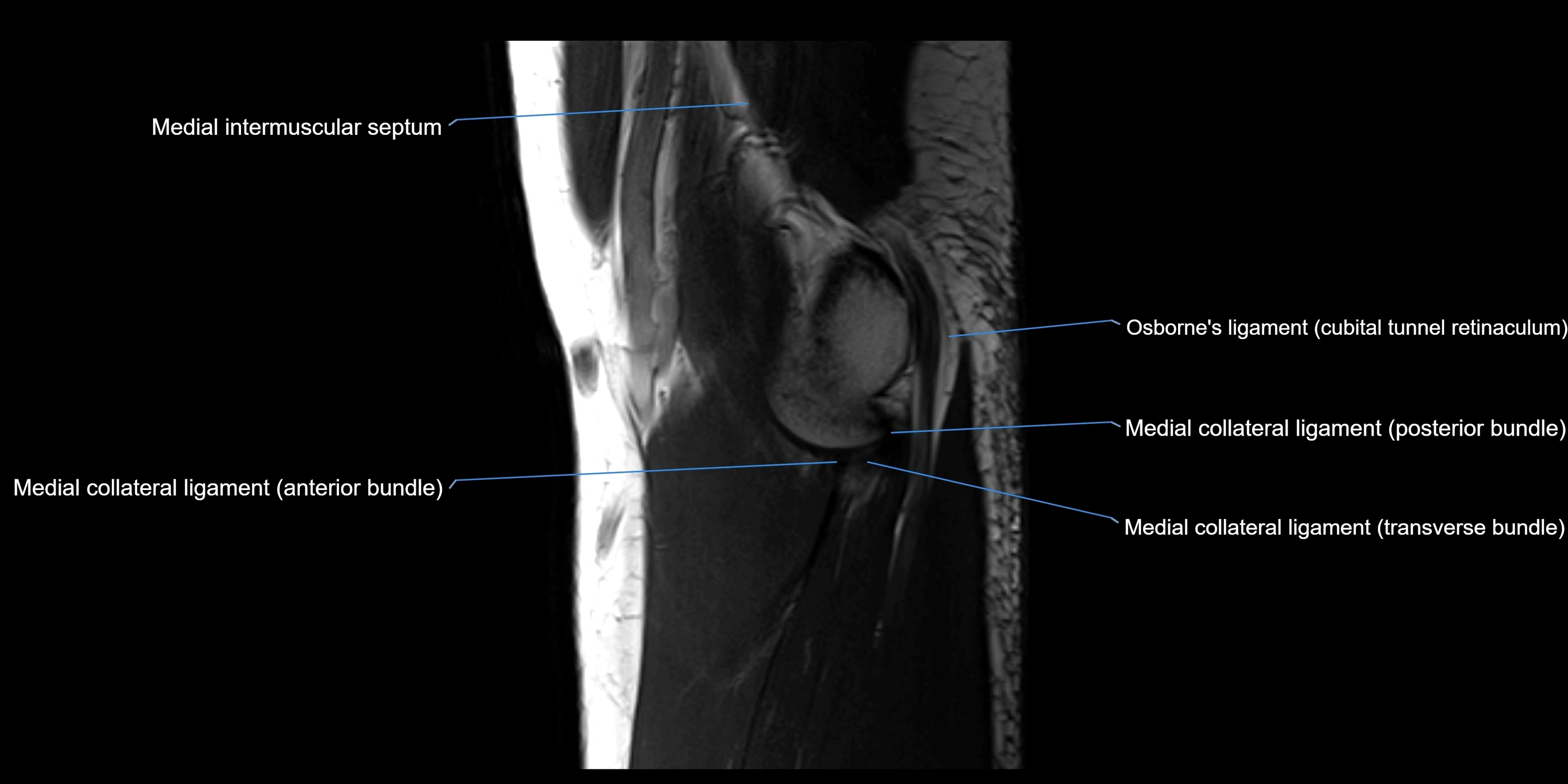
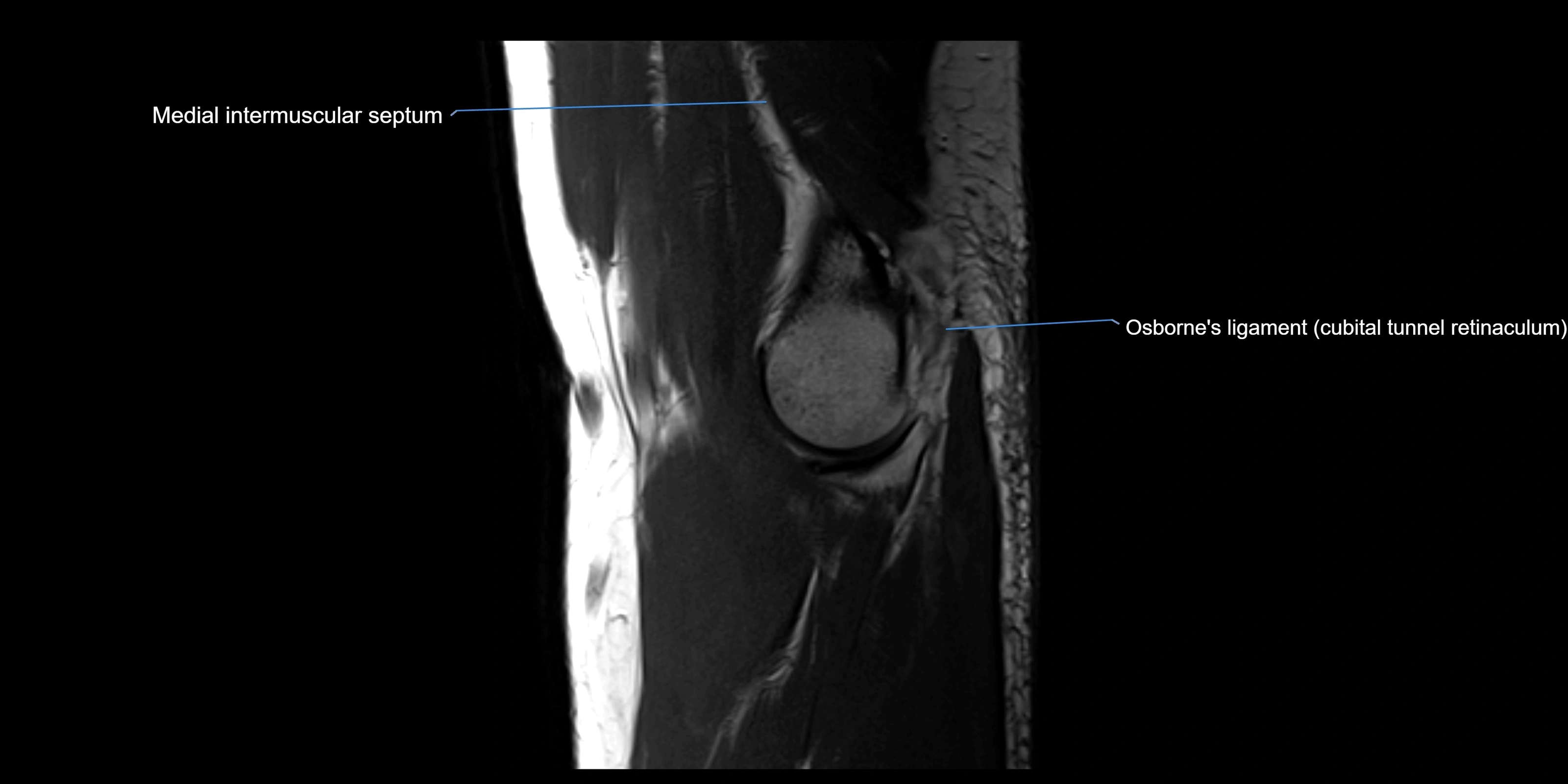
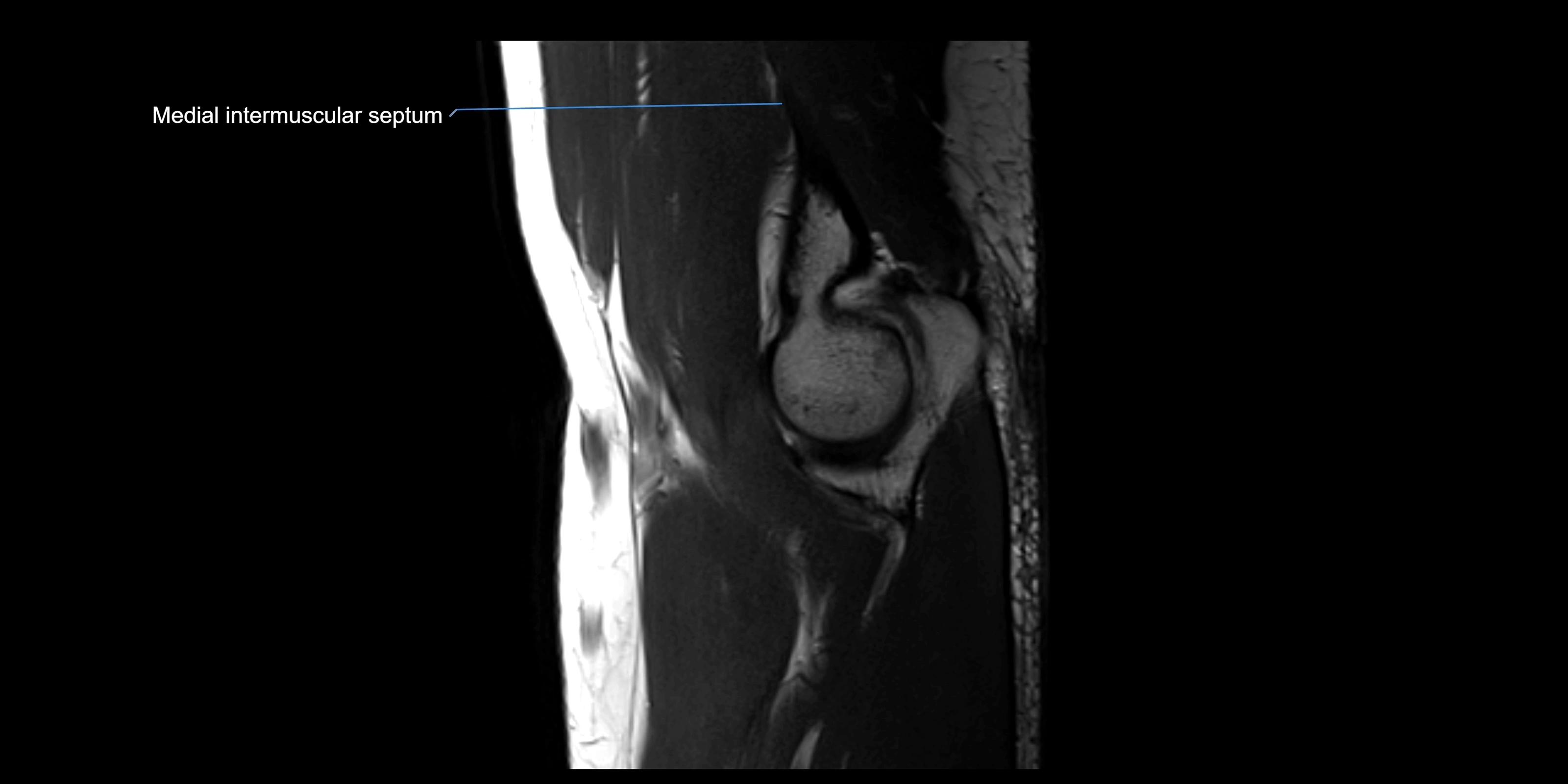
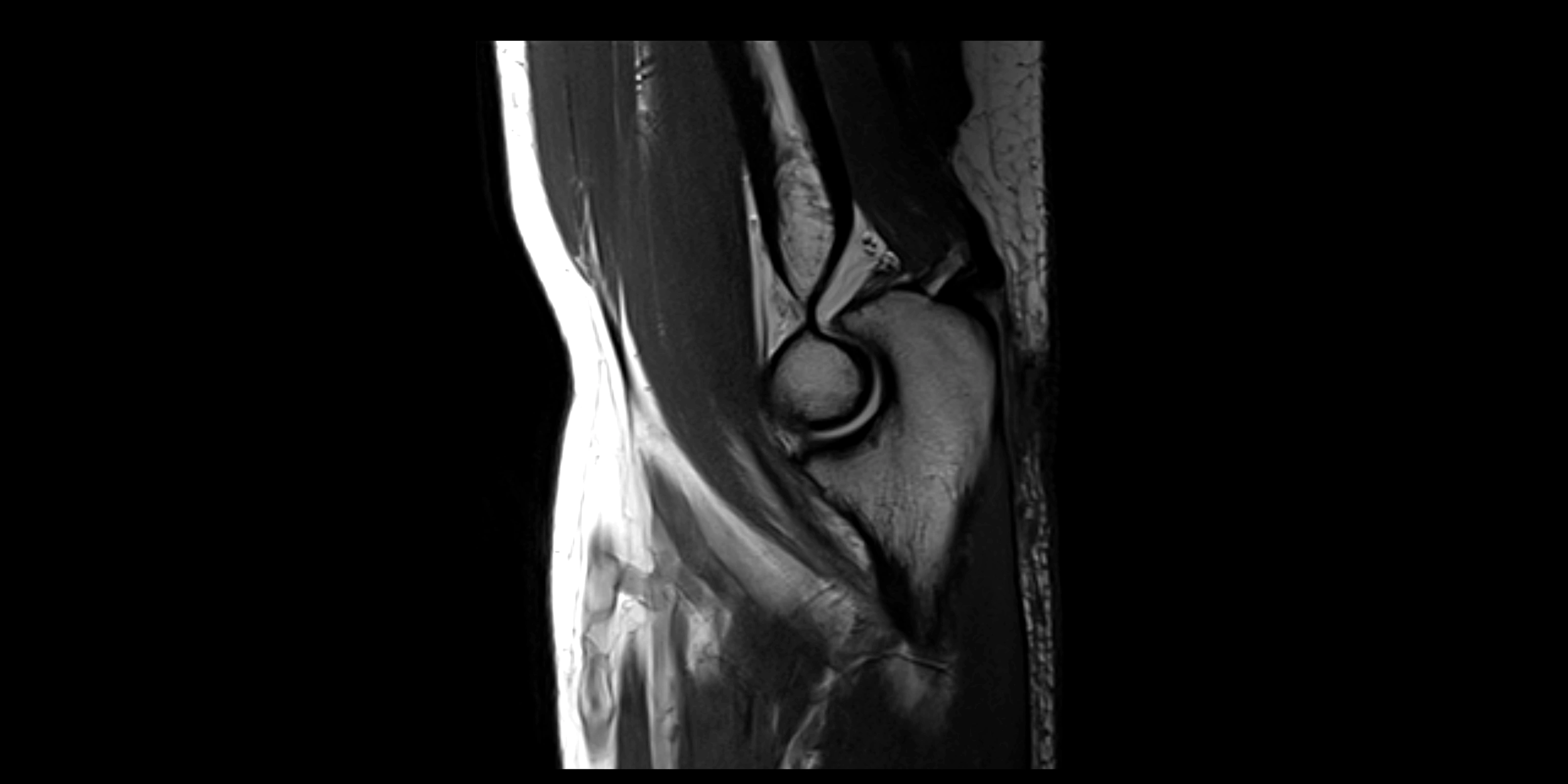
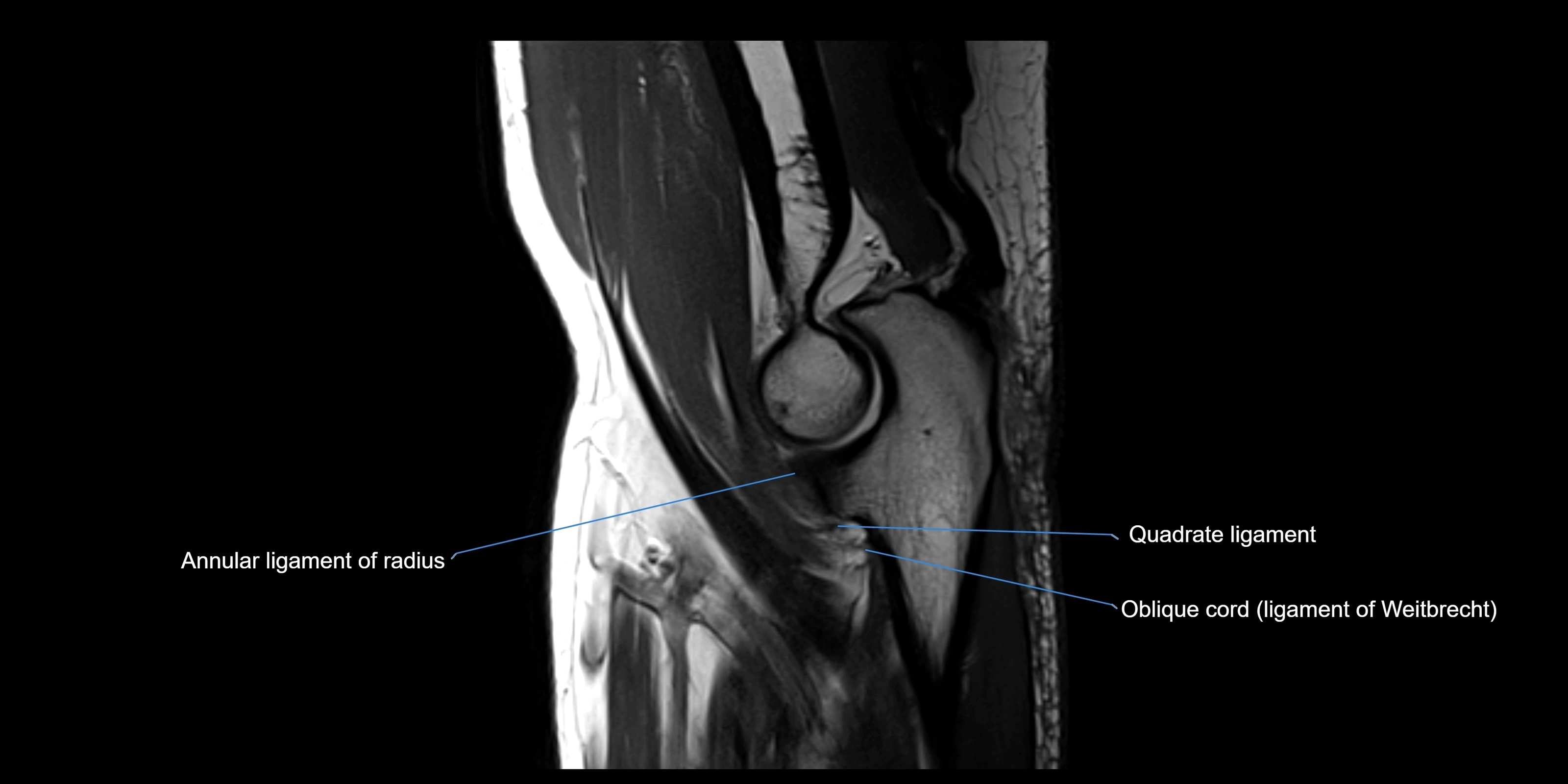
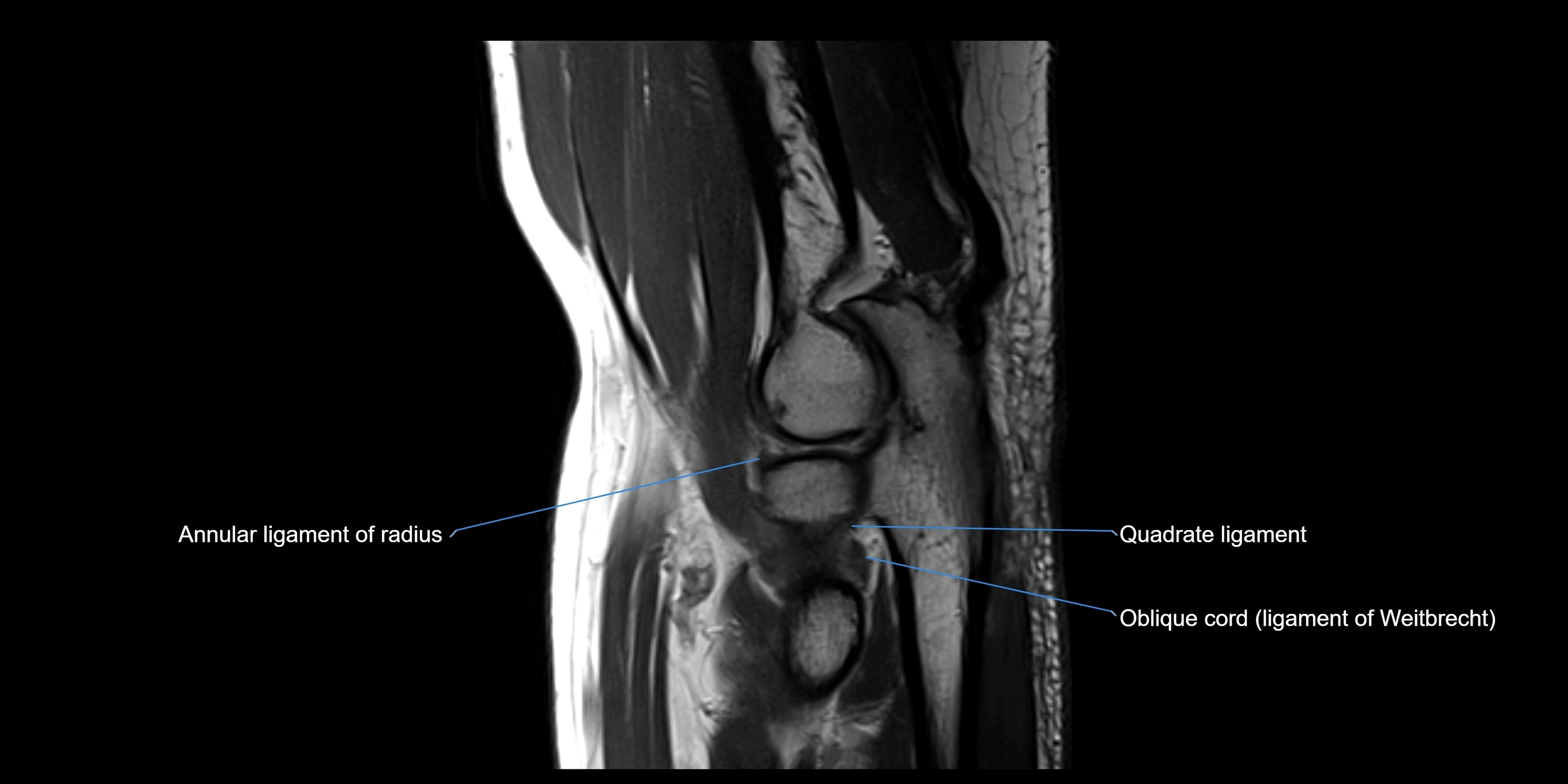
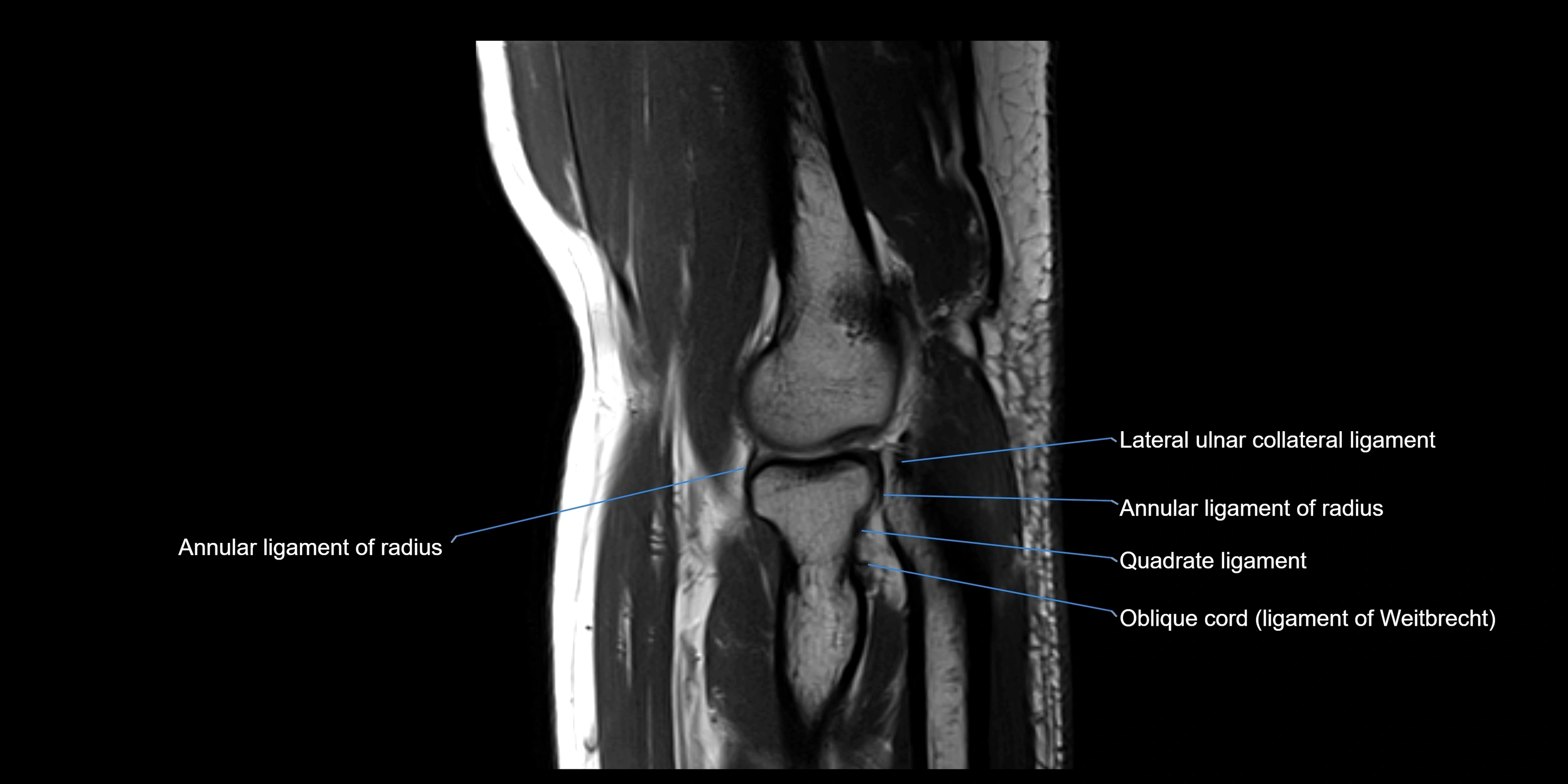
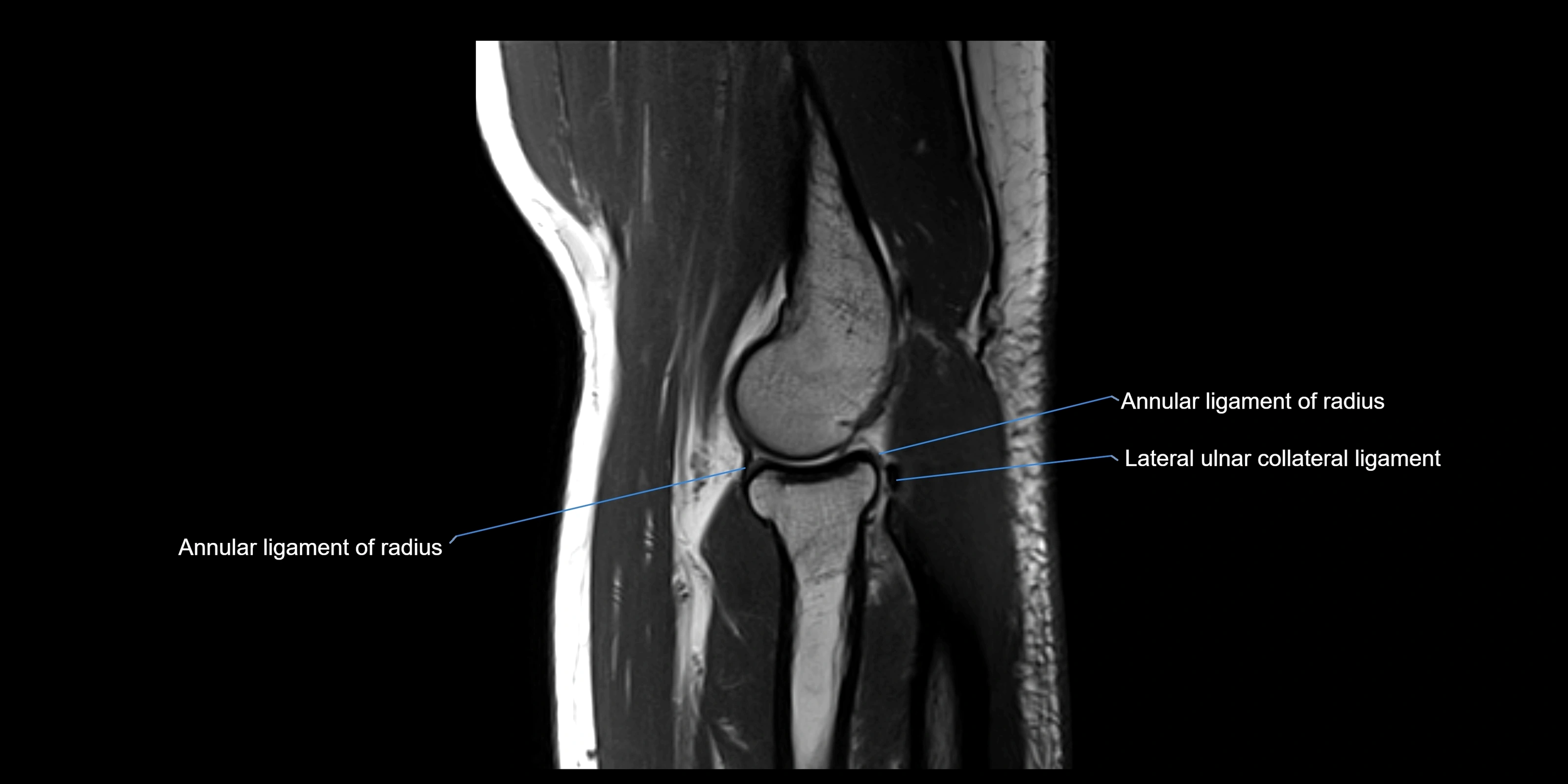
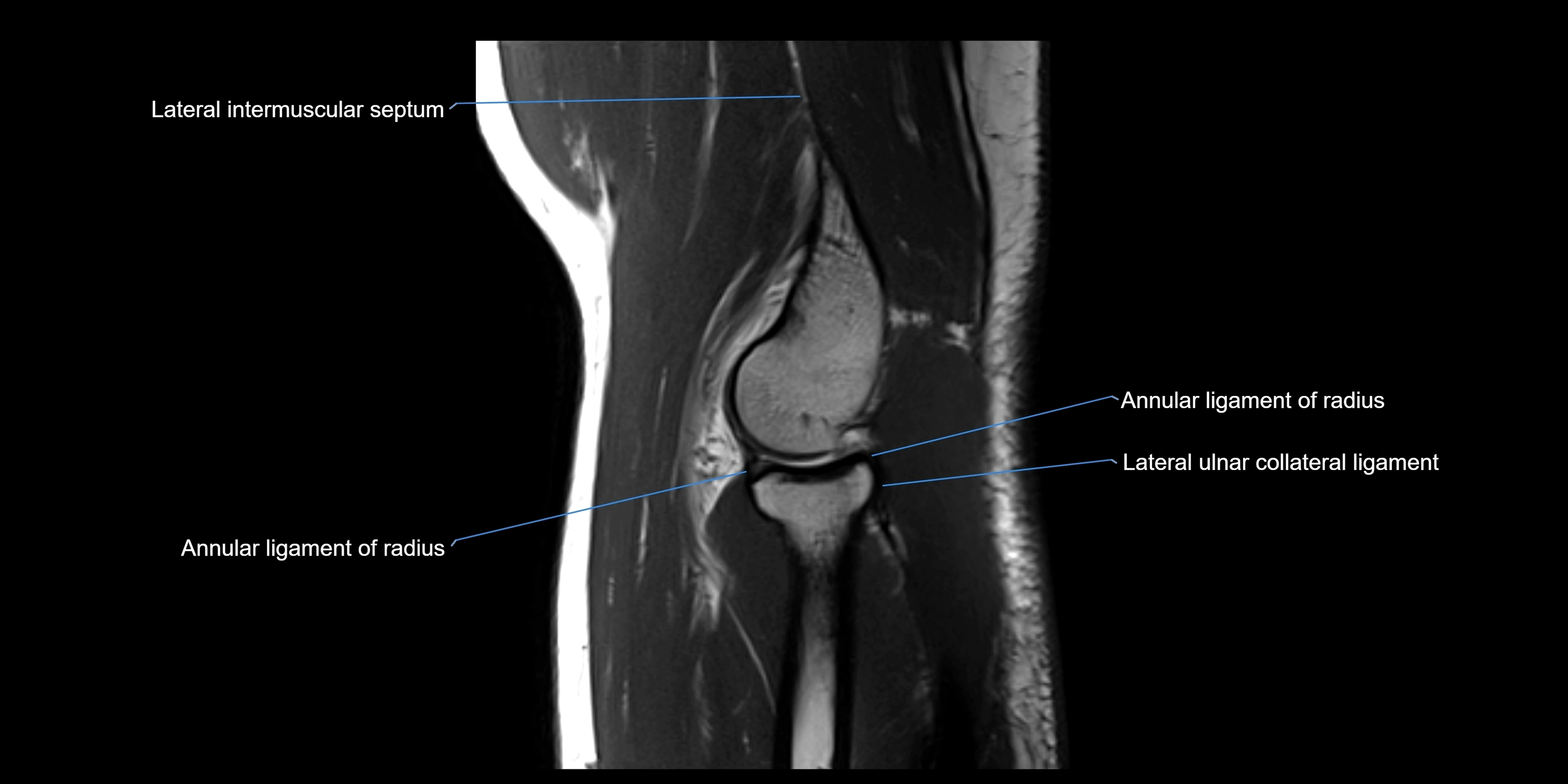
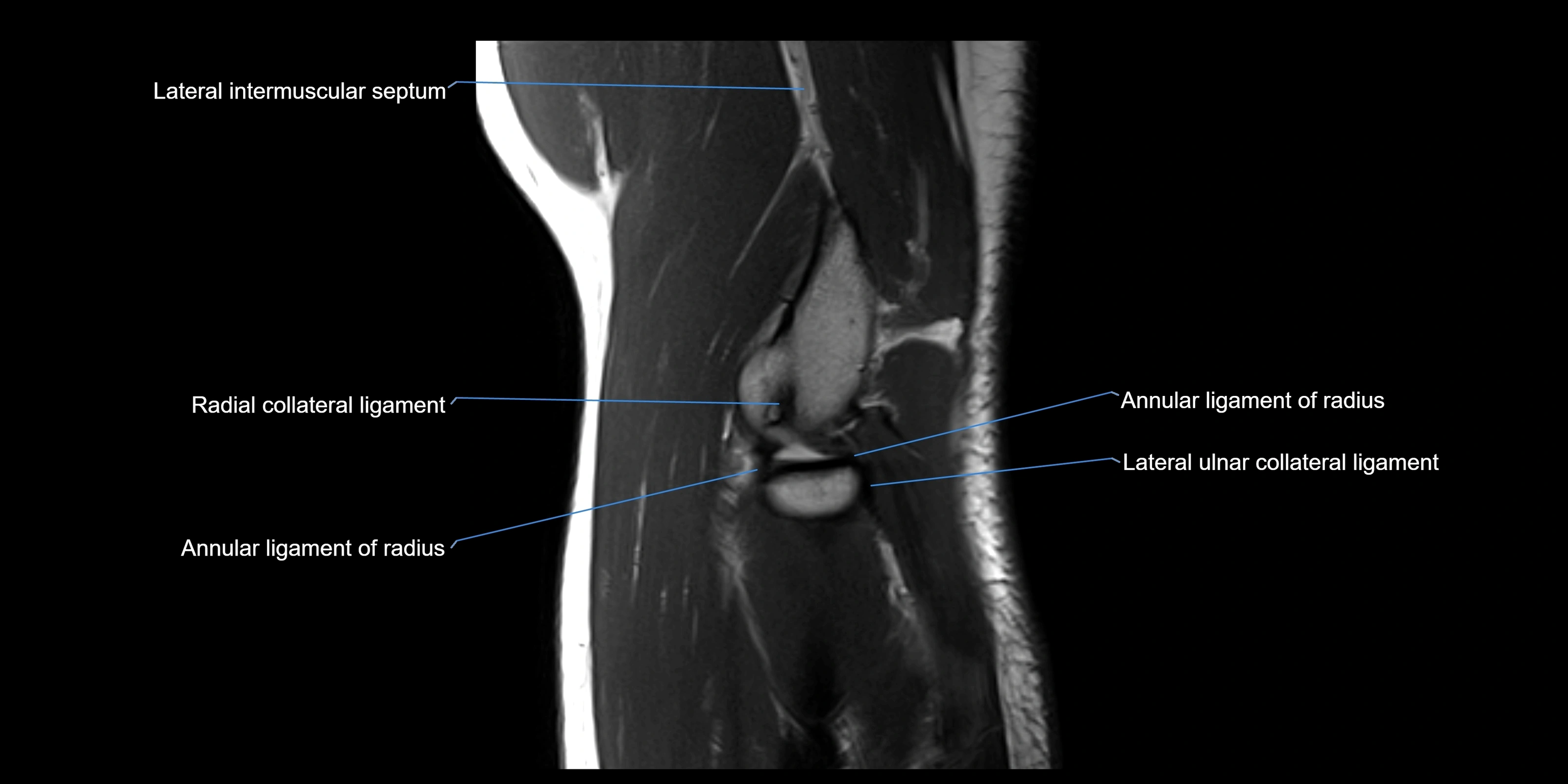
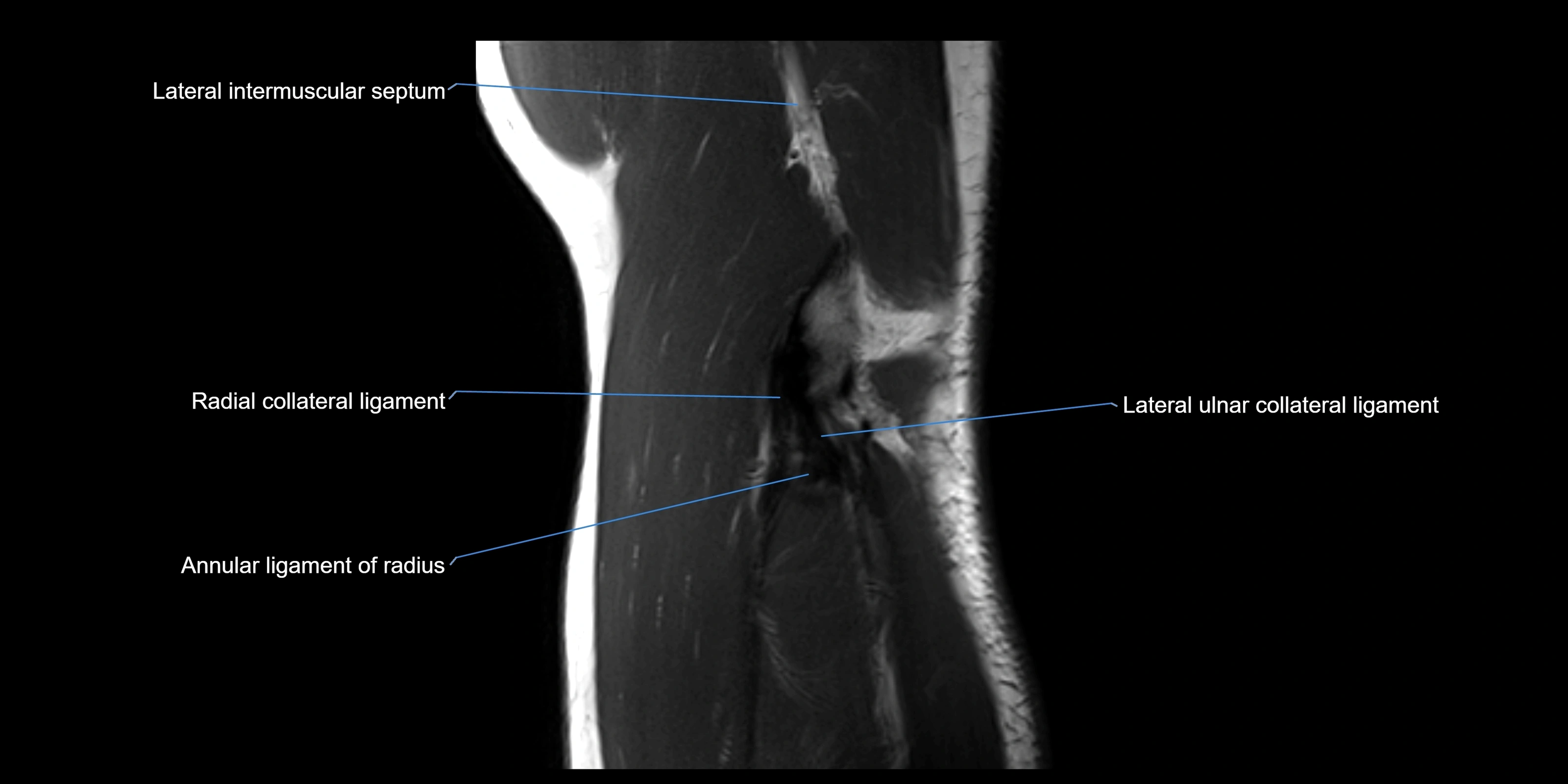
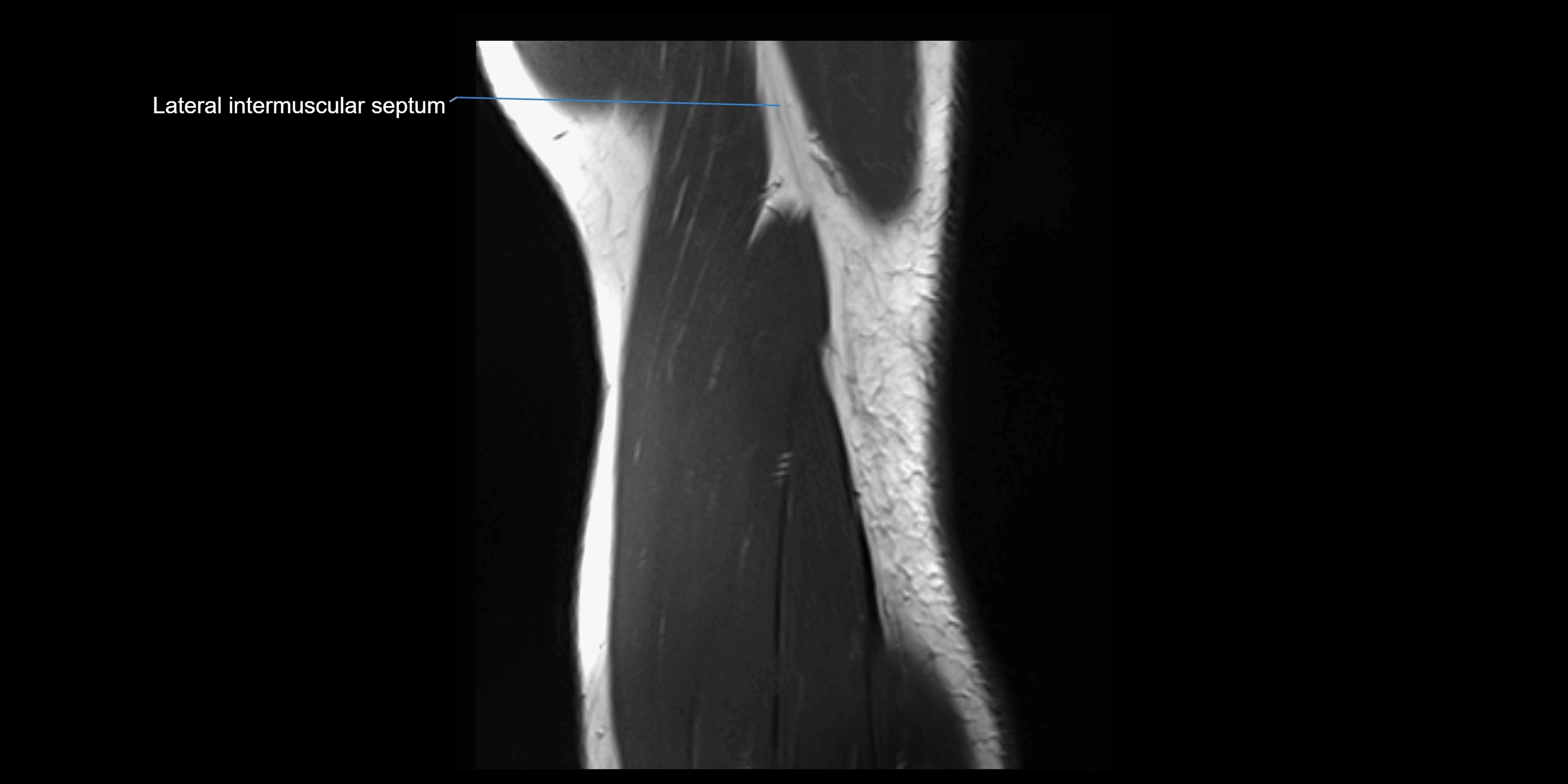
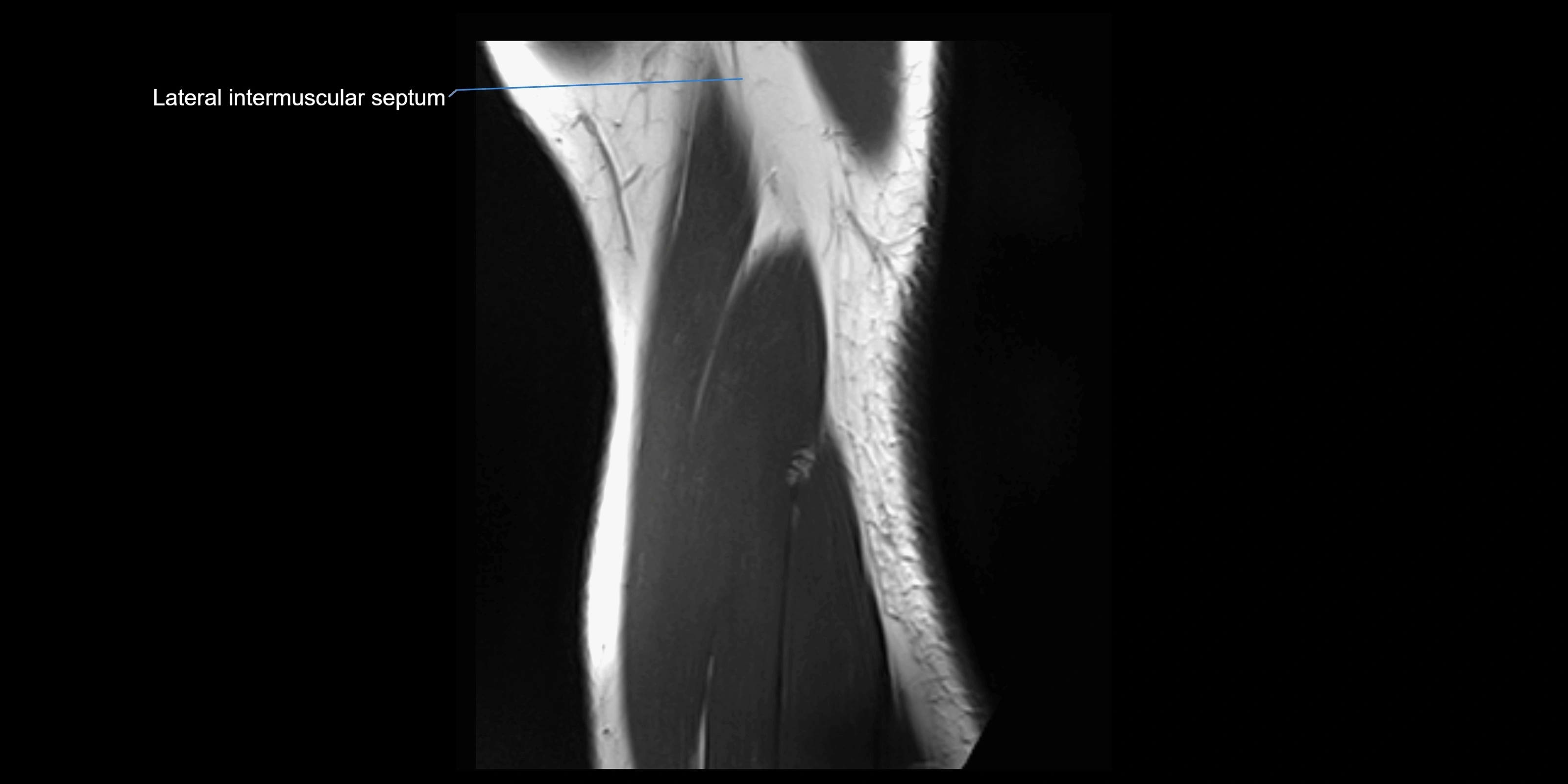
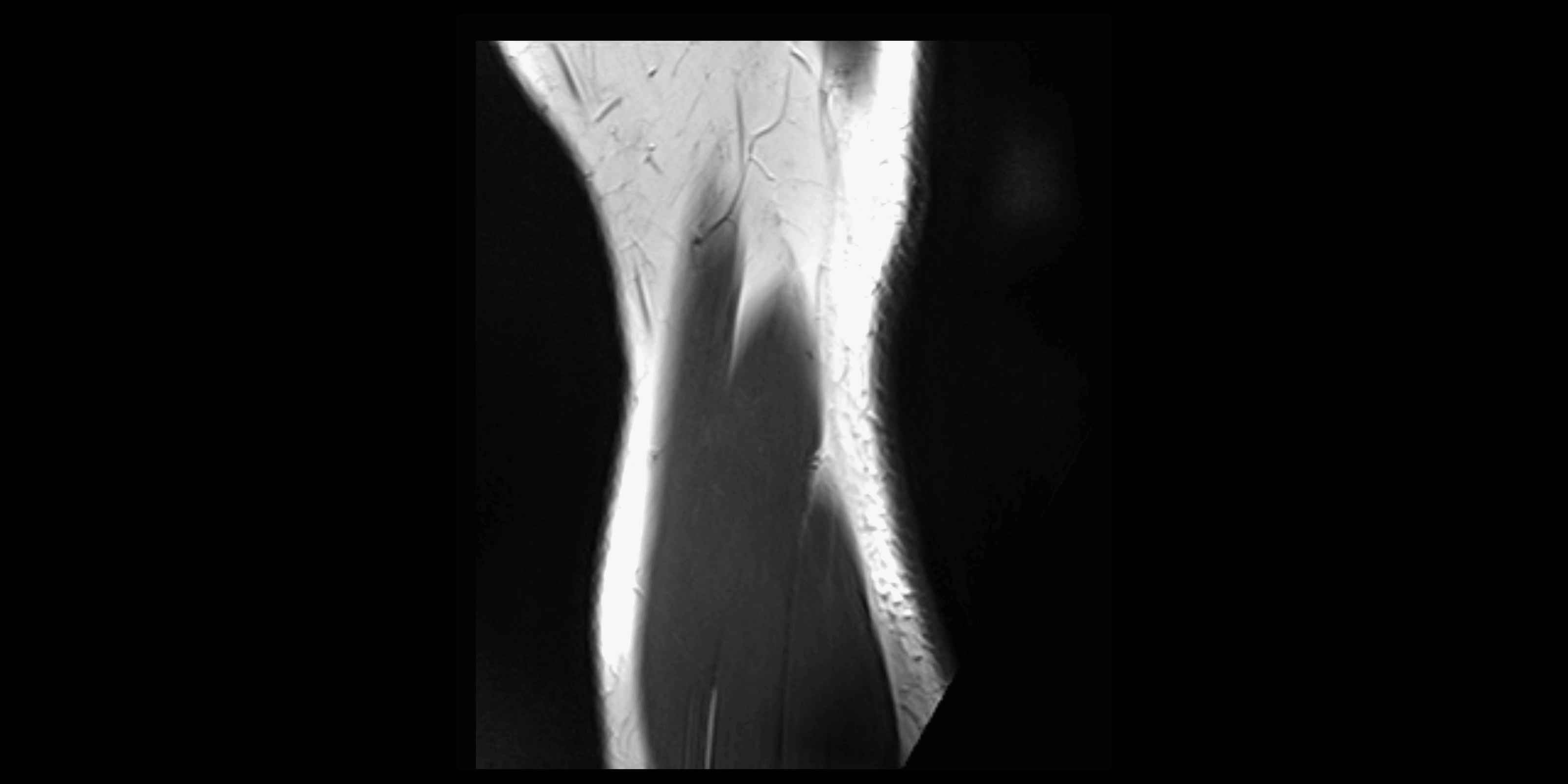
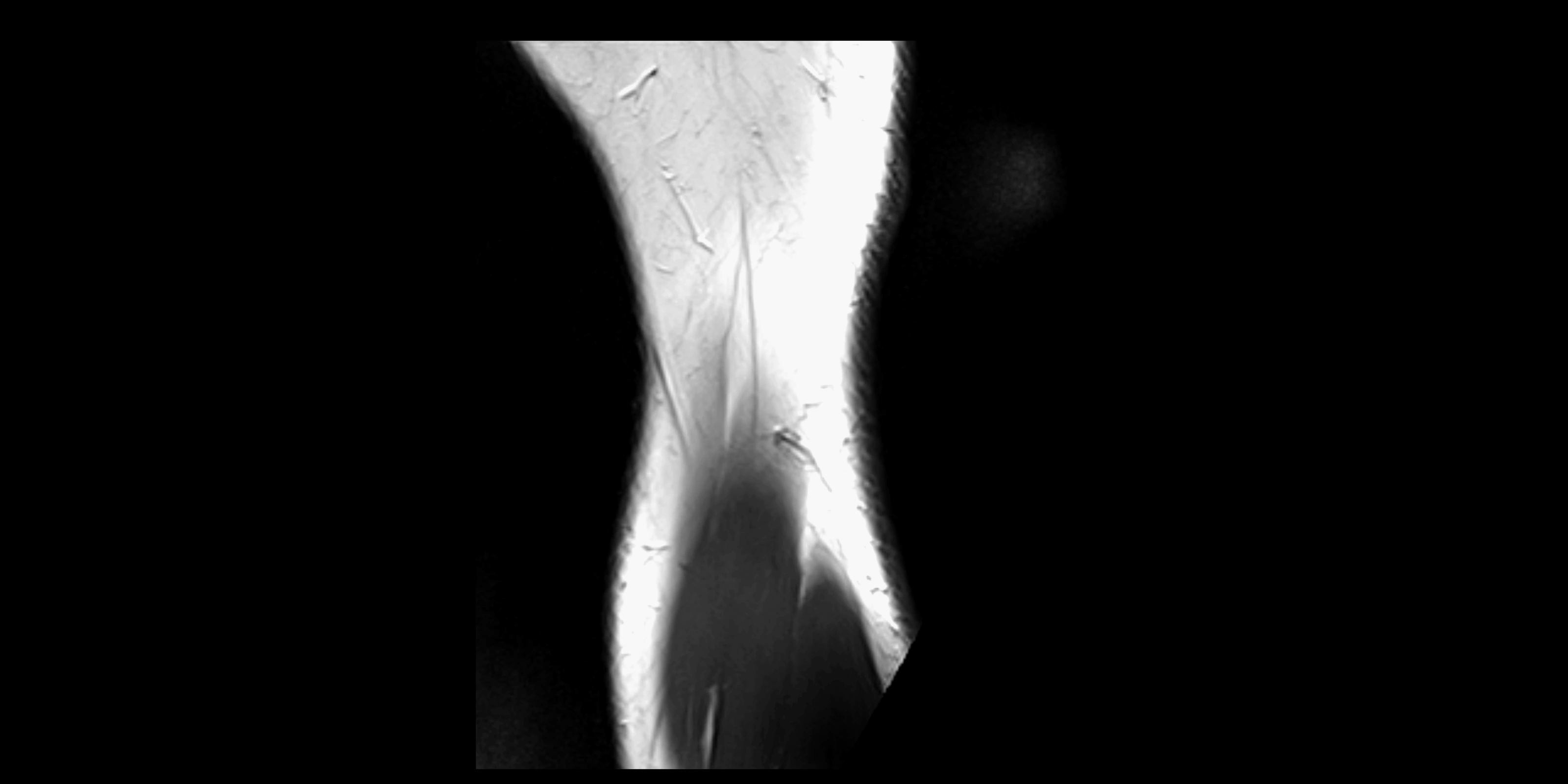
MRI images

MRI images

MRI images